
Thirty-Day Readmission Rates after Takotsubo Syndrome with or without Malignancy: A Nationwide Readmissions Database Analysis

 , ,
, ,
Abstract
1. Introduction
2. Methods
2.1. Data Source
2.2. Study Population and Variables
2.3. Study Outcomes
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
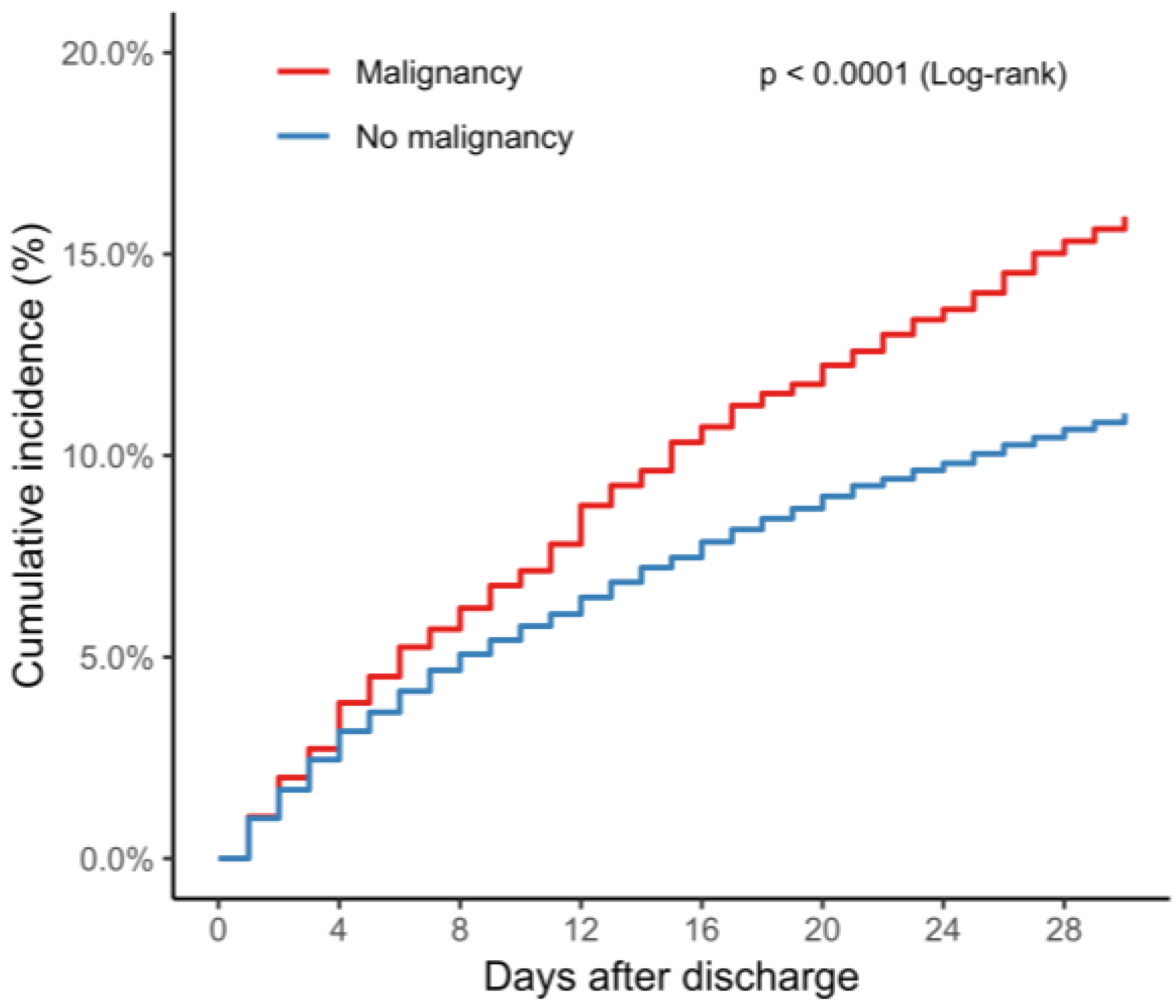
3.2. Clinical Outcomes of TTS Patients with or without Malignancy
3.3. Timing and Cause of Readmission
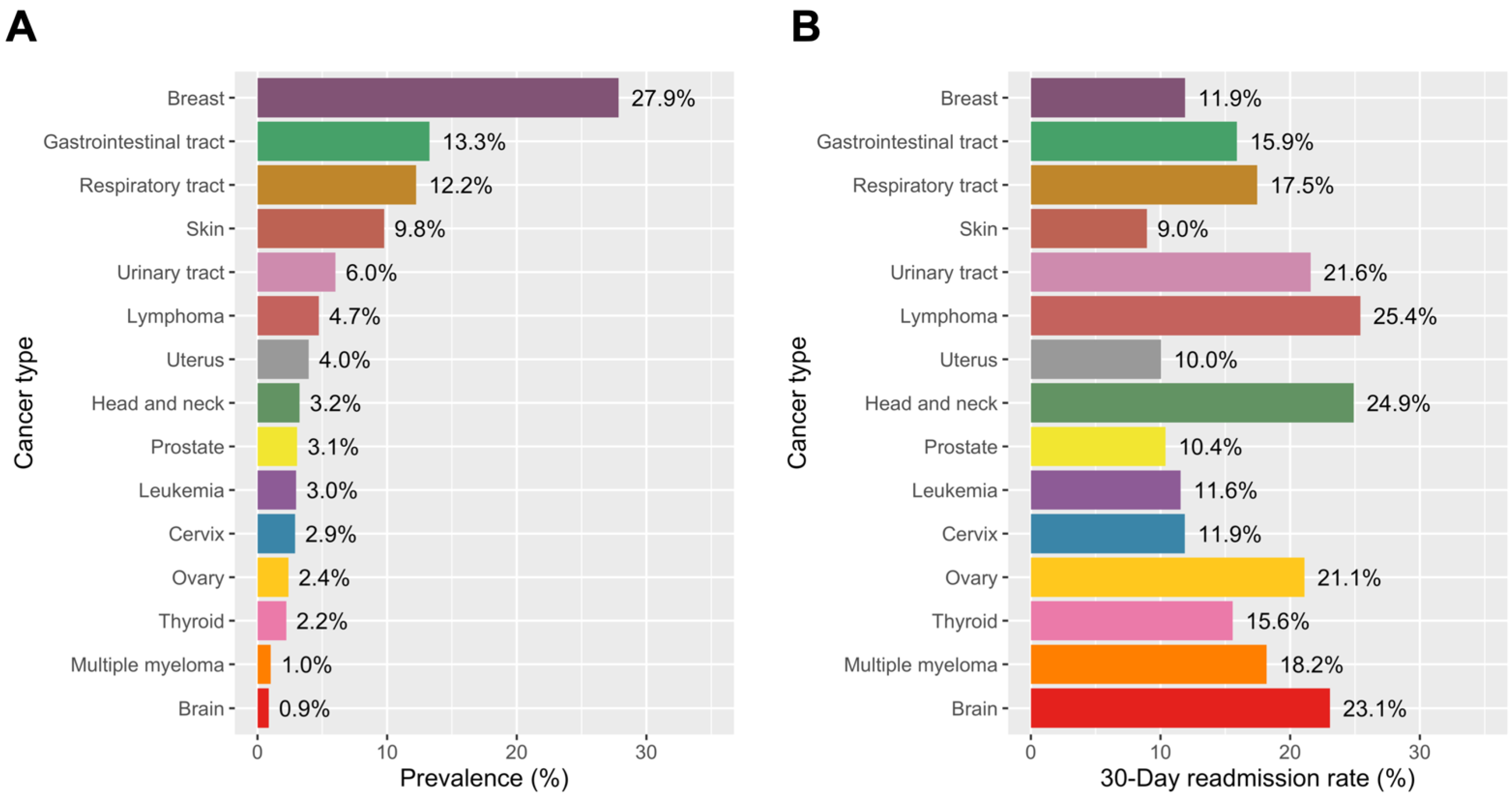
3.4. Specific Cancer Type and Readmission
3.5. Total Charges and Costs by the Presence of Malignancy and Predictors of Total Cost
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akashi, Y.J.; Goldstein, D.S.; Barbaro, G.; Ueyama, T. Takotsubo cardiomyopathy: A new form of acute, reversible heart failure. Circulation 2008, 118, 2754–2762. [Google Scholar] [CrossRef]
- Ghadri, J.R.; Wittstein, I.S.; Prasad, A.; Sharkey, S.; Dote, K.; Akashi, Y.J.; Cammann, V.L.; Crea, F.; Galiuto, L.; Desmet, W.; et al. International expert consensus document on takotsubo syndrome (part i): Clinical characteristics, diagnostic criteria, and pathophysiology. Eur. Heart J. 2018, 39, 2032–2046. [Google Scholar] [CrossRef]
