
Characterization and Prediction of the Clinical Outcome of Intense Pulsed Light-Based Treatment in Dry Eye Associated to Meibomian Gland Dysfunction

 ,
,  ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
- Evaporative dry eye: OSDI (ocular surface disease index) ≥ 13, NIBUT (non-invasive break-up time) < 7 s, tear film osmolarity ≥ 308 mOsm/L, Schirmer I with topical anesthesia ≥ 7 mm in 5 min
- Mixed dry eye: OSDI ≥ 13, NIBUT < 7 s, tear film osmolarity ≥ 308 mOsm/L, Schirmer I with topical anesthesia < 7 mm in 5 min
2.2. Clinical Protocol
2.3. Treatment Sessions
2.4. Data Analysis
3. Results
3.1. Demographics
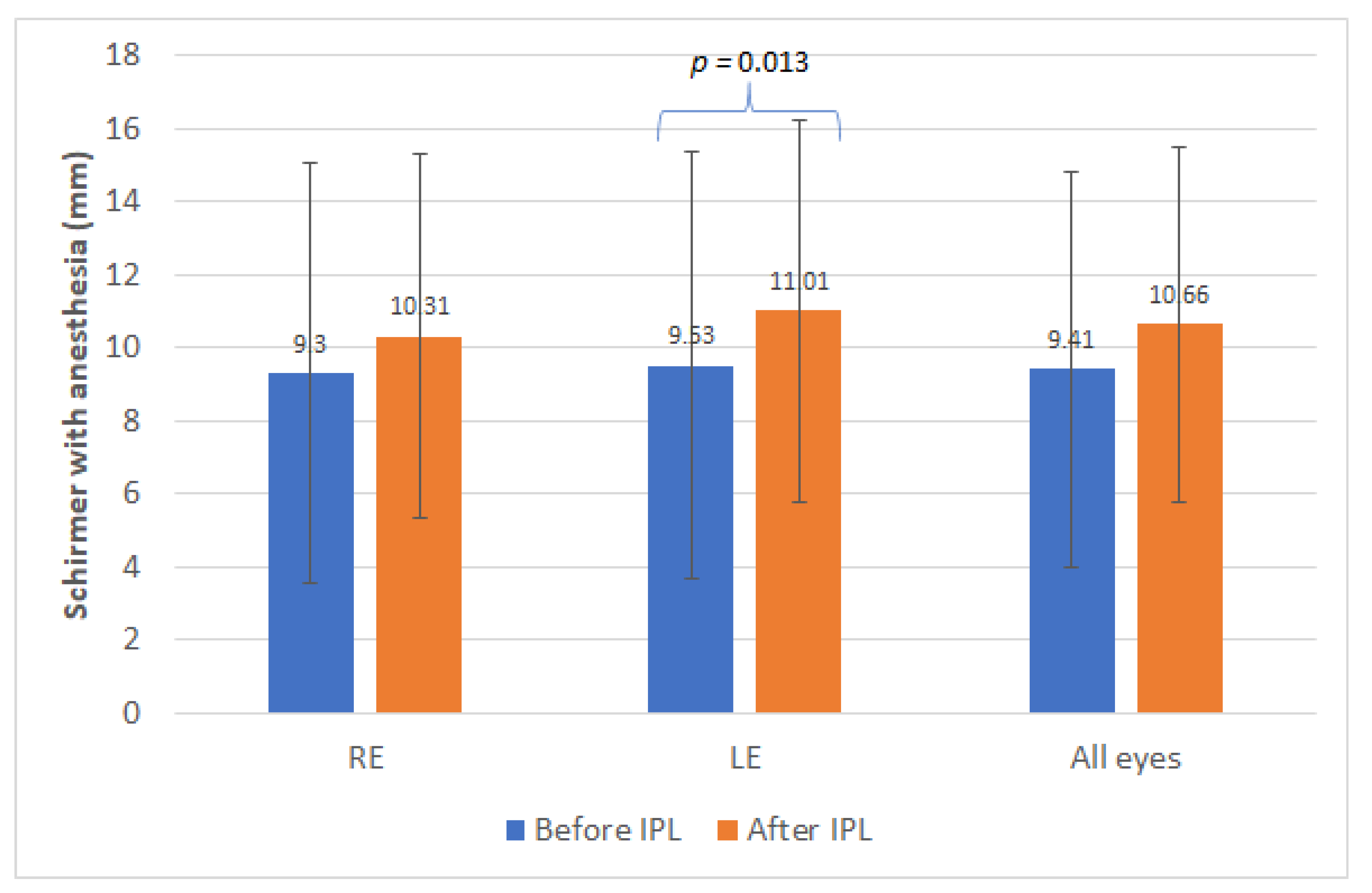
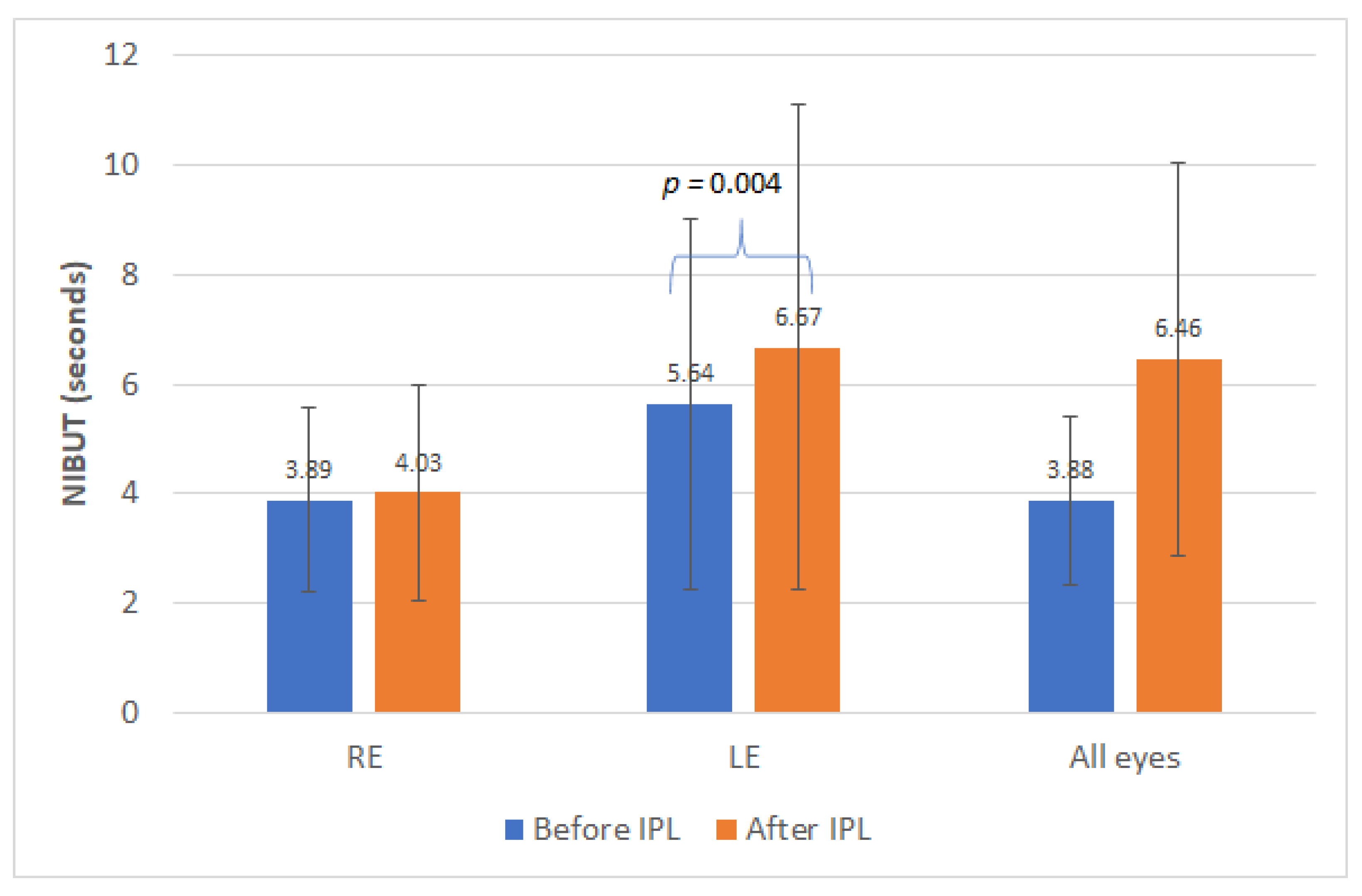
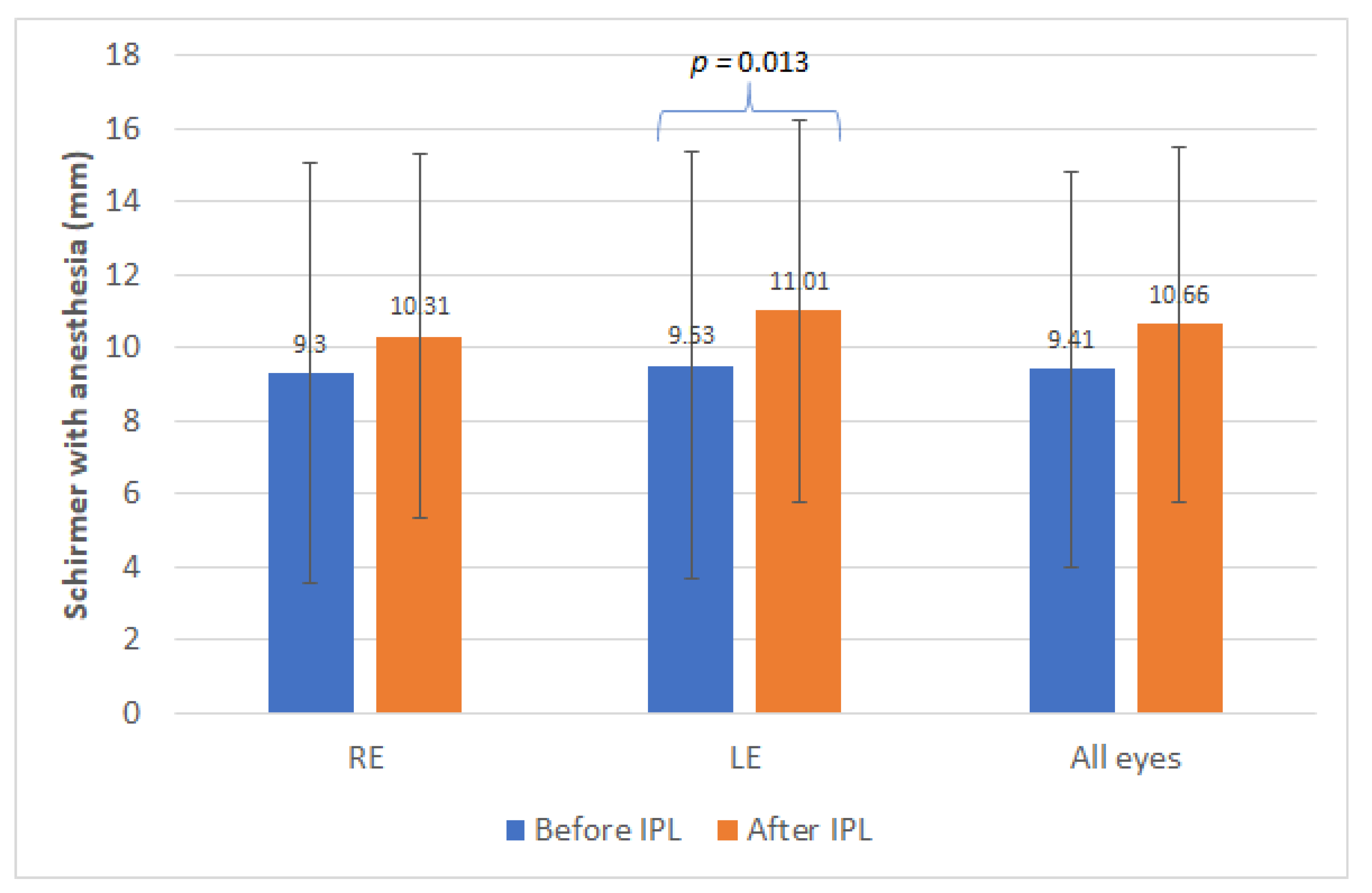
3.2. Changes in Schirmer Test with Anesthesia, NIBUT and Meibomian Losses and Secretions
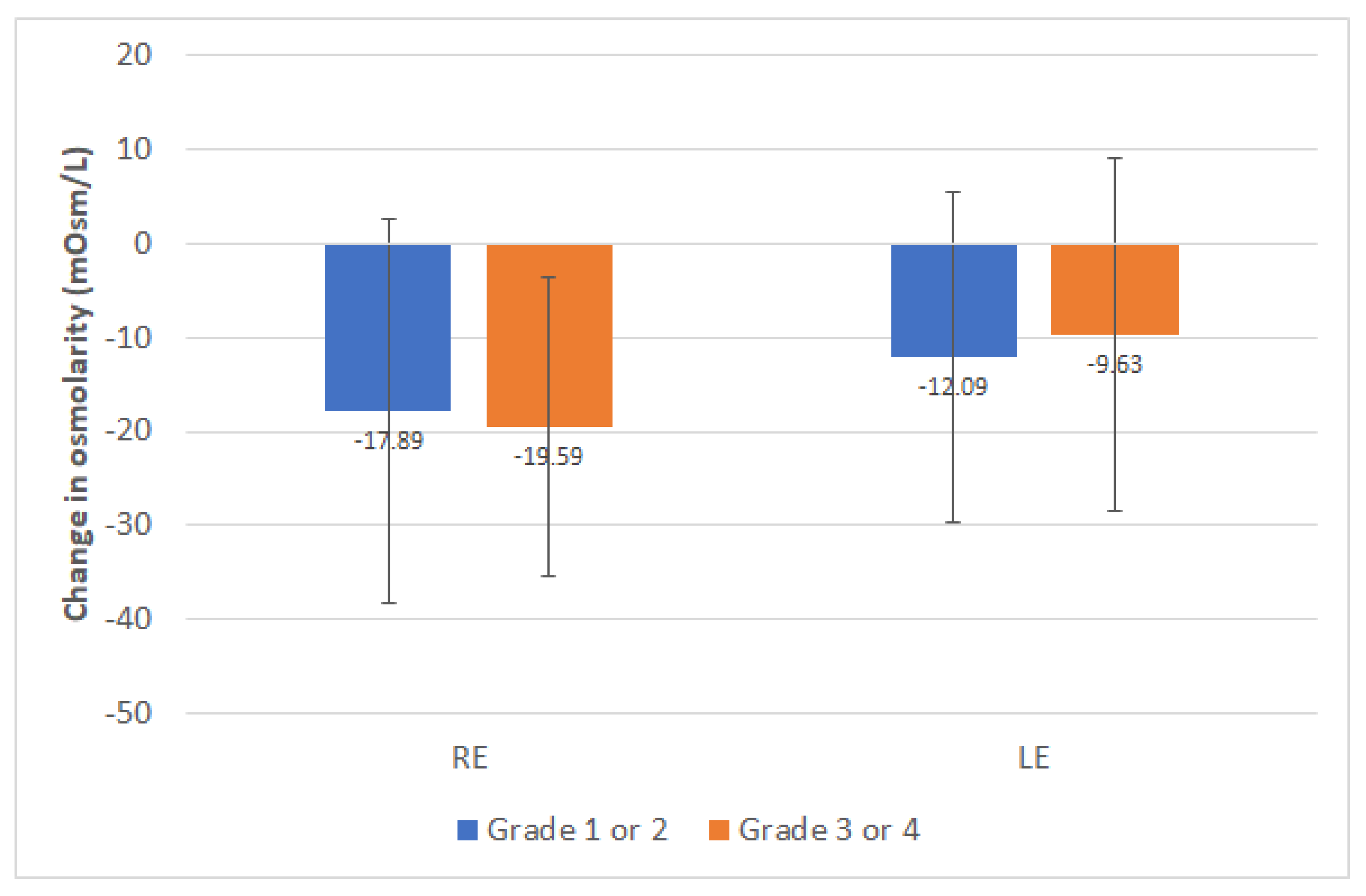
3.3. Changes in Tear Film Osmolarity
3.4. Changes in Symptomatology
3.5. Predictive Model for the Change in Symptomatology with IPL Therapy
3.6. Comparison between Evaporative and Mixed Dry Eye
3.7. Adverse Events
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wat, H.; Wu, D.C.; Rao, J.; Goldman, M.P. Application of intense pulsed light in the treatment of dermatologic disease: A systematic review. Dermatol. Surg. 2014, 40, 359–377. [Google Scholar] [CrossRef]
- Toyos, R.; McGill, W.; Briscoe, D. Intense pulsed light treatment for dry eye disease due to meibomian gland dysfunction; a 3-year retrospective study. Photomed. Laser Surg. 2015, 33, 41–46. [Google Scholar] [CrossRef] [Green Version]
