
A Demographic and Regional Comparison of Opioid-Related Hospital Visits within Community Type in the United States

 ,
,  and
and
Abstract
:1. Introduction
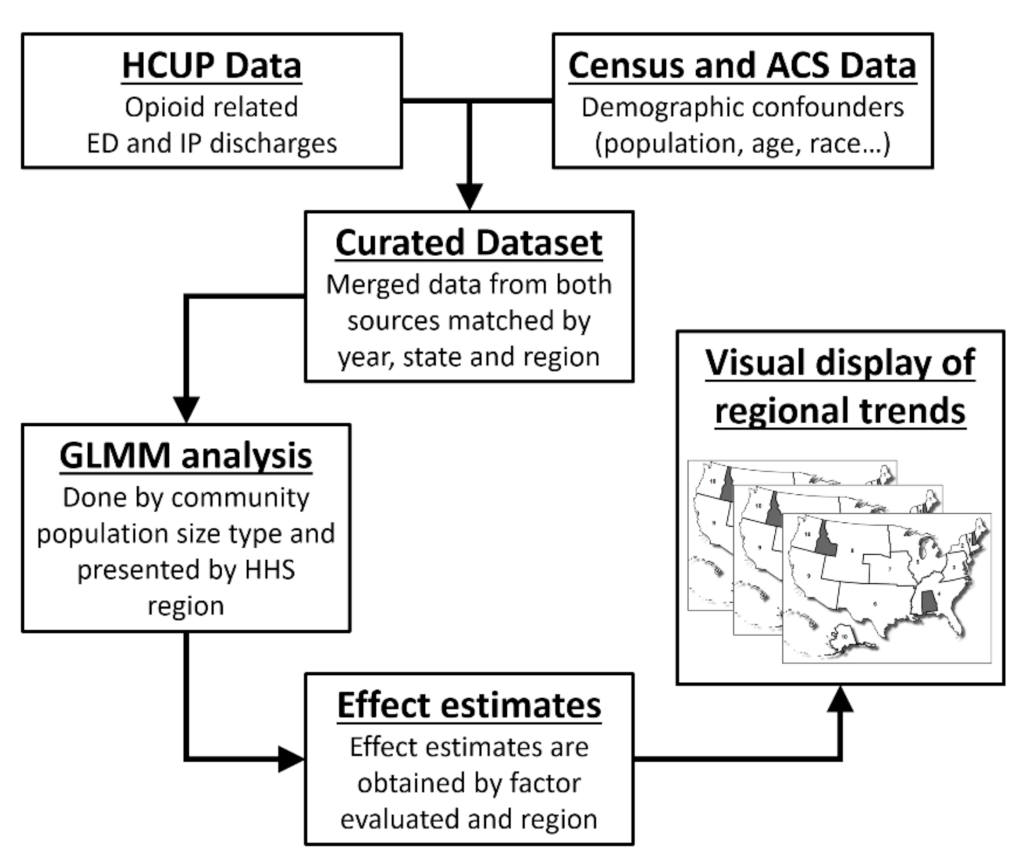
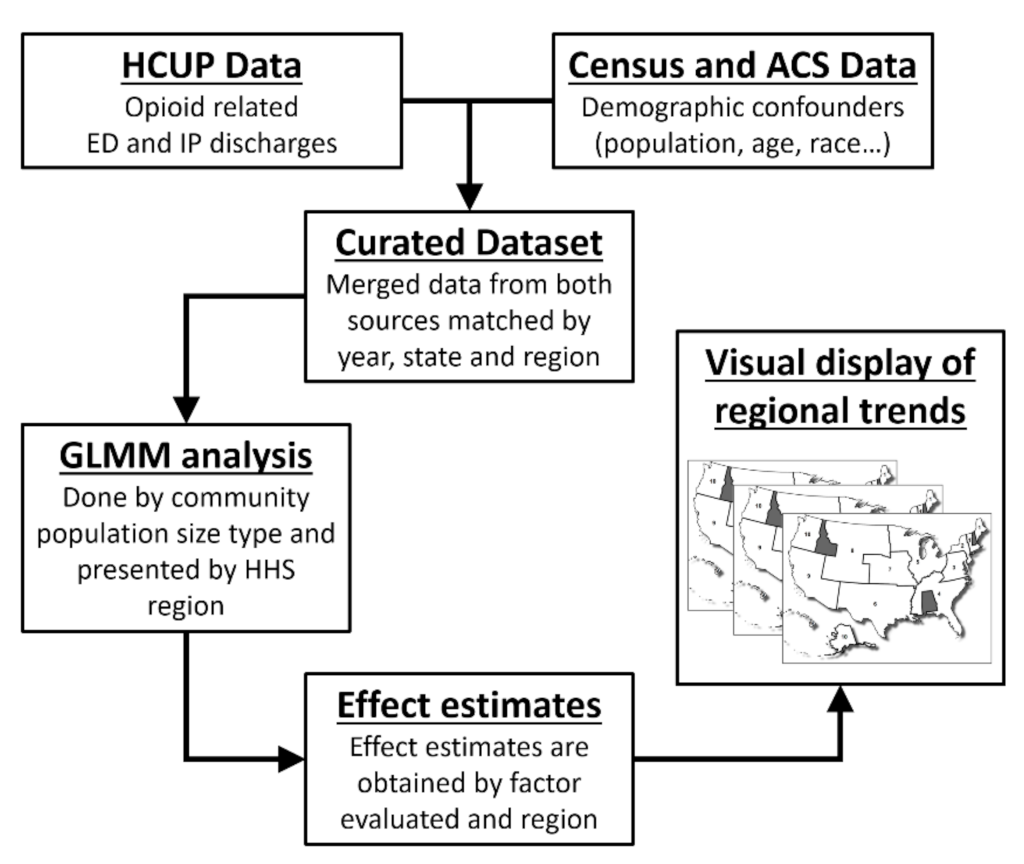
2. Materials and Methods
2.1. Opioid-Related Hospital Visit Data
2.2. Demographic Covariate Data
2.3. Statistical Analysis
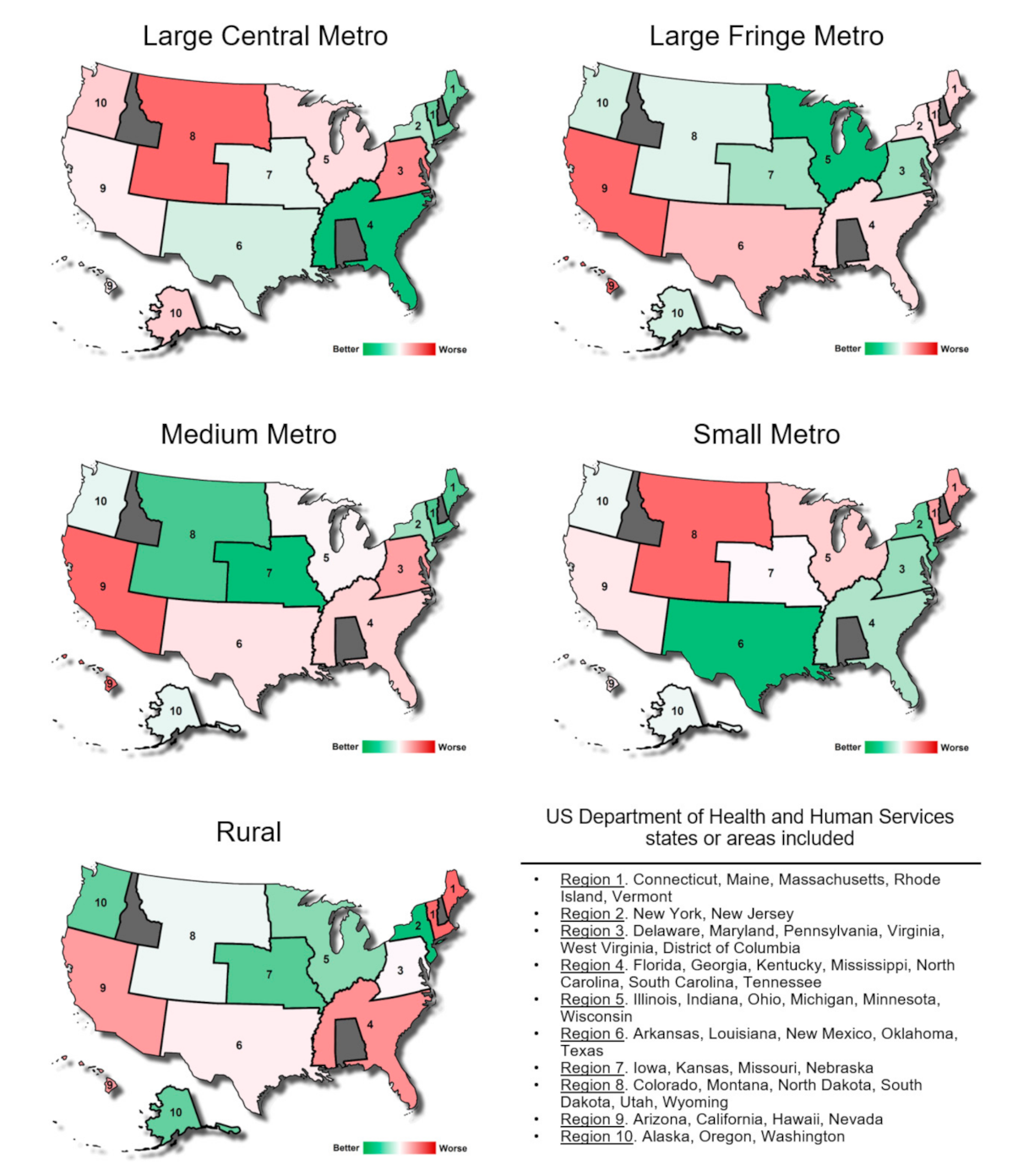
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brennan, F. The US Congressional “Decade on Pain Control and Research” 2001–2011: A Review. J. Pain Palliat. Care Pharmacother. 2015, 29, 212–227. [Google Scholar] [CrossRef] [PubMed]
- Inocencio, T.J.; Carroll, N.V.; Read, E.J.; Holdford, D.A. The Economic Burden of Opioid-Related Poisoning in the United States. Pain Med. 2013, 14, 1534–1547. [Google Scholar] [CrossRef] [Green Version]