- Ghadri, J.R.; Ruschitzka, F.; Luscher, T.F.; Templin, C. Takotsubo cardiomyopathy: Still much more to learn. Heart 2014, 100, 1804–1812. [Google Scholar] [CrossRef]
- Templin, C.; Ghadri, J.R.; Diekmann, J.; Napp, L.C.; Bataiosu, D.R.; Jaguszewski, M.; Cammann, V.L.; Sarcon, A.; Geyer, V.; Neumann, C.A.; et al. Clinical features and outcomes of takotsubo (stress) cardiomyopathy. N. Engl. J. Med. 2015, 373, 929–938. [Google Scholar] [CrossRef]
- Ghadri, J.R.; Kato, K.; Cammann, V.L.; Gili, S.; Jurisic, S.; Di Vece, D.; Candreva, A.; Ding, K.J.; Micek, J.; Szawan, K.A.; et al. Long-term prognosis of patients with takotsubo syndrome. J. Am. Coll. Cardiol. 2018, 72, 874–882. [Google Scholar] [CrossRef] [PubMed]
- Fingar, K.; Washington, R. Trends in Hospital Readmissions for Four High-Volume Conditions, 2009–2013. HCUP Statistical Brief # 196. Published November 2015. Available online: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb196-Readmissions-Trends-High-Volume-Conditions.pdf. (accessed on 11 September 2019).
