
Clinical Outcomes of Early Endoscopic Transpapillary Biliary Drainage for Acute Cholangitis Associated with Disseminated Intravascular Coagulation

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
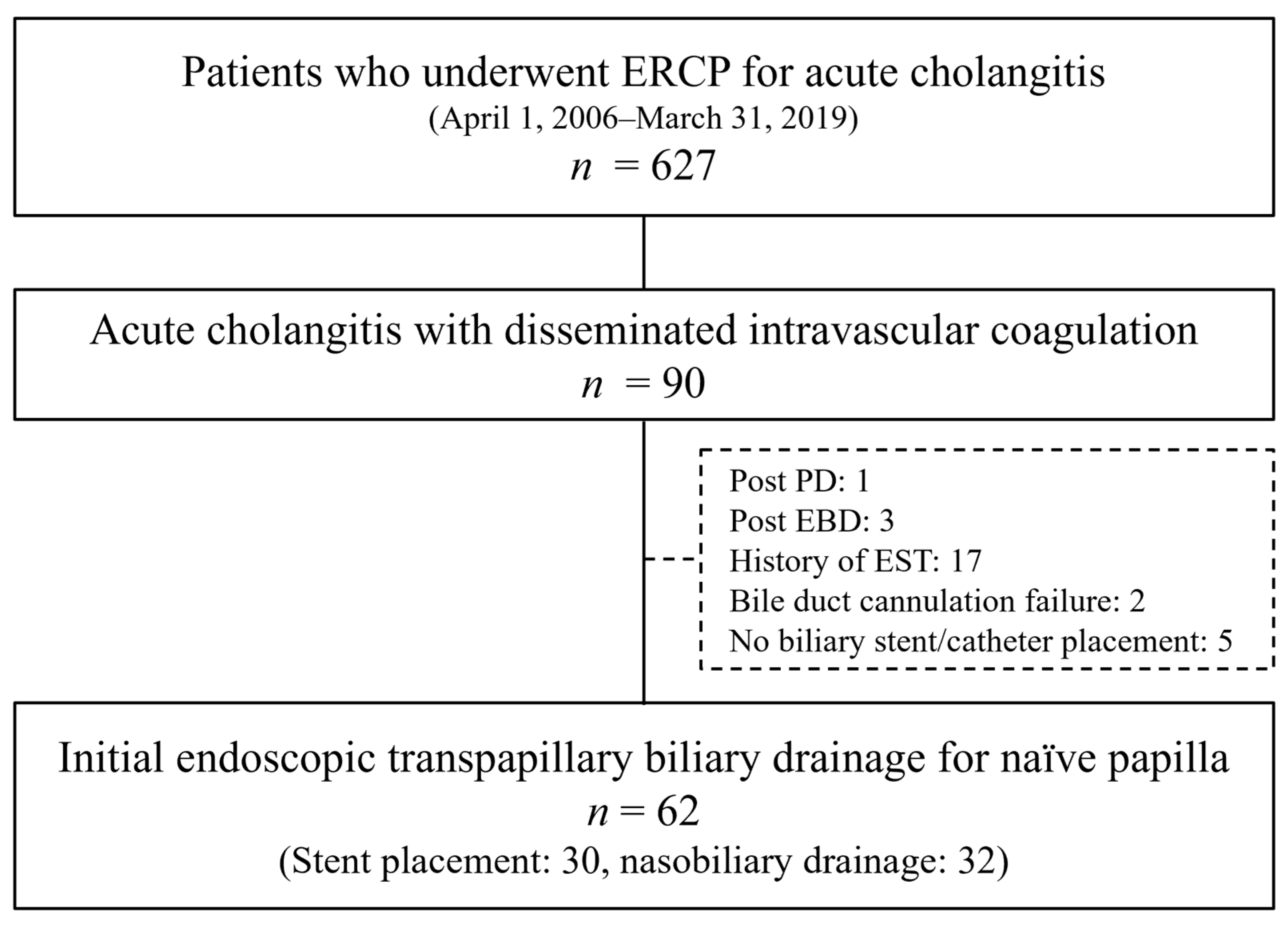
2.1. Patients
2.2. Endoscopic Procedures
2.3. Measurements
2.4. Definitions
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Endoscopic Procedures
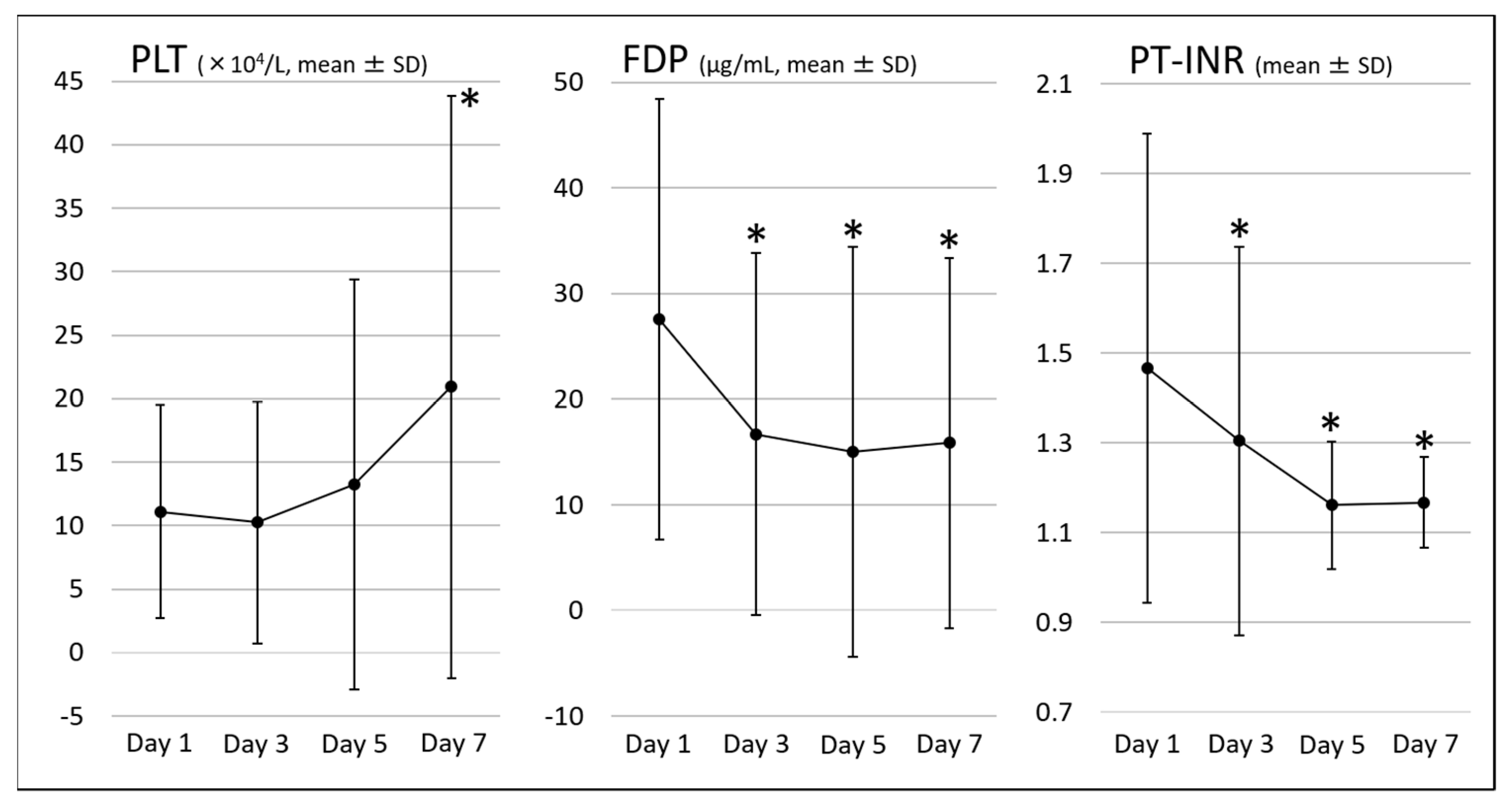
3.3. Clinical Outcomes
3.4. Adverse Events
3.5. Comparison of EBS and ENBD Groups
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wada, H.; Asakura, H.; Okamoto, K.; Iba, T.; Uchiyama, T.; Kawasugi, K.; Koga, S.; Mayumi, T.; Koike, K.; Gando, S.; et al. Expert consensus for the treatment of disseminated intravascular coagulation in Japan. Thromb. Res. 2010, 125, 6–11. [Google Scholar] [CrossRef]
- Miura, F.; Okamoto, K.; Takada, T.; Strasberg, S.M.; Asbun, H.J.; Pitt, H.A.; Gomi, H.; Solomkin, J.S.; Schlossberg, D.; Han, H.S.; et al. Tokyo Guidelines 2018: Initial management of acute biliary infection and flowchart for acute cholangitis. J. Hepatobiliary Pancreat Sci. 2018, 25, 31–40. [Google Scholar] [CrossRef]
- Mukai, S.; Itoi, T.; Baron, T.H.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Ukai, T.; Shikata, S.; Teoh, A.Y.B.; Kim, M.H.; et al. Indications and techniques of biliary drainage for acute cholangitis in updated Tokyo Guidelines 2018. J. Hepatobiliary Pancreat Sci. 2017, 24, 537–549. [Google Scholar] [CrossRef]
- Simmons, D.T.; Petersen, B.T.; Gostout, C.J.; Levy, M.J.; Topazian, M.D.; Baron, T.H. Risk of pancreatitis following endoscopically placed large-bore plastic biliary stents with and without biliary sphincterotomy for management of postoperative bile leaks. Surg. Endosc. 2008, 22, 1459–1463. [Google Scholar] [CrossRef]
- Cui, P.J.; Yao, J.; Zhao, Y.J.; Han, H.Z.; Yang, J. Biliary stenting with or without sphincterotomy for malignant biliary obstruction: A meta-analysis. World J. Gastroenterol. 2014, 20, 14033–14039. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.W.; Chan, A.C.; Lam, Y.H.; Ng, E.K.; Lau, J.Y.; Law, B.K.; Lai, C.W.; Sung, J.J.; Chung, S.C. Biliary decompression by nasobiliary catheter or biliary stent in acute suppurative cholangitis: A prospective randomized trial. Gastrointest Endosc. 2002, 56, 361–365. [Google Scholar] [CrossRef]
