
Risk Factors Associated with 30-Day Mortality in Older Patients with Influenza

 ,
, 
Abstract
1. Introduction
2. Materials and Methods
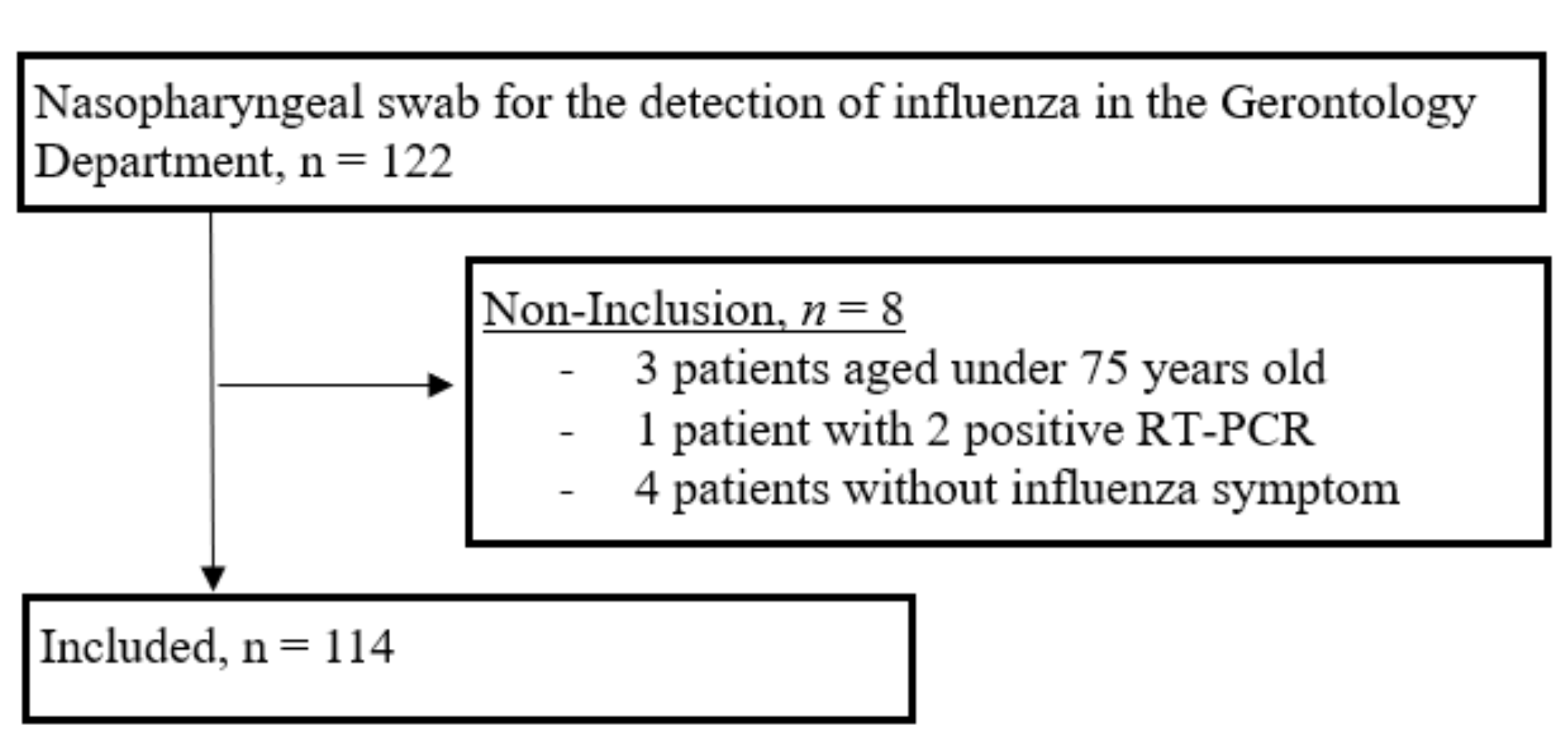
2.1. Study Population
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Factors Associated with Short-Term Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Iuliano, A.D.; Roguski, K.M.; Chang, H.H.; Muscatello, D.J.; Palekar, R.; Tempia, S.; Cohen, C.; Gran, J.M.; Schanzer, D.; Cowling, B.J.; et al. Estimates of global seasonal influenza-associated respiratory mortality: A modelling study. Lancet 2018, 391, 1285–1300. [Google Scholar] [CrossRef]
- Bonmarin, I.; Belchior, E.; Lévy-Bruhl, D. Impact of influenza vaccination on mortality in the French elderly population during the 2000–2009 period. Vaccine 2015, 33, 1099–1101. [Google Scholar] [CrossRef]
- Pop-Vicas, A.; Gravenstein, S. Influenza in the elderly: A mini-review. Gerontology. 2011, 57, 397–404. [Google Scholar] [CrossRef]
- Li, G.; Yilmaz, M.; Kojicic, M.; Fernández-Pérez, E.; Wahab, R.; Huskins, W.C.; Afessa, B.; Truwit, J.D.; Gajic, O. Outcome of critically ill patients with influenza virus infection. J. Clin. Virol. 2009, 46, 275–278. [Google Scholar] [CrossRef] [PubMed]
- Xi, X.; Xu, Y.; Jiang, L.; Li, A.; Duan, J.; Du, B.; Chinese Critical Care Clinical Trial Group (2010). Hospitalized adult patients with 2009 influenza A(H1N1) in Beijing, China: Risk factors for hospital mortality. BMC Infect. Dis. 2010, 10, 256. [Google Scholar] [CrossRef]
- Vandermeer, M.L.; Thomas, A.R.; Kamimoto, L.; Reingold, A.; Gershman, K.; Meek, J.; Farley, M.M.; Ryan, P.; Lynfield, R.; Baumbach, J.; et al. Association between use of statins and mortality among patients hospitalized with laboratory-confirmed influenza virus infections: A multistate study. J. Infect. Dis. 2012, 205, 13–19. [Google Scholar] [CrossRef]
- Chowell, G.; Ayala, A.; Berisha, V.; Viboud, C.; Schumacher, M. Risk factors for mortality among 2009 A/H1N1 influenza hospitalizations in Maricopa County, Arizona, April 2009 to March 2010. Comput. Math. Methods Med. 2012, 2012, 914196. [Google Scholar] [CrossRef] [PubMed]
- Balaganesakumar, S.R.; Murhekar, M.V.; Swamy, K.K.; Kumar, M.R.; Manickam, P.; Pandian, P. Risk factors associated with death among influenza A (H1N1) patients, Tamil Nadu, India, 2010. J. Postgrad. Med. 2013, 59, 9–14. [Google Scholar]