- Smilowitz, N.R.; Hausvater, A.; Reynolds, H.R. Hospital readmission following takotsubo syndrome. Eur. Heart J. Qual Care Clin. Outcomes 2019, 5, 114–120. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, E.; Saliba, A.; McKenzie, K. Subjective wellbeing in the Indian general population: A validation study of the personal wellbeing index. Qual Life Res. 2020, 29, 1073–1081. [Google Scholar] [CrossRef]
- Agency for Healthcare Research and Quality. Overview of hospital stays in the United States. 2012. Available online: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb180-Hospitalizations-United-States-2012.pdf (accessed on 1 May 2021).
- Rivera, D.R.; Gallicchio, L.; Brown, J.; Liu, B.; Kyriacou, D.N.; Shelburne, N. Trends in adult cancer-related emergency department utilization: An analysis of data from the nationwide emergency department sample. JAMA Oncol. 2017, 3, e172450. [Google Scholar] [CrossRef] [PubMed]
- Kim, L.K.; Yeo, I.; Cheung, J.W.; Swaminathan, R.V.; Wong, S.C.; Charitakis, K.; Adejumo, O.; Chae, J.; Minutello, R.M.; Bergman, G.; et al. Thirty-Day readmission rates, timing, causes, and costs after st-segment-elevation myocardial infarction in the United States: A national readmission database analysis 2010-2014. J. Am. Heart Assoc. 2018, 7, e009863. [Google Scholar] [CrossRef] [PubMed]
- Cheng, E.P.; Liu, C.F.; Yeo, I.; Markowitz, S.M.; Thomas, G.; Ip, J.E.; Kim, L.K.; Lerman, B.B.; Cheung, J.W. Risk of mortality following catheter ablation of atrial fibrillation. J. Am. Coll. Cardiol. 2019, 74, 2254–2264. [Google Scholar] [CrossRef] [PubMed]
- Cheung, J.W.; Cheng, E.P.; Wu, X.; Yeo, I.; Christos, P.J.; Kamel, H.; Markowitz, S.M.; Liu, C.F.; Thomas, G.; Ip, J.E.; et al. Sex-based differences in outcomes, 30-day readmissions, and costs following catheter ablation of atrial fibrillation: The United States Nationwide Readmissions Database 2010-14. Eur. Heart J. 2019, 40, 3035–3043. [Google Scholar] [CrossRef] [PubMed]
- Agency for Healthcare Research and Quality. Introduction to the HCUP Nationwide Readmissions Database (NRD). Available online: https://www.hcupus.ahrq.gov/db/nation/nrd/Introduction_NRD_2010-2014.pdf (accessed on 1 September 2019).
- Lohr, S.L. Sampling: Design and Analysis; Duxbury Press: Pacific Grove, CA, USA, 1999. [Google Scholar]
- Shah, M.; Ram, P.; Lo, K.B.U.; Sirinvaravong, N.; Patel, B.; Tripathi, B.; Patil, S.; Figueredo, V.M. Etiologies, predictors, and economic impact of readmission within 1 month among patients with takotsubo cardiomyopathy. Clin. Cardiol. 2018, 41, 916–923. [Google Scholar] [CrossRef]
- Arora, S.; Patel, P.; Lahewala, S.; Patel, N.; Patel, N.J.; Thakore, K.; Amin, A.; Tripathi, B.; Kumar, V.; Shah, H.; et al. Etiologies, trends, and predictors of 30-day readmission in patients with heart failure. Am. J. Cardiol. 2017, 119, 760–769. [Google Scholar] [CrossRef] [PubMed]
- Leppin, A.L.; Gionfriddo, M.R.; Kessler, M.; Brito, J.P.; Mair, F.S.; Gallacher, K.; Wang, Z.; Erwin, P.J.; Sylvester, T.; Boehmer, K.; et al. Preventing 30-day hospital readmissions: A systematic review and meta-analysis of randomized trials. JAMA Intern. Med. 2014, 174, 1095–1107. [Google Scholar] [CrossRef] [PubMed]
