
Immunomodulatory Effect of Withania somnifera (Ashwagandha) Extract—A Randomized, Double-Blind, Placebo Controlled Trial with an Open Label Extension on Healthy Participants

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
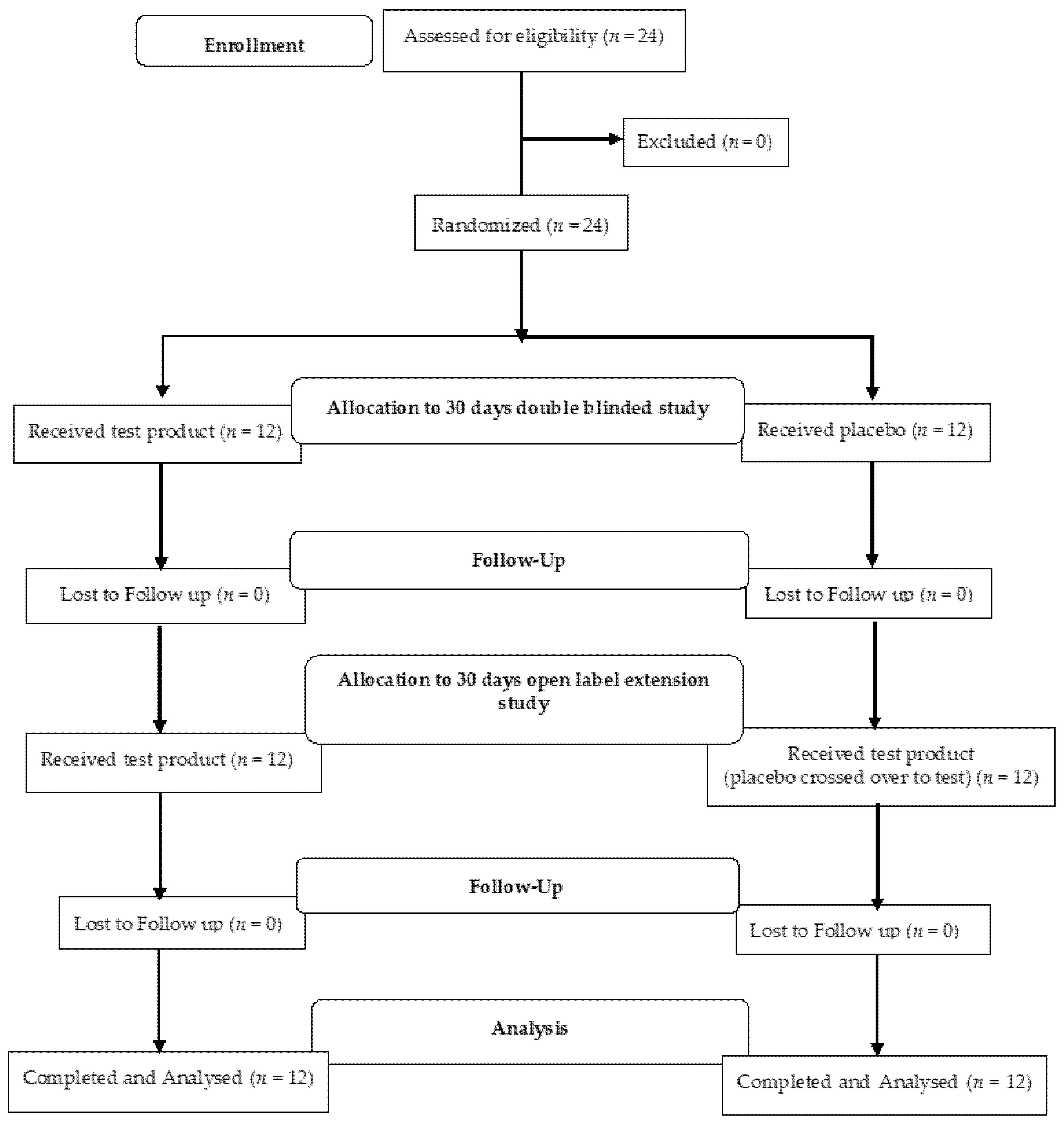
2.1. Study Design
2.2. Subjects and Inclusion/Exclusion Criteria
2.3. Intervention and Dosing
2.4. Randomization, Blinding and Unblinding
2.5. Outcome Assessments
2.5.1. Immunoglobulin Assay (IgG, IgM, IgA)
2.5.2. Cytokines Assay
2.5.3. TBNK Assay
2.6. Biochemical and Safety Analysis
2.7. Statistical Analysis
3. Results
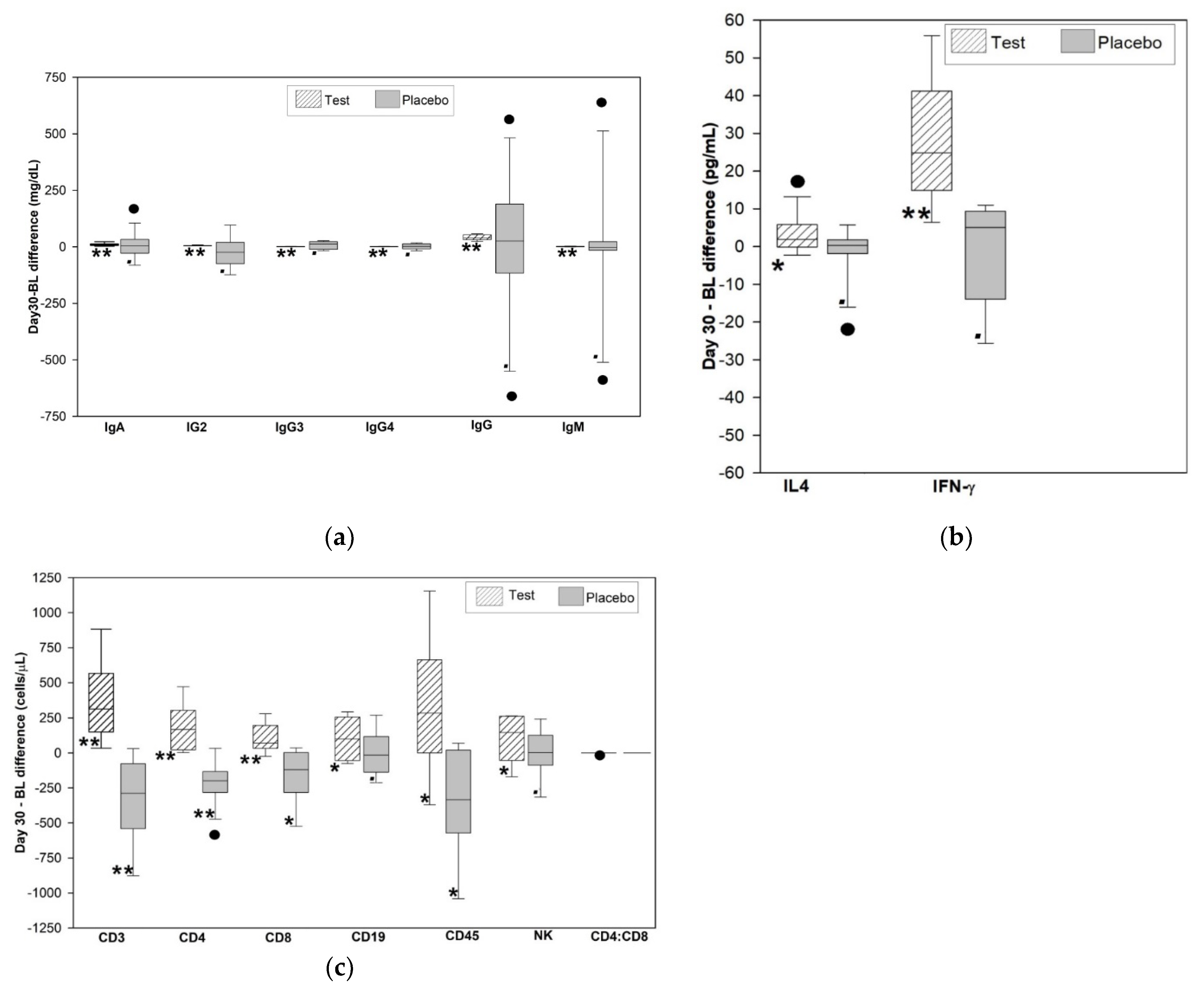
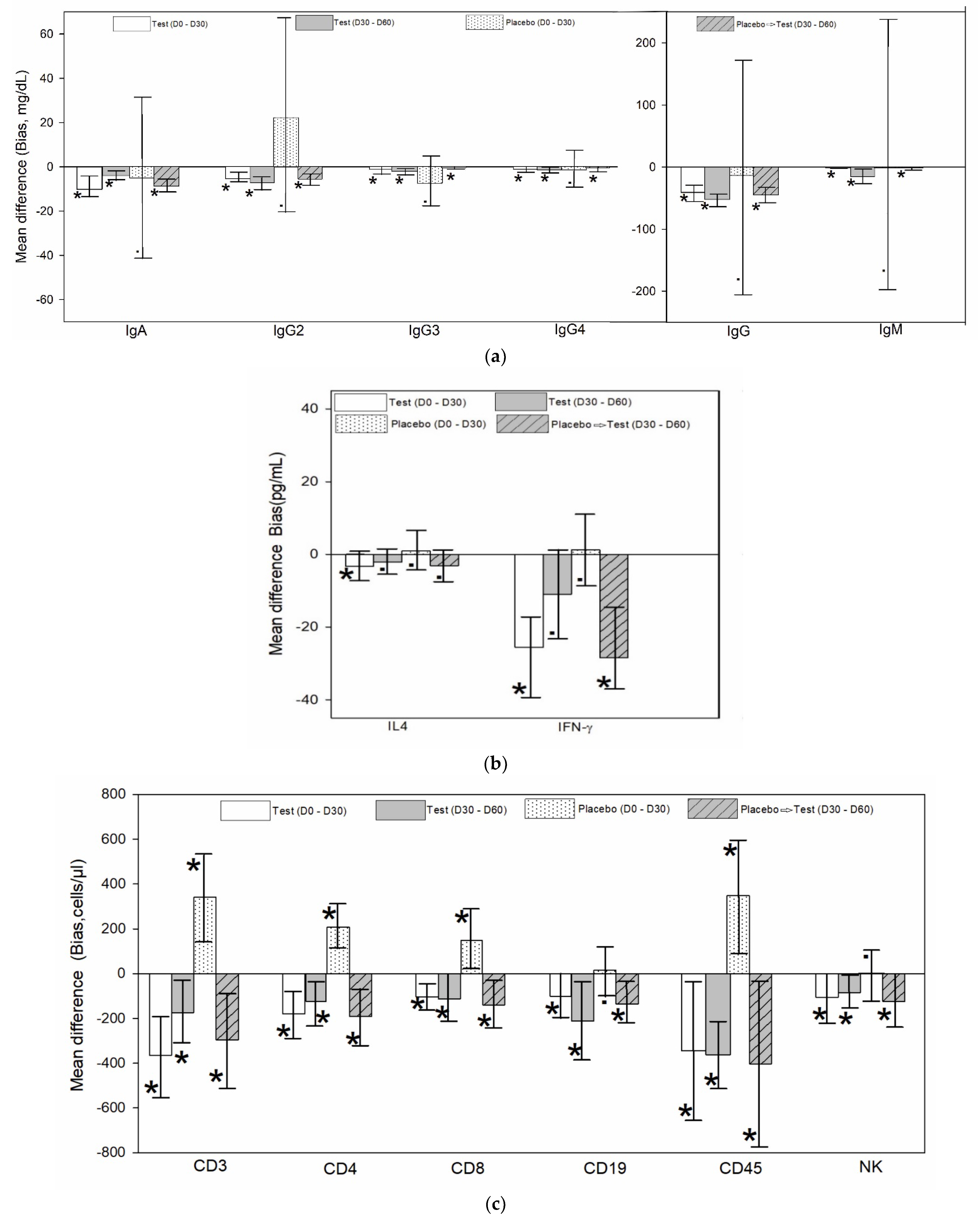
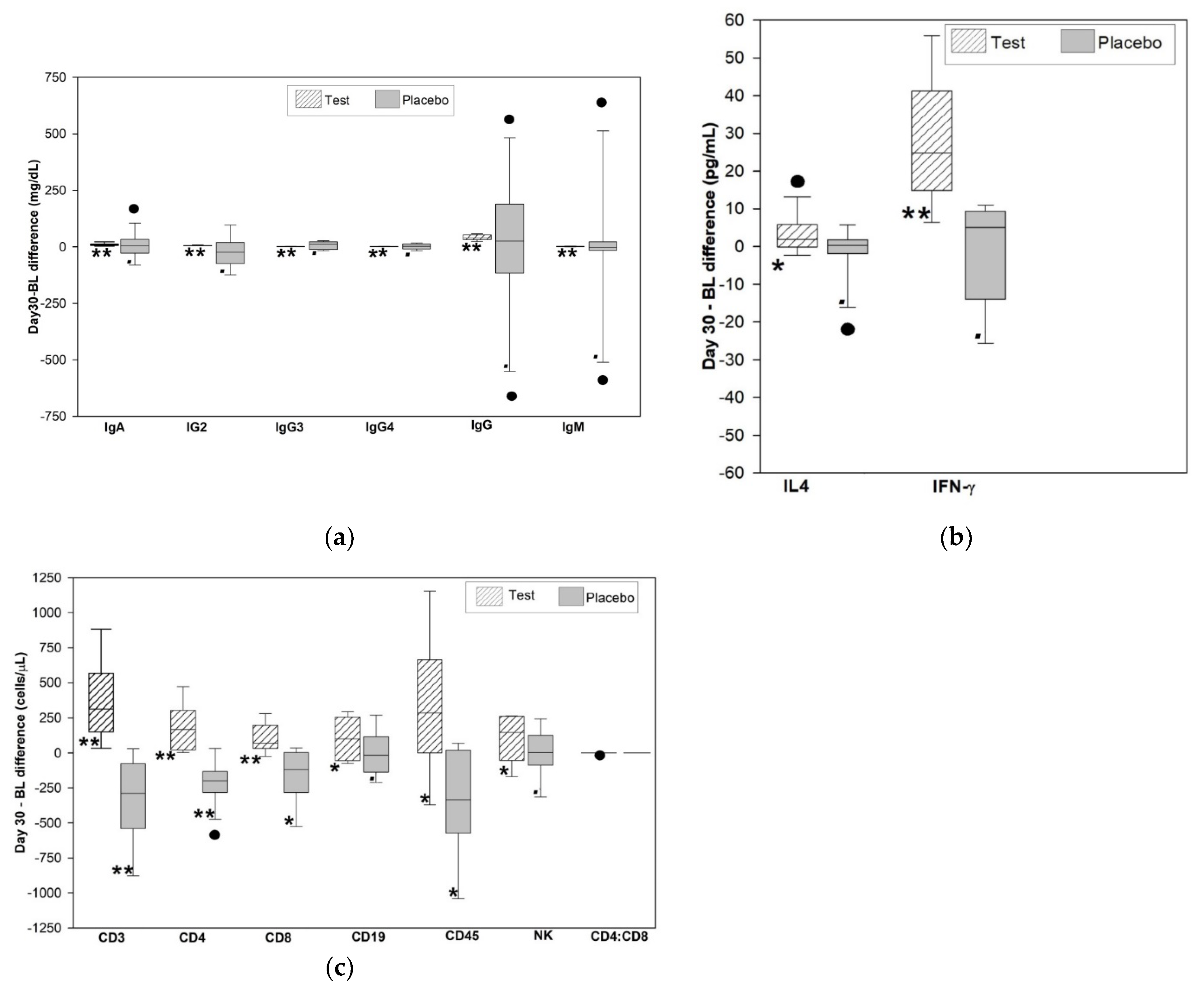
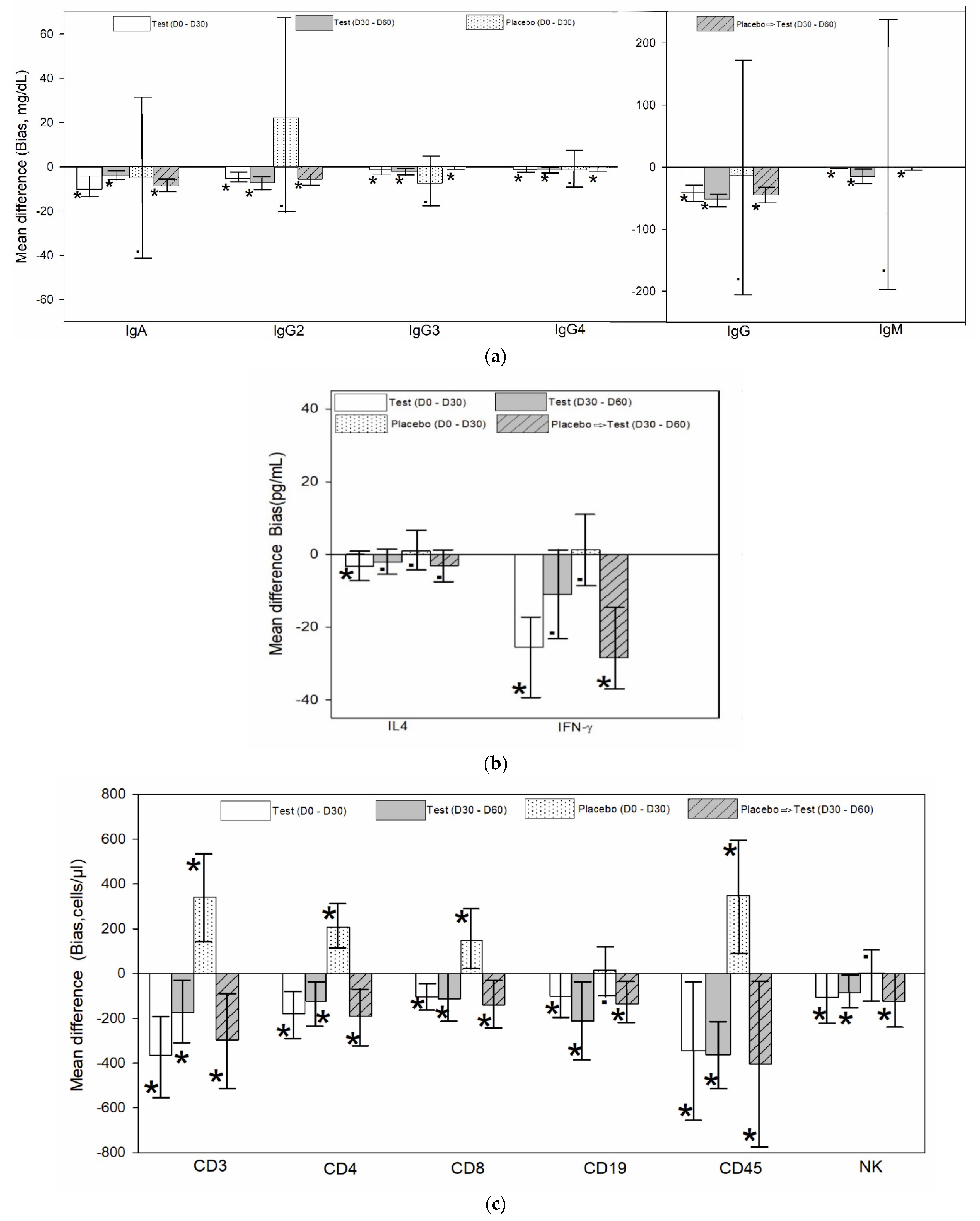
3.1. Analysis of the Immunoglobulin Level in the Test Group Compared to Placebo
3.2. Analysis of the Cytokines (IFN γ and IL4) Level in the Test Group Compared to Placebo
3.3. Analysis of the TBNK Cell Absolute Count in the Test Group Compared to Placebo
3.4. Biochemical and Safety Analysis
4. Discussion
Limitations and Future Directions of Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Clinical Trial Registration
References
- Chaplin, D.D. Overview of the immune response. J. Allergy Clin. Immunol. 2010, 125, S3–S23. [Google Scholar] [CrossRef] [PubMed]
- Ghosal, S.; Lal, J.; Srivastava, R.; Bhattacharya, S.K.; Upadhyay, S.N.; Jaiswal, A.K.; Chattopadhyay, U. Immunomodulatory and CNS effects of sitoindosides IX and X, two new glycowithanolides from Withania somnifera. Phytother. Res. 1989, 3, 201–206. [Google Scholar] [CrossRef]
- Kuttan, L.D.G. Amelioration of cyclophosphamide induced toxicity using Withania somnifera. Amala Res. Bull. 1996, 16, 109–112. [Google Scholar]
- Antony, B.; Benny, M.; Kuruvilla, B.T.; Sebastian, A.; Pillai, A.A.A.; Joseph, B.; Chandran, S.E. Development and validation of an RP-HPLC method for the simultaneous determination of total withanolide glycosides and Withaferin A in Withania somnifera (Ashwagandha). Curr. Chromatogr. 2020, 7, 106–120. [Google Scholar] [CrossRef]
- Julious, S.A. Sample size of 12 per group rule of thumb for a pilot study. Pharm. Stat. 2005, 4, 287–291. [Google Scholar] [CrossRef]
