
Age-Related Changes in Left Ventricular Vortex Formation and Flow Energetics


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Transthoracic Echocardiography
2.3. Vector Flow Mapping Analysis
2.4. Statistical Analysis
3. Results
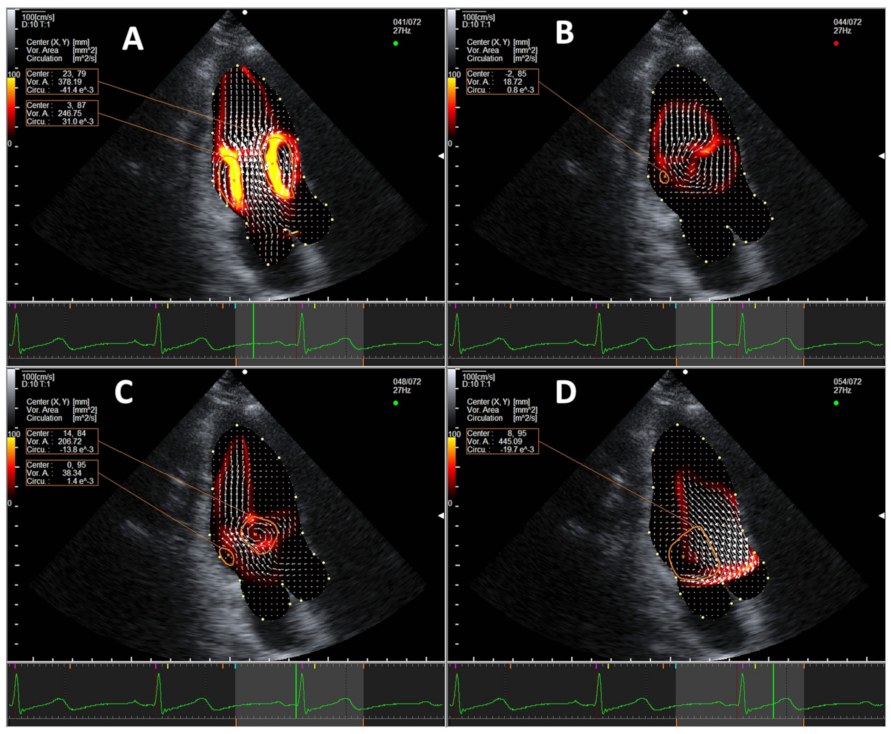
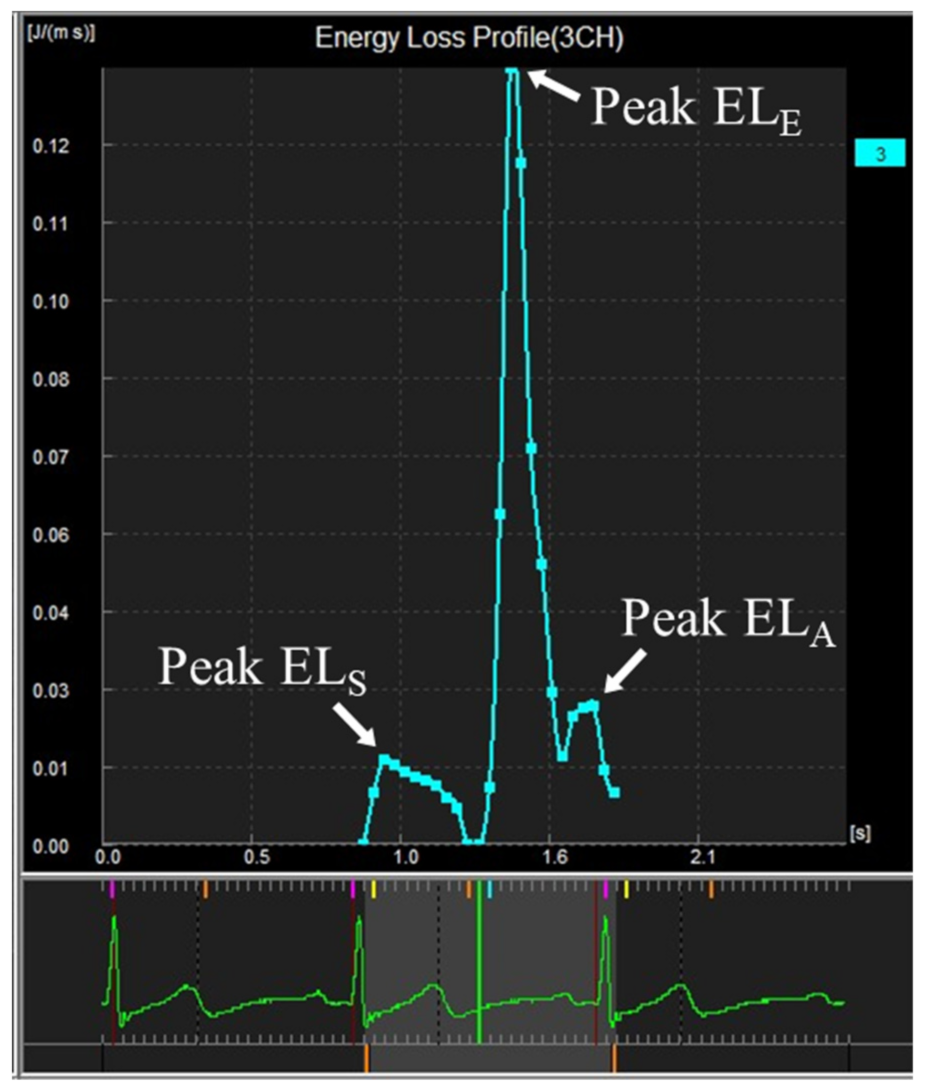
3.1. Normal Intracardiac Vortex Flow and EL
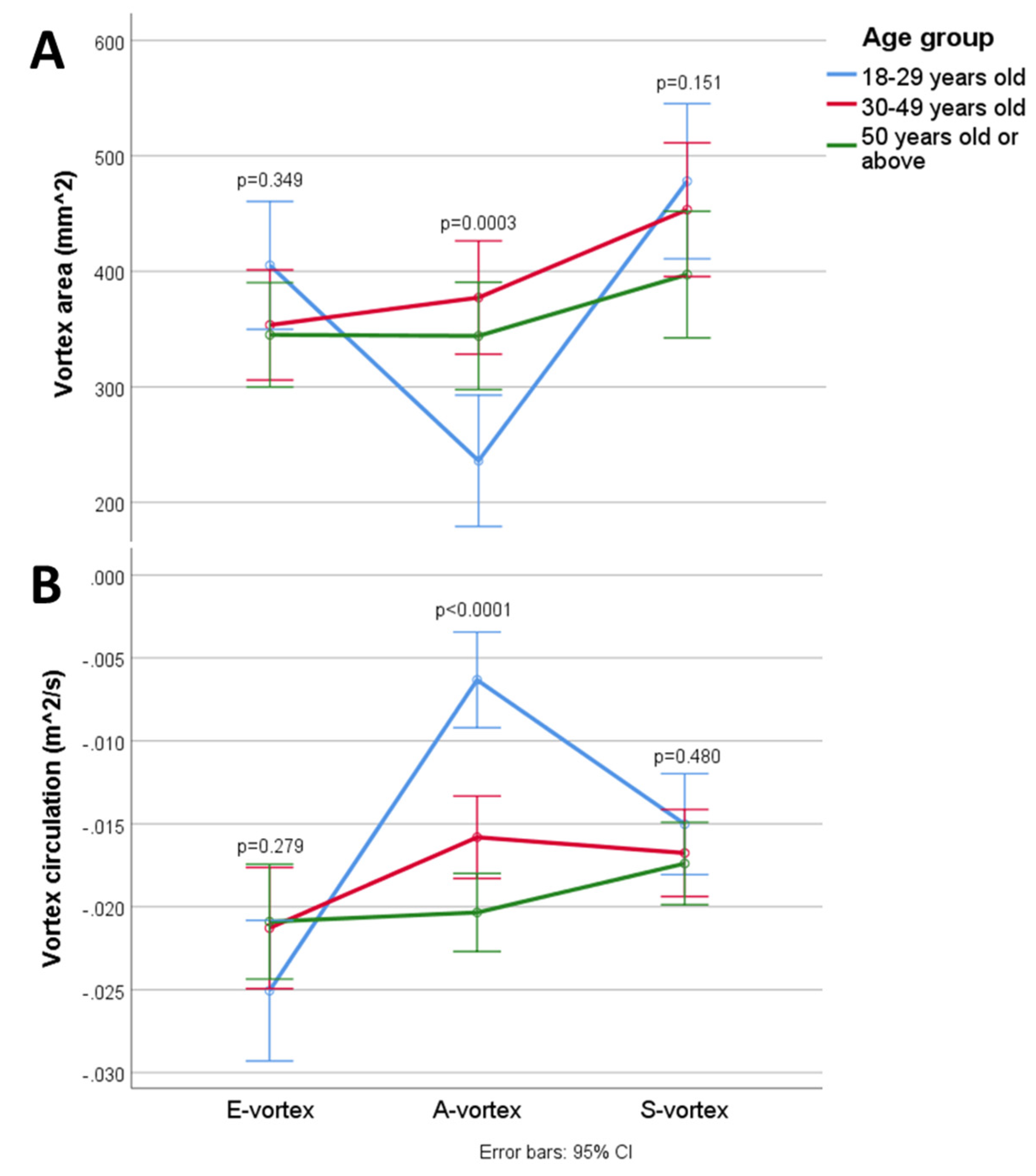
3.2. Intracardiac Vortex Flow Characteristics and Aging
3.3. Interrelations among Intracardiac Flow, Energetics, and Aging
4. Discussion
4.1. Clinical Significance
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kim, I.-C.; Hong, G.-R. Intraventricular Flow: More than Pretty Pictures. Heart Fail. Clin. 2019, 15, 257–265. [Google Scholar] [CrossRef]
- Hansen, K.L.; Nielsen, M.B.; Jensen, J.A. Vector velocity estimation of blood flow—A new application in medical ultrasound. Ultrasound 2017, 25, 189–199. [Google Scholar] [CrossRef]
- Mele, D.; Smarrazzo, V.; Pedrizzetti, G.; Capasso, F.; Pepe, M.; Severino, S.; Luisi, G.A.; Maglione, M.; Ferrari, R. Intracardiac Flow Analysis: Techniques and Potential Clinical Applications. J. Am. Soc. Echocardiogr. 2019, 32, 319–332. [Google Scholar] [CrossRef]
- Li, C.; Zhang, J.; Li, X.; Zhou, C.; Li, H.; Tang, H.; Rao, L. Quantification of chronic aortic regurgitation by vector flow mapping: A novel echocardiographic method. Eur. J. Echocardiogr. 2009, 11, 119–124. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hong, G.-R.; Pedrizzetti, G.; Tonti, G.; Li, P.; Wei, Z.; Kim, J.K.; Baweja, A.; Liu, S.; Chung, N.; Houle, H.; et al. Characterization and Quantification of Vortex Flow in the Human Left Ventricle by Contrast Echocardiography Using Vector Particle Image Velocimetry. JACC Cardiovasc. Imaging 2008, 1, 705–717. [Google Scholar] [CrossRef] [PubMed]