- Seo, K.Y.; Kang, S.M.; Ha, D.Y.; Chin, H.S.; Jung, J.W. Long-term effects of intense pulsed light treatment on the ocular surface in patients with rosacea-associated meibomian gland dysfunction. Contact Lens Anterior Eye 2018, 41, 430–435. [Google Scholar] [CrossRef]
- Sagaser, S.; Butterfield, R.; Kosiorek, H.; Kusne, Y.; Maldonado, J.; Fautsch, M.P.; Patel, D.; Shen, J.F. Effects of intense pulsed light on tear film TGF-β and microbiome in ocular rosacea with dry eye. Clin. Ophthalmol. 2021, 15, 323–330. [Google Scholar] [CrossRef] [PubMed]
- Craig, J.P.; Chen, Y.H.; Turnbull, P.R.K. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Investig. Ophthalmol. Vis. Sci. 2015, 56, 1965–1970. [Google Scholar] [CrossRef] [Green Version]
- Gupta, P.K.; Vora, G.K.; Matossian, C.; Kim, M.; Stinnett, S. Outcomes of intense pulsed light therapy for treatment of evaporative dry eye disease. Can. J. Ophthalmol. 2016, 51, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.; Rong, B.; Tu, P.; Tang, Y.; Song, W.; Toyos, R.; Toyos, M.; Yan, X. Analysis of cytokine levels in tears and clinical correlations after intense pulsed light treating meibomian gland dysfunction. Am. J. Ophthalmol. 2017, 183, 81–90. [Google Scholar] [CrossRef] [Green Version]
- Mejía, L.F.; Gil, J.C.; Jaramillo, M. Intense pulsed light therapy: A promising complementary treatment for dry eye disease. Arch. Soc. Esp. Oftalmol. 2019, 94, 331–336. [Google Scholar] [CrossRef]
- Vigo, L.; Giannaccare, G.; Sebastiani, S.; Pellegrini, M.; Carones, F. Intense pulsed light for the treatment of dry eye owing to meibomian gland dysfunction. J. Vis. Exp. 2019. [Google Scholar] [CrossRef]
