
Surviving to Acute Myocardial Infarction: The Role of Psychological Factors and Alexithymia in Delayed Time to Searching Care: A Systematic Review

 , , and
, , and 
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.2. Definition of Pre-Hospital Delay (PHD) and Patients’ Decisional Delay (PDD)
2.3. Data Extraction
2.4. Quality Assessment
2.5. Data Analyses
3. Results
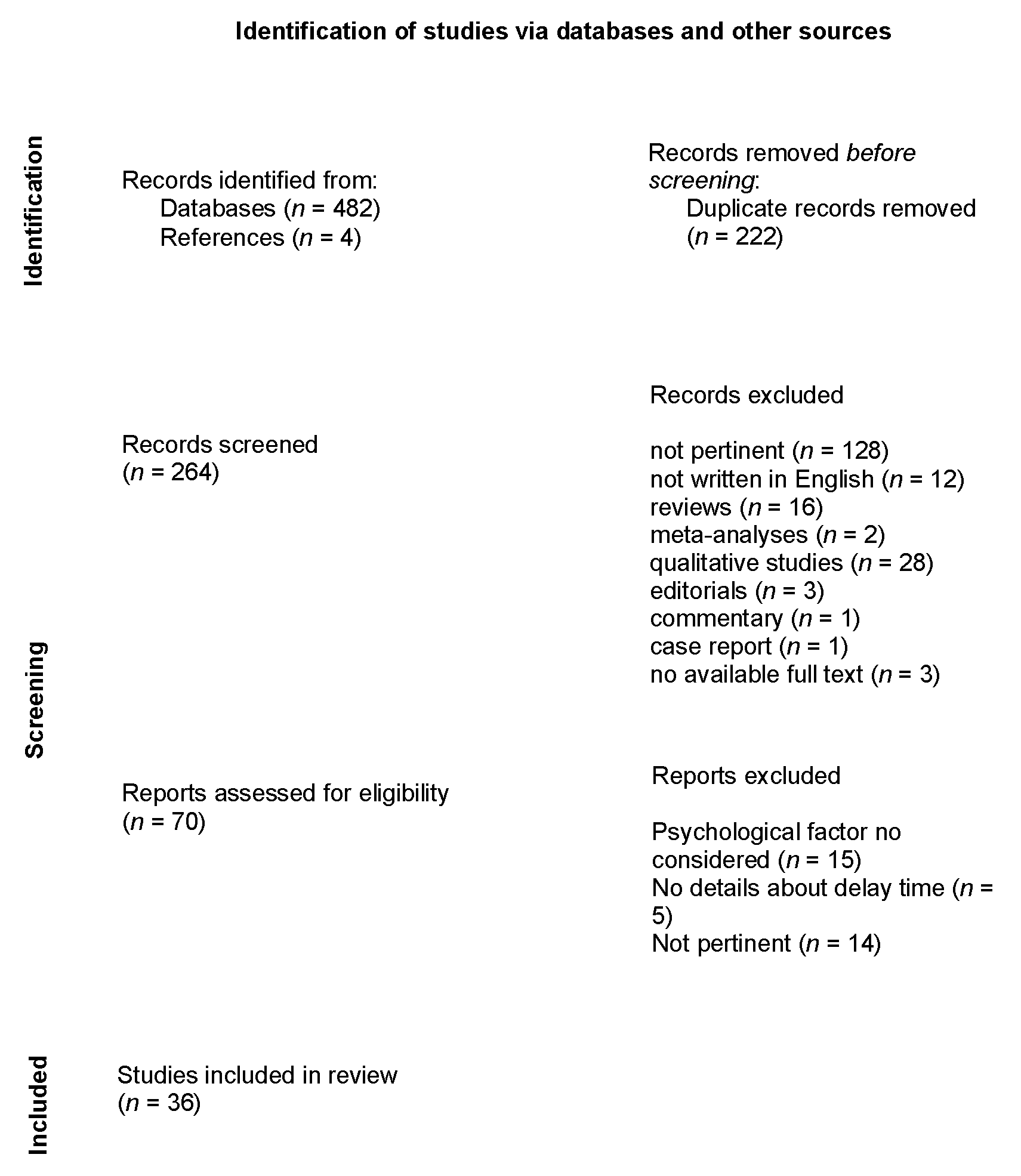
3.1. Search
3.2. Characteristics of the Included Studies
3.3. Psychological Factors Impacting Pre-Hospital or Decisional Delay
3.3.1. Appraisal of AMI Symptoms
3.3.2. Coping Strategies
3.3.3. Alexithymia
3.3.4. Other Psychological Factors
4. Discussion
4.1. Emotion Regulation in AMI
4.2. The Role Alexithymia in the Acute Phase of AMI
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Windecker, S.; Kolh, P.; Alfonso, F.; Collet, J.-P.; Cremer, J.; Falk, V.; Filippatos, G.; Hamm, C.W.; Head, S.J.; Jüni, P.; et al. 2014 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2014, 35, 2541–2619. [Google Scholar] [CrossRef]
- Moser, D.K.; Kimble, L.P.; Alberts, M.J.; Alonzo, A.; Croft, J.B.; Dracup, K.; Evenson, K.R.; Go, A.S.; Hand, M.M.; Kothari, R.U.; et al. Reducing delay in seeking treatment by patients with acute coronary syndrome and stroke: A scientific statement from the American Heart Association Council on cardiovascular nursing and stroke council. Circulation 2006, 11, 168–182. [Google Scholar] [CrossRef] [PubMed]
- De Luca, G.; Suryapranata, H.; Ottervanger, J.P.; Antman, E.M. Time delay to treatment and mortality in primary angioplasty for acute myocardial infarction: Every minute of delay counts. Circulation 2004, 109, 1223–1225. [Google Scholar] [CrossRef]
- Wijns, W.; Naber, C.K. Reperfusion delay in patients with high-risk ST-segment elevation myocardial infarction: Every minute counts, much more than suspected. Eur. Heart J. 2018, 39, 1075–1077. [Google Scholar] [CrossRef] [PubMed]
- Kenyon, L.W.; Ketterer, M.W.; Preisman, R.C. Psychological factors relevant to the prehospital and in-hospital phases of acute myocardial infarction. Henry Ford Hosp. Med. J. 1991, 39, 176–183. [Google Scholar] [PubMed]
- Dubayova, T.; van Dijk, J.P.; Nagyova, I.; Rosenberger, J.; Havlikova, E.; Gdovinova, Z.; Middel, B.; Groothoff, J.W. The impact of the intensity of fear on patient’s delay regarding health care seeking behavior: A systematic review. Int. J. Public Health 2010, 55, 459–468. [Google Scholar] [CrossRef] [PubMed]
- Dracup, K.; Moser, D.K.; Eisenberg, M.; Meischke, H.; Alonzo, A.A.; Braslow, A. Causes of delay in seeking treatment for heart attack symptoms. Soc. Sci. Med. 1995, 40, 379–392. [Google Scholar] [CrossRef]
- Gärtner, C.; Walz, L.; Bauernschmitt, E.; Ladwig, K.H. The causes of prehospital delay in myocardial infarction. Dtsch. Arztebl. Int. 2008, 105, 286–291. [Google Scholar] [CrossRef]
- Wielgosz, A.T.; Nolan, R.P. Understanding delay in response to symptoms of acute myocardial infarction: A compelling agenda. Circulation 1991, 84, 2193–2195. [Google Scholar] [CrossRef]