- Elbaz, M.S.M.; Calkoen, E.; Westenberg, J.J.M.; Lelieveldt, B.P.F.; Roest, A.A.W.; Van Der Geest, R.J. Vortex flow during early and late left ventricular filling in normal subjects: Quantitative characterization using retrospectively-gated 4D flow cardiovascular magnetic resonance and three-dimensional vortex core analysis. J. Cardiovasc. Magn. Reson. 2014, 16, 78. [Google Scholar] [CrossRef] [PubMed]
- Martinez-Legazpi, P.; Bermejo, J.; Benito, Y.; Yotti, R.; del Villar, C.P.; González-Mansilla, A.; Barrio, A.; Villacorta, E.; Sanchez, P.L.; Fernández-Avilés, F.; et al. Contribution of the Diastolic Vortex Ring to Left Ventricular Filling. J. Am. Coll. Cardiol. 2014, 64, 1711–1721. [Google Scholar] [CrossRef] [PubMed]
- Hong, G.-R.; Kim, M.; Pedrizzetti, G.; Vannan, M. Current Clinical Application of Intracardiac Flow Analysis Using Echocardiography. J. Cardiovasc. Ultrasound 2013, 21, 155–162. [Google Scholar] [CrossRef] [PubMed]
- Parikh, J.D.; Hollingsworth, K.G.; Wallace, D.; Blamire, A.; MacGowan, G.A. Normal age-related changes in left ventricular function: Role of afterload and subendocardial dysfunction. Int. J. Cardiol. 2016, 223, 306–312. [Google Scholar] [CrossRef]
- Wang, W.; Wang, Y.; Chen, X.; Yuan, L.; Bai, H. Evaluation of left ventricular diastolic function based on flow energetic parameters in chronic kidney disease with diastolic dysfunction. Echocardiography 2019, 36, 567–576. [Google Scholar] [CrossRef]
- Zhang, X.; Niu, J.; Wu, L.; Li, Q.; Han, Y.; Li, Y.; Wu, X.; Che, X.; Li, Z.; Ma, N.; et al. Factors influencing the end-diastolic vortex assessed by using vector flow mapping. Echocardiography 2019, 36, 1639–1645. [Google Scholar] [CrossRef] [PubMed]
- Wong, J.; Chabiniok, R.; Devecchi, A.; Dedieu, N.; Sammut, E.; Schaeffter, T.; Razavi, R. Age-related changes in intraventricular kinetic energy: A physiological or pathological adaptation? Am. J. Physiol. Circ. Physiol. 2016, 310, H747–H755. [Google Scholar] [CrossRef]
