
Metformin Use Is Associated with Decreased Mortality in COVID-19 Patients with Diabetes: Evidence from Retrospective Studies and Biological Mechanism


 , ,
, , 
Abstract
:1. Introduction
1.1. Rationale
1.2. Goal of Investigation
1.3. Hypothesis
- Magnitude of the risk of mortality among COVID-19 patients with metformin and those without metformin;
- Difference of magnitude of the risk of mortality among COVID-19 patients in the various continents.
2. Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Statistical Analysis
3. Results
3.1. Literature Search
3.2. Study Characteristics
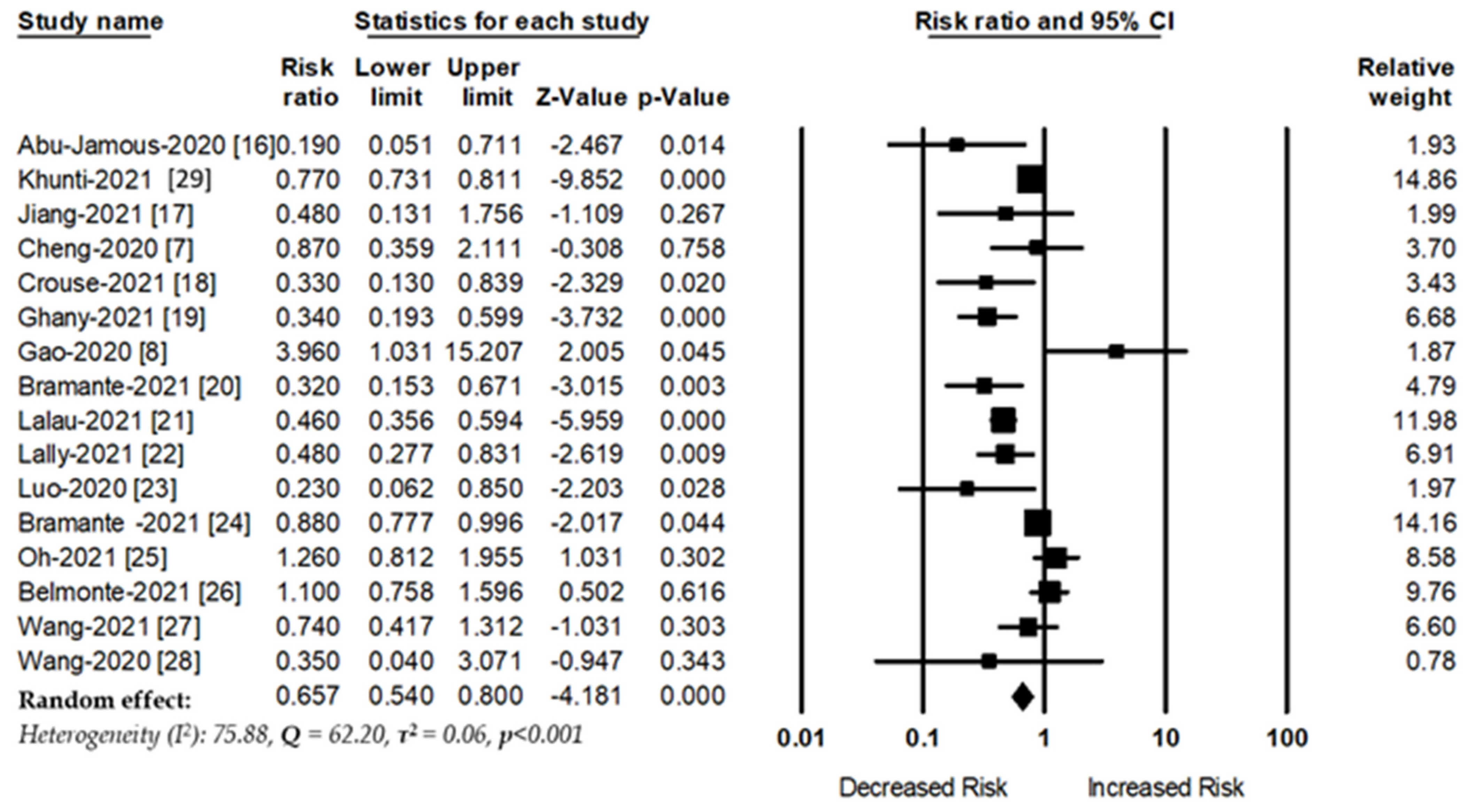
3.3. Primary Analysis
3.3.1. Metformin Use and COVID-19 Mortality
3.3.2. Subgroup Analysis
3.3.3. Sensitivity Analysis
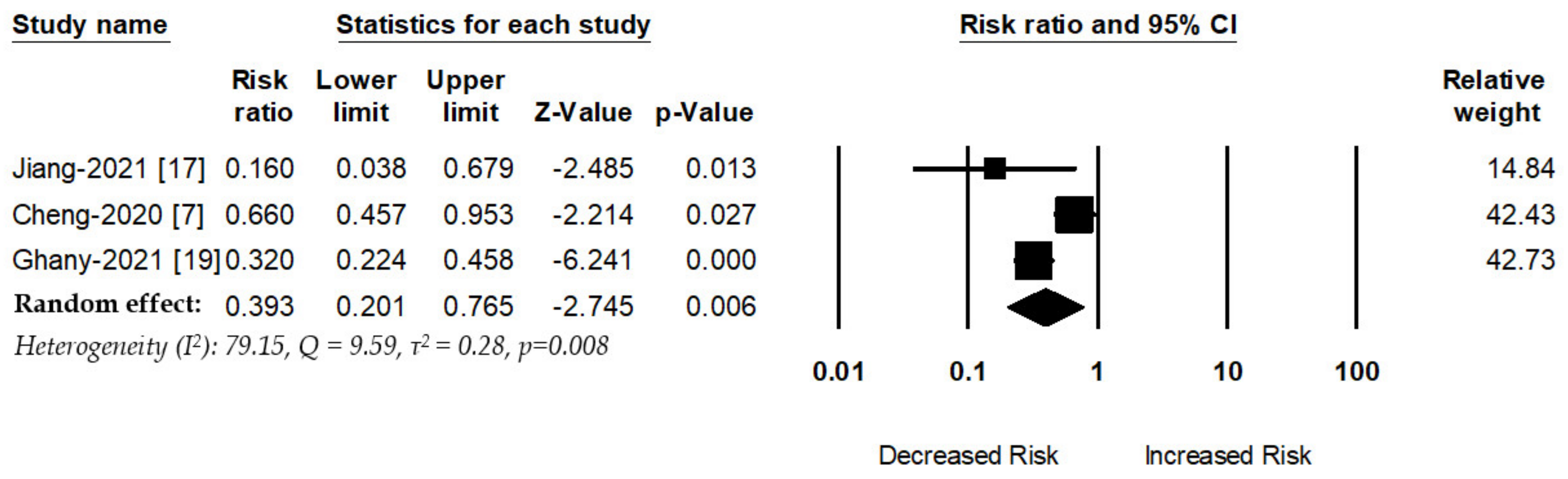
3.4. Secondary Analysis:
Metformin Use and Acute Respiratory Distress Syndrome Risk
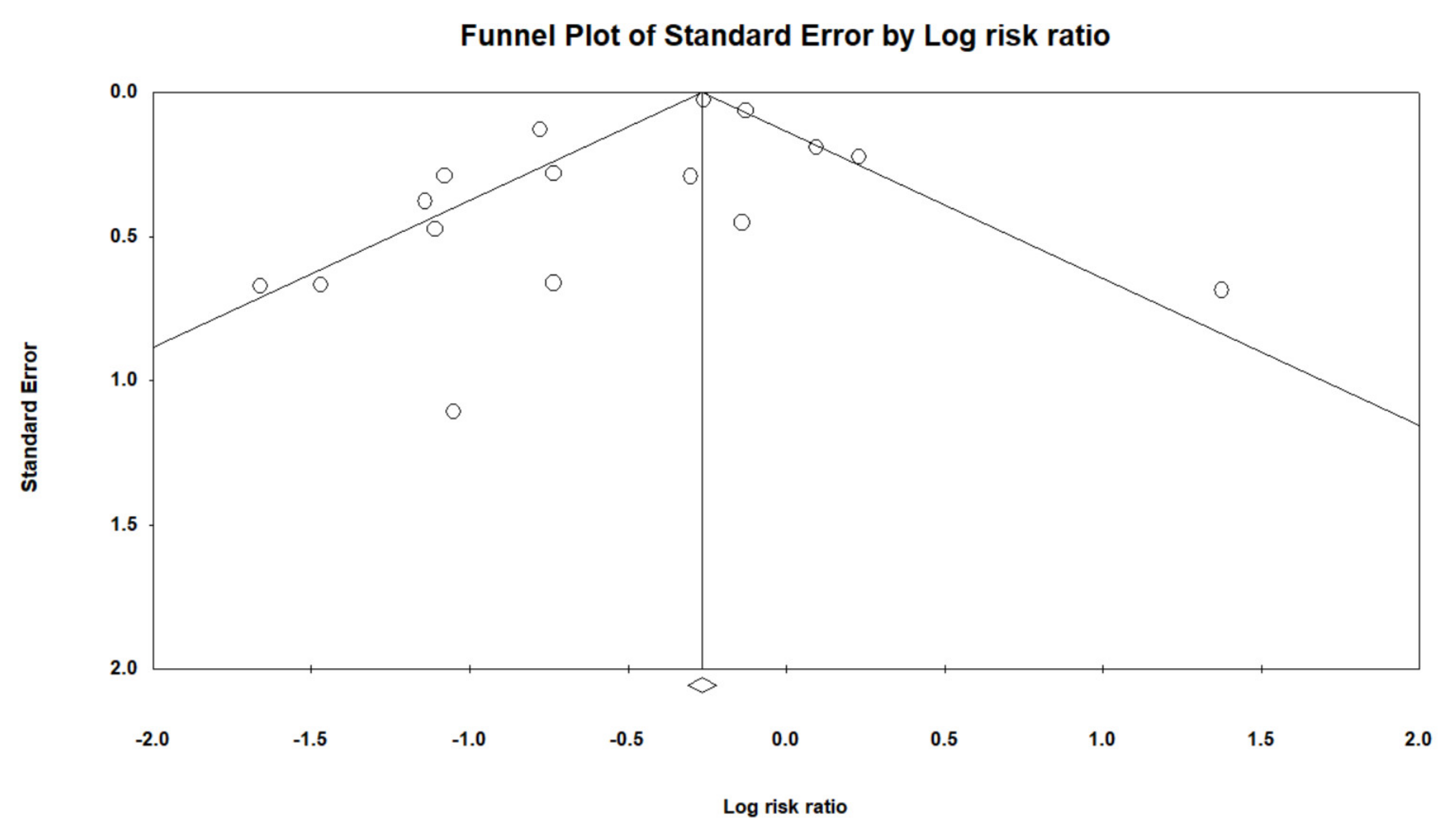
3.5. Publication Bias
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, C.; Horby, P.W.; Hayden, F.G.; Gao, G.F. A novel coronavirus outbreak of global health concern. Lancet 2020, 395, 470–473. [Google Scholar] [CrossRef] [Green Version]
- Yao, X.; Ye, F.; Zhang, M.; Cui, C.; Huang, B.; Niu, P.; Liu, X.; Zhao, L.; Dong, E.; Song, C. In vitro antiviral activity and projection of optimized dosing design of hydroxychloroquine for the treatment of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Clin. Infect. Dis. 2020, 71, 732–739. [Google Scholar] [CrossRef] [Green Version]
- Poly, T.N.; Islam, M.M.; Yang, H.C.; Lin, M.C.; Jian, W.-S.; Hsu, M.-H.; Li, Y.-C.J. Obesity and Mortality Among Patients Diagnosed With COVID-19: A Systematic Review and Meta-Analysis. Front. Med. 2021, 8, 620044. [Google Scholar] [CrossRef]
- Lippi, G.; Wong, J.; Henry, B.M. Hypertension and its severity or mortality in Coronavirus Disease 2019 (COVID-19): A pooled analysis. Pol. Arch. Intern. Med. 2020, 130, 304–309. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Arora, A.; Sharma, P.; Anikhindi, S.A.; Bansal, N.; Singla, V.; Khare, S.; Srivastava, A. Is diabetes mellitus associated with mortality and severity of COVID-19? A meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 535–545. [Google Scholar] [CrossRef] [PubMed]
- Pranata, R.; Huang, I.; Lim, M.A.; Wahjoepramono, E.J.; July, J. Impact of cerebrovascular and cardiovascular diseases on mortality and severity of COVID-19–systematic review, meta-analysis, and meta-regression. J. Stroke Cerebrovasc. Dis. 2020, 29, 104949. [Google Scholar] [CrossRef] [PubMed]
- Cheng, X.; Liu, Y.-M.; Li, H.; Zhang, X.; Lei, F.; Qin, J.-J.; Chen, Z.; Deng, K.-Q.; Lin, L.; Chen, M.-M.; et al. Metformin Is Associated with Higher Incidence of Acidosis, but Not Mortality, in Individuals with COVID-19 and Pre-existing Type 2 Diabetes. Cell Metab. 2020, 32, 537–547.e533. [Google Scholar] [CrossRef]
