
Diagnostic Value of EUS-Guided Fine-Needle Aspiration Biopsy for Gastric Linitis Plastica with Negative Endoscopic Biopsy

 , , ,
, , , 

Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Eligibility and Study Design
2.2. Endoscopic Procedures
2.3. Outcome Measures
2.4. Statistical Analysis
3. Results
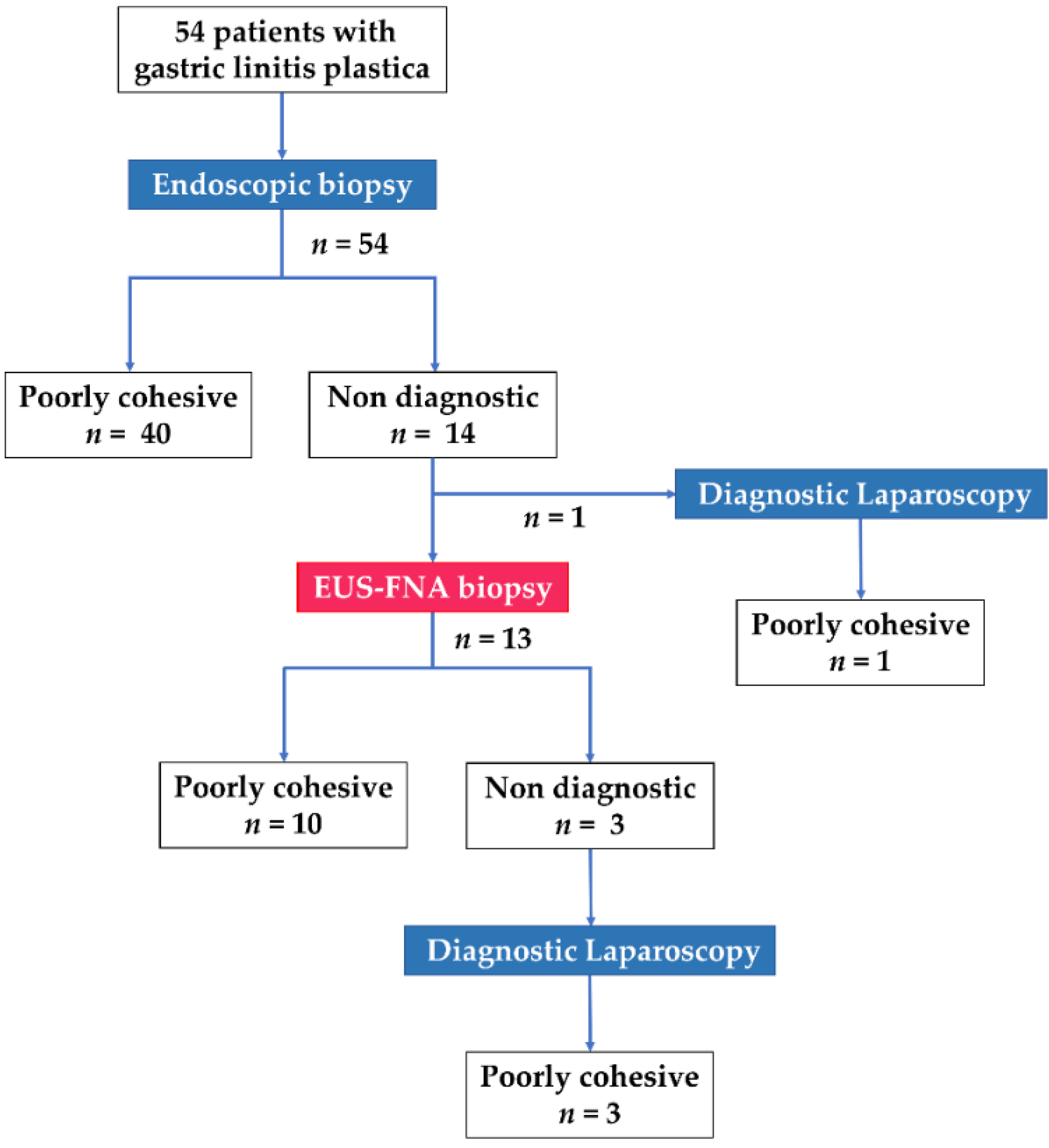
3.1. Selection of Patients with GLP
3.2. Characteristics of Patients with GLP
3.3. Utility of EUS-FNA Biopsy for Patients with GLP
3.4. Factors Associated with Negative Conventional Biopsy Findings in Patients with GLP
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Nagtegaal, I.D.; Odze, R.D.; Klimstra, D.; Paradis, V.; Rugge, M.; Schirmacher, P.; Washington, K.M.; Carneiro, F.; Cree, I.A.; WHO Classification of Tumours Editorial Board. The 2019 WHO Classification of Tumours of the Digestive System. Histopathology 2020, 76, 182–188. [Google Scholar] [CrossRef] [PubMed]
- Lauren, P. The Two Histological Main Types of Gastric Carcinoma: Diffuse and So-Called Intestinal-Type Carcinoma. An Attempt at a Histo-Clinical Classification. Acta Pathol. Microbiol. Scand. 1965, 64, 31–49. [Google Scholar] [CrossRef]
- Tan, I.B.; Ivanova, T.; Lim, K.H.; Ong, C.W.; Deng, N.; Lee, J.; Tan, S.H.; Wu, J.; Lee, M.H.; Ooi, C.H.; et al. Intrinsic Subtypes of Gastric Cancer, Based on Gene Expression Pattern, Predict Survival and Respond Differently to Chemotherapy. Gastroenterology 2011, 141, 476–485.e1. [Google Scholar] [CrossRef] [PubMed]
- Cristescu, R.; Lee, J.; Nebozhyn, M.; Kim, K.M.; Ting, J.C.; Wong, S.S.; Liu, J.; Yue, Y.G.; Wang, J.; Yu, K.; et al. Molecular Analysis of Gastric Cancer Identifies Subtypes Associated with Distinct Clinical Outcomes. Nat. Med. 2015, 21, 449–456. [Google Scholar] [CrossRef]
- Mastoraki, A.; Papanikolaou, I.S.; Sakorafas, G.; Safioleas, M. Facing the Challenge of Managing Linitis Plastica--Review of the Literature. Hepatogastroenterology 2009, 56, 1773–1778. [Google Scholar]
- Agnes, A.; Estrella, J.S.; Badgwell, B. The Significance of a Nineteenth Century Definition in the Era of Genomics: Linitis Plastica. World J. Surg. Oncol. 2017, 15, 123. [Google Scholar] [CrossRef]
- Sowa, M.; Kato, Y.; Kubo, T.; Nakanishi, K.; Nishimura, M.; Chung, Y.S.; Umeyama, K. Clinicopathological and Histochemical Studies of Linitis Plastica Type Gastric Cancer with Special Reference to Early Gastric Cancer in the Region of the Fundic Gland. Osaka City Med. J. 1991, 37, 11–22. [Google Scholar]