- Mitchell, C.; Rahko, P.S.; Blauwet, L.A.; Canaday, B.; Finstuen, J.A.; Foster, M.C.; Horton, K.; Ogunyankin, K.O.; Palma, R.A.; Velazquez, E.J. Guidelines for Performing a Comprehensive Transthoracic Echocardiographic Examination in Adults: Recommendations from the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2019, 32, 1–64. [Google Scholar] [CrossRef] [PubMed]
- Nagueh, S.F.; Smiseth, O.A.; Appleton, C.P.; Byrd, B.F.; Dokainish, H.; Edvardsen, T.; Flachskampf, F.A.; Gillebert, T.; Klein, A.L.; Lancellotti, P.; et al. Recommendations for the Evaluation of Left Ventricular Diastolic Function by Echocardiography: An Update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2016, 29, 277–314. [Google Scholar] [CrossRef] [PubMed]
- Itatani, K.; Okada, T.; Uejima, T.; Tanaka, T.; Ono, M.; Miyaji, K.; Takenaka, K. Intraventricular Flow Velocity Vector Visualization Based on the Continuity Equation and Measurements of Vorticity and Wall Shear Stress. Jpn. J. Appl. Phys. 2013, 52, 07HF16. [Google Scholar] [CrossRef]
- Garcia, D.; Del Alamo, J.C.; Tanne, D.; Yotti, R.; Cortina, C.; Bertrand, E.; Antoranz, J.C.; David, E.P.; Rieu, R.; Fernandez-Aviles, F.; et al. Two-Dimensional Intraventricular Flow Mapping by Digital Processing Conventional Color-Doppler Echocardiography Images. IEEE Trans. Med. Imaging 2010, 29, 1701–1713. [Google Scholar] [CrossRef] [PubMed]
- Itatani, K. When the blood flow becomes bright. Eur. Heart J. 2014, 35, 747–752. [Google Scholar]
- Faludi, R.; Szulik, M.; D’Hooge, J.; Herijgers, P.; Rademakers, F.; Pedrizzetti, G.; Voigt, J.-U. Left ventricular flow patterns in healthy subjects and patients with prosthetic mitral valves: An in vivo study using echocardiographic particle image velocimetry. J. Thorac. Cardiovasc. Surg. 2010, 139, 1501–1510. [Google Scholar] [CrossRef]
- Muñoz, D.; Mur, J.L.M.; Fernández-Golfín, C.; Filho, D.C.B.; Gómez, A.G.; Santos, S.F.; Rivera, C.L.; Díaz, L.M.R.; Rojo, E.C.; Gómez, J.L.Z. Left Ventricular Vortices as Observed by Vector Flow Mapping: Main Determinants and their Relation to Left Ventricular Filling. Echocardiography 2014, 32, 96–105. [Google Scholar] [CrossRef]