- Ergönül, Ö.; Alan, S.; Ak, Ö.; Sargın, F.; Kantürk, A.; Gündüz, A.; Engin, D.; Öncül, O.; Balkan, I.I.; Ceylan, B.; et al. Predictors of fatality in pandemic influenza A (H1N1) virus infection among adults. BMC Infect. Dis. 2014, 14, 317. [Google Scholar] [CrossRef]
- Shi, S.J.; Li, H.; Liu, M.; Liu, Y.M.; Zhou, F.; Liu, B.; Qu, J.X.; Cao, B. Mortality prediction to hospitalized patients with influenza pneumonia: PO2 /FiO2 combined lymphocyte count is the answer. Clin. Respir. J. 2015, 11, 352–360. [Google Scholar] [CrossRef]
- Mata-Marín, L.A.; Mata-Marín, J.A.; Vásquez-Mota, V.C.; Arroyo-Anduiza, C.I.; Gaytán-Martínez, J.E.; Manjarrez-Téllez, B.; Ochoa-Carrera, L.A.; Sandoval-Ramírez, J.L. Risk factors associated with mortality in patients infected with influenza A/H1N1 in Mexico. BMC Res. Notes 2015, 8, 432. [Google Scholar] [CrossRef]
- Shah, N.S.; Greenberg, J.A.; McNulty, M.C.; Gregg, K.S.; Riddell, J.; Mangino, J.E.; Weber, D.M.; Hebert, C.L.; Marzec, N.S.; Barron, M.A.; et al. Severe Influenza in 33 US Hospitals, 2013–2014: Complications and Risk Factors for Death in 507 Patients. Infect. Control. Hosp. Epidemiol. 2015, 36, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.T.; Chang, C.H.; Hsu, Y.F.; Chuang, J.H. Prognostic factors for mortality in patients hospitalized with influenza complications, in Taiwan. Int. Health 2015, 7, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Cvetanovska, M.; Milenkovik, Z.; Uroshevik, V.K.; Demiri, I.; Cvetanovski, V. Factors Associated with Lethal Outcome in Patients with Severe Form of Influenza. Prilozi 2016, 37, 63–72. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hak, E.; Verheij, T.J.; van Essen, G.A.; Lafeber, A.B.; Grobbee, D.E.; Hoes, A.W. Prognostic factors for influenza-associated hospitalization and death during an epidemic. Epidemiol. Infect. 2001, 126, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Gozalo, P.L.; Pop-Vicas, A.; Feng, Z.; Gravenstein, S.; Mor, V. Effect of influenza on functional decline. J. Am. Geriatr. Soc. 2012, 60, 1260–1267. [Google Scholar] [CrossRef] [PubMed]