- Sharma, B.C.; Kumar, R.; Agarwal, N.; Sarin, S.K. Endoscopic biliary drainage by nasobiliary drain or by stent placement in patients with acute cholangitis. Endoscopy 2005, 37, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Park, S.Y.; Park, C.H.; Cho, S.B.; Yoon, K.W.; Lee, W.S.; Kim, H.S.; Choi, S.K.; Rew, J.S. The safety and effectiveness of endoscopic biliary decompression by plastic stent placement in acute suppurative cholangitis compared with nasobiliary drainage. Gastrointest Endosc. 2008, 68, 1076–1080. [Google Scholar] [CrossRef]
- Kumar, R.; Sharma, B.C.; Singh, J.; Sarin, S.K. Endoscopic biliary drainage for severe acute cholangitis in biliary obstruction as a result of malignant and benign diseases. J. Gastroenterol. Hepatol. 2004, 19, 994–997. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.L.; Cheng, L.; Cai, X.B.; Zhao, H.; Zhu, F.; Wan, X.J. Comparison of the safety and effectiveness of endoscopic biliary decompression by nasobiliary catheter and plastic stent placement in acute obstructive cholangitis. Swiss Med. Wkly. 2013, 143, w13823. [Google Scholar] [CrossRef]
- Kiriyama, S.; Kozaka, K.; Takada, T.; Strasberg, S.M.; Pitt, H.A.; Gabata, T.; Hata, J.; Liau, K.H.; Miura, F.; Horiguchi, A.; et al. Tokyo Guidelines 2018: Diagnostic criteria and severity grading of acute cholangitis (with videos). J. Hepatobiliary Pancreat Sci. 2018, 25, 17–30. [Google Scholar] [CrossRef]
- Gando, S.; Iba, T.; Eguchi, Y.; Ohtomo, Y.; Okamoto, K.; Koseki, K.; Mayumi, T.; Murata, A.; Ikeda, T.; Ishikura, H.; et al. A multicenter, prospective validation of disseminated intravascular coagulation diagnostic criteria for critically ill patients: Comparing current criteria. Crit. Care Med. 2006, 34, 625–631. [Google Scholar] [CrossRef]
- Cotton, P.B.; Lehman, G.; Vennes, J.; Geenen, J.E.; Russell, R.C.; Meyers, W.C.; Liguory, C.; Nickl, N. Endoscopic sphincterotomy complications and their management: An attempt at consensus. Gastrointest Endosc. 1991, 37, 383–393. [Google Scholar] [CrossRef]
- Nakahara, K.; Okuse, C.; Adachi, S.; Suetani, K.; Kitagawa, S.; Okano, M.; Michikawa, Y.; Takagi, R.; Shigefuku, R.; Itoh, F. Use of antithrombin and thrombomodulin in the management of disseminated intravascular coagulation in patients with acute cholangitis. Gut Liver 2013, 7, 363–370. [Google Scholar] [CrossRef][Green Version]