- Kolodny, A. How FDA Failures Contributed to the Opioid Crisis. AMA J. Ethics 2020, 22, E743–E750. [Google Scholar] [CrossRef]
- Mattson, C.L.; Tanz, L.J.; Quinn, K.; Kariisa, M.; Patel, P.; Davis, N.L. Trends and Geographic Patterns in Drug and Synthetic Opioid Overdose Deaths—United States, 2013–2019. Morb. Mortal. Wkly. Rep. 2021, 70, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Dowell, D.; Haegerich, T.M.; Chou, R. CDC Guideline for Prescribing Opioids for Chronic Pain—United States, 2016. MMWR Recomm. Rep. 2016, 65, 1–49. [Google Scholar] [CrossRef] [PubMed]
- Thomas, N.; van de Ven, K.; Mulrooney, K.J.D. The impact of rurality on opioid-related harms: A systematic review of qualitative research. Int. J. Drug Policy 2020, 85, 102607. [Google Scholar] [CrossRef] [PubMed]
- Rigg, K.K.; Monnat, S.M.; Chavez, M.N. Opioid-related mortality in rural America: Geographic heterogeneity and intervention strategies. Int. J. Drug Policy 2018, 57, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Palombi, L.C.; St Hill, C.A.; Lipsky, M.S.; Swanoski, M.T.; Lutfiyya, M.N. A scoping review of opioid misuse in the rural United States. Ann. Epidemiol. 2018, 28, 641–652. [Google Scholar] [CrossRef]
- Weiss, A.J.; Elixhauser, A.; Barrett, M.L.; Steiner, C.A.; Bailey, M.K.; O’Malley, L. Opioid-Related Inpatient Stays and Emergency Department Visits by State, 2009–2014. In Statistical Brief #219 [Internet]; 2016. Available online: https://hcup-us.ahrq.gov/reports/statbriefs/sb219-Opioid-Hospital-Stays-ED-Visits-by-State.jsp (accessed on 27 April 2021).