- Cosci, F. Assessment of personality in psychosomatic medicine: Current concepts. Adv. Psychosom. Med. 2012, 32, 133–159. [Google Scholar] [PubMed]
- Lumley, M.A.; Neely, L.C.; Burger, A.J. The assessment of alexithymia in medical settings: Implications for understanding and treating health problems. J. Pers. Assess. 2007, 89, 230–246. [Google Scholar] [CrossRef]
- Solano, L.; Pirrotta, E.; Ingravalle, V.; Fayella, P. The family physician and the psychologist in the office together: A response to fragmentation. Ment. Health Fam. Med. 2009, 6, 91–98. [Google Scholar]
- Porcelli, P.; Guidi, J.; Sirri, L.; Grandi, S.; Grassi, L.; Ottolini, F.; Pasquini, P.; Picardi, A.; Rafanelli, C.; Rigatelli, M.; et al. Alexithymia in the medically ill. Analysis of 1190 patients in gastroenterology, cardiology, oncology and dermatology. Gen. Hosp. Psychiatry 2013, 35, 521–527. [Google Scholar] [CrossRef] [PubMed]
- Sifneos, P. The Prevalence of ‘Alexithymic’ Characteristics in Psychosomatic Patients. Psychother. Psychosom. 1973, 22, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Taylor, G.J.; Bagby, R.M.; Parker, J.D.A. Disorders of Affect Regulation: Alexithymia in Medical and Psychiatric Illness; Cambridge University Press: Cambridge, UK, 1999. [Google Scholar]
- De Timary, P.; Roy, E.; Luminet, O.; Fillée, C.; Mikolajczak, M. Relationship between alexithymia, alexithymia factors and salivary cortisol in men exposed to a social stress test. Psychoneuroendocrinology 2008, 33, 1160–1164. [Google Scholar] [CrossRef]
- Pollatos, O.; Werner, N.S.; Duschek, S.; Schandry, R.; Matthias, E.; Traut-Mattausch, E.; Herbert, B.M. Differential effects of alexithymia subscales on autonomic reactivity and anxiety during social stress. J. Psychosom. Res. 2011, 70, 525–533. [Google Scholar] [CrossRef]
- Preti, A.; Sancassiani, F.; Cadoni, F.; Carta, M.G. Alexithymia affects pre-hospital delay of patients with acute myocardial infarction: Meta-analysis of existing studies. Clin. Pract. Epidemiol. Ment. Health 2013, 19, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Caltabellotta, T.; Magne, J.; Salerno, B.; Pradel, V.; Petitcolin, P.-B.; Auzemery, G.; Virot, P.; Aboyans, V. Characteristics associated with patient delay during the management of ST-segment elevated myocardial infarction, and the influence of awareness campaigns. Arch. Cardiovasc. Dis. 2020, 114, 305–315. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; A Goudevenos, J.; Halvorsen, S.; et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2017, 39, 119–177. [Google Scholar] [CrossRef]
- Downs, S.H.; Black, N. The feasibility of creating a checklist for the assessment of the methodological quality both of randomised and non-randomised studies of health care interventions. J. Epidemiol. Community Health 1998, 52, 377–384. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Song, L.; Yan, H.; Yang, J.; Sun, Y.; Hu, D. Impact of patients’ symptom interpretation on care-seeking behaviors of patients with acute myocardial infarction. Chin. Med. J. 2010, 123, 1840–1844. [Google Scholar]