- Lochmiller, R.L.; Vestey, M.R.; McMurry, S.T. Temporal Variation in Humoral and Cell-Mediated Immune Response in a Sigmodon Hispidus Population. Ecology 1994, 75, 236–245. [Google Scholar] [CrossRef]
- Silverin, B. Stress responses in birds. Avian Poult. Biol. Rev. 1998, 9, 153–168. [Google Scholar]
- Nelson, S.L.; Klein, S.L. Immune function, mating systems, and seasonal breeding. In Reproduction in Context; Wallen, K., Schneider, J.E., Eds.; MIT Press: Cambridge, MA, USA, 1999; pp. 219–256. [Google Scholar]
- Khan, S.; Malik, F.; Suri, K.A.; Singh, J. Molecular insight into the immune up-regulatory properties of the leaf extract of Ashwagandha and identification of Th1 immunostimulatory chemical entity. Vaccine 2009, 27, 6080–6087. [Google Scholar] [CrossRef] [PubMed]
- Bani, S.; Gautam, M.; Sheikh, F.A.; Khan, B.; Satti, N.K.; Suri, K.A.; Qazi, G.N.; Patwardhan, B. Selective Th1 up-regulating activity of Withania somnifera aqueous extract in an experimental system using flow cytometry. J. Ethnopharmacol. 2006, 107, 107–115. [Google Scholar] [CrossRef]
- Kuttan, G. Use of Withania somnifera Dunal as an adjuvant during radiation therapy. Indian J. Exp. Boil. 1996, 34, 854–856. [Google Scholar]
- Ziauddin, M.; Phansalkar, N.; Patki, P.; Diwanay, S.; Patwardhan, B. Studies on the immunomodulatory effects of Ashwagandha. J. Ethnopharmacol. 1996, 50, 69–76. [Google Scholar] [CrossRef]
- Davis, L.; Kuttan, G. Effect of Withania somnifera on CTL activity. J. Exp. Clin. Cancer Res. 2002, 21, 115–118. [Google Scholar] [PubMed]
- Malik, F.; Singh, J.; Khajuria, A.; Suri, K.A.; Satti, N.K.; Singh, S.; Kaul, M.K.; Kumar, A.; Bhatia, A.; Qazi, G.N. A standardized root extract of Withania somnifera and its major constituent withanolide—A elicit humoral and cell-mediated immune responses by up regulation of Th1-dominant polarization in BALB/c mice. Life Sci. 2007, 80, 1525–1538. [Google Scholar] [CrossRef] [PubMed]
- Romagnani, S. Th1/Th2 cells. Inflamm. Bowel Dis. 2007, 5, 285–294. [Google Scholar] [CrossRef] [PubMed]
- Nelson, R.J.; Demas, G.E. Seasonal Changes in Immune Function. Q. Rev. Biol. 1996, 71, 511–548. [Google Scholar] [CrossRef]