- Garnacho-Montero, J.; Gutiérrez-Pizarraya, A.; Màrquez, J.A.; Zaragoza, R.; Granada, R.; Ruiz-Santana, S.; Rello, J.; Rodríguez, A.; Spanish Society of Intensive Care Medicine and Coronary Units Working Group. Epidemiology, clinical features, and prognosis of elderly adults with severe forms of influenza A (H1N1). J. Am. Geriatr. Soc. 2013, 61, 350–356. [Google Scholar] [CrossRef] [PubMed]
- Molbak, K.; Espenhain, L.; Nielsen, J.; Tersago, K.; Bossuyt, N.; Denissov, G.; Baburin, A.; Virtanen, M.; Fouillet, A.; Sideroglou, T.; et al. Excess mortality among the elderly in European countries, December 2014 to February 2015. Eurosurveillance 2015, 20, 21065. [Google Scholar] [CrossRef]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Katz, S.; Downs, T.D.; Cash, H.R.; Grotz, R.C. Progress in development of the index of ADL. Gerontologist 1970, 10, 20–30. [Google Scholar] [CrossRef]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef]
- Mertz, D.; Kim, T.H.; Johnstone, J.; Lam, P.P.; Science, M.; Kuster, S.P.; Fadel, S.A.; Tran, D.; Fernandez, E.; Bhatnagar, N.; et al. Populations at risk for severe or complicated influenza illness: Systematic review and meta-analysis. BMJ 2013, 347, f5061. [Google Scholar] [CrossRef]
- Bürkle, A.; Moreno-Villanueva, M.; Bernhard, J.; Blasco, M.; Zondag, G.; Hoeijmakers, J.H.J.; Toussaint, O.; Grubeck-Loebenstein, B.; Mocchegiani, E.; Collino, S.; et al. MARK-AGE biomarkers of ageing. Mech. Ageing Dev. 2015, 151, 2–12. [Google Scholar] [CrossRef] [PubMed]
- Keef, E.; Zhang, L.A.; Swigon, D.; Urbano, A.; Ermentrout, G.B.; Matuszewski, M.; Toapanta, F.R.; Ross, T.M.; Parker, R.S.; Clermont, G. Discrete Dynamical Modeling of Influenza Virus Infection Suggests Age-Dependent Differences in Immunity. J. Virol. 2017, 91, e00395-17. [Google Scholar] [CrossRef]
- Dobson, J.; Whitley, R.J.; Pocock, S.; Monto, A.S. Oseltamivir treatment for influenza in adults: A meta-analysis of randomised controlled trials. Lancet 2015, 385, 1729–1737. [Google Scholar] [CrossRef]
- Fiore, A.E.; Fry, A.; Shay, D.; Gubareva, L.; Bresee, J.S.; Uyeki, T.M.; Centers for Disease Control and Prevention (CDC) (2011). Antiviral agents for the treatment and chemoprophylaxis of influenza --- recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 2011, 60, 1–24. [Google Scholar]
- Demicheli, V.; Jefferson, T.; Di Pietrantonj, C.; Ferroni, E.; Thorning, S.; Thomas, R.E.; Rivetti, A. Vaccines for preventing influenza in the elderly. Cochrane Database Syst. Rev. 2018, 2, CD004876. [Google Scholar] [CrossRef] [PubMed]