- Stromberg, A.; Martensson, J.; Fridlund, B.; Levin, L.A.; Karlsson, J.E.; Dahlstrom, U. Nurse-led heart failure clinics improve survival and self-care behaviour in patients with heart failure: Results from a prospective, randomised trial. Eur. Heart J. 2003, 24, 1014–1023. [Google Scholar] [CrossRef]
- Wakefield, B.J.; Ward, M.M.; Holman, J.E.; Ray, A.; Scherubel, M.; Burns, T.L.; Kienzle, M.G.; Rosenthal, G.E. Evaluation of home telehealth following hospitalization for heart failure: A randomized trial. Telemed J. E Health 2008, 14, 753–761. [Google Scholar] [CrossRef]
- Linne, A.B.; Liedholm, H. Effects of an interactive CD-program on 6 months readmission rate in patients with heart failure—A randomised, controlled trial [NCT00311194]. BMC Cardiovasc. Disord. 2006, 6, 30. [Google Scholar] [CrossRef]
- Rich, M.W.; Beckham, V.; Wittenberg, C.; Leven, C.L.; Freedland, K.E.; Carney, R.M. A multidisciplinary intervention to prevent the readmission of elderly patients with congestive heart failure. N. Engl. J. Med. 1995, 333, 1190–1195. [Google Scholar] [CrossRef] [PubMed]
- Coleman, E.A.; Parry, C.; Chalmers, S.; Min, S.J. The care transitions intervention: Results of a randomized controlled trial. Arch. Intern. Med. 2006, 166, 1822–1828. [Google Scholar] [CrossRef] [PubMed]
- Vento, S.; Cainelli, F. Infections in patients with cancer undergoing chemotherapy: Aetiology, prevention, and treatment. Lancet Oncol. 2003, 4, 595–604. [Google Scholar] [CrossRef]
- Elesber, A.A.; Prasad, A.; Lennon, R.J.; Wright, R.S.; Lerman, A.; Rihal, C.S. Four-year recurrence rate and prognosis of the apical ballooning syndrome. J. Am. Coll. Cardiol. 2007, 50, 448–452. [Google Scholar] [CrossRef]
- Singh, K.; Carson, K.; Usmani, Z.; Sawhney, G.; Shah, R.; Horowitz, J. Systematic review and meta-analysis of incidence and correlates of recurrence of takotsubo cardiomyopathy. Int. J. Cardiol. 2014, 174, 696–701. [Google Scholar] [CrossRef] [PubMed]
- Gianni, M.; Dentali, F.; Grandi, A.M.; Sumner, G.; Hiralal, R.; Lonn, E. Apical ballooning syndrome or takotsubo cardiomyopathy: A systematic review. Eur. Heart J. 2006, 27, 1523–1529. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Santoro, F.; Stiermaier, T.; Moller, C.; Guastafierro, F.; Novo, G.; Novo, S.; Mariano, E.; Romeo, F.; Romeo, F.; et al. Incidence and clinical impact of recurrent takotsubo syndrome: Results from the GEIST registry. J. Am. Heart Assoc. 2019, 8, e010753. [Google Scholar] [CrossRef] [PubMed]
- Cammann, V.L.; Sarcon, A.; Ding, K.J.; Seifert, B.; Kato, K.; Di Vece, D.; Szawan, K.A.; Gili, S.; Jurisic, S.; Bacchi, B.; et al. Clinical features and outcomes of patients with malignancy and takotsubo syndrome: Observations from the international takotsubo registry. J. Am. Heart Assoc. 2019, 8, e010881. [Google Scholar] [CrossRef]
- Desai, A.; Noor, A.; Joshi, S.; Kim, A.S. Takotsubo cardiomyopathy in cancer patients. Cardiooncology 2019, 5, 7. [Google Scholar] [CrossRef]
- Tornvall, P.; Collste, O.; Ehrenborg, E.; Jarnbert-Petterson, H. A case-control study of risk markers and mortality in takotsubo stress cardiomyopathy. J. Am. Coll. Cardiol. 2016, 67, 1931–1936. [Google Scholar] [CrossRef]