- Suetani, K.; Okuse, C.; Nakahara, K.; Michikawa, Y.; Noguchi, Y.; Suzuki, M.; Morita, R.; Sato, N.; Kato, M.; Itoh, F. Thrombomodulin in the management of acute cholangitis-induced disseminated intravascular coagulation. World J. Gastroenterol. 2015, 21, 533–540. [Google Scholar] [CrossRef]
- Du, L.; Cen, M.; Zheng, X.; Luo, L.; Siddiqui, A.; Kim, J.J. Timing of Performing Endoscopic Retrograde Cholangiopancreatography and Inpatient Mortality in Acute Cholangitis: A Systematic Review and Meta-Analysis. Clin. Transl. Gastroenterol. 2020, 11, e00158. [Google Scholar] [CrossRef] [PubMed]
- Sawas, T.; Arwani, N.; Al Halabi, S.; Vargo, J. Sphincterotomy with endoscopic biliary drainage for severe acute cholangitis: A meta-analysis. Endosc. Int. Open 2017, 5, E103–E109. [Google Scholar] [CrossRef][Green Version]
- Saito, H.; Maruyama, I.; Shimazaki, S.; Yamamoto, Y.; Aikawa, N.; Ohno, R.; Hirayama, A.; Matsuda, T.; Asakura, H.; Nakashima, M.; et al. Efficacy and safety of recombinant human soluble thrombomodulin (ART-123) in disseminated intravascular coagulation: Results of a phase III, randomized, double-blind clinical trial. J. Thromb. Haemost. 2007, 5, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Aikawa, N.; Shimazaki, S.; Yamamoto, Y.; Saito, H.; Maruyama, I.; Ohno, R.; Hirayama, A.; Aoki, Y.; Aoki, N. Thrombomodulin alfa in the treatment of infectious patients complicated by disseminated intravascular coaglation: Subanalysis from the phase 3 trial. Shock 2011, 35, 349–354. [Google Scholar] [CrossRef] [PubMed]
- Vincent, J.L.; Ramesh, M.K.; Ernest, D.; LaRosa, S.P.; Pachl, J.; Aikawa, N.; Hoste, E.; Levy, H.; Hirman, J.; Levi, M.; et al. A randomized, double-blind, placebo-controlled, Phase 2b study to evaluate the safety and efficacy of recombinant human soluble thrombomodulin, ART-123, in patients with sepsis and suspected disseminated intravascular coagulation. Crit. Care Med. 2013, 41, 2069–2079. [Google Scholar] [CrossRef] [PubMed]
- Yamakawa, K.; Aihara, M.; Ogura, H.; Yuhara, H.; Hamasaki, T.; Shimazu, T. Recombinant human soluble thrombomodulin in severe sepsis: A systematic review and meta-analysis. J. Thromb. Haemost. 2015, 13, 508–519. [Google Scholar] [CrossRef] [PubMed]