- Gao, Y.; Liu, T.; Zhong, W.; Liu, R.; Zhou, H.; Huang, W.; Zhang, W. Risk of Metformin in Patients with Type 2 Diabetes with COVID-19: A Preliminary Retrospective Report. Clin. Transl. Sci. 2020, 13, 1055–1059. [Google Scholar] [CrossRef] [PubMed]
- Foretz, M.; Guigas, B.; Viollet, B. Understanding the glucoregulatory mechanisms of metformin in type 2 diabetes mellitus. Nat. Rev. Endocrinol. 2019, 15, 569–589. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Šestan, M.; Marinović, S.; Kavazovic, I.; Cekinović, Đ.; Wueest, S.; Wensveen, T.T.; Brizić, I.; Jonjic, S.; Konrad, D.; Wensveen, F.; et al. Virus-Induced Interferon-γ Causes Insulin Resistance in Skeletal Muscle and Derails Glycemic Control in Obesity. Immunity 2018, 49, 164–177.e166. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andrzejewski, S.; Siegel, P.M.; St-Pierre, J. Metabolic profiles associated with metformin efficacy in cancer. Front. Endocrinol. 2018, 9, 372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siska, P.J.; Rathmell, J.C. T cell metabolic fitness in antitumor immunity. Trends Immunol. 2015, 36, 257–264. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Islam, M.; Iqbal, U.; Walther, B.; Atique, S.; Dubey, N.K.; Nguyen, P.-A.; Poly, T.N.; Masud, J.H.B.; Li, Y.-C.; Shabbir, S.-A. Benzodiazepine Use and Risk of Dementia in the Elderly Population: A Systematic Review and Meta-Analysis. Neuroepidemiology 2016, 47, 181–191. [Google Scholar] [CrossRef]
- Wu, C.C.; Lee, A.J.; Su, C.H.; Huang, C.Y.; Islam, M.; Weng, Y.C. Statin Use Is Associated with a Decreased Risk of Mortality among Patients with COVID-19. J. Clin. Med. 2021, 10, 1450. [Google Scholar] [CrossRef]
- Abu-Jamous, B.; Anisimovich, A.; Baxter, J.; Mackillop, L.; Vizcaychipi, M.P.; McCarthy, A.; Khan, R.T. Associations of comorbidities and medications with COVID-19 outcome: A retrospective analysis of real-world evidence data. medRxiv 2020. [Google Scholar] [CrossRef]
- Jiang, N.; Chen, Z.; Liu, L.; Yin, X.; Yang, H.; Tan, X.; Wang, J.; Li, H.; Tian, M.; Lu, Z.; et al. Association of metformin with mortality or ARDS in patients with COVID-19 and type 2 diabetes: A retrospective cohort study. Diabetes Res. Clin. Pr. 2021, 173, 108619. [Google Scholar] [CrossRef] [PubMed]
- Crouse, A.B.; Grimes, T.; Li, P.; Might, M.; Ovalle, F.; Shalev, A. Metformin Use Is Associated with Reduced Mortality in a Diverse Population with COVID-19 and Diabetes. Front. Endocrinol. 2021, 11, 600439. [Google Scholar] [CrossRef]
- Ghany, R.; Palacio, A.; Dawkins, E.; Chen, G.; McCarter, D.; Forbes, E.; Chung, B.; Tamariz, L. Metformin is associated with lower hospitalizations, mortality and severe coronavirus infection among elderly medicare minority patients in 8 states in USA. Diabetes Metab. Syndr. Clin. Res. Rev. 2021, 15, 513–518. [Google Scholar] [CrossRef] [PubMed]
- Bramante, C.T.; Buse, J.; Tamaritz, L.; Palacio, A.; Cohen, K.; Vojta, D.; Liebovitz, D.; Mitchell, N.; Nicklas, J.; Lingvay, I.; et al. Outpatient metformin use is associated with reduced severity of COVID-19 disease in adults with overweight or obesity. J. Med. Virol. 2021, 93, 4273–4279. [Google Scholar] [CrossRef]