- Curigliano, G.; Cardinale, D.; Dent, S.; Criscitiello, C.; Aseyev, O.; Lenihan, D.; Cipolla, C.M. Cardiotoxicity of anticancer treatments: Epidemiology, detection, and management. CA Cancer J. Clin. 2016, 66, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Ewer, M.S.; Ewer, S.M. Cardiotoxicity of anticancer treatments. Nat. Rev. Cardiol. 2015, 12, 620. [Google Scholar] [CrossRef] [PubMed]
- Desai, R.; Abbas, S.A.; Goyal, H.; Durairaj, A.; Fong, H.K.; Hung, O.; Sachdeva, R.; Barac, A.; Yusuf, S.W.; Kumar, G. Frequency of takotsubo cardiomyopathy in adult patients receiving chemotherapy (from a 5-year nationwide inpatient study). Am. J. Cardiol. 2019, 123, 667–673. [Google Scholar] [CrossRef]
- Ederhy, S.; Cautela, J.; Ancedy, Y.; Escudier, M.; Thuny, F.; Cohen, A. Takotsubo-like syndrome in cancer patients treated with immune checkpoint inhibitors. JACC Cardiovasc. Imaging 2018, 11, 1187–1190. [Google Scholar] [CrossRef] [PubMed]
- Anderson, R.D.; Brooks, M. Apical takotsubo syndrome in a patient with metastatic breast carcinoma on novel immunotherapy. Int. J. Cardiol. 2016, 222, 760–761. [Google Scholar] [CrossRef] [PubMed]
- Joy, P.S.; Guddati, A.K.; Shapira, I. Outcomes of takotsubo cardiomyopathy in hospitalized cancer patients. J. Cancer Res. Clin. Oncol. 2018, 144, 1539–1545. [Google Scholar] [CrossRef] [PubMed]
- Dharmarajan, K.; Wang, Y.; Lin, Z.; Normand, S.T.; Ross, J.S.; Horwitz, L.I.; Desai, N.R.; Suter, L.G.; Drye, E.E.; Bernheim, S.M.; et al. Association of changing hospital readmission rates with mortality rates after hospital discharge. JAMA 2017, 318, 270–278. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | ||||
|---|---|---|---|---|
| All | Malignancy | No Malignancy | p Value | |
| Number of admissions | 61,583 | 7542 (12.2) * | 54,041 (87.8) | |
| Patient characteristics | ||||
| Age, mean (SE), y | 66.7 (0.1) | 70.6 (0.2) | 66.1 (0.1) | <0.001 † |
| Age ≥ 70 yrs | 27,109 (44.0) | 4328 (57.4) | 22,781 (42.2) | <0.001 ‡ |
| Female | 54,708 (88.8) | 6499 (86.2) | 48,209 (89.2) | <0.001 |
| Smoking history | 21,834 (35.5) | 2864 (38.0) | 18,970 (35.1) | 0.005 |
| Hypertension | 40,597 (65.9) | 4900 (65.0) | 35,697 (66.1) | 0.350 |
| Diabetes mellitus | 11,701 (19.0) | 1405 (18.6) | 10,296 (19.1) | 0.620 |
| Dyslipidemia | 26,830 (43.6) | 3102 (41.1) | 23,728 (43.9) | 0.014 |
| Known coronary artery disease | 25,910 (42.1) | 3495 (46.3) | 22,415 (41.5) | <0.001 |
| Previous myocardial infarction | 3833 (6.2) | 444 (5.9) | 3389 (6.3) | 0.463 |
| Previous PCI | 2988 (4.9) | 341 (4.5) | 2647 (4.9) | 0.458 |
| Previous CABG | 933 (1.5) | 91 (1.2) | 842 (1.6) | 0.177 |
| Family history of coronary artery disease | 5249 (8.5) | 448 (5.9) | 4801 (8.9) | <0.001 |
| Congestive heart failure | 18,531 (30.1) | 2552 (33.8) | 15,979 (29.6) | <0.001 |
| Peripheral vascular disease | 4544 (7.4) | 608 (8.1) | 3936 (7.3) | 0.156 |
| Chronic pulmonary disease | 17,732 (28.8) | 2396 (31.8) | 15,336 (28.4) | <0.001 |
| Chronic kidney disease | 4862 (7.9) | 670 (8.9) | 4192 (7.8) | 0.075 |
| Liver disease | 1238 (2.0) | 116 (1.5) | 1122 (2.1) | 0.070 |
| Anemia | 9425 (15.3) | 1456 (19.3) | 7969 (14.7) | <0.001 |
| Atrial fibrillation | 8744 (14.2) | 1338 (17.7) | 7406 (13.7) | <0.001 |
| Coagulopathy | 2699 (4.4) | 485 (6.4) | 2214 (4.1) | <0.001 |
| Collagen vascular disease | 2683 (4.4) | 282 (3.7) | 2401 (4.4) | 0.117 |
| Fluid/electrolyte disorders | 18,576 (30.2) | 2658 (35.2) | 15,918 (29.5) | <0.001 |