- Govindarajan, V.; Mousel, J.; Udaykumar, H.S.; Vigmostad, S.C.; McPherson, D.D.; Kim, H.; Chandran, K.B. Synergy between Diastolic Mitral Valve Function and Left Ventricular Flow Aids in Valve Closure and Blood Transport during Systole. Sci. Rep. 2018, 8, 6187. [Google Scholar] [CrossRef]
- Akiyama, K.; Maeda, S.; Matsuyama, T.; Kainuma, A.; Ishii, M.; Naito, Y.; Kinoshita, M.; Hamaoka, S.; Kato, H.; Nakajima, Y.; et al. Vector flow mapping analysis of left ventricular energetic performance in healthy adult volunteers. BMC Cardiovasc. Disord. 2017, 17, 21. [Google Scholar] [CrossRef]
- Charonko, J.J.; Kumar, R.; Stewart, K.; Little, W.C.; Vlachos, P.P. Vortices formed on the mitral valve tips aid normal left ventricular filling. Ann. Biomed. Eng. 2013, 41, 1049–1061. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Huang, L.; Ma, N.; Li, Z.; Han, Y.; Wu, L.; Zhang, X.; Li, Y.; Zhang, H. Relationship between left ventricular vortex and preejectional flow velocity during isovolumic contraction studied by using vector flow mapping. Echocardiography 2019, 36, 558–566. [Google Scholar] [CrossRef]
- Xu, L.; Sun, C.; Zhu, X.; Liu, W.; Ta, S.; Zhao, D.; Wang, F.; Liu, L. Characterization of left ventricle energy loss in healthy adults using vector flow mapping: Preliminary results. Echocardiography 2017, 34, 700–708. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, T.; Itatani, K.; Inuzuka, R.; Shimizu, N.; Shindo, T.; Hirata, Y.; Miyaji, K. Dissipative energy loss within the left ventricle detected by vector flow mapping in children: Normal values and effects of age and heart rate. J. Cardiol. 2015, 66, 403–410. [Google Scholar] [CrossRef]
- Zhong, Y.; Liu, Y.; Wu, T.; Song, H.; Chen, Z.; Zhu, W.; Cai, Y.; Zhang, W.; Bai, W.; Tang, H.; et al. Assessment of Left Ventricular Dissipative Energy Loss by Vector Flow Mapping in Patients with End-Stage Renal Disease. J. Ultrasound Med. 2016, 35, 965–973. [Google Scholar] [CrossRef] [PubMed]