- Park, J.C.; Lee, Y.C.; Kim, J.H.; Kim, Y.J.; Lee, S.K.; Hyung, W.J.; Noh, S.H.; Kim, C.B. Clinicopathological Aspects and Prognostic Value with Respect to Age: An Analysis of 3362 Consecutive Gastric Cancer Patients. J. Surg. Oncol. 2009, 99, 395–401. [Google Scholar] [CrossRef]
- Schauer, M.; Peiper, M.; Theisen, J.; Knoefel, W. Prognostic Factors in Patients with Diffuse Type Gastric Cancer (Linitis Plastica) After Operative Treatment. Eur. J. Med. Res. 2011, 16, 29–33. [Google Scholar] [CrossRef]
- Petrelli, F.; Berenato, R.; Turati, L.; Mennitto, A.; Steccanella, F.; Caporale, M.; Dallera, P.; de Braud, F.; Pezzica, E.; Di Bartolomeo, M.; et al. Prognostic Value of Diffuse Versus Intestinal Histotype in Patients with Gastric Cancer: A Systematic Review and Meta-Analysis. J. Gastrointest. Oncol. 2017, 8, 148–163. [Google Scholar] [CrossRef] [PubMed]
- Xiao, H.; Ma, M.; Xiao, Y.; Ouyang, Y.; Tang, M.; Zhou, K.; Hong, Y.; Tang, B.; Zuo, C. Incomplete Resection and Linitis Plastica Are Factors for Poor Survival after Extended Multiorgan Resection in Gastric Cancer Patients. Sci. Rep. 2017, 7, 15800. [Google Scholar] [CrossRef] [PubMed]
- Vivier-Chicoteau, J.; Lambert, J.; Coriat, R.; Bonnot, P.E.; Goere, D.; Roche, B.; Dior, M.; Goujon, G.; Morgant, S.; Pocard, M.; et al. Development and Internal Validation of a Diagnostic Score for Gastric Linitis Plastica. Gastric Cancer 2020, 23, 639–647. [Google Scholar] [CrossRef]
- Levine, M.S.; Kong, V.; Rubesin, S.E.; Laufer, I.; Herlinger, H. Scirrhous Carcinoma of the Stomach: Radiologic and Endoscopic Diagnosis. Radiology 1990, 175, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Song, W.; Chen, C.Y.; Xu, J.B.; Ye, J.N.; Wang, L.; Chen, C.Q.; Zhang, X.H.; Cai, S.R.; Zhan, W.H.; He, Y.L. Pathological Diagnosis Is Maybe Non-Essential for Special Gastric Cancer: Case Reports and Review. World J. Gastroenterol. 2013, 19, 3904–3910. [Google Scholar] [CrossRef]
- Bree, R.L.; McGough, M.F.; Schwab, R.E. CT or US-Guided Fine Needle Aspiration Biopsy in Gastric Neoplasms. J. Comput. Assist. Tomogr. 1991, 15, 565–569. [Google Scholar] [CrossRef] [PubMed]
- Green, J.; Katz, S.; Phillips, G.; Bank, S.; Ilardi, C.; Hadju, E.; Siegel, F. Percutaneous Sonographic Needle Aspiration Biopsy of Endoscopically Negative Gastric Carcinoma. Am. J. Gastroenterol. 1988, 83, 1150–1153. [Google Scholar]