| Obesity | 6554 (10.6) | 537 (7.1) | 6017 (11.1) | <0.001 |
| Other neurological disorders | 5196 (8.4) | 599 (7.9) | 4597 (8.5) | 0.429 |
| Pulmonary circulatory disease | 1243 (2.0) | 252 (3.3) | 991 (1.8) | <0.001 |
| Valvular heart disease | 1592 (2.6) | 296 (3.9) | 1296 (2.4) | <0.001 |
| Median household income | <0.001 | |||
| First quartile | 16,024 (26.4) | 1739 (23.3) | 14,285 (26.8) | |
| Second quartile | 15,865 (26.1) | 1957 (26.2) | 13,908 (26.1) | |
| Third quartile | 14,949 (24.6) | 1816 (24.3) | 13,133 (24.7) | |
| Fourth quartile | 13,849 (22.8) | 1953 (26.2) | 11,896 (22.4) | |
| Primary payer | <0.001 | |||
| Medicare | 37,851 (61.5) | 5462 (72.4) | 32,389 (59.9) | |
| Medicaid | 4028 (6.5) | 389 (5.2) | 3639 (6.7) | |
| Private including HMO | 15,388 (25.0) | 1435 (19.0) | 13,953 (25.8) | |
| Self-pay/no charge/other | 4315 (7.0) | 256 (3.4) | 4059 (7.5) | |
| Hospital characteristics | ||||
| Hospital teaching status | <0.001 | |||
| Teaching | 35,931 (58.3) | 4799 (63.6) | 31,132 (57.6) | |
| Nonteaching | 25,652 (41.7) | 2743 (36.4) | 22,909 (42.4) | |
| Hospital location | 0.149 | |||
| Rural | 212 (0.3) | 13 (0.2) | 199 (0.4) | |
| Urban | 61,371 (99.7) | 7529 (99.8) | 53,842 (99.6) | |
| Hospital bed size | 0.240 | |||
| Small | 4612 (7.5) | 503 (6.7) | 4109 (7.6) | |
| Medium | 13,769 (22.4) | 1643 (21.8) | 12,126 (22.4) | |
| Large | 43,203 (70.2) | 5396 (71.5) | 37,807 (70.0) | |
| Length of stay > 5 days | 18,588 (30.2 | 3134 (41.6) | 15,454(28.6) | <0.001 |
| Disposition | <0.001 | |||
| Home | 44,092 (71.6) | 4552 (60.4) | 39,540 (73.2) | |
| Facility § | 15,710 (25.5) | 2632 (34.9) | 13,078 (24.2) | |
| AMA/unknown | 1777 (2.9) | 358 (4.7) | 1419 (2.6) | |
| Mood disorders | 11,502 (18.7) | 11,354 (18.0) | 10,148 (18.8) | 0.378 |
| Substance abuse | 2676 (4.3) | 165 (2.2) | 2511 (4.6) | <0.001 |
| Delirium/Dementia | 2667 (4.3) | 365 (4.8) | 2302 (4.3) | 0.213 |
| Personality disorder | 103 (0.2) | 0 (0) | 103 (0.2) | 0.061 |
| Acute decompensated heart failure | 10,571 (17.2) | 1472 (19.5) | 9099 (16.8) | 0.003 |
| Cardiogenic shock | 3564 (5.8) | 582 (7.7) | 2982 (5.5) | <0.001 |
| Cardiac arrest | 1663 (2.7) | 221 (2.9) | 1442 (2.7) | 0.544 |
| Postop stroke (complication) | 792 (1.3) | 103 (1.4) | 689 (1.3) | 0.704 |
| Arrhythmia | 16,868 (27.4) | 2394 (31.7) | 14,474 (26.8) | <0.001 |
| Unadjusted | Adjusted * | ||||
|---|---|---|---|---|---|
| Outcomes | N (%) | OR (95% CI) | p Value | OR (95% CI) | p Value |
| Number of patients | 7542 (12.2) | ||||
| Inhospital mortality | |||||
| Overall | 1472 (2.4) | ||||
| No malignancy | 1161 (2.1) | 1 (Ref) | 1 (Ref) | ||
| Malignancy | 311 (4.1) | 1.96 (1.56–2.46) | <0.001 | 1.68 (1.29–2.17) | <0.001 |
| 30-day readmission mortality | |||||
| Overall | 254 (0.4) | ||||
| No malignancy | 205 (0.4) | 1 (Ref) | |||
| Malignancy | 49 (0.6) | 1.73 (0.88–3.42) | 0.114 | - | |
| 30-day total mortality † | |||||
| Overall | 1726 (2.8) | ||||
| No malignancy | 1366 (2.5) | 1 (Ref) | 1 (Ref) | ||
| Malignancy | 360 (4.8) | 1.96 (1.56–2.46) | <0.001 | 1.62 (1.25–2.10) | <0.001 |
| 30-day readmission | |||||
| Overall | 7173 (11.6) | ||||
| No malignancy | 5971 (11.0) | 1 (Ref) | 1 (Ref) | ||
| Malignancy | 1202 (15.9) | 1.53 (1.34–1.75) | <0.001 | 1.33 (1.15–1.53) | <0.001 |