- Deshpande, A.; Irani, N.; Balkrishnan, R.; Benny, I.R. A randomized, double blind, placebo controlled study to evaluate the effects of ashwagandha (Withania somnifera) extract on sleep quality in healthy adults. Sleep Med. 2020, 72, 28–36. [Google Scholar] [CrossRef]
- MacMurray, J.P.; Barker, J.P.; Armstrong, J.D.; Bozzetti, L.P.; Kuhn, I.N. Circannual changes in immune function. Life Sci. 1983, 32, 2363–2370. [Google Scholar] [CrossRef]
- Van Rood, Y.; Goulmy, E.; Blokland, E.; Pool, J.; Van Rood, J.; van Houwelingen, H.C. Month-related variability in immunological test results; implications for immunological follow-up studies. Clin. Exp. Immunol. 1991, 86, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Straub, R.; Schölmerich, J.; Zietz, B. Replacement therapy with DHEA plus corticosteroids in patients with chronic inflammatory diseases—substitutes of adrenal and sex hormones. Z. Rheumatologie 2000, 59, 108–118. [Google Scholar] [CrossRef]
- Semple, C.G.; Gray, C.E.; Beastall, G.H. Adrenal androgens and illness. Acta Endocrinol. Copenh. 2008, 116, 155–160. [Google Scholar] [CrossRef]
- Lopresti, A.L.; Drummond, P.D.; Smith, S.J. A Randomized, Double-Blind, Placebo-Controlled, Crossover Study Examining the Hormonal and Vitality Effects of Ashwagandha (Withania somnifera) in Aging, Overweight Males. Am. J. Men’s Health 2019, 13, 13. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kaur, T.; Singh, H.; Mishra, R.; Manchanda, S.; Gupta, M.; Saini, V.; Sharma, A.; Kaur, G. Withania somnifera as a potential anxiolytic and immunomodulatory agent in acute sleep deprived female Wistar rats. Mol. Cell. Biochem. 2016, 427, 91–101. [Google Scholar] [CrossRef] [PubMed]
- Priyanka, G.; Kumar, B.A.; Lakshman, M.; Manvitha, V. Adaptogenic and Immunomodulatory Activity of Ashwagandha Root Extract: An Experimental Study in an Equine Model. Front. Veter Sci. 2020, 7, 541112. [Google Scholar] [CrossRef] [PubMed]
- Kumar, J.; Mitra, M.D.; Hussain, A.; Kaul, G. Exploration of immunomodulatory and protective effect of Withania somnifera on trace metal oxide (zinc oxide nanoparticles) induced toxicity in Balb/c mice. Mol. Biol. Rep. 2019, 46, 2447–2459. [Google Scholar] [CrossRef] [PubMed]