- Clark, L.T.; Bellam, S.V.; Shah, A.H.; Feldman, J.G. Analysis of prehospital delay among inner city patients with symptoms of myo-cardial infarction: Implications for therapeutic intervention. J. Natl. Med. Assoc. 1992, 84, 11. [Google Scholar]
- Dracup, K.; Moser, D.K. Beyond sociodemographics: Factors influencing the decision to seek treatment for symptoms of acute myocardial infarction. Heart Lung 1997, 26, 253–262. [Google Scholar] [CrossRef]
- Dracup, K.; McKinley, S.M.; Moser, D.K. Australian patients’ delay in response to heart attack symptoms. MJA 1997, 166, 233–236. [Google Scholar] [CrossRef] [PubMed]
- Fukuoka, Y.; Dracup, K.; Rankin, S.H.; Froelicher, E.S.; Kobayashi, F.; Hirayama, H.; Ohno, M.; Matsumoto, D. Prehospital delay and independent/interdependent construal of self among Japanese patients with acute myocardial infarction. Soc. Sci. Med. 2005, 60, 2025–2034. [Google Scholar] [CrossRef] [PubMed]
- Markus, H.R.; Kitayama, S. Culture and the self: Implications for cognition, emotion, and motivation. Psychol. Rev. 1991, 98, 224–253. [Google Scholar] [CrossRef]
- Horne, R.; James, D.; Petrie, K.; Weinman, J.; Vincent, R. Patients’ interpretation of symptoms as a cause of delay in reaching hospital during acute myocardial infarction. Heart 2000, 83, 388–393. [Google Scholar] [CrossRef] [PubMed]
- McKinley, S.; Moser, D.K.; Dracup, K. Treatment-seeking behavior for acute myocardial infarction symptoms in North America and Australia. Heart Lung 2000, 29, 4. [Google Scholar] [CrossRef] [PubMed]
- McKinley, S.; Dracup, K.; Moser, D.K.; Ball, C.; Yamasaki, K.; Kim, C.J.; Barnett, M. International comparison of factors associated with delay in presentation for AMI treatment. Eur. J. Cardiovasc. Nurs. 2004, 3, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Khraim, F.M.; Scherer, Y.K.; Dorn, J.M.; Carey, M.G. Predictors of Decision Delay to Seeking Health Care among Jordanians With Acute Myocardial Infarction. J. Nurs. Scholarsh. 2009, 41, 260–267. [Google Scholar] [CrossRef]
- Perry, K.; Petrie, K.J.; Ellis, C.J.; Horne, R.; Moss-Morris, R. Symptom expectations and delay in acute myocardial infarction patients. Heart 2001, 86, 91–93. [Google Scholar] [CrossRef][Green Version]
- O’Carroll, R.E.; Smith, K.B.; Grubb, N.R.; Fox, K.A.A.; Masterton, G. Psychological factors associated with delay in attending hospital following a myocardial infarction. J. Psychosom. Res. 2001, 51, 611–614. [Google Scholar] [CrossRef]
- Carney, R.; Fitzsimon, D.; Dempster, M. Why people experiencing acute myocardial infarction delay seeking medical assistance. Eur. J. Cardiovasc. Nurs. 2002, 1, 237–242. [Google Scholar] [CrossRef]
- Al-Hassan, M.A.; Omran, S.M. The effects of health beliefs on health care-seeking decisions of Jordanian patients with myocardial infarction symptom. Int. J. Nurs. Pract. 2005, 11, 13–20. [Google Scholar] [CrossRef]