- Zhang-Nunes, S.; Guo, S.; Lee, D.; Chang, J.; Nguyen, A. Safety and efficacy of an augmented intense pulsed light protocol for dry eye syndrome and blepharitis. Photobiomodul. Photomed. Laser Surg. 2021, 39, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.; Li, J.; Hu, M.; Zhao, Y.; Lin, X.; Chen, Y.; Li, L.; Zhao, Y.E. Comparison of two intense pulsed light patterns for treating patients with meibomian gland dysfunction. Int. Ophthalmol. 2020, 40, 1695–1705. [Google Scholar] [CrossRef]
- Fan, Q.; Pazo, E.E.; You, Y.; Zhang, C.; Zhang, C.; Xu, L.; He, W. Subjective quality of vision in evaporative dry eye patients after intense pulsed light. Photobiomodul. Photomed. Laser Surg. 2020, 38, 444–451. [Google Scholar] [CrossRef] [PubMed]
- Ocak, S.Y.; Karakus, S.; Ocak, O.B.; Cakir, A.; Bolukbasi, S.; Erden, B.; Bas, E.; Elcioglu, M. Intense pulse light therapy treatment for refractory dry eye disease due to meibomian gland dysfunction. Int. Ophthalmol. 2020, 40, 1135–1141. [Google Scholar] [CrossRef] [PubMed]
- Li, D.; Lin, S.B.; Zhang, M.Z.; Cheng, B. Preliminary assessment of intense pulsed light treatment on the upper eyelids for meibomian gland dysfunction. Photobiomodul. Photomed. Laser Surg. 2020, 38, 249–254. [Google Scholar] [CrossRef] [PubMed]
- Vergés, C.; Salgado-Borges, J.; March de Ribot, F. Prospective evaluation of a new intense pulsed light, thermaeye plus, in the treatment of dry eye disease due to meibomian gland dysfunction. J. Optom. 2021, 14, 103–113. [Google Scholar] [CrossRef]
- Egri, S.; Van Hollebecke, I.; Guindolet, D.; Manenti, C.; Rougier, H.; Gabison, E.; Cochereau, I.; Doan, S. Efficacy of intense pulsed light therapy in the treatment of meibomian gland dysfunction-related severe dry eye. J. Fr. Ophthalmol. 2021, 44, 169–175. [Google Scholar] [CrossRef]