- Barua, A.; Bradaric, M.; Bitterman, P.; Abramowicz, J.; Sharma, S.; Basu, S.; Lopez, H.; Bahr, J.M. Dietary Supplementation of Ashwagandha (Withania somnifera, Dunal) Enhances NK Cell Function in Ovarian Tumors in the Laying Hen Model of Spontaneous Ovarian Cancer. Am. J. Reprod. Immunol. 2013, 70, 538–550. [Google Scholar] [CrossRef] [PubMed]
- Turrini, E.; Calcabrini, C.; Sestili, P.; Catanzaro, E.; De Gianni, E.; Diaz, A.R.; Hrelia, P.; Tacchini, M.; Guerrini, A.; Canonico, B.; et al. Withania somnifera Induces Cytotoxic and Cytostatic Effects on Human T Leukemia Cells. Toxins 2016, 8, 147. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maurya, S.P.; Das, B.K.; Singh, R.; Tyagi, S. Effect of Withania somnifer on CD38 expression on CD8+ T lymphocytes among patients of HIV infection. Clin. Immunol. 2019, 203, 122–124. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Test Group | Placebo Group | Between the Groups | |
|---|---|---|---|
| Mean ± SE | Mean ± SE | p Value * | |
| Age (years) | 53.92 ± 1.83 | 56.17 ± 2.39 | 0.461 |
| Height (cm) | 156.50 ± 1.69 | 156.75 ± 2.12 | 0.929 |
| Weight (kg) | 65.13 ± 2.85 | 67.75 ± 2.07 | 0.467 |
| BMI (kg/m2) | 26.47 ± 0.80 | 27.51 ± 0.42 | 0.258 |
| Test Group | Within Group Analysis of Test Group | Placebo Group | P➔T ** | Within Group Analysis | Between Group Analysis | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Crossover Group | Placebo Group | P➔T ** Crossover Group | ||||||||||||||||
| Day 0 | Day 30 | Day 60 | Day 0–30 | Day 30–60 | Day 0–60 | Day 0 | Day 30 | Day 60 | Day 0–30 | Day 30–60 | Day 0 | Day 30 | ||||||
| Mean ± SE | Mean ± SE | Mean ± SE | % Change | p Value # | % Change | p Value # | % Change | p Value # | Mean ± SE | Mean ± SE | Mean ± SE | % Change | p Value # | % Change | p Value # | p Value $ | p Value $ | |
| IgA | 170.06 ± 16.99 | 180.2 ± 18.28 | 184.13 ± 18.66 | 5.96 | <0.001 | 2.18 | <0.001 | 8.27 | <0.001 | 169.9 ± 14.95 | 174.88 ± 15.76 | 183.62 ± 16.55 | 2.93 | 0.764 | 5 | <0.001 | 0.994 | 0.828 |
| IgG2 | 212.16 ± 16.4 | 217.5 ± 16.71 | 224.69 ± 17.25 | 2.52 | <0.001 | 3.31 | <0.001 | 5.91 | <0.001 | 205.97 ± 21.36 | 183.74 ± 15.4 | 189.25 ± 15.86 | −10.79 | 0.286 | 3 | <0.001 | 0.82 | 0.151 |