- Abed, M.A.; Khalil, A.A.; Moser, D.K. The Contribution of Symptom Incongruence to Prehospital Delay for Acute Myocardial Infarction Symptoms among Jordanian Patients. Res. Nurs. Health 2015, 38, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Burnett, R.E.; Blumenthal, J.A.; Mark, D.; Leimberger, J.D.; Califf, R.M. Distinguishing between early and late responders to symptoms of acute myocardial infarction. Am. J. Cardiol. 1995, 75, 1019–1022. [Google Scholar] [CrossRef]
- Nymark, C.; Henriksson, P.; Mattiasson, A.-C.; Saboonchi, F.; Kiessling, A. Inability to act was associated with an extended delay prior to care-seeking, in patients with an acute myocardial infarction. Eur. J. Cardiovasc. Nurs. 2019, 18, 512–520. [Google Scholar] [CrossRef]
- Khan, M.S.; Jafary, F.H.; Faruqui, A.M.; Rasool, S.I.; Hatcher, J.; Chaturvedi, N.; Jafar, T.H. High prevalence of lack of knowledge of symptoms of acute myocardial infarction in Pakistan and its contribution to delayed presentation to the hospital. BMC Public Health 2007, 9, 284. [Google Scholar]
- Hwang, S.Y.; Jeong, M.H. Cognitive factors that influence delayed decision to seek treatment among older patients with acute myocardial infarction in Korea. Eur. J. Cardiovasc. Nurs. 2012, 11, 154–159. [Google Scholar] [CrossRef]
- Morgan, D.M. Effect of incongruence of acute myocardial infarction symptoms on the decision to seek treatment in a rural population. J. Cardiovasc. Nurs. 2005, 20, 365–371. [Google Scholar] [CrossRef] [PubMed]
- Momeni, M.; Salari, A.; Shafighnia, S.; Ghanbari, A.; Mirbolouk, F. Factors influencing pre-hospital delay among patients with acute myocardial infarction in Iran. Chin. Med. J. 2012, 125, 3404–3409. [Google Scholar] [PubMed]
- Li, P.; Yu, D.S.F. Testing a Model to Reveal the Predictive Mechanism of Care-Seeking Decisions among Patients with Acute Myocardial Infarction. J. Cardiovasc. Nurs. 2017, 32, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Yu, D.S. Predictors of pre-hospital delay in Hong Kong Chinese patients with acute myocardial infarction. Eur. J. Cardiovasc. Nurs. 2017, 17, 75–84. [Google Scholar] [CrossRef]
- Lesneski, L. Factors influencing treatment delay for patients with acute myocardial infarction. Appl. Nurs. Res. 2010, 23, 185–190. [Google Scholar] [CrossRef]
- Meloni, L.; Montisci, R.; Pippia, V.; Sancassiani, F.; Carta, M.G. Alexithymia affects the time from symptom onset to calling the emergency system in STEMI patients referred for primary PCI. Int. J. Cardiol. 2016, 219, 428–432. [Google Scholar] [CrossRef] [PubMed]
- Fox-Wasylyshyn, S.M.; El-Masri, M.; Artinian, N.T. Testing a Model of Delayed Care-Seeking for Acute Myocardial Infarction. Clin. Nurs. Res. 2010, 19, 38–54. [Google Scholar] [CrossRef]
- Kentsch, M.; Rodemerk, U.; Müller-Esch, G.; Schnoor, U.; Münzel, T.; Ittel, T.H.; Mitusch, R. Emotional attitudes toward symptoms and inadequate coping strategies are major determinants of patient delay in acute myocardial infarction. Z. Kardiol. 2002, 91, 147–155. [Google Scholar] [CrossRef]