- Lalau, J.-D.; Al-Salameh, A.; Hadjadj, S.; Goronflot, T.; Wiernsperger, N.; Pichelin, M.; Allix, I.; Amadou, C.; Bourron, O.; Duriez, T.; et al. Metformin use is associated with a reduced risk of mortality in patients with diabetes hospitalised for COVID-19. Diabetes Metab. 2021, 47, 101216. [Google Scholar] [CrossRef] [PubMed]
- Lally, M.A.; Tsoukas, P.; Halladay, C.W.; O’Neill, E.; Gravenstein, S.; Rudolph, J.L. Metformin is associated with decreased 30-day mortality among nursing home residents infected with SARS-CoV2. J. Am. Med Dir. Assoc. 2021, 22, 193–198. [Google Scholar] [CrossRef]
- Luo, P.; Qiu, L.; Liu, Y.; Liu, X.-l.; Zheng, J.-l.; Xue, H.-y.; Liu, W.-h.; Liu, D.; Li, J. Metformin treatment was associated with decreased mortality in COVID-19 patients with diabetes in a retrospective analysis. Am. J. Trop. Med. Hyg. 2020, 103, 69–72. [Google Scholar] [CrossRef]
- Bramante, C.T.; Ingraham, N.E.; Murray, T.A.; Marmor, S.; Hovertsen, S.; Gronski, J.; McNeil, C.; Feng, R.; Guzman, G.; Abdelwahab, N.; et al. Metformin and risk of mortality in patients hospitalised with COVID-19: A retrospective cohort analysis. Lancet Health Longev. 2021, 2, e34–e41. [Google Scholar] [CrossRef]
- Oh, T.K.; Song, I.-A. Metformin use and risk of COVID-19 among patients with type II diabetes mellitus: An NHIS-COVID-19 database cohort study. Acta Diabetol. 2021, 58, 771–778. [Google Scholar] [CrossRef]
- Pérez-Belmonte, L.M.; Torres-Peña, J.D.; López-Carmona, M.D.; Ayala-Gutiérrez, M.M.; Fuentes-Jiménez, F.; Huerta, L.J.; Muñoz, J.A.; Rubio-Rivas, M.; Madrazo, M.; Garcia, M.G.; et al. Mortality and other adverse outcomes in patients with type 2 diabetes mellitus admitted for COVID-19 in association with glucose-lowering drugs: A nationwide cohort study. BMC Med. 2020, 18, 359. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Cooper, J.M.; Gokhale, K.; Acosta-Mena, D.; Dhalla, S.; Byne, N.; Chandan, J.S.; Anand, A.; Okoth, K.; Subramanian, A.; et al. Association of Metformin with Susceptibility to COVID-19 in People with Type 2 Diabetes. J. Clin. Endocrinol. Metab. 2021, 106, 1255–1268. [Google Scholar] [CrossRef]
- Wang, B.; Van Oekelen, O.; Mouhieddine, T.H.; Del Valle, D.M.; Richter, J.; Cho, H.J.; Richard, S.; Chari, A.; Gnjatic, S.; Merad, M.; et al. A tertiary center experience of multiple myeloma patients with COVID-19: Lessons learned and the path forward. J. Hematol. Oncol. 2020, 13, 94. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Knighton, P.; Zaccardi, F.; Bakhai, C.; Barron, E.; Holman, N.; Kar, P.; Meace, C.; Sattar, N.; Sharp, S.; et al. Prescription of glucose-lowering therapies and risk of COVID-19 mortality in people with type 2 diabetes: A nationwide observational study in England. Lancet Diabetes Endocrinol. 2021, 9, 293–303. [Google Scholar] [CrossRef]