- Beyer, W.E.P.; McElhaney, J.; Smith, D.J.; Monto, A.S.; Nguyen-Van-Tam, J.S.; Osterhaus ADME. Cochrane re-arranged: Support for policies to vaccinate elderly people against influenza. Vaccine 2013, 31, 6030–6033. [Google Scholar] [CrossRef]
- Fireman, B.; Lee, J.; Lewis, N.; Bembom, O.; van der Laan, M.; Baxter, R. Influenza vaccination and mortality: Differentiating vaccine effects from bias. Am. J. Epidemiol. 2009, 170, 650–656. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Total n = 114 | Survivors n = 100 (87.7%) | Non-Survivors n = 14 (12.3%) | Missing Data | p-Value | |
|---|---|---|---|---|---|
| Patient characteristics | |||||
| Age, years, mean, ± SD | 87.9 ± 5.5 | 87.3 ± 5.4 | 91.5 ± 4.7 | - | 0.006 |
| Gender, female, n (%) | 82 (71.9) | 72 (72) | 10 (71.4) | - | 1.000 |
| Charlson Comorbidity Index score, ± SD | 2.83 ± 1.7 | 2.73 ± 1.7 | 3.57 ± 1.7 | - | 0.119 |
| Diabetes, n (%) | 25 (21.9) | 23 (23) | 2 (14.3) | - | 0.731 |
| Chronic renal disease, n (%) | 15 (13.2) | 14 (14) | 1 (7.1) | - | 0.690 |
| Chronic respiratory disease, n (%) | 16 (14) | 13 (13) | 3 (21.4) | - | 0.413 |
| Chronic cardiac disease, n (%) | 37 (32.5) | 29 (29) | 8 (57.1) | - | 0.063 |
| Immunosuppression, n (%) | 17 (14.9) | 15 (15) | 2 (14.3) | - | 1.000 |
| ADL, mean ± SD | 3.08 ± 2.1 | 3.25 ± 2.1 | 1.82 ± 1.7 | - | 0.020 |
| Number of drugs, n ± SD | 6.32 ± 3.0 | 6.15 ± 3.2 | 7.50 ± 1.8 | - | 0.026 |
| Statin therapy, n (%) | 23 (20.2) | 20 (20) | 3 (21.4) | - | 1.000 |
| Vaccination, n (%) | 44 (38.6) | 37 (37) | 7 (50) | 70 (61.4) | 0.576 |
| Influenza infection characteristics | |||||
| Influenza A, n (%) | 107 (93.9) | 93 (93) | 14 (100) | - | 0.594 |
| Delay between diagnosis and the onset of symptoms, days, n ± SD | 2.91 ± 3.5 | 2.94 ± 3.6 | 2.71 ± 2.1 | - | 0.408 |
| Nosocomial infection, n (%) | 35 (30.7) | 32 (32) | 3 (21.4) | - | 0.545 |
| Antiviral < 48 h, n (%) | 48 (42.1) | 45 (45) | 3 (21.4) | - | 0.147 |
| Pneumonia, n (%) | 56 (49.1) | 46 (46) | 10 (71.4) | - | 0.092 |
| Antibiotic prescription, n (%) | 61 (53.5) | 50 (50) | 11 (78.6) | - | 0.051 |
| SOFA score, mean ± SD | 1.3 (1,4) | 1.12 (1.3) | 2.57 (1.6) | - | 0.001 |