- Cicero, T.J.; Dart, R.C.; Inciardi, J.A.; Woody, G.E.; Schnoll, S.; Muñoz, A. The development of a comprehensive risk-management program for prescription opioid analgesics: Researched abuse, diversion and addiction-related surveillance (RADARS). Pain Med. 2007, 8, 157–170. [Google Scholar] [CrossRef] [Green Version]
- Monnat, S.M.; Peters, D.J.; Berg, M.T.; Hochstetler, A. Using Census Data to Understand County-Level Differences in Overall Drug Mortality and Opioid-Related Mortality by Opioid Type. Am. J. Public Health 2019, 109, 1084–1091. [Google Scholar] [CrossRef]
- Cerdá, M.; Gaidus, A.; Keyes, K.M.; Ponicki, W.; Martins, S.; Galea, S.; Gruenewald, P. Prescription opioid poisoning across urban and rural areas: Identifying vulnerable groups and geographic areas. Addiction 2017, 112, 103–112. [Google Scholar] [CrossRef] [PubMed]
- Jalal, H.; Buchanich, J.M.; Sinclair, D.R.; Roberts, M.S.; Burke, D.S. Age and generational patterns of overdose death risk from opioids and other drugs. Nat. Med. 2020, 26, 699–704. [Google Scholar] [CrossRef] [PubMed]
- Chapman, A.; Verdery, A.M.; Monnat, S.M. Opioid misuse and family structure: Changes and continuities in the role of marriage and children over two decades. Drug Alcohol Depend. 2021, 222, 108668. [Google Scholar] [CrossRef]
- Moriya, A.S.; Xu, L. The complex relationships among race/ethnicity, social determinants, and opioid utilization. Health Serv. Res. 2021, 56, 310–322. [Google Scholar] [CrossRef]
- Park, J.N.; Rouhani, S.; Beletsky, L.; Vincent, L.; Saloner, B.; Sherman, S.G. Situating the Continuum of Overdose Risk in the Social Determinants of Health: A New Conceptual Framework. Milbank Q. 2020, 98, 700–746. [Google Scholar] [CrossRef]
- Schoenfeld, E.R.; Leibowitz, G.S.; Wang, Y.; Chen, X.; Hou, W.; Rashidian, S.; Saltz, M.M.; Saltz, J.H.; Wang, F. Geographic, Temporal, and Sociodemographic Differences in Opioid Poisoning. Am. J. Prev. Med. 2019, 57, 153–164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Florence, C.S.; Zhou, C.; Luo, F.; Xu, L. The Economic Burden of Prescription Opioid Overdose, Abuse, and Dependence in the United States, 2013. Med. Care 2016, 54, 901–906. [Google Scholar] [CrossRef] [PubMed]
- Birnbaum, H.G.; White, A.G.; Schiller, M.; Waldman, T.; Cleveland, J.M.; Roland, C.L. Societal Costs of Prescription Opioid Abuse, Dependence, and Misuse in the United States. Pain Med. 2011, 12, 657–667. [Google Scholar] [CrossRef] [Green Version]
- Owens, P.L.; Weiss, A.J.; Barrett, M.L. Hospital Burden of Opioid-Related Inpatient Stays: Metropolitan and Rural Hospitals, 2016. 2020. Available online: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb258-Opioid-Hospitalizations-Rural-Metro-Hospitals-2016.jsp (accessed on 23 July 2021).
- Vivolo-Kantor, A.M.; Seth, P.; Gladden, R.M.; Mattson, C.L.; Baldwin, G.T.; Kite-Powell, A.; Coletta, M.A. Vital Signs: Trends in Emergency Department Visits for Suspected Opioid Overdoses—United States, July 2016–September 2017. Morb. Mortal. Wkly. Rep. 2018, 67, 279–285. [Google Scholar] [CrossRef] [Green Version]
- Wilson, N.; Kariisa, M.; Seth, P.; Smith, H.; Davis, N.L. Drug and Opioid-Involved Overdose Deaths—United States, 2017–2018. Morb. Mortal. Wkly. Rep. 2020, 69, 290–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- AHRQ. Healthcare Cost and Utilization Project (HCUP). 2019. Available online: https://www.ahrq.gov/data/hcup/index.html (accessed on 27 April 2021).
- Ingram, D.D.; Franco, S.J. 2013 NCHS urban–rural classification scheme for counties. In National Center Health Statistics Vital Health Statistics; 2014; Volume 2. Available online: https://www.cdc.gov/nchs/data/series/sr_02/sr02_166.pdf (accessed on 25 August 2020).