- Cai, X.-L.; Ji, L.-N. Treatment response between Asian and non-Asian patients with type 2 diabetes: Is there any similarity or difference? Chin. Med. J. 2019, 132, 1. [Google Scholar] [CrossRef]
- Di Xiao, J.Y.; Zhang, S.M.; Liu, R.R.; Yin, J.Y.; Han, X.Y.; Li, X.; Zhang, W.; Chen, X.P.; Zhou, H.H.; Ji, L.N.; et al. A Two-Stage Study Identifies Two Novel Polymorphisms in PRKAG2 Affecting Metformin Response in Chinese Type 2 Diabetes Patients. Pharm. Pers. Med. 2021, 14, 745. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Kurniawan, A. Metformin use is associated with reduced mortality rate from coronavirus disease 2019 (COVID-19) infection. Obes. Med. 2020, 19, 100290. [Google Scholar] [CrossRef] [PubMed]
- Kow, C.S.; Hasan, S. Mortality risk with preadmission metformin use in patients with COVID-19 and diabetes: A meta-analysis. J. Med. Virol. 2021, 93, 695–697. [Google Scholar] [CrossRef] [PubMed]
- Scheen, A.J. Metformin and COVID-19: From cellular mechanisms to reduced mortality. Diabetes Metab. 2020, 46, 423–426. [Google Scholar] [CrossRef]
- Lukito, A.A.; Pranata, R.; Henrina, J.; Lim, M.A.; Lawrensia, S.; Suastika, K. The Effect of Metformin Consumption on Mortality in Hospitalized COVID-19 patients: A systematic review and meta-analysis. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 2177–2183. [Google Scholar] [CrossRef] [PubMed]
- Zangiabadian, M.; Nejadghaderi, S.A.; Zahmatkesh, M.M.; Hajikhani, B.; Mirsaeidi, M.; Nasiri, M.J. The Efficacy and Potential Mechanisms of Metformin in the Treatment of COVID-19 in the Diabetics: A Systematic Review. Front. Endocrinol. 2021, 12, 263. [Google Scholar] [CrossRef]
- Sukumar, M.; Liu, J.; Ji, Y.; Subramanian, M.; Crompton, J.G.; Yu, Z.; Roychoudhuri, R.; Palmer, D.C.; Muranski, P.; Karoly, E.D.; et al. Inhibiting glycolytic metabolism enhances CD8+ T cell memory and antitumor function. J. Clin. Investig. 2013, 123, 4479–4488. [Google Scholar] [CrossRef]
- Jung, T.W.; Lee, M.W.; Lee, Y.J.; Kim, S.M. Metformin prevents endoplasmic reticulum stress-induced apoptosis through AMPK-PI3K-c-Jun NH2 pathway. Biochem. Biophys. Res. Commun. 2012, 417, 147–152. [Google Scholar] [CrossRef]
- Isoda, K.; Young, J.L.; Zirlik, A.; MacFarlane, L.A.; Tsuboi, N.; Gerdes, N.; Schonbeck, U.; Libby, P. Metformin inhibits proinflammatory responses and nuclear factor-κB in human vascular wall cells. Arterioscler. Thromb. Vasc. Biol. 2006, 26, 611–617. [Google Scholar] [CrossRef] [Green Version]
- Siri, M.; Dastghaib, S.; Zamani, M.; Rahmani-Kukia, N.; Geraylow, K.R.; Fakher, S.; Keshvarzi, F.; Mehrbod, P.; Ahmadi, M.; Mokarram, P. Autophagy, Unfolded Protein Response, and Neuropilin-1 Cross-Talk in SARS-CoV-2 Infection: What Can Be Learned from Other Coronaviruses. Int. J. Mol. Sci. 2021, 22, 5992. [Google Scholar] [CrossRef]
- Kaneto, H.; Kimura, T.; Obata, A.; Shimoda, M.; Kaku, K. Multifaceted Mechanisms of Action of Metformin Which Have Been Unraveled One after Another in the Long History. Int. J. Mol. Sci. 2021, 22, 2596. [Google Scholar] [CrossRef] [PubMed]