- Abe, H.; Caracciolo, G.; Kheradvar, A.; Pedrizzetti, G.; Khandheria, B.K.; Narula, J.; Sengupta, P.P. Contrast echocardiography for assessing left ventricular vortex strength in heart failure: A prospective cohort study. Eur. Heart J. Cardiovasc. Imaging 2013, 14, 1049–1060. [Google Scholar] [CrossRef]
- Vixege, F.; Courand, P.Y.; Blanc-Benon, P.; Mendez, S.; Nicoud, F.; Vray, D.; Garcia, D. Intraventricular vector flow mapping 3-D by triplane Doppler echocardiography. Comput. Methods Biomech. Biomed. Eng. 2020, 23, S300–S302. [Google Scholar] [CrossRef]
- Sherrid, M.V.; Kushner, J.; Yang, G.; Ro, R. Mitral valve coaptation and its relationship to late diastolic flow: A color Doppler and vector flow map echocardiographic study in normal subjects. Echocardiography 2017, 34, 537–548. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Age Groups | ||||
|---|---|---|---|---|
| 18−29 Years (n = 26) | 30–49 Years (n = 35) | 50 Years or Above (n = 39) | p Value | |
| Age, years | 22.4 ± 2.5 | 41.3 ± 5.8 | 58.0 ± 4.9 | <0.0001 |
| BSA, m2 | 1.68 ± 0.19 | 1.75 ± 0.25 | 1.63 ± 0.16 | 0.097 |
| Female, N (%) | 16 (61.5) | 23 (65.7) | 28 (71.8) | 0.782 |
| LVEDD, mm | 44.1 ± 4.7 | 44.1 ± 4.6 | 43.4 ± 25.1 | 0.886 |
| LVESD, mm | 26.5 ± 4.1 | 26.9 ± 3.6 | 25.1 ± 3.7 | 0.102 |
| LVEDV, mL | 78.8 ± 17.1 | 75.7 ± 19.1 | 24.5 ± 5.8 | 0.117 |
| LVESV, mL | 26.2 ± 5.3 | 25.6 ± 6.9 | 65.4 ± 2.6 | 0.489 |
| LVEF, % | 66.6 ± 2.43 | 66.3 ± 2.3 | 71.7 ± 14.7 | 0.139 |
| E, cm/s | 84.0 ± 19.4 | 75.0 ± 14.5 | 60.6 ± 14.2 | 0.011 |
| A, cm/s | 34.9 ± 13.6 | 53.2 ± 12.4 | 60.6 ± 14.2 | <0.0001 |
| E/A | 2.70 ± 1.11 | 1.48 ± 0.40 | 1.25 ± 0.42 | <0.0001 |
| e’, cm/s | 12.3 ± 0.80 | 9.64 ± 2.07 | 8.68 ± 1.56 | <0.0001 |
| a’, cm/s | 8.28 ±1.58 | 9.54 ± 1.84 | 10.6 ± 1.96 | <0.0001 |
| s’, cm/s | 7.90 ± 1.06 | 7.75 ± 1.14 | 7.77 ± 1.62 | 0.905 |
| e’/a’ | 1.52 ± 0.33 | 1.05 ± 0.30 | 0.845 ± 0.216 | <0.0001 |