- Services UD of H and H. Regional Offices. 2015. Available online: https://www.hhs.gov/about/agencies/regional-offices/index.html (accessed on 24 July 2021).
- Lippold, K.M.; Jones, C.M.; Olsen, E.O.; Giroir, B.P. Racial/Ethnic and Age Group Differences in Opioid and Synthetic Opioid–Involved Overdose Deaths Among Adults Aged ≥18 Years in Metropolitan Areas—United States, 2015–2017. Morb. Mortal. Wkly. Rep. 2019, 68, 967–973. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Häuser, W.; Schug, S.; Furlan, A.D. The opioid epidemic and national guidelines for opioid therapy for chronic noncancer pain: A perspective from different continents. Pain Rep. 2017, 2, e599. [Google Scholar] [CrossRef]
- Bedene, A.; van Dorp, E.L.A.; Faquih, T.; Cannegieter, S.C.; Mook-Kanamori, D.O.; Niesters, M.; Van Velzen, M.; Gademan, M.G.J.; Rosendaal, F.R.; Bouvy, M.L.; et al. Causes and consequences of the opioid epidemic in the Netherlands: A population-based cohort study. Sci. Rep. 2020, 10, 15309. [Google Scholar] [CrossRef]
- Rosner, B.; Neicun, J.; Yang, J.C.; Roman-Urrestarazu, A. Opioid prescription patterns in Germany and the global opioid epidemic: Systematic review of available evidence. PLoS ONE 2019, 14, e0221153. [Google Scholar] [CrossRef]
- Wilde, M.; Pichini, S.; Pacifici, R.; Tagliabracci, A.; Busardò, F.P.; Auwärter, V.; Solimini, R. Metabolic Pathways and Potencies of New Fentanyl Analogs. Frontiers in Pharmacology. 2019, p. 238. Available online: https://www.frontiersin.org/article/10.3389/fphar.2019.00238 (accessed on 23 July 2021).
- Rose, M.E. Are Prescription Opioids Driving the Opioid Crisis? Assumptions vs Facts. Pain Med. 2018, 19, 793–807. [Google Scholar] [CrossRef] [PubMed]
- Peters, D.J.; Monnat, S.M.; Hochstetler, A.L.; Berg, M.T. The Opioid Hydra: Understanding Overdose Mortality Epidemics and Syndemics Across the Rural-Urban Continuum. Rural Sociol. 2020, 85, 589–622. [Google Scholar] [CrossRef]
- Haffajee, R.L.; Lin, L.A.; Bohnert, A.S.B.; Goldstick, J.E. Characteristics of US Counties With High Opioid Overdose Mortality and Low Capacity to Deliver Medications for Opioid Use Disorder. JAMA Netw. Open 2019, 2, e196373. [Google Scholar] [CrossRef]
- Christie, N.C. The role of social isolation in opioid addiction. Soc. Cogn. Affect. Neurosci. 2021, 16, 645–656. [Google Scholar] [CrossRef] [PubMed]
- Marotta, P.L.; Hunt, T.; Gilbert, L.; Wu, E.; Goddard-Eckrich, D.; El-Bassel, N. Assessing Spatial Relationships between Prescription Drugs, Race, and Overdose in New York State from 2013 to 2015. J. Psychoact. Drugs 2019, 51, 360–370. [Google Scholar] [CrossRef] [PubMed]
- Langabeer, J.R.; Stotts, A.L.; Bobrow, B.J.; Wang, H.E.; Chambers, K.A.; Yatsco, A.J.; Cardenas-Turanzas, M.; Champagne-Langabeer, T. Prevalence and charges of opioid-related visits to U.S. emergency departments. Drug Alcohol Depend. 2021, 221, 108568. [Google Scholar] [CrossRef]
- Jackson, G.; Brown, A.M.; DeFrances, C. No Opioid-involved Emergency Department Visits in the National Hospital Care Survey and the National Hospital Ambulatory Medical Care Survey. In National Health Statistics Reports; 2020; Volume 149. Available online: https://www.cdc.gov/nchs/data/nhsr/nhsr149-508.pdf (accessed on 23 July 2021).