- Groen, B.B.L.; Hamer, H.M.; Snijders, T.; Van Kranenburg, J.; Frijns, D.; Vink, H.; van Loon, L.J. Skeletal muscle capillary density and microvascular function are compromised with aging and type 2 diabetes. J. Appl. Physiol. 2014, 116, 998–1005. [Google Scholar] [CrossRef] [Green Version]
- Yamaoka-Tojo, M. Endothelial glycocalyx damage as a systemic inflammatory microvascular endotheliopathy in COVID-19. Biomed. J. 2020, 43, 399–413. [Google Scholar] [CrossRef] [PubMed]
- Eskens, B.J.M.; Zuurbier, C.J.; Van Haare, J.; Vink, H.; Van Teeffelen, J.W.G.E. Effects of two weeks of metformin treatment on whole-body glycocalyx barrier properties in db/db mice. Cardiovasc. Diabetol. 2013, 12, 175. [Google Scholar] [CrossRef] [Green Version]
- Targosz-Korecka, M.; Malek-Zietek, K.E.; Kloska, D.; Rajfur, Z.; Stepien, E.Ł.; Grochot-Przeczek, A.; Szymonski, M. Metformin attenuates adhesion between cancer and endothelial cells in chronic hyperglycemia by recovery of the endothelial glycocalyx barrier. Biochim. Biophys. Acta (BBA) Gen. Subj. 2020, 1864, 129533. [Google Scholar] [CrossRef]
- Ceriello, A. Hyperglycemia and the worse prognosis of COVID-19. Why a fast blood glucose control should be mandatory. Diabetes Res. Clin. Pract. 2020, 163, 108186. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A.; De Nigris, V.; Prattichizzo, F. Why is hyperglycaemia worsening COVID-19 and its prognosis? Diabetes Obes. Metab. 2020, 22, 1951–1952. [Google Scholar] [CrossRef]
- Chen, Y.; Gu, F.; Guan, J.-L. Metformin Might Inhibit Virus through Increasing Insulin Sensitivity. Chin. Med. J. 2018, 131, 376–377. [Google Scholar] [CrossRef]
- Sharma, S.; Ray, A.; Sadasivam, B. Metformin in COVID-19: A possible role beyond diabetes. Diabetes Res. Clin. Pr. 2020, 164, 108183. [Google Scholar] [CrossRef]
- Jing, Y.; Wu, F.; Li, D.; Yang, L.; Li, Q.; Li, R. Metformin improves obesity-associated inflammation by altering macrophages polarization. Mol. Cell. Endocrinol. 2018, 461, 256–264. [Google Scholar] [CrossRef]
- Desai, N.; Roman, A.; Rochelson, B.; Gupta, M.; Xue, X.; Chatterjee, P.K.; Tam, H.T.; Metz, C.N. Maternal metformin treatment decreases fetal inflammation in a rat model of obesity and metabolic syndrome. Am. J. Obstet. Gynecol. 2013, 209, 136.e131–136.e139. [Google Scholar] [CrossRef]
- El-Arabey, A.A.; Abdalla, M. Metformin and COVID-19: A novel deal of an old drug. J. Med. Virol. 2020, 92, 2293–2294. [Google Scholar] [CrossRef]
- Seifarth, C.; Schehler, B.; Schneider, H.J. Effectiveness of Metformin on Weight Loss in Non-Diabetic Individuals with Obesity. Exp. Clin. Endocrinol. Diabetes 2012, 121, 27–31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ansari, G.; Mojtahedzadeh, M.; Kajbaf, F.; Najafi, A.; Khajavi, M.R.; Khalili, H.; Rouini, M.R.; Ahmadi, H.; Abdollahi, M. How does blood glucose control with metformin influence intensive insulin protocols? Evidence for involvement of oxidative stress and inflammatory cytokines. Adv. Ther. 2008, 25, 681–702. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Liu, X.; Ye, S. Effects of metformin on blood and urine pro-inflammatory mediators in patients with type 2 diabetes. J. Inflamm. 2016, 13, 34. [Google Scholar] [CrossRef] [PubMed]