- Kodani, T.; Osada, T.; Matsumoto, K.; Kato, J.; Higashihara, Y.; Morimoto, T.; Ogata, C.; Taniguchi, G.; Mizui, T.; Matsumura, Y.; et al. Endoscopic Mucosal Resection Using a Cap-Fitted Panendoscope as a Diagnostic Procedure in a Case of Scirrhous Gastric Carcinoma. Dig. Endosc. 2012, 24, 190. [Google Scholar] [CrossRef]
- Zhou, X.X.; Pan, H.H.; Usman, A.; Ji, F.; Jin, X.; Zhong, W.X.; Chen, H.T. Endoscopic Ultrasound-Guided Deep and Large Biopsy for Diagnosis of Gastric Infiltrating Tumors with Negative Malignant Endoscopy Biopsies. World J. Gastroenterol. 2015, 21, 3607–3613. [Google Scholar] [CrossRef]
- Chiyo, T.; Kobara, H.; Mori, H.; Katsuki, N.; Haba, R.; Masaki, T. Submucosal Endoscopic Sampling for Indefinite Gastric Linitis Plastica Infiltrating into the Submucosal Layer. J. Gastrointestin. Liver Dis. 2015, 24, 375–378. [Google Scholar] [CrossRef]
- Carter, J.E.; Nelson, J.J.; Eves, M.; Boudreaux, C. Diagnosis of Linitis Plastica-Type Gastric Adenocarcinoma by Endoscopic Ultrasound-Guided Fine Needle Aspiration: A Case Report. Acta Cytol. 2008, 52, 725–728. [Google Scholar] [CrossRef]
- Liu, Y.; Chen, K.; Yang, X.J. Endoscopic Ultrasound-Guided Fine-Needle Aspiration Used in Diagnosing Gastric Linitis Plastica: Metastatic Lymph Nodes Can Be Valuable Targets. J. Gastroenterol. Hepatol. 2019, 34, 202–206. [Google Scholar] [CrossRef] [PubMed]
- Muraoka, S.; Tsuchida, K.; Iwasaki, M.; Izawa, N.; Jinnai, H.; Komatsubara, T.; Tsunemi, M.; Sakuma, F.; Kashima, K.; Fukushi, K.; et al. A Case Report of Gastric Linitis Plastica Diagnosed by Endoscopic Ultrasound-Guided Fine Needle Aspiration. Medicine 2017, 96, e8937. [Google Scholar] [CrossRef] [PubMed]
- Yoshinaga, S.; Hilmi, I.N.; Kwek, B.E.; Hara, K.; Goda, K. Current Status of Endoscopic Ultrasound for the Upper Gastrointestinal Tract in Asia. Dig. Endosc. 2015, 27, 2–10. [Google Scholar] [CrossRef] [PubMed]
- Amin, M.B.; Greene, F.L.; Edge, S.B.; Compton, C.C.; Gershenwald, J.E.; Brookland, R.K.; Meyer, L.; Gress, D.M.; Byrd, D.R.; Winchester, D.P. The, 8th ed AJCC Cancer Staging Manual: Continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J. Clin. 2017, 67, 93–99. [Google Scholar] [CrossRef]
- Choi, Y.; Choi, H.S.; Jeon, W.K.; Kim, B.I.; Park, D.I.; Cho, Y.K.; Kim, H.J.; Park, J.H.; Sohn, C.I. Optimal Number of Endoscopic Biopsies in Diagnosis of Advanced Gastric and Colorectal Cancer. J. Korean Med. Sci. 2012, 27, 36–39. [Google Scholar] [CrossRef] [PubMed]