- Kienast, J.; Juers, M.; Wiedermann, C.J.; Hoffmann, J.N.; Ostermann, H.; Strauss, R.; Keinecke, H.O.; Warren, B.L.; Opal, S.M.; KyberSept Investigators. Treatment effects of high-dose antithrombin without concomitant heparin in patients with severe sepsis with or without disseminated intravascular coagulation. J. Thromb. Haemost. 2006, 4, 90–97. [Google Scholar] [CrossRef] [PubMed]
- Warren, B.L.; Eid, A.; Singer, P.; Pillay, S.S.; Carl, P.; Novak, I.; Chalupa, P.; Atherstone, A.; Pénzes, I.; Kübler, A.; et al. Caring for the critically ill patient. High-dose antithrombin III in severe sepsis: A randomized controlled trial. JAMA 2001, 286, 1869–1878. [Google Scholar] [CrossRef]
- Morita, N.; Nakahara, K.; Morita, R.; Suetani, K.; Michikawa, Y.; Sato, J.; Tsuji, K.; Ikeda, H.; Matsunaga, K.; Watanabe, T.; et al. Efficacy of Combined Thrombomodulin and Antithrombin in Anticoagulant Therapy for Acute Cholangitis-induced Disseminated Intravascular Coagulation. Intern. Med. 2019, 58, 907–914. [Google Scholar] [CrossRef] [PubMed]
- Ogura, T.; Eguchi, T.; Nakahara, K.; Kanno, Y.; Omoto, S.; Itonaga, M.; Kuroda, T.; Hakoda, A.; Ikeoka, S.; Takagi, M.; et al. Clinical impact of recombinant thrombomodulin administration on disseminated intravascular coagulation due to severe acute cholangitis (Recover-AC study). J. Hepatobiliary Pancreat Sci. 2021. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Diagnostic Criteria for Disseminated Intravascular Coagulation | Points |
|---|---|
| Systemic inflammatory response syndrome (SIRS) criteria * | |
| >3 | 1 |
| 0–2 | 0 |
| Platelet count (PLT), ×103/L | |
| <80 or >50% decrease within 24 h | 3 |
| >80 and <120; or >30% decrease within 24 h | 1 |
| >120 | 0 |
| Prothrombin time international-normalized ratio (PT-INR) | |
| >1.2 | 1 |
| <1.2 | 0 |
| Fibrin/fibrinogen degradation products (FDPs), μg/L | |
| >25 | 3 |
| >10 and <25 | 1 |
| <10 | 0 |
| Diagnosis of disseminated intravascular coagulation ≥4 points | |
* Systemic inflammatory response syndrome (SIRS) criteria
| |
| n = 62 | |
|---|---|
| Age (mean ± SD) | 77.7 ± 9.4 |
| Sex (Male/Female) | 40/22 |
| Etiology of acute cholangitis | |
| Bile duct stone/Malignant biliary stricture | 50/12 |
| Severity of acute cholangitis | |
| Mild/Moderate/Severe | 2/10/50 |
| APACHE II score (mean ± SD) | 13.8 ± 6.4 |
| DIC score (mean ± SD) | 5.5 ± 1.3 |
| SIRS score (mean ± SD) | 2.7 ± 1.1 |
| Serum parameters (mean ± SD) | |
| WBC (×103/μL) | 15.2 ± 8.6 |