- Algire, C.; Moiseeva, O.; Deschênes-Simard, X.; Amrein, L.; Petruccelli, L.; Birman, E.; Viollet, B.; Ferbeyre, G.; Pollak, M.N. Metformin Reduces Endogenous Reactive Oxygen Species and Associated DNA Damage. Cancer Prev. Res. 2012, 5, 536–543. [Google Scholar] [CrossRef] [Green Version]
- Ouslimani, N.; Peynet, J.; Bonnefont-Rousselot, D.; Thérond, P.; Legrand, A.; Beaudeux, J.-L. Metformin decreases intracellular production of reactive oxygen species in aortic endothelial cells. Metabolism 2005, 54, 829–834. [Google Scholar] [CrossRef]
- Hou, X.; Song, J.; Li, X.-N.; Zhang, L.; Wang, X.; Chen, L.; Shen, Y.H. Metformin reduces intracellular reactive oxygen species levels by upregulating expression of the antioxidant thioredoxin via the AMPK-FOXO3 pathway. Biochem. Biophys. Res. Commun. 2010, 396, 199–205. [Google Scholar] [CrossRef]
- Malhotra, A.; Hepokoski, M.; McCowen, K.C.; Shyy, J.Y.-J. ACE2, Metformin, and COVID-19. iScience 2020, 23, 101425. [Google Scholar] [CrossRef]
- Nesti, L.; Natali, A. Metformin effects on the heart and the cardiovascular system: A review of experimental and clinical data. Nutr. Metab. Cardiovasc. Dis. 2017, 27, 657–669. [Google Scholar] [CrossRef]
- Borges, C.M.; Fujihara, C.K.; Malheiros, D.M.A.C.; De Ávila, V.F.; Formigari, G.P.; De Faria, J.B.L. Metformin arrests the progression of established kidney disease in the subtotal nephrectomy model of chronic kidney disease. Am. J. Physiol. Physiol. 2020, 318, F1229–F1236. [Google Scholar] [CrossRef]
- Sturmlechner, I.; Durik, M.; Sieben, C.J.; Baker, D.J.; Van Deursen, J.M. Cellular senescence in renal ageing and disease. Nat. Rev. Nephrol. 2016, 13, 77–89. [Google Scholar] [CrossRef] [PubMed]
- Christensen, M.; Schiffer, T.; Gustafsson, H.; Krag, S.P.; Nørregaard, R.; Palm, F. Metformin attenuates renal medullary hypoxia in diabetic nephropathy through inhibition uncoupling protein-2. Diabetes/Metab. Res. Rev. 2019, 35, e3091. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Ruan, X.-l.; Xue, Y.-x.; Yang, S.; Shi, M.; Wang, L.-n. Metformin reduces the senescence of renal tubular epithelial cells in diabetic nephropathy via the MBNL1/miR-130a-3p/STAT3 pathway. Oxidative Med. Cell. Longev. 2020, 2020, 8708236. [Google Scholar] [CrossRef] [PubMed]