- Vilmann, P.; Jacobsen, G.K.; Henriksen, F.W.; Hancke, S. Endoscopic Ultrasonography with Guided Fine Needle Aspiration Biopsy in Pancreatic Disease. Gastrointest. Endosc. 1992, 38, 172–173. [Google Scholar] [CrossRef]
- Wang, K.X.; Ben, Q.W.; Jin, Z.D.; Du, Y.Q.; Zou, D.W.; Liao, Z.; Li, Z.S. Assessment of Morbidity and Mortality Associated with EUS-Guided FNA: A Systematic Review. Gastrointest. Endosc. 2011, 73, 283–290. [Google Scholar] [CrossRef]
- Minaga, K.; Takenaka, M.; Katanuma, A.; Kitano, M.; Yamashita, Y.; Kamata, K.; Yamao, K.; Watanabe, T.; Maguchi, H.; Kudo, M. Needle Tract Seeding: An Overlooked Rare Complication of Endoscopic Ultrasound-Guided Fine-Needle Aspiration. Oncology 2017, 93, 107–112. [Google Scholar] [CrossRef]
- Smith, E.H. Complications of Percutaneous Abdominal Fine-Needle Biopsy. Radiology 1991, 178, 253–258. [Google Scholar] [CrossRef]
- Wardeh, R.; Lee, J.G.; Gu, M. Endoscopic ultrasound-guided paracentesis of ascitic fluid: A morphologic study with ultrasonographic correlation. Cancer Cytopathol. 2011, 119, 27–36. [Google Scholar] [CrossRef] [PubMed]
- Ye, Y.; Tan, S. Endoscopic Ultrasound-Guided Fine-Needle Aspiration Biopsy for Diagnosis of Gastric Linitis Plastica with Negative Malignant Endoscopy Biopsies. Oncol. Lett. 2018, 16, 4915–4920. [Google Scholar] [CrossRef]
- Bang, J.Y.; Hebert-Magee, S.; Hasan, M.K.; Navaneethan, U.; Hawes, R.; Varadarajulu, S. Endoscopic Ultrasonography-Guided Biopsy Using a Franseen Needle Design: Initial Assessment. Dig. Endosc. 2017, 29, 338–346. [Google Scholar] [CrossRef] [PubMed]
- Zimmer, V.; Heinrich, C.; Mues, E.P. Gastrointestinal: Franseen-Tip Transmural Fine-Needle Biopsy for Localized Gastric Linitis Plastica. J. Gastroenterol. Hepatol. 2021, 36, 1389. [Google Scholar] [CrossRef] [PubMed]
- Cheng, B.; Zhang, Y.; Chen, Q.; Sun, B.; Deng, Z.; Shan, H.; Dou, L.; Wang, J.; Li, Y.; Yang, X.; et al. Analysis of Fine-Needle Biopsy vs Fine-Needle Aspiration in Diagnosis of Pancreatic and Abdominal Masses: A Prospective, Multicenter, Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2018, 16, 1314–1321. [Google Scholar] [CrossRef]
- Songür, Y.; Okai, T.; Watanabe, H.; Motoo, Y.; Sawabu, N. Endosonographic evaluation of giant gastric folds. Gastrointest. Endosc. 1995, 41, 468–474. [Google Scholar] [CrossRef]
- Probst, A.; Schaller, T.; Sommer, F.; Geissler, B.; Agaimy, A.; Messmann, H.; Märkl, B. Immunoglobulin G4 (IgG4)-related disease of the stomach—A challenging differential diagnosis in suspected gastric cancer. Z. Gastroenterol. 2019, 57, 1298–1303. [Google Scholar] [CrossRef]