| IgG3 | 47.63 ± 3.72 | 48.83 ± 3.81 | 50.87 ± 3.97 | 2.52 | <0.001 | 4.18 | <0.001 | 6.8 | <0.001 | 43.03 ± 3.5 | 50.36 ± 5.38 | 50.76 ± 5.42 | 17.03 | 0.172 | 0.79 | <0.001 | 0.377 | 0.819 |
| IgG4 | 24.96 ± 2.64 | 25.97 ± 2.76 | 27.37 ± 2.90 | 4.05 | <0.001 | 5.39 | <0.001 | 9.66 | <0.001 | 24.95 ± 2.67 | 26.42 ± 2.47 | 26.95 ± 2.52 | 5.89 | 0.704 | 2.01 | <0.001 | 0.997 | 0.906 |
| IgG | 801.44 ± 59.19 | 842.23 ± 62.2 | 894.14 ± 66.12 | 5.09 | <0.001 | 6.16 | <0.001 | 11.57 | <0.001 | 822.99 ± 69.52 | 836.58 ± 70.88 | 881.75 ± 74.71 | 1.65 | 0.879 | 5.4 | <0.001 | 0.816 | 0.953 |
| IgM | 183.9 ± 34.41 | 185.43 ± 34.67 | 200.7 ± 37.54 | 0.83 | <0.001 | 8.23 | <0.001 | 9.14 | <0.001 | 184.14 ± 55.64 | 185.17 ± 55.97 | 186.41 ± 56.34 | 0.56 | 0.99 | 0.67 | 0.002 * | 0.997 | 0.299 * |
| Test Group | Within Group Analysis of Test Group | Placebo Group | P➔T ** Crossover Group | Within Group Analysis | Between Group Analysis | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Placebo Group | P➔T ** Crossover Group | |||||||||||||||||
| Day 0 | Day 30 | Day 60 | Day 0–30 | Day 30–60 | Day 0–60 | Day 0 | Day 30 | Day 60 | Day 0–30 | Day 30–60 | Day 0 | Day 30 | ||||||
| Mean ± SE | Mean ± SE | Mean ± SE | % Change | p Value # | % Change | p Value # | % Change | p Value # | Mean ± SE | Mean ± SE | Mean ± SE | % Change | p Value # | % Change | p Value # | p Value $ | p Value $ | |
| CD45 | 2148.03 ± 159.54 | 2492.41 ± 105.24 | 2854.3 ± 92.85 | 12.07 | 0.032 | 14.52 | <0.001 | 32.88 | 0.001 | 2201.22 ± 191.39 | 1852.96 ± 122.25 | 2255.87 ± 132.64 | −15.44 | 0.009 | 21.74 | 0.036 | 0.833 | 0.001 |
| CD3 | 1334.71 ± 98.24 | 1699.4 ± 76.06 | 1874.02 ± 90.06 | 19.46 | 0.001 | 10.28 | 0.026 | 40.41 | 0.002 | 1595.16 ± 109.60 | 1253.94 ± 68.87 | 1550.93 ± 96.93 | −22.00 | 0.002 | 23.68 | 0.01 | 0.091 | <0.001 |
| CD4 | 738.23 ± 54.71 | 918.25 ± 49.85 | 1042.82 ± 49.84 | 17.26 | 0.003 | 13.57 | 0.018 | 41.26 | 0.001 | 876.88 ± 59.59 | 669.3 ± 47.57 | 860.34 ± 54.87 | −24.13 | 0.001 | 28.54 | 0.005 | 0.101 | 0.002 |