| Variables | Unadjusted OR | Lower CI | Higher CI | p Value | Adjusted OR * | Lower CI | Higher CI | p Value |
|---|---|---|---|---|---|---|---|---|
| Malignancy | 1.53 | 1.34 | 1.75 | <0.001 | 1.33 | 1.15 | 1.53 | <0.001 |
| Length of stay > 5 days | 2.45 | 2.23 | 2.69 | <0.001 | 1.48 | 1.31 | 1.68 | <0.001 |
| Age ≥ 70 yrs | 1.34 | 1.22 | 1.46 | <0.001 | 0.95 | 0.84 | 1.07 | 0.378 |
| Diabetes mellitus | 1.27 | 1.13 | 1.42 | <0.001 | 1.14 | 1.01 | 1.28 | 0.035 |
| Family hx of CAD | 0.56 | 0.46 | 0.69 | <0.001 | 0.78 | 0.63 | 0.97 | 0.024 |
| Chronic pulmonary disease | 1.69 | 1.54 | 1.86 | <0.001 | 1.40 | 1.27 | 1.55 | <0.001 |
| Chronic Kidney disease | 1.88 | 1.64 | 2.16 | <0.001 | 1.36 | 1.17 | 1.59 | <0.001 |
| Anemia | 1.90 | 1.70 | 2.12 | <0.001 | 1.26 | 1.12 | 1.42 | <0.001 |
| Atrial fibrillation | 1.61 | 1.43 | 1.81 | <0.001 | 1.24 | 1.08 | 1.41 | 0.002 |
| Fluid and electrolyte disturbance | 1.75 | 1.58 | 1.92 | <0.001 | 1.20 | 1.07 | 1.34 | 0.001 |
| Median household income (Ref: 1st quartile) | ||||||||
| Second quartile | 0.92 | 0.80 | 1.04 | 0.188 | 0.97 | 0.85 | 1.11 | 0.689 |
| Third quartile | 0.83 | 0.72 | 0.94 | 0.004 | 0.90 | 0.79 | 1.03 | 0.10 |
| Fourth quartile | 0.75 | 0.66 | 0.85 | <0.001 | 0.85 | 0.74 | 0.97 | 0.01 |
| Primary payer (Ref: Medicare) | ||||||||
| Medicaid | 1.11 | 0.93 | 1.31 | 0.250 | 1.25 | 1.02 | 1.53 | 0.032 |
| Private including HMO | 0.53 | 0.46 | 0.60 | <0.001 | 0.75 | 0.64 | 0.88 | <0.001 |
| Self-pay/no charge/other | 0.61 | 0.50 | 0.74 | <0.001 | 0.82 | 0.66 | 1.00 | 0.054 |
| Disposition (Ref: Home) | ||||||||
| Facility | 2.60 | 2.35 | 2.87 | <0.001 | 1.65 | 1.46 | 1.87 | <0.001 |
| AMA/unknown | 0.37 | 0.22 | 0.62 | <0.001 | 0.25 | 0.15 | 0.41 | <0.001 |
| Unadjusted | Adjusted * | |||||||
|---|---|---|---|---|---|---|---|---|
| Variables | Beta | Lower CI | Higher CI | p Value | Beta | Lower CI | Higher CI | p Value |
| Malignancy | 0.093 | 0.078 | 0.108 | <0.001 | 0.013 | 0.005 | 0.022 | 0.003 |
| 30-day readmission | 0.327 | 0.312 | 0.341 | <0.001 | 0.223 | 0.212 | 0.234 | <0.001 |
| Length of stay > 5 days | 0.459 | 0.449 | 0.469 | <0.001 | 0.31 | 0.301 | 0.318 | <0.001 |
| Age ≥ 70 yrs | 0.033 | 0.023 | 0.042 | <0.001 | −0.026 | −0.033 | −0.018 | <0.001 |
| Female (Ref: male) | −0.109 | −0.130 | −0.089 | <0.001 | −0.048 | −0.061 | −0.036 | <0.001 |
| Diabetes mellitus | 0.041 | 0.029 | 0.052 | <0.001 | 0.015 | 0.007 | 0.022 | <0.001 |
| Dyslipidemia | −0.070 | −0.080 | −0.061 | <0.001 | −0.014 | −0.02 | −0.008 | <0.001 |
| Previous PCI | −0.024 | −0.043 | −0.005 | 0.015 | −0.02 | −0.034 | −0.006 | 0.005 |
| Family history of CAD | −0.125 | −0.138 | −0.112 | <0.001 | −0.013 | −0.024 | −0.003 | 0.009 |
| Congestive heart failure | 0.184 | 0.173 | 0.194 | <0.001 | 0.027 | 0.019 | 0.034 | <0.001 |
| Peripheral vascular disease | 0.121 | 0.102 | 0..139 | <0.001 | 0.028 | 0.016 | 0.04 | <0.001 |
| Chronic pulmonary disease | 0.107 | 0.096 | 0.118 | <0.001 | 0.019 | 0.012 | 0.026 | <0.001 |
| Chronic kidney disease | 0.169 | 0.150 | 0.188 | <0.001 | 0.03 | 0.017 | 0.044 | <0.001 |
| Chronic liver disease | 0.200 | 0.157 | 0.242 | <0.001 | 0.04 | 0.012 | 0.068 | 0.005 |
| Anemia | 0.217 | 0.203 | 0.231 | <0.001 | 0.031 | 0.022 | 0.041 | <0.001 |
| Atrial fibrillation | 0.140 | 0.124 | 0.156 | <0.001 | 0.018 | 0.008 | 0.028 | <0.001 |