- Matynia, A.P.; Schmidt, R.L.; Barraza, G.; Layfield, L.J.; Siddiqui, A.A.; Adler, D.G. Impact of rapid on-site evaluation on the adequacy of endoscopic-ultrasound guided fine-needle aspiration of solid pancreatic lesions: A systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2014, 29, 697–705. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patient Characteristics | n = 54 |
|---|---|
| Median age, years (IQR) | 66 (50–72) |
| Sex, male/female, n (%) | 29 (53.7)/25 (46.3) |
| Cancer stage (UICC 8th classification) | |
| Ib/IIIb/IV, n (%) | 1 (1.9)/2 (3.7)/51 (94.4) |
| Affected part of the stomach | |
| Diffuse/segmental, n (%) | 31 (57.4)/23 (42.6) |
| Median serum CEA, ng/mL (IQR) | 2.75 (1.7–5.55) |
| Ulcerations | |
| Yes/No, n (%) | 24 (44.4)/30 (55.6) |
| Saint Louis linitis score | |
| 3/3.5/4/5/6, n (%) | 9 (16.7)/2 (3.7)/15 (27.8)/26 (48.1)/2 (3.7) |
| Median number of biopsies (IQR) | 6 (5–9) |
| Endoscopic biopsy result | |
| Poorly cohesive/no malignancy, n (%) | 40 (74.1)/14 (25.9) |
| Treatment, n (%) | |
| Chemotherapy | 29 (53.7) |
| Surgical resection | 1 (1.9) |
| Surgical resection after chemotherapy | 16 (29.6) |
| Best supportive care | 8 (14.8) |
| Age, Sex | CEA, ng/mL | Affected Part of the Stomach | Endoscopy | EUS | ||||
|---|---|---|---|---|---|---|---|---|
| Ulceration | Number of Biopsies | Wall Thickness, mm | Type of Needle | Number of Needle Passes | EUS-FNA Biopsy Result | |||
| 40, F | 1.0 | Diffuse | No | 17 | 20 | 22-gauge, FNA | 3 | Atypical cells |
| 81, M | 5.4 | Segmental | No | 10 | 25 | 22-gauge, FNA | 3 | Poorly cohesive |
| 83, M | 2.4 | Diffuse | No | 8 | 20 | 22-gauge, FNA | 3 | No malignancy |
| 53, M | 1.4 | Diffuse | No | 13 | 15 | 22-gauge, FNB | 5 | Poorly cohesive |
| 82, M | 6.9 | Segmental | Yes | 6 | 25 | 22-gauge, FNB | 3 | Poorly cohesive |
| 75, F | 6.6 | Segmental | No | 7 | 15 | 22-gauge, FNB | 3 | Poorly cohesive |
| 60, F | 4.6 | Segmental | No | 5 | 15 | 22-gauge, FNB | 3 | Poorly cohesive |
| 84, M | 7.4 | Segmental | No | 16 | 20 | 22-gauge, FNB | 3 | Poorly cohesive |
| 81, M | 4.7 | Segmental | No | 6 | 15 | 22-gauge, FNB | 3 | Poorly cohesive |
| 42, F | 1.7 | Diffuse | No | 13 | 20 | 22-gauge, FNB | 3 | Poorly cohesive |
| 68, M | 2.3 | Diffuse | No | 22 | 20 | 22-gauge, FNB | 3 | Poorly cohesive |
| 60, M | 7.5 | Segmental | No | 9 | 18 | 22-gauge, FNB | 5 | Poorly cohesive |