- Dell, S.J.; Gaster, R.N.; Barbarino, S.C.; Cunningham, D.N. Prospective evaluation of intense pulsed light and meibomian gland expression efficacy on relieving signs and symptoms of dry eye disease due to meibomian gland dysfunction. Clin. Ophthalmol. 2017, 11, 817–827. [Google Scholar] [CrossRef] [Green Version]
- Rong, B.; Tang, Y.; Tu, P.; Liu, R.; Qiao, J.; Song, W.; Toyos, R.; Yan, X. Intense pulsed light applied directly on eyelids combined with meibomian gland expression to treat meibomian gland dysfunction. Photomed. Laser Surg. 2018, 36, 326–332. [Google Scholar] [CrossRef]
- Arita, R.; Fukuoka, S.; Morishige, N. Therapeutic efficacy of intense pulsed light in patients with refractory meibomian gland dysfunction. Ocul. Surf. 2019, 17, 104–110. [Google Scholar] [CrossRef]
- Toyos, R.; Toyos, M.; Willcox, J.; Mulliniks, H.; Hoover, J. Evaluation of the safety and efficacy of intense pulsed light treatment with meibomian gland expression of the upper eyelids for dry eye disease. Photobiomodul. Photomed. Laser Surg. 2019, 37, 527–531. [Google Scholar] [CrossRef]
- Chen, Y.; Li, J.; Wu, Y.; Lin, X.; Deng, X.; Yun, Z. Comparative evaluation in intense pulsed light therapy combined with or without meibomian gland expression for the treatment of meibomian gland dysfunction. Curr. Eye Res. 2021, 46, 1125–1131. [Google Scholar] [CrossRef] [PubMed]
- Yan, X.; Hong, J.; Jin, X.; Chen, W.; Rong, B.; Feng, Y.; Huang, X.; Li, J.; Song, W.; Lin, L.; et al. The efficacy of intense pulsed light combined with meibomian gland expression for the treatment of dry eye disease due to meibomian gland dysfunction: A multicenter, randomized controlled trial. Eye Contact Lens 2021, 47, 45–53. [Google Scholar] [CrossRef]