- Zegrean, M.; Fox-Wasylyshyn, S.M.; El-Masri, M.M. Alternative Coping Strategies and Decision Delay in Seeking Care for Acute Myocardial Infarction. J. Cardiovasc. Nurs. 2009, 24, 151–155. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Bleeker, J.K.; Lamers, L.M.; Leenders, I.M.; Kruyssen, D.C.; Simoons, M.L.; Trijsburg, R.W.; Erdman, R.A. Psychological and knowledge factors related to delay of help-seeking by patients with acute myocardial infarction. Psychother. Psychosom. 1995, 63, 151–158. [Google Scholar] [CrossRef] [PubMed]
- Dracup, K.; Moser, D.K.; McKinley, S.; Ball, C.; Yamasaki, K.; Kim, C.; Doering, L.V.; Caldwell, M.A. An International Perspective on the Time to Treatment for Acute Myocardial Infarction. J. Nurs. Scholarsh. 2003, 35, 317–323. [Google Scholar] [CrossRef]
- Walsh, J.C.; Lynch, M.; Murphy, A.W.; Daly, K. Factors influencing the decision to seek treatment for symptoms of acute myocardial infarction. An evaluation of the Self-Regulatory Model of illness behaviour. J. Psychosom. Res. 2004, 56, 67–73. [Google Scholar] [CrossRef]
- Fang, X.; Albarqouni, L.; Rothe, A.V.E.; Hoschar, S.; Ronel, J.; Ladwig, K.-H. Is denial a maladaptive coping mechanism which prolongs pre-hospital delay in patients with ST-segment elevation myocardial infarction? Psychosomatics 2016, 91, 68–74. [Google Scholar] [CrossRef][Green Version]
- Kenyon, L.W.; Ketterer, M.W.; Gheorghiade, M.; Goldstein, S. Psychological factors related to prehospital delay during acute myocardial infarction. Circulation 1991, 84, 1969–1976. [Google Scholar] [CrossRef]
- Carta, M.G.; Sancassiani, F.; Pippia, V.; Bhat, K.M.; Sardu, C.; Meloni, L. Alexithymia is associated with delayed treatment seeking in acute myocardial infarction. Psychother. Psychosom. 2013, 28, 190–192. [Google Scholar] [CrossRef]
- Albarqouni, L.; Rothe, A.V.E.; Ronel, J.; Meinertz, T.; Ladwig, K. Frequency and covariates of fear of death during myocardial infarction and its impact on prehospital delay: Findings from the multicentre MEDEA Study. Clin. Res. Cardiol. 2015, 105, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wu, S.; Pan, J.; Hoschar, S.; Wang, Z.; Tu, R.; Ladwig, K.-H.; Ma, W. The impact of the Type D Personality pattern on prehospital delay in patients suffering from acute myocardial infarction. J. Thorac. Dis. 2020, 12, 4680–4689. [Google Scholar] [CrossRef] [PubMed]
- Luepker, R.V. Barriers to patients seeking emergency care for acute coronary heart disease. JAMA 2000, 1, 2184. [Google Scholar]
- Theisen, M.E.; MacNeill, S.E.; Lumley, M.A.; Ketterer, M.W.; Goldberg, A.D.; Borzak, S. Psychosocial factors related to unrecognized acute myocardial infarction. Am. J. Cardiol. 1995, 15, 1211–1213. [Google Scholar] [CrossRef]
- Fang, X.Y.; Spieler, D.; Albarqouni, L.; Ronel, J.; Ladwig, K.-H. Impact of generalized anxiety disorder (GAD) on prehospital delay of acute myocardial infarction patients. Findings from the multicenter MEDEA study. Clin. Res. Cardiol. 2018, 107, 471–478. [Google Scholar] [CrossRef] [PubMed]
- Perkins-Porras, L.; Whitehead, D.L.; Strike, P.C.; Steptoe, A. Causal beliefs, cardiac denial and pre-hospital delays following the onset of acute coronary syndromes. J. Behav. Med. 2008, 31, 498–505. [Google Scholar] [CrossRef]