| Lymphopenia, n (%) | 77 (73.3) | 66 (66) | 11 (78.6) | 9 (7.9) | 0.506 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| OR (95% CI) | p-Value | OR (95% CI) | p-Value | |
| Age | 1.18 (1.04;1.35) | 0.013 | 1.37 (1.05;1.79) | 0.021 |
| Female | 0.97 (0.28;3.36) | 0.964 | 3.01 (0.31;29.20) | 0.342 |
| Charlson Comorbidity Index | 1.31 (0.96;1.80) | 0.092 | 1.39 (0.78;2.48) | 0.268 |
| Diabetes | 0.56 (0.12;2.68) | 0,466 | 0.60 (0.06;5.91) | 0.662 |
| Chronic respiratory disease | 1.83 (0.45;7.43) | 0.401 | 0.27 (0.02;3.91) | 0.334 |
| Chronic cardiac disease | 3.26 (1.04;10.24) | 0.043 | 6.48 (0.56;74.69) | 0.134 |
| Immunosuppression | 0.94 (0.19;4.65) | 0.944 | 1.62 (0.16;16.40) | 0.683 |
| ADL score | 0.69 (0.50;0.95) | 0.027 | 0.36 (0.17;0.75) | 0.006 |
| Number of drugs | 1.16 (0.96;1.40) | 0.128 | 1.15 (0.83;1.61) | 0.405 |
| Nosocomial infection | 0.58 (0.15;2.22) | 0.426 | 2.17 (0.18;26.76) | 0.545 |
| Antiviral < 48 h | 0.33 (0.09;1.27) | 0.107 | 0.04 (0.002;0.78) | 0.034 |
| Antibiotic prescription | 3.67 (0.97;13.94) | 0.057 | 0.64 (0.07;6.28) | 0.704 |
| SOFA score | 1.83 (1.27;2.64) | 0.001 | 2.30 (1.07;4.94) | 0.034 |
| Lymphopenia | 2.17 (0.45;10.45) | 0.336 | 0.42 (0.04;4.03) | 0.453 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Guesneau, C.; Boureau, A.S.; Bourigault, C.; Berrut, G.; Lepelletier, D.; de Decker, L.; Chapelet, G. Risk Factors Associated with 30-Day Mortality in Older Patients with Influenza. J. Clin. Med. 2021, 10, 3521. https://doi.org/10.3390/jcm10163521
Guesneau C, Boureau AS, Bourigault C, Berrut G, Lepelletier D, de Decker L, Chapelet G. Risk Factors Associated with 30-Day Mortality in Older Patients with Influenza. Journal of Clinical Medicine. 2021; 10(16):3521. https://doi.org/10.3390/jcm10163521
Chicago/Turabian StyleGuesneau, Charles, Anne Sophie Boureau, Céline Bourigault, Gilles Berrut, Didier Lepelletier, Laure de Decker, and Guillaume Chapelet. 2021. "Risk Factors Associated with 30-Day Mortality in Older Patients with Influenza" Journal of Clinical Medicine 10, no. 16: 3521. https://doi.org/10.3390/jcm10163521
APA StyleGuesneau, C., Boureau, A. S., Bourigault, C., Berrut, G., Lepelletier, D., de Decker, L., & Chapelet, G. (2021). Risk Factors Associated with 30-Day Mortality in Older Patients with Influenza. Journal of Clinical Medicine, 10(16), 3521. https://doi.org/10.3390/jcm10163521