| CRP (mg/dL) | 13.7 ± 6.4 |
| T-bil (mg/dL) | 4.8 ± 3.1 |
| AST (IU/L) | 312.2 ± 393.6 |
| ALT (IU/L) | 252.4 ± 264.3 |
| Plt (×104/L) | 11.1 ± 8.4 |
| FDP (μg/mL) | 27.6 ± 20.9 |
| PT-INR | 1.47 ± 0.52 |
| Antibiotics | |
| Carbapenem | 46 |
| Sulbactam/Cefoperazone | 8 |
| Tazobactam/Piperacillin | 3 |
| Others | 5 |
| Anticoagulant drugs | |
| Thrombomodulin | 45 |
| Antithrombin | 35 |
| Gabexate | 39 |
| Gamma globulin | 42 |
| n = 62 | |
| Bile duct cannulation | |
| Conventional method | 50 |
| Pancreatic guidewire method | 10 |
| Pancreatic stent placement method | 1 |
| Precut | 1 |
| Procedure for papilla | |
| EST | 7 |
| Incision range (small/moderate) | 3/4 |
| EPBD | 2 |
| Biliary drainage | |
| EBS | 30 |
| ENBD | 32 |
| Stone removal | 4 |
| Use of mechanical lithotripsy | 0 |
| Incidental pancreatography | 29 |
| Prophylactic pancreatic stenting | 13 |
| Procedure time (min, mean ± SD) | 31.4 ± 19.8 |
| n = 62 | |
|---|---|
| Clinical success rate for acute cholangitis (% (n)) | 90.3 (56) |
| DIC resolution rate (% (n)) | 88.7 (55) |
| Number of ERCP sessions (mean ± SD) | 2.0 ± 0.6 |
| Hospitalization period (day, mean ± SD) | 31.7 ± 21.4 |
| Mortality rate (% (n)) | 4.8 (3) |
| n = 62 | |
|---|---|
| Total ERCP-related adverse events (% (n)) | 3.2 (2) |
| Pancreatitis (% (n)) | 0 (0) |
| Bleeding (% (n)) | 3.2 (2) |
| Perforation (% (n)) | 0 (0) |
| Stent dysfunction (% (n)) | 3.2 (2) |
| Hyperamylasemia (% (n)) | 6.4 (4) |
| EBS Group (n = 30) | ENBD Group (n = 32) | p-Value | |
|---|---|---|---|
| Patient backgrounds | |||
| Age (mean ± SD) | 79.2 ± 8.7 | 76.5 ± 9.9 | 0.27 |
| Etiology of acute cholangitis | |||
| Bile duct stone/Malignant disease | 24/6 | 26/6 | 1.00 |
| Severity of acute cholangitis | |||
| Mild/Moderate/Severe | 2/8/20 | 0/2/30 | 0.02 |
| APACHE II score (mean ± SD) | 11.4 ± 3.9 | 16.2 ± 7.4 | <0.01 |
| DIC score (mean ± SD) | 5.1 ± 0.9 | 5.8 ± 1.3 | 0.09 |
| SIRS score (mean ± SD) | 2.3 ± 1.0 | 2.9 ± 1.1 | 0.04 |
| Serum parameters (mean ± SD) | |||
| WBC (×103/μL) | 15.0 ± 8.9 | 15.3 ± 8.6 | 0.90 |
| CRP (mg/dL) | 12.7 ± 6.9 | 14.7 ± 5.8 | 0.23 |
| T-bil (mg/dL) | 3.4 ± 1.7 | 6.0 ± 3.6 | <0.01 |
| AST (IU/L) | 344.0 ± 515.6 | 290.6 ± 240.5 | 0.61 |
| ALT (IU/L) | 268.3 ± 306.6 | 243.5 ± 224.8 | 0.72 |
| Plt (×104/L) | 11.2 ± 5.7 | 11.0 ± 10.4 | 0.90 |