- Wladis, E.J.; Aakalu, V.K.; Foster, J.A.; Freitag, S.K.; Sobel, R.K.; Tao, J.P.; Yen, M.T. Intense pulsed light for meibomian gland disease: A report by the American Academy of Ophthalmology. Ophthalmology 2020, 127, 1227–1233. [Google Scholar] [CrossRef]
- Arita, R.; Fukuoka, S.; Mizoguchi, T.; Morishige, N. Multicenter study of intense pulsed light for patients with refractory aqueous-deficient dry eye accompanied by mild meibomian gland dysfunction. J. Clin. Med. 2020, 9, 3467. [Google Scholar] [CrossRef]
- Pazo, E.E.; Huang, H.; Fan, Q.; Zhang, C.; Yue, Y.; Yang, L.; Xu, L.; Moore, J.E.; He, W. Intense pulse light for treating post-LASIK refractory dry eye. Photobiomodul. Photomed. Laser Surg. 2021, 39, 155–163. [Google Scholar] [CrossRef]
- Fuentes Páez, G.; Soler Tomás, J.R.; Burillo, S. Intense pulsed light: Results in chronic dry eye syndrome after LASIK. Arch. Soc. Esp. Oftalmol. 2020, 95, 226–230. [Google Scholar] [CrossRef]
- Fishman, H.A.; Periman, L.M.; Shah, A.A. Real-time video microscopy of in vitro demodex death by intense pulsed light. Photobiomodul. Photomed. Laser Surg. 2020, 38, 472–476. [Google Scholar] [CrossRef]
- Li, D.; Lin, S.B.; Cheng, B. Intense pulsed light treatment for meibomian gland dysfunction in skin types III/IV. Photobiomodul. Photomed. Laser Surg. 2019, 37, 70–76. [Google Scholar] [CrossRef] [PubMed]
- Schuh, A.; Priglinger, S.; Messmer, E.M. Intense pulsed light (IPL) as a therapeutic option for meibomian gland dysfunction. Ophthalmologe 2019, 116, 982–988. [Google Scholar] [CrossRef]