- Dalan, R. Metformin, neutrophils and COVID-19 infection. Diabetes Res. Clin. Pract. 2020, 164, 108230. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, H.; Nomura, N.; Shoda, W.; Isobe, K.; Kikuchi, H.; Yamamoto, K.; Fujimaru, T.; Ando, F.; Mori, T.; Okado, T.; et al. Metformin increases urinary sodium excretion by reducing phosphorylation of the sodium-chloride cotransporter. Metabolism 2018, 85, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Liu, L.; Xu, L.; Xing, Y.; Ye, S. Metformin alleviates renal injury in diabetic rats by inducing Sirt1/FoxO1 autophagic signal axis. Clin. Exp. Pharmacol. Physiol. 2020, 47, 599–608. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author | Country | Design | Data Collection (2020) | Participants | COVID-19 Patients | No. of Metformin Users | Age | Male (%) | Patient Criteria | HR/OR | Outcome (within Days) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Abu-Jamous [16] | UK | Retrospective | 1 January–27 May | 5294 | 1253 | 21 | N/R | N/R | Type-2 | 0.19 (0.05–0.70) | In-hospital (21 days) |
| Khunti [30] | UK | Retrospective | 16 February–31 August | 2,851,465 | 13,479 # | 1,800,005 | Range | 55.9 | Type-2 | 0.77 (0.73–0.81) | In-hospital |
| Jiang [17] | China | Retrospective | 31 December–31 March | 328 | 328 | 100 | 65 | 44.6 | Type-2 | 0.48 (0.13–1.74) | In-hospital (30 days) |
| Cheng [7] | China | Retrospective | 1 January–17 March | 1213 | 1213 | 687 | N/R | N/R | Type-2 | 0.87 (0.36–2.12) | In-hospital (28 days) |
| Crouse [18] | USA | Retrospective | 15 February–22 June | 25,326 | 604 | 239 | Range | 45 | Type-2 | 0.33 (0.13–0.84) | In-hospital |
| Ghany [19] | USA | Retrospective | 1 January–14 August | 1139 | 1139 | 392 | 70.9 | 39 | Type-2 | 0.34 (0.19–0.59) | In-hospital |
| Gao [8] | China | Retrospective | 31 January–20 March | 2399 | 2399 | 56 | Rang | 39.3 | Type-2 | 3.96(1.03–15.19) | In-hospital |
| Bramante [20] | USA | Retrospective | 4 March–4 December | 9555 | 9555 | 342 | 60.4 | 56.2 | Type-2 | 0.32 (0.15–0.66) | In-hospital |
| Lalau [21] | France | Retrospective | 10 March–10 April | 2449 | 2449 | 1496 | 70.9 | 64 | Type-2 | 0.46 (0.36–0.60) | In-hospital (28 days) |
| Lally [22] | USA | Retrospective | 1 March–13 May | 775 | 775 | 39 | 75.6 | 97.3 | Type-2 | 0.48 (0.28, 0.84) | Nursing home (30 days) |
| Luo [23] | China | Retrospective | 27 January–24 March | 283 | 283 | 104 | 63 | 51 | Type-2 | 0.23 (0.06–0.82) | In-hospital |
| Bramante [24] | USA | Retrospective | 1 January–7 June | 6256 | 6256 | 2333 | 73 | 51.6 | Type-2 | 0·88 (0·78–1·00) | In-hospital |
| Oh [25] | Korea | Retrospective | 1 January–4 June | 122,040 | 8070 | 5946 | Range | 44.7 | Type-2 | 1.26 (0.81, 1.95) | In-hospital |
| P. Belmonte [26] | Spain | Retrospective | 1 March–19 July | 2666 | 2666 | 465 | 74.9 | 61.9 | Type-2 | 1.10 (0.76–1.60) | In-hospital |
| Wang #[27] | UK | Retrospective | 30 January–13 October | 71,634 | 39,829 | 59,724 | 64.8 | 61.9 | Type-2 | 0.74 (0.42, 1.32) | In-hospital |
| Wang [28] | USA | Retrospective | 1 March–30 April | 58 | 58 | 9 | 67 | 52 | Type-2 | 0.35 (0.01–3.08) | In-hospital |
| Subgroup | No. of Study | Effect Size | 95% CI | p-Value | I2 | Q-Value | τ2 |
|---|---|---|---|---|---|---|---|