| CD8 | 498.95 ± 39.11 | 603.31 ± 24.77 | 716.47 ± 52.85 | 14.57 | 0.005 | 18.76 | 0.028 | 43.6 | 0.003 | 604.37 ± 53.12 | 455.06 ± 24.24 | 594.18 ± 43.47 | −25.13 | 0.02 | 30.57 | 0.01 | 0.124 | <0.001 |
| CD19 | 661.53 ± 29.81 | 761.98 ± 30.87 | 974.39 ± 63.75 | 10.31 | 0.034 | 27.88 | 0.021 | 47.29 | 0.004 | 751.06 ± 32.04 | 734.83 ± 28.08 | 870.1 ± 42.12 | −1.87 | 0.733 | 18.41 | 0.006 | 0.053 | 0.522 |
| NK | 361.92 ± 66.06 | 467.36 ± 68.41 | 552.68 ± 62.51 | 19.08 | 0.046 | 18.26 | 0.015 | 52.71 | <0.001 | 341.95 ± 60.83 | 341.26 ± 42.73 | 465.47 ± 35.37 | −0.15 | 0.989 | 36.4 | 0.027 | 0.826 | 0.132 |
| IFNγ | 72.15 ± 7.25 | 100.60 ± 10.67 | 111.61 ± 7.64 | 39.44 | <0.001 | 10.94 | 0.056 | 54.69 | <0.001 | 73.36 ± 6.11 | 72.06 ± 5.70 | 97.65 ± 9.01 | −1.77 | 0.749 | 35.51 | <0.001 | 0.899 | 0.028 |
| IL4 | 3.92 ± 1.42 | 7.16 ± 1.51 | 9.30 ± 1.13 | 82.53 | 0.047 | 29.89 | 0.053 | 137.06 | 0.004 | 4.20 ± 1.94 | 3.21 ± 1.35 | 6.29 ± 0.80 | −23.50 | 0.814 * | 95.87 | 0.038 * | 0.817 | 0.03 |
| Test Group | Within Group Analysis of Test Group | Placebo | P➔T ** Crossover Group | Within Group Analysis | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Placebo | P➔T ** Crossover Group | |||||||||
| Day 0 | Day 30 | Day 60 | Day 0–30 | Day 0–60 | Day 0 | Day 30 | Day 60 | Day 0–30 | Day 30–60 | |
| Mean + SE | Mean + SE | Mean + SE | p-Value # | p-Value # | Mean + SE | Mean + SE | Mean + SE | p-Value # | p-Value # | |
| Red Blood Cell | 4.46 ± 0.08 | 4.58 ± 0.10 | 4.49 ± 0.08 | 0.244 | 0.755 | 4.52 ± 0.07 | 4.56 ± 0.05 | 4.55 ± 0.10 | 0.587 | 0.931 |
| (1012/L) | ||||||||||
| Hemoglobin (g/dl) | 12.98 ± 0.27 | 13.04 ± 0.29 | 13.00 ± 0.22 | 0.792 | 0.946 | 12.62 ± 0.32 | 12.38 ± 0.20 | 12.49 ± 0.22 | 0.446 | 0.567 |
| Hematocrit (%) | 44.00 ± 0.85 | 42.18 ± 1.02 | 41.34 ± 1.05 | 0.078 | 0.021 | 40.92 ± 1.02 | 40.78 ± 0.86 | 41.76 ± 0.84 | 0.871 | 0.432 |
| Platelet count (109/L) | 248.42 ± 19.20 | 286.92 ± 21.33 | 299.25 ± 18.36 | 0.017 | 0.009 | 226.08 ± 12.12 | 288.08 ± 14.95 | 301.75 ± 16.56 | 0.006 | 0.511 |
| Neutrophil count (cells/mm3) | 3611.73 ± 92.30 | 3930.02 ± 73.19 | 4089.26 ± 126.28 | 0.001 | <0.001 | 3658.69 ± 138.22 | 3624.15 ± 107.61 | 3561.05 ± 118.30 | 0.772 | 0.716 |