- Tashbayev, B.; Yazdani, M.; Arita, R.; Fineide, F.; Utheim, T.P. Intense pulsed light treatment in meibomian gland dysfunctions: A concise review. Ocul. Surf. 2020, 18, 583–594. [Google Scholar] [CrossRef]
- Dell, S.J. Intense pulsed light for evaporative dry eye disease. Clin. Ophthalmol. 2017, 11, 1167–1173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pult, H.; Riede-Pult, B. Comparison of subjective grading and objective assessment in meibography. Contact Lens Anterior Eye 2013, 36, 22–27. [Google Scholar] [CrossRef] [PubMed]
- Willcox, M.D.P.; Argüeso, P.; Georgiev, G.A.; Holopainen, J.M.; Laurie, G.V.; Millar, T.J.; Papas, E.B.; Rolland, J.P.; Schmidt, T.A.; Stahl, U.; et al. TFOS DEWS II Tear Film Report. Ocul. Surf. 2017, 15, 366–403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McAlinden, C.; Gao, R.; Wang, Q.; Zhu, S.; Yang, J.; Yu, A.; Bron, A.J.; Huang, J. Rasch analysis of three dry eye questionnaires and correlates with objective clinical tests. Ocul. Surf. 2017, 15, 202–210. [Google Scholar] [CrossRef]
- Ozulken, K.; Aydemir, G.A.; Tekin, K.; Mumcuoğlu, T. Correlation of non-invasive tear break-up time with tear osmolarity and other invasive tear function tests. Semin. Ophthalmol. 2020, 35, 78–85. [Google Scholar] [CrossRef]
- Shehzad, D.; Gorcuyeva, S.; Dag, T.; Bozkurt, B. Novel application software for the semi-automated analysis of infrared meibography images. Cornea 2019, 38, 1456–1464. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dematol. 1998, 124, 869–871. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Mean (SD) Median (Range) | Preoperative | Postoperative | p-Value (Test) |