- Hwang, S.Y.; Zerwic, J.J.; Jeong, M.H. Impact of prodromal symptoms on prehospital delay in patients with first-time acute myo-cardial infarction in Korea. J. Cardiovasc. Nurs. 2011, 26, 194–201. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, T.; Fox-Wasylyshyn, S. Predictors of cardiac symptom attribution among AMI patients. Can. J. Cardiovasc. Nurs. 2011, 21, 14–22. [Google Scholar]
- Krystal, H. Integration and Self-Healing: Affect, Trauma, Alexithymia; Analytic Press: Hillsdale, NJ, USA, 1998. [Google Scholar]
- Alonzo, A.A.; Reynolds, N.R. The structure of emotions during acute myocardial infarction: A model of coping. Soc. Sci. Med. 1998, 46, 1099–1110. [Google Scholar] [CrossRef]
- Alonzo, A.A. Acute myocardial infarction and posttraumatic stress disorder: The consequences of cumulative adversity. J. Cardiovasc. Nurs. 1999, 13, 33–45. [Google Scholar] [CrossRef] [PubMed]
- Kano, M.; Fukudo, S.; Gyoba, J.; Kamachi, M.; Tagawa, M.; Mochizuki, H.; Itoh, M.; Hongo, M.; Yanai, K. Specific brain processing of facial expressions in people with alexithymia: An H2 15O-PET study. Brain 2003, 126, 1474–1484. [Google Scholar] [CrossRef] [PubMed]
- Almeida, O.P.; Garrido, G.J.; Beer, C.; Lautenschlager, N.T.; Arnolda, L.; Lenzo, N.P.; Campbell, A.; Flicker, L. Coronary heart disease is associated with regional grey matter volume loss: Implications for cognitive function and behaviour. Intern. Med. J. 2008, 38, 599–606. [Google Scholar] [CrossRef] [PubMed]
- Beresnevaite, M. Exploring the benefits of group psychotherapy in reducing alexithymia in coronary heart disease patients: A preliminary study. Psychother. Psychosom. 2000, 69, 117–122. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sancassiani, F.; Montisci, R.; Preti, A.; Paribello, P.; Meloni, L.; Romano, F.; Nardi, A.E.; Carta, M.G. Surviving to Acute Myocardial Infarction: The Role of Psychological Factors and Alexithymia in Delayed Time to Searching Care: A Systematic Review. J. Clin. Med. 2021, 10, 3813. https://doi.org/10.3390/jcm10173813
Sancassiani F, Montisci R, Preti A, Paribello P, Meloni L, Romano F, Nardi AE, Carta MG. Surviving to Acute Myocardial Infarction: The Role of Psychological Factors and Alexithymia in Delayed Time to Searching Care: A Systematic Review. Journal of Clinical Medicine. 2021; 10(17):3813. https://doi.org/10.3390/jcm10173813
Chicago/Turabian StyleSancassiani, Federica, Roberta Montisci, Antonio Preti, Pasquale Paribello, Luigi Meloni, Ferdinando Romano, Antonio E. Nardi, and Mauro Giovanni Carta. 2021. "Surviving to Acute Myocardial Infarction: The Role of Psychological Factors and Alexithymia in Delayed Time to Searching Care: A Systematic Review" Journal of Clinical Medicine 10, no. 17: 3813. https://doi.org/10.3390/jcm10173813
APA StyleSancassiani, F., Montisci, R., Preti, A., Paribello, P., Meloni, L., Romano, F., Nardi, A. E., & Carta, M. G. (2021). Surviving to Acute Myocardial Infarction: The Role of Psychological Factors and Alexithymia in Delayed Time to Searching Care: A Systematic Review. Journal of Clinical Medicine, 10(17), 3813. https://doi.org/10.3390/jcm10173813