- Davis, C.S.; Lieberman, A.J.; Hernandez-Delgado, H.; Suba, C. Laws limiting the prescribing or dispensing of opioids for acute pain in the United States: A national systematic legal review. Drug Alcohol Depend. 2019, 194, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Kiang, M.V.; Humphreys, K.; Cullen, M.R.; Basu, S. Opioid prescribing patterns among medical providers in the United States, 2003–2017: Retrospective, observational study. BMJ 2020, 368, 16968. [Google Scholar] [CrossRef] [Green Version]
- US Center for Disease Control. U.S. Opioid Dispensing Rate Maps. In Opioid Overdose [Internet]; 2020. Available online: https://www.cdc.gov/drugoverdose/maps/rxrate-maps.html (accessed on 8 June 2021).
- Heslin, K.C.; Owens, P.L.; Karaca, Z.; Barrett, M.L.; Moore, B.J.; Elixhauser, A. Trends in Opioid-related Inpatient Stays Shifted After the US Transitioned to ICD-10-CM Diagnosis Coding in 2015. Med. Care 2017, 55, 918–923. [Google Scholar] [CrossRef] [PubMed]
- Blanco, C.; Wiley, T.R.A.; Lloyd, J.J.; Lopez, M.F.; Volkow, N.D. America’s opioid crisis: The need for an integrated public health approach. Transl. Psychiatry 2020, 10, 167. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Community Size Type | Description |
|---|---|
| Large central netro | Counties in metropolitan statistical areas (MSAs) of 1 million or more population that contain the entire population of the largest principal city of the MSA, have their entire population contained in the largest principal city of the MSA, or contain at least 250,000 inhabitants of any principal city of the MSA. |
| Large fringe metro | Counties in MSAs of 1 million or more population that did not qualify as large central metropolitan counties. |
| Medium metro | Counties in MSAs of populations of 250,000 to 999,999 inhabitants. |
| Small metro | Counties in MSAs of population less than 250,000 inhabitants. |
| Rural | Counties in micropolitan statistical areas and other nonmetropolitan counties. |
| Effect | Rural | Small Metro | Medium Metro | Large Fringe Metro | Large Central Metro | |
|---|---|---|---|---|---|---|
| Year | 0.0173 * | 0.6158 | 0.0978 | 0.0662 | 0.2024 | |
| Region | 0.0068 * | 0.0526 | 0.7631 | 0.0440 * | 0.0220 * | |
| Hospital Setting | 5.6E-10 ** | 3.5E-18 ** | 0.0230 * | 0.6325 | 0.2670 | |
| All Inpatient Stays | 8.3E-63 ** | 1.1E-27 ** | 1.3E-83 ** | 1.1E-83 ** | 3.1E-84 ** | |
| Population | Total population (LN) | 0.9903 | 0.0742 | 0.3347 | 0.0087 * | 0.5864 |
| Population Density | 0.3039 | 0.5301 | 0.1120 | 0.3751 | 0.2355 | |
| Sex Ratio | 0.7881 | 0.6347 | 0.2171 | 0.6009 | 0.0072 * | |
| Age | % Under 25 | 0.3341 | 0.0391 * | 0.3676 | 0.1979 | 0.5547 |
| % 25 to 65 | 0.9127 | 0.3929 | 0.3521 | 0.0462 * | 0.3990 | |
| % 65 and over | 0.4891 | 0.1442 | 0.2020 | 1.0000 | 1.0000 | |
| Race | % White Alone | 0.7485 | 0.0239 * | 0.0495 * | 0.4587 | 0.0447 * |
| % African-American | 0.9024 | 0.0681 | 0.0711 | 0.7270 | 0.0694 | |
| % Asian | 0.3011 | 0.1842 | 0.0080 * | 0.8004 | 0.0348 * | |
| % Native American | 0.8485 | 0.0038 * | 0.0052 * | 0.8062 | 0.0311 * | |
| % Hispanic | 0.9594 | 0.0603 | 0.0607 | 0.8827 | 0.0561 | |
| Education | % No High School | 0.8248 | 0.5890 | 0.2024 | 0.2893 | 0.7425 |
| % High School | 0.4069 | 0.7209 | 0.2026 | 0.5208 | 0.7715 | |