|---|---|---|---|
| OSDI | 24.59 (9.06) | 13.16 (9.96) | <0.001 |
| 23.00 (15.00 to 50.00) | 10.00 (0.00 to 40.00) | (Paired Student t) | |
| Schirmer with anesthesia (mm) | |||
| RE | 9.30 (5.76) | 10.31 (4.99) | 0.365 |
| 9.00 (0.00 to 25.00) | 10.00 (0.00 to 20.00) | (Wilcoxon) | |
| LE | 9.53 (5.84) | 11.01 (5.21) | 0.013 |
| 9.00 (0.00 to 27.00) | 10.00 (0.00 to 20.00) | (Wilcoxon) | |
| p-value RE vs. LE | 0.464 (Wilcoxon) | 0.134 (Wilcoxon) | |
| All eyes | 9.41 (5.44) | 10.66 (4.86) | 0.058 |
| 9.00 (0.00 to 25.00) | 10.00 (0.00 to 20.00) | (Paired Student t) | |
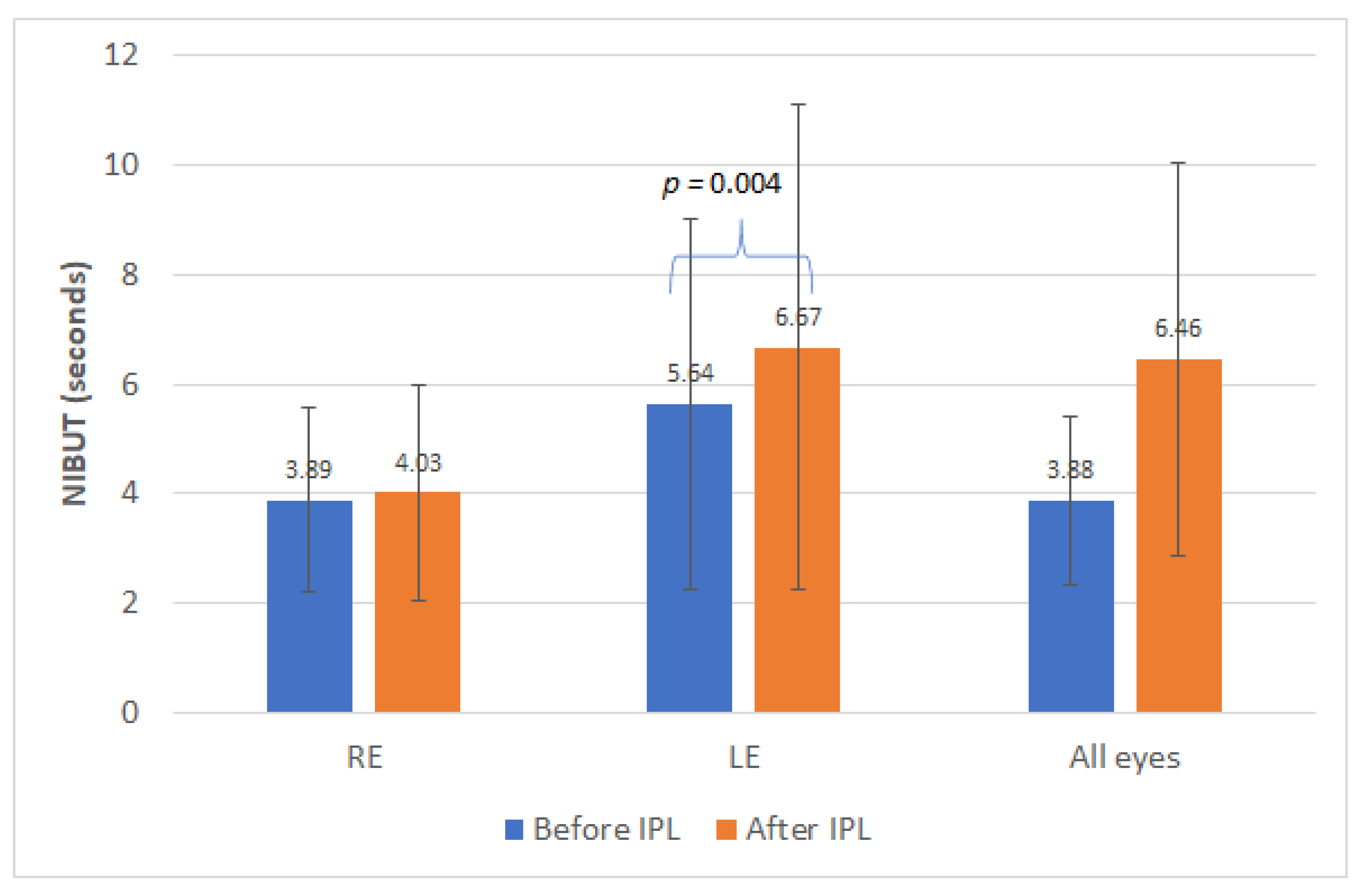
| NIBUT (s) | |||
| RE | 3.89 (1.70) | 5.64 (3.38) | 0.110 |
| 3.80 (1.10 to 6.70) | 4.95 (1.20 to 16.80) | (Wilcoxon) | |
| LE | 4.03 (1.97) | 6.67 (4.44) | 0.004 |
| 3.70 (1.00 to 6.80) | 5.05 (1.00 to 16.80) | (Wilcoxon) | |
| p-value RE vs. LE | 0.759 (Wilcoxon) | 0.071 (Wilcoxon) | |
| All eyes | 3.88 (1.55) | 6.46 (3.60) | <0.001 |
| 3.80 (1.00 to 6.80) | 5.50 (1.20 to 16.80) | (Wilcoxon) | |
| Tear osmolarity (mOsm/L) | |||
| RE | 321.33 (12.30) | 303.54 (14.90) | <0.001 |
| 317.00 (310.00 to 370.00) | 304.00 (236.00 to 336.00) | (Wilcoxon) | |
| LE | 319.27 (12.09) | 307.05 (15.25) | <0.001 |
| 315.00 (310.00 to 359.00) | 307.00 (278.00 to 375.00) | (Wilcoxon) | |
| p-value RE vs. LE | 0.033 (Wilcoxon) | 0.239 (Wilcoxon) | |
| 320.29 (10.44) | 305.23 (11.72) | <0.001 | |
| All eyes | 317.75 (310.00 to 353.00) | 304.50 (276.00 to 337.00) | (Wilcoxon) |
| Meibomian gland loss (grade 1/grade 2/grade 3/grade 4) | |||
| RE | 0.0%/53.4%/44.2%/2.4% | 6.5%/67.7%/25.8%/0.0% | 0.661 (Chi-square) |