| Eosinophil count (cells/mm3) | 149.72 ± 6.01 | 150.10 ± 5.97 | 155.05 ± 4.84 | 0.945 | 0.241 | 142.69 ± 5.13 | 141.24 ± 4.11 | 142.16 ± 5.29 | 0.846 | 0.859 |
| Basophil count | 55.46 ± 5.84 | 61.42 ± 6.14 | 55.67 ± 5.32 | 0.358 | 0.969 | 57.58 ± 5.84 | 56.38 ± 4.76 | 58.09 ± 5.69 | 0.894 | 0.826 |
| (cells/mm3) | ||||||||||
| Monocyte count (cells/mm3) | 459.25 ± 15.58 | 457.76 ± 16.11 | 495.37 ± 14.70 | 0.899 | 0.033 | 464.19 ± 17.59 | 442.73 ± 14.28 | 459.03 ± 18.53 | 0.267 | 0.532 |
| Leukocytes | 5706.67 ± 126.82 | 5875.81 ± 128.18 | 6095.51 ± 140.05 | <0.001 | <0.001 | 5701.67 ± 138.70 | 5630.00 ± 115.13 | 5496.67 ± 162.25 | 0.087 | 0.529 |
| (cells/mm3) | ||||||||||
| Lymphocytes | 1830.45 ± 130.18 | 2297.50 ± 152.05 | 2656.51 ± 210.26 | 0.004 | 0.002 | 1711.42 ± 46.66 | 1131.61 ± 95.09 | 1644.33 ± 132.33 | <0.001 | 0.008 |
| (cells/mm3) | ||||||||||
| Total Cholesterol (mg/dL) | 184.17 ± 7.83 | 180.67 ± 8.37 | 171.67 ± 6.88 | 0.561 | 0.172 | 186.83 ± 3.95 | 168.25 ± 4.11 | 172.17 ± 4.39 | 0.009 | 0.424 |
| Triglycerides (mg/dL) | 156.75 ± 5.89 | 154.68 ± 5.56 | 150.83 ± 5.77 | 0.529 | 0.267 | 161.00 ± 5.66 | 151.62 ± 3.59 | 152.33 ± 4.74 | 0.077 | 0.661 |
| LDL Cholesterol (mg/dL) | 72.00 ± 3.08 | 67.58 ± 3.34 | 63.33 ± 3.31 | 0.183 | 0.013 | 71.75 ± 3.08 | 67.50 ± 2.66 | 67.28 ± 1.70 | 0.035 | 0.096 |
| VLDL Cholesterol (mg/dL) | 32.67 ± 1.32 | 32.00 ± 1.84 | 32.36 ± 2.38 | 0.627 | 0.883 | 29.25 ± 1.42 | 30.28 ± 1.50 | 27.87 ± 1.52 | 0.599 | 0.044 |
| HDL Cholesterol (mg/dL) | 32.17 ± 0.84 | 33.03 ± 0.71 | 31.08 ± 1.16 | 0.308 | 0.469 | 34.42 ± 4.04 | 33.03 ± 0.73 | 32.25 ± 0.66 | 0.769 | 0.334 |
| SGOT (U/L) | 22.28 ± 1.35 | 26.25 ± 1.83 | 26.08 ± 1.07 | 0.076 | 0.021 | 24.00 ± 1.31 | 27.30 ± 1.52 | 26.98 ± 1.27 | 0.079 | 0.647 |
| SGPT (U/L) | 46.20 ± 3.00 | 51.71 ± 2.43 | 52.94 ± 2.70 | 0.115 | 0.067 | 48.60 ± 3.82 | 52.15 ± 3.27 | 51.33 ± 2.55 | 0.382 | 0.711 |
| Blood Urea (mg/dL) | 15.32 ± 0.67 | 15.02 ± 0.69 | 14.42 ± 0.48 | 0.499 | 0.192 | 14.58 ± 0.87 | 14.83 ± 0.54 | 14.95 ± 0.72 | 0.799 | 0.792 |
| Serum creatinine (mg/dL) | 0.73 ± 0.03 | 0.56 ± 0.06 | 0.57 ± 0.05 | 0.02 | 0.007 | 0.72 ± 0.02 | 0.66 ± 0.06 | 0.68 ± 0.07 | 0.408 | 0.634 |