| E/e’ | 6.99 ±2.01 | 8.02 ± 1.91 | 8.40 ± 1.82 | <0.0001 |
| Age Groups | ||||
|---|---|---|---|---|
| 18−29 Years (n = 26) | 30–49 Years (n = 35) | 50 Years or Above (n = 39) | p Value | |
| E-Vortex area, mm2 | 405 ± 169 | 354 ± 124 | 345 ± 138 | 0.349 |
| E-Vortex circulation, m2/s | −0.0251 ± 0.0149 | −0.0213 ± 0.0085 | −0.0209 ± 0.0097 | 0.279 |
| A-Vortex area, mm2 | 236 ± 160 | 377 ± 141 | 344 ± 141 | 0.0003 |
| A-Vortex circulation, m2/s | −0.00632 ± 0.00409 | −0.0158 ± 0.0073 | −0.0203 ± 0.0090 | <0.0001 |
| S-Vortex area, mm2 | 478 ± 172 | 453 ± 172 | 397 ± 174 | 0.151 |
| S-Vortex circulation, m2/s | −0.0150 ± 0.0079 | −0.0168 ± 0.0078 | −0.0174 ± 0.0078 | 0.480 |
| Peak ELE, J/m3s | 35.5 ± 17.9 | 24.3 ± 15.8 | 22.2 ± 13.7 | 0.005 |
| Peak ELA, J/m3s | 3.42 ± 2.83 | 8.03 ± 5.71 | 12.3 ± 8.6 | <0.0001 |
| Peak ELS, J/m3s | 10.6 ± 7.2 | 8.54 ± 4.48 | 10.4 ± 6.67 | 0.714 |
| Mean ELD, J/m3s | 9.59 ± 5.52 | 8.96 ± 5.27 | 9.93 ± 5.85 | 0.772 |
| Mean ELS, J/m3s | 4.27 ± 2.60 | 4.30 ± 2.21 | 4.93 ± 2.68 | 0.297 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chan, J.S.K.; Lau, D.H.H.; Fan, Y.; Lee, A.P.-W. Age-Related Changes in Left Ventricular Vortex Formation and Flow Energetics. J. Clin. Med. 2021, 10, 3619. https://doi.org/10.3390/jcm10163619
Chan JSK, Lau DHH, Fan Y, Lee AP-W. Age-Related Changes in Left Ventricular Vortex Formation and Flow Energetics. Journal of Clinical Medicine. 2021; 10(16):3619. https://doi.org/10.3390/jcm10163619
Chicago/Turabian StyleChan, Jeffrey Shi Kai, Dawnie Ho Hei Lau, Yiting Fan, and Alex Pui-Wai Lee. 2021. "Age-Related Changes in Left Ventricular Vortex Formation and Flow Energetics" Journal of Clinical Medicine 10, no. 16: 3619. https://doi.org/10.3390/jcm10163619
APA StyleChan, J. S. K., Lau, D. H. H., Fan, Y., & Lee, A. P.-W. (2021). Age-Related Changes in Left Ventricular Vortex Formation and Flow Energetics. Journal of Clinical Medicine, 10(16), 3619. https://doi.org/10.3390/jcm10163619