| LE | 0.0%/48.5%/47.9%/3.6% | 10.8%/63.4%/24.7%/1.1% | 0.166 (Chi-square) |
| All eyes | 0.0%/50.9%/46.1%/3.0% | 8.6%/65.6%/25.3%/0.5% | 0.077 (Chi-square) |
| Expression of Meibomian glands (clear/yellow/granular/solid) | 15.8%/30.9%/27.9%/25.5% | 22.8%/52.6%/22.8%/1.8% | <0.001 (Chi-square) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iradier, M.T.; del Buey, M.Á.; Peris-Martínez, C.; Cedano, P.; Piñero, D.P. Characterization and Prediction of the Clinical Outcome of Intense Pulsed Light-Based Treatment in Dry Eye Associated to Meibomian Gland Dysfunction. J. Clin. Med. 2021, 10, 3573. https://doi.org/10.3390/jcm10163573
Iradier MT, del Buey MÁ, Peris-Martínez C, Cedano P, Piñero DP. Characterization and Prediction of the Clinical Outcome of Intense Pulsed Light-Based Treatment in Dry Eye Associated to Meibomian Gland Dysfunction. Journal of Clinical Medicine. 2021; 10(16):3573. https://doi.org/10.3390/jcm10163573
Chicago/Turabian StyleIradier, María T., María Ángeles del Buey, Cristina Peris-Martínez, Priscilla Cedano, and David P. Piñero. 2021. "Characterization and Prediction of the Clinical Outcome of Intense Pulsed Light-Based Treatment in Dry Eye Associated to Meibomian Gland Dysfunction" Journal of Clinical Medicine 10, no. 16: 3573. https://doi.org/10.3390/jcm10163573
APA StyleIradier, M. T., del Buey, M. Á., Peris-Martínez, C., Cedano, P., & Piñero, D. P. (2021). Characterization and Prediction of the Clinical Outcome of Intense Pulsed Light-Based Treatment in Dry Eye Associated to Meibomian Gland Dysfunction. Journal of Clinical Medicine, 10(16), 3573. https://doi.org/10.3390/jcm10163573