| FDP (μg/mL) | 25.1 ± 15.7 | 29.9 ± 24.9 | 0.41 |
| PT-INR | 1.50 ± 0.71 | 1.43 ± 0.26 | 0.62 |
| Antibiotics | |||
| Carbapenem | 22 | 24 | 0.89 |
| Sulbactam/Cefoperazone | 4 | 4 | 0.78 |
| Tazobactam/Piperacillin | 2 | 1 | 0.95 |
| Others | 2 | 3 | 0.94 |
| Endoscopic procedures | |||
| Conventional cannulation | 24 | 27 | 0.33 |
| EST | 4 | 3 | 1.00 |
| Stone removal | 0 | 4 | 0.11 |
| Procedure time (min, mean ± SD) | 32.5 ± 20.0 | 30.38 ± 19.89 | 0.67 |
| Clinical outcomes | |||
| Clinical success for acute cholangitis (% (n)) | 96.7 (29) | 84.4 (27) | 0.36 |
| DIC resolution rate (% (n)) | 93.3 (28) | 84.4 (27) | 0.67 |
| Number of ERCP sessions (mean ± SD) | 2.0 ± 0.61 | 2.0 ± 0.57 | 0.83 |
| Hospitalization period (mean ± SD) | 27.6 ± 11.8 | 35.6 ± 26.9 | 0.15 |
| Mortality rate (% (n)) | 0 (0) | 9.4 (3) | 0.24 |
| Adverse events | |||
| Bleeding (% (n)) | 3.3 (1) | 3.1 (1) | 1.00 |
| Stent dysfunction (% (n)) | 0 (0) | 6.3 (2) | 0.49 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sekine, A.; Nakahara, K.; Sato, J.; Michikawa, Y.; Suetani, K.; Morita, R.; Igarashi, Y.; Itoh, F. Clinical Outcomes of Early Endoscopic Transpapillary Biliary Drainage for Acute Cholangitis Associated with Disseminated Intravascular Coagulation. J. Clin. Med. 2021, 10, 3606. https://doi.org/10.3390/jcm10163606
Sekine A, Nakahara K, Sato J, Michikawa Y, Suetani K, Morita R, Igarashi Y, Itoh F. Clinical Outcomes of Early Endoscopic Transpapillary Biliary Drainage for Acute Cholangitis Associated with Disseminated Intravascular Coagulation. Journal of Clinical Medicine. 2021; 10(16):3606. https://doi.org/10.3390/jcm10163606
Chicago/Turabian StyleSekine, Akihiro, Kazunari Nakahara, Junya Sato, Yosuke Michikawa, Keigo Suetani, Ryo Morita, Yosuke Igarashi, and Fumio Itoh. 2021. "Clinical Outcomes of Early Endoscopic Transpapillary Biliary Drainage for Acute Cholangitis Associated with Disseminated Intravascular Coagulation" Journal of Clinical Medicine 10, no. 16: 3606. https://doi.org/10.3390/jcm10163606
APA StyleSekine, A., Nakahara, K., Sato, J., Michikawa, Y., Suetani, K., Morita, R., Igarashi, Y., & Itoh, F. (2021). Clinical Outcomes of Early Endoscopic Transpapillary Biliary Drainage for Acute Cholangitis Associated with Disseminated Intravascular Coagulation. Journal of Clinical Medicine, 10(16), 3606. https://doi.org/10.3390/jcm10163606