| 67, M | 2.8 | Segmental | No | 9 | 20 | 22-gauge, FNB | 3 | No malignancy |
| Univariable Analysis | Multivariable Analysis | |||||
|---|---|---|---|---|---|---|
| Variables | OR | 95% CI | p Value | OR | 95% CI | p Value |
| Age ≥ 67 years at diagnosis | 1.33 | 0.39–4.72 | 0.646 | |||
| Sex | ||||||
| Male | Reference | |||||
| Female | 0.56 | 0.15–1.90 | 0.359 | |||
| Affected part of the stomach | ||||||
| Diffuse | Reference | Reference | ||||
| Segmental | 3.34 | 0.97–12.8 | 0.063 | 0.43 | 0.01–17.6 | 0.642 |
| Ulcerations | ||||||
| Yes | Reference | Reference | ||||
| No | 30.33 | 5.17–582.9 | 0.002 | 30.13 | 4.72–666.0 | 0.003 |
| Serum CEA | ||||||
| ≤5 | Reference | |||||
| >5 | 1.67 | 0.43–6.11 | 0.443 | |||
| Number of biopsies | ||||||
| <6 | Reference | |||||
| ≥6 | 3.14 | 0.83–15.5 | 0.115 | |||
| Saint Louis linitis score | ||||||
| ≥5 | Reference | Reference | ||||
| <5 | 3.75 | 1.06–15.64 | 0.049 | 6.30 | 0.15–306.6 | 0.316 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takada, R.; Minaga, K.; Hara, A.; Otsuka, Y.; Omoto, S.; Kamata, K.; Yamao, K.; Takenaka, M.; Hagiwara, S.; Honjo, H.; et al. Diagnostic Value of EUS-Guided Fine-Needle Aspiration Biopsy for Gastric Linitis Plastica with Negative Endoscopic Biopsy. J. Clin. Med. 2021, 10, 3716. https://doi.org/10.3390/jcm10163716
Takada R, Minaga K, Hara A, Otsuka Y, Omoto S, Kamata K, Yamao K, Takenaka M, Hagiwara S, Honjo H, et al. Diagnostic Value of EUS-Guided Fine-Needle Aspiration Biopsy for Gastric Linitis Plastica with Negative Endoscopic Biopsy. Journal of Clinical Medicine. 2021; 10(16):3716. https://doi.org/10.3390/jcm10163716
Chicago/Turabian StyleTakada, Ryutaro, Kosuke Minaga, Akane Hara, Yasuo Otsuka, Shunsuke Omoto, Ken Kamata, Kentaro Yamao, Mamoru Takenaka, Satoru Hagiwara, Hajime Honjo, and et al. 2021. "Diagnostic Value of EUS-Guided Fine-Needle Aspiration Biopsy for Gastric Linitis Plastica with Negative Endoscopic Biopsy" Journal of Clinical Medicine 10, no. 16: 3716. https://doi.org/10.3390/jcm10163716
APA StyleTakada, R., Minaga, K., Hara, A., Otsuka, Y., Omoto, S., Kamata, K., Yamao, K., Takenaka, M., Hagiwara, S., Honjo, H., Matsui, S., Chikugo, T., Watanabe, T., & Kudo, M. (2021). Diagnostic Value of EUS-Guided Fine-Needle Aspiration Biopsy for Gastric Linitis Plastica with Negative Endoscopic Biopsy. Journal of Clinical Medicine, 10(16), 3716. https://doi.org/10.3390/jcm10163716