| % Some College | 0.2828 | 0.6936 | 0.1957 | 0.2164 | 0.7529 | |
| % Bachelors or more | 0.4021 | 0.9609 | 0.5795 | 0.7986 | 0.5975 | |
| Income | Household Adjusted Income | 0.9076 | 0.4611 | 0.0033 * | 0.9670 | 0.9979 |
| % Poverty Level | 0.3760 | 0.1402 | 0.7839 | 0.6598 | 0.7576 | |
| % Unemployment | 0.4837 | 0.0005 * | 0.0120 * | 0.3315 | 3.5E-5 ** | |
| Effect by Population Type | Estimate | Standard Error | 95% Confidence Limits |
|---|---|---|---|
| Rural | |||
| Hospital Setting ED vs ID | −0.7219 | 0.114 | (−0.946, −0.498) |
| All Inpatient Stays | 0.021 | 0.001 | (0.019, 0.024) |
| Small Metro | |||
| Hospital Setting ED vs ID | −1.4378 | 0.159 | (−1.750, −1.125) |
| All Inpatient Stays | 0.018 | 0.002 | (0.015, 0.021) |
| % Under 25 | −0.9129 | 0.442 | (−1.780, −0.046) |
| % White Alone | −0.7876 | 0.348 | (−1.471, −0.105) |
| % Native American | −1.2863 | 0.443 | (−2.157, −0.416) |
| % Unemployment | −0.3691 | 0.105 | (−0.575, −0.163) |
| Medium Metro | |||
| Hospital Setting ED vs. ID | −0.2493 | 0.109 | (−0.464, −0.034) |
| All Inpatient Stays | 0.026 | 0.001 | (0.024, 0.028) |
| % White Alone | 0.548 | 0.278 | (0.001, 1.094) |
| % Asian | 1.021 | 0.384 | (0.267, 1.775) |
| % Native American | 1.054 | 0.376 | (0.316, 1.792) |
| Household Adjusted Income | −0.00012 | 0.00004 | (−0.00021, −0.00004) |
| % Unemployment | −0.1874 | 0.074 | (−0.334, −0.041) |
| Large Fringe Metro | |||
| All Inpatient Stays | 0.027 | 0.001 | (0.025, 0.029) |
| Total population (LN) | 2.131 | 0.809 | (0.541, 3.722) |
| % 25 to 65 | 0.548 | 0.274 | (0.009, 1.086) |
| Large Central Metro | |||
| All Inpatient Stays | 0.039 | 0.002 | (0.036, 0.042) |
| Sex Ratio | −82.7949 | 30.670 | (−143.090, −22.496) |
| % White Alone | −0.953 | 0.473 | (−1.883, −0.023) |
| % Asian | −1.3688 | 0.646 | (−2.639, −0.098) |
| % Native American | −1.6092 | 0.744 | (−3.071, −0.147) |
| % Unemployment | 0.485 | 0.116 | (0.257, 0.712) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wilkes, J.L.; Montalban, J.N.; Pringle, B.D.; Monroe, D.; Miller, A.; Zapata, I.; Brooks, A.E.; Ross, D.W. A Demographic and Regional Comparison of Opioid-Related Hospital Visits within Community Type in the United States. J. Clin. Med. 2021, 10, 3460. https://doi.org/10.3390/jcm10163460
Wilkes JL, Montalban JN, Pringle BD, Monroe D, Miller A, Zapata I, Brooks AE, Ross DW. A Demographic and Regional Comparison of Opioid-Related Hospital Visits within Community Type in the United States. Journal of Clinical Medicine. 2021; 10(16):3460. https://doi.org/10.3390/jcm10163460
Chicago/Turabian StyleWilkes, Jordan L., Jessica N. Montalban, Brian D. Pringle, Devin Monroe, Adela Miller, Isain Zapata, Amanda E. Brooks, and David W. Ross. 2021. "A Demographic and Regional Comparison of Opioid-Related Hospital Visits within Community Type in the United States" Journal of Clinical Medicine 10, no. 16: 3460. https://doi.org/10.3390/jcm10163460
APA StyleWilkes, J. L., Montalban, J. N., Pringle, B. D., Monroe, D., Miller, A., Zapata, I., Brooks, A. E., & Ross, D. W. (2021). A Demographic and Regional Comparison of Opioid-Related Hospital Visits within Community Type in the United States. Journal of Clinical Medicine, 10(16), 3460. https://doi.org/10.3390/jcm10163460