| Nationwide/EHR | 8 | 0.74 | 0.60–0.89 | 0.002 | 80.88 | 36.62 | 0.04 |
| Hospital | 8 | 0.45 | 0.27–0.74 | 0.002 | 58.48 | 16.86 | 0.26 |
| North America | 6 | 0.43 | 0.26–0.72 | 0.01 | 85.57 | 34.65 | 0.31 |
| Europe | 5 | 0.67 | 0.47–0.94 | 0.02 | 82.69 | 23.11 | 0.10 |
| Asia | 5 | 0.90 | 0.43–1.86 | 0.78 | 64.12 | 11.15 | 0.40 |
| Author | Number of Article Included | OR/RR with 95% CI | p-Value | Q | I2 (%) | τ2 | p-Value | Subgroup Analysis |
|---|---|---|---|---|---|---|---|---|
| Scheen 2020 [34] | 4 | 0.75 (0.67–0.85) | – | – | 61 | – | 0.05 | No |
| Hariyanto 2020 [32] | 5 | 0.54 (0.32–0.90) | 0.02 | – | 54 | 0.17 | 0.07 | No |
| Kow 2020 [33] | 5 | 0.62 (0.43–0.89) | – | 5.62 | 29 | – | 0.23 | No |
| Lukito 2020 [35] | 9 | 0.64 (0.43–0.97) | 0.03 | 52.1 | – | – | – | No |
| Our study | 16 | 0.65 (0.54–0.80) | <0.001 | 75.88 | 62.20 | 0.06 | <0.001 | Yes |
| Drug | Mechanism | References |
|---|---|---|
| Metformin | Improve glucose control | [46,47] |
| Increase insulin sensitivity | [48,49] | |
| Improves low-grade inflammation in obesity | [50,51] | |
| Reduction in body weight | [52,53] | |
| Decrease inflammatory cytokines | [54,55] | |
| Decrease reactive oxygen species production | [56,57,58] | |
| Protective arm of the renin-angiotensin-aldosterone system (RAAS) | [49,59,60] | |
| Decrease oxidative stress | [61] | |
| Decrease fibrosis | [62] | |
| Decrease renal hypoxia | [63,64] | |
| Reduction in neutrophils | [65] | |
| Increased urinary sodium excretion and decrease NCC activity | [66] | |
| Increase autophagy and Sirt1/FoxO1 and decrease GBM thickness | [67] | |
| Reduce inflammatory marker release | [39] |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Poly, T.N.; Islam, M.M.; Li, Y.-C.; Lin, M.-C.; Hsu, M.-H.; Wang, Y.-C. Metformin Use Is Associated with Decreased Mortality in COVID-19 Patients with Diabetes: Evidence from Retrospective Studies and Biological Mechanism. J. Clin. Med. 2021, 10, 3507. https://doi.org/10.3390/jcm10163507
Poly TN, Islam MM, Li Y-C, Lin M-C, Hsu M-H, Wang Y-C. Metformin Use Is Associated with Decreased Mortality in COVID-19 Patients with Diabetes: Evidence from Retrospective Studies and Biological Mechanism. Journal of Clinical Medicine. 2021; 10(16):3507. https://doi.org/10.3390/jcm10163507
Chicago/Turabian StylePoly, Tahmina Nasrin, Md. Mohaimenul Islam, Yu-Chuan (Jack) Li, Ming-Chin Lin, Min-Huei Hsu, and Yao-Chin Wang. 2021. "Metformin Use Is Associated with Decreased Mortality in COVID-19 Patients with Diabetes: Evidence from Retrospective Studies and Biological Mechanism" Journal of Clinical Medicine 10, no. 16: 3507. https://doi.org/10.3390/jcm10163507
APA StylePoly, T. N., Islam, M. M., Li, Y.-C., Lin, M.-C., Hsu, M.-H., & Wang, Y.-C. (2021). Metformin Use Is Associated with Decreased Mortality in COVID-19 Patients with Diabetes: Evidence from Retrospective Studies and Biological Mechanism. Journal of Clinical Medicine, 10(16), 3507. https://doi.org/10.3390/jcm10163507