| Coagulopathy | 0.339 | 0.309 | 0.368 | <0.001 | 0.097 | 0.078 | 0.115 | <0.001 |
| Drug abuse | 0.114 | 0.089 | 0.140 | <0.001 | 0.027 | 0.01 | 0.043 | 0.001 |
| Fluid/electrolyte disorders | 0.257 | 0.246 | 0.269 | <0.001 | 0.059 | 0.051 | 0.068 | <0.001 |
| Other neurological disorders | 0.132 | 0.112 | 0.152 | <0.001 | 0.027 | 0.014 | 0.04 | <0.001 |
| Pulmonary circulatory disease | 0.407 | 0.369 | 0.444 | <0.001 | 0.096 | 0.065 | 0.127 | <0.001 |
| Valvular heart disease | 0.323 | 0.293 | 0.353 | <0.001 | 0.06 | 0.038 | 0.083 | <0.001 |
| Cardiogenic shock | 0.418 | 0.396 | 0.440 | <0.001 | 0.122 | 0.102 | 0.142 | <0.001 |
| Cardiac arrest | 0.403 | 0.372 | 0.434 | <0.001 | 0.147 | 0.122 | 0.173 | <0.001 |
| Intraaortic balloon pump | 0.415 | 0.383 | 0.448 | <0.001 | 0.086 | 0.058 | 0.114 | <0.001 |
| Median household income (Ref: first quartile) | ||||||||
| Second quartile | 0.007 | −0.008 | 0.023 | 0.339 | 0.027 | 0.018 | 0.036 | <0.001 |
| Third quartile | 0.025 | 0.010 | 0.040 | 0.001 | 0.051 | 0.042 | 0.061 | <0.001 |
| Fourth quartile | 0.037 | 0.022 | 0.053 | <0.001 | 0.077 | 0.067 | 0.088 | <0.001 |
| Primary payer (Ref: medicare) | ||||||||
| Medicaid | 0.041 | 0.020 | 0.062 | <0.001 | 0.033 | 0.019 | 0.047 | <0.001 |
| Private | −0.083 | −0.094 | −0.072 | <0.001 | −0.003 | −0.011 | 0.006 | 0.506 |
| Self-pay/no charge/others | −0.069 | −0.087 | −0.050 | <0.001 | −0.001 | −0.014 | 0.012 | 0.897 |
| Disposition (Ref: home) | ||||||||
| Facility | 0.316 | 0.304 | 0.327 | <0.001 | 0.077 | 0.069 | 0.086 | <0.001 |
| AMA/unknown | 0.346 | 0.311 | 0.380 | <0.001 | 0.116 | 0.091 | 0.141 | <0.001 |
| Year (per year) | 0.009 | 0.004 | 0.014 | <0.001 | 0.006 | −0.000 | 0.011 | 0.060 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, S.-J.; Yeo, I.; Jonas, C.; Goyal, P.; Cheung, J.W.; Feldman, D.N.; McCullough, S.A.; Krishnan, U.; Narotsky, D.L.; Singh, H.S.; et al. Thirty-Day Readmission Rates after Takotsubo Syndrome with or without Malignancy: A Nationwide Readmissions Database Analysis. J. Clin. Med. 2021, 10, 3701. https://doi.org/10.3390/jcm10163701
Jang S-J, Yeo I, Jonas C, Goyal P, Cheung JW, Feldman DN, McCullough SA, Krishnan U, Narotsky DL, Singh HS, et al. Thirty-Day Readmission Rates after Takotsubo Syndrome with or without Malignancy: A Nationwide Readmissions Database Analysis. Journal of Clinical Medicine. 2021; 10(16):3701. https://doi.org/10.3390/jcm10163701
Chicago/Turabian StyleJang, Sun-Joo, Ilhwan Yeo, Chanel Jonas, Parag Goyal, Jim W. Cheung, Dmitriy N. Feldman, S. Andrew McCullough, Udhay Krishnan, David L. Narotsky, Harsimran S. Singh, and et al. 2021. "Thirty-Day Readmission Rates after Takotsubo Syndrome with or without Malignancy: A Nationwide Readmissions Database Analysis" Journal of Clinical Medicine 10, no. 16: 3701. https://doi.org/10.3390/jcm10163701
APA StyleJang, S.-J., Yeo, I., Jonas, C., Goyal, P., Cheung, J. W., Feldman, D. N., McCullough, S. A., Krishnan, U., Narotsky, D. L., Singh, H. S., Minutello, R. M., Bergman, G., Wong, S. C., & Kim, L. K. (2021). Thirty-Day Readmission Rates after Takotsubo Syndrome with or without Malignancy: A Nationwide Readmissions Database Analysis. Journal of Clinical Medicine, 10(16), 3701. https://doi.org/10.3390/jcm10163701