| Fasting Blood Sugar (mg/dL) | 88.17 ± 2.55 | 88.25 ± 2.55 | 88.62 ± 2.71 | 0.984 | 0.907 | 90.67 ± 2.60 | 90.37 ± 2.04 | 89.19 ± 2.21 | 0.914 | 0.561 |
| Systolic Blood Pressure (mm/Hg) | 127.08 ± 0.96 | 126.50 ± 0.89 | 126.92 ± 0.75 | 0.669 | 0.845 | 128.25 ± 1.56 | 127.75 ± 1.02 | 126.92 ± 0.84 | 0.784 | 0.372 |
| Diastolic Blood Pressure (mm/Hg) | 84.42 ± 1.18 | 84.67 ± 0.88 | 85.33 ± 1.09 | 0.891 | 0.613 | 83.92 ± 1.50 | 85.67 ± 0.87 | 85.50 ± 1.00 | 0.358 | 0.883 |
| Pulse rate (beats/min) | 74.25 ± 1.90 | 71.75 ± 1.15 | 73.42 ± 1.29 | 0.106 | 0.493 | 75.58 ± 1.11 | 74.83 ± 1.05 | 72.42 ± 0.82 | 0.529 | 0.092 |
| Temperature (°C) | 36.74 ± 0.11 | 36.63 ± 0.09 | 36.53 ± 0.09 | 0.463 | 0.138 | 36.79 ± 0.13 | 36.64 ± 0.12 | 36.41 ± 0.07 | 0.523 | 0.14 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tharakan, A.; Shukla, H.; Benny, I.R.; Tharakan, M.; George, L.; Koshy, S. Immunomodulatory Effect of Withania somnifera (Ashwagandha) Extract—A Randomized, Double-Blind, Placebo Controlled Trial with an Open Label Extension on Healthy Participants. J. Clin. Med. 2021, 10, 3644. https://doi.org/10.3390/jcm10163644
Tharakan A, Shukla H, Benny IR, Tharakan M, George L, Koshy S. Immunomodulatory Effect of Withania somnifera (Ashwagandha) Extract—A Randomized, Double-Blind, Placebo Controlled Trial with an Open Label Extension on Healthy Participants. Journal of Clinical Medicine. 2021; 10(16):3644. https://doi.org/10.3390/jcm10163644
Chicago/Turabian StyleTharakan, Ajit, Himanshu Shukla, Irin Rosanna Benny, Matthan Tharakan, Lekha George, and Santhosh Koshy. 2021. "Immunomodulatory Effect of Withania somnifera (Ashwagandha) Extract—A Randomized, Double-Blind, Placebo Controlled Trial with an Open Label Extension on Healthy Participants" Journal of Clinical Medicine 10, no. 16: 3644. https://doi.org/10.3390/jcm10163644
APA StyleTharakan, A., Shukla, H., Benny, I. R., Tharakan, M., George, L., & Koshy, S. (2021). Immunomodulatory Effect of Withania somnifera (Ashwagandha) Extract—A Randomized, Double-Blind, Placebo Controlled Trial with an Open Label Extension on Healthy Participants. Journal of Clinical Medicine, 10(16), 3644. https://doi.org/10.3390/jcm10163644