
Control of Glucose, Blood Pressure, and Cholesterol among Adults with Diabetes: The Brazilian National Health Survey

 , , , and
, , , and
Abstract
1. Introduction
2. Methods
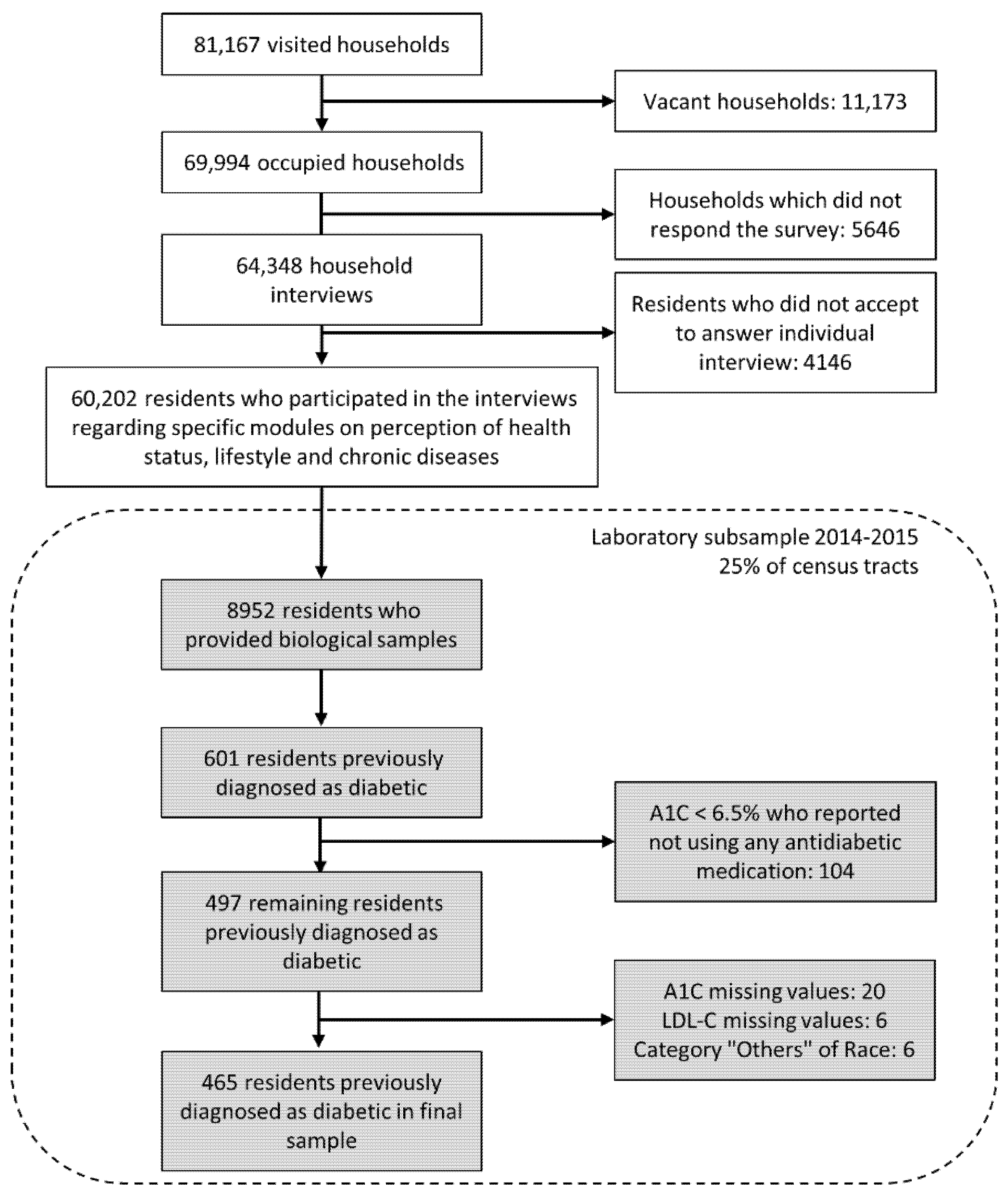
2.1. The PNS Survey
2.2. Study Variables
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- International Diabetes Federation. IDF Diabetes Atlas, 9th ed.; International Diabetes Federation: Brussels, Belgium, 2019. [Google Scholar]
- GBD Compare|IHME Viz Hub. Available online: http://vizhub.healthdata.org/gbd-compare (accessed on 24 June 2021).
- Duncan, B.B.; Cousin, E.; Naghavi, M.; Afshin, A.; França, E.B.; de Passos, V.M.A.; Malta, D.; Nascimento, B.R.; Schmidt, M.I. The Burden of Diabetes and Hyperglycemia in Brazil: A Global Burden of Disease Study 2017. Popul. Health Metr. 2020, 18, 9. [Google Scholar] [CrossRef] [PubMed]
- Klein, R. Hyperglycemia and Microvascular and Macrovascular Disease in Diabetes. Diabetes Care 1995, 18, 258–268. [Google Scholar] [CrossRef] [PubMed]
- Barrett-Connor, E.; Wingard, D.; Wong, N.; Goldberg, R. Heart Disease and Diabetes. In Diabetes in America; Cowie, C.C., Casagrande, S.S., Menke, A., Cissell, M.A., Eberhardt, M.S., Meigs, J.B., Gregg, E.W., Knowler, W.C., Barrett-Connor, E., Becker, D.J., et al., Eds.; National Institute of Diabetes and Digestive and Kidney Diseases (US): Bethesda, MD, USA, 2018. [Google Scholar]
- Gæde, P.; Lund-Andersen, H.; Parving, H.-H.; Pedersen, O. Effect of a Multifactorial Intervention on Mortality in Type 2 Diabetes. N. Engl. J. Med. 2008, 358, 580–591. [Google Scholar] [CrossRef] [PubMed]
- Rawshani, A.; Rawshani, A.; Franzén, S.; Sattar, N.; Eliasson, B.; Svensson, A.-M.; Zethelius, B.; Miftaraj, M.; McGuire, D.K.; Rosengren, A.; et al. Risk Factors, Mortality, and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N. Engl. J. Med. 2018, 379, 633–644. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Glycemic Targets: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S73–S84. [Google Scholar] [CrossRef]
- Emdin, C.A.; Rahimi, K.; Neal, B.; Callender, T.; Perkovic, V.; Patel, A. Blood Pressure Lowering in Type 2 Diabetes: A Systematic Review and Meta-Analysis. JAMA 2015, 313, 603. [Google Scholar] [CrossRef]
- De Vries, F.M.; Denig, P.; Pouwels, K.B.; Postma, M.J.; Hak, E. Primary Prevention of Major Cardiovascular and Cerebrovascular Events with Statins in Diabetic Patients. Drugs 2012, 72, 2365–2373. [Google Scholar] [CrossRef]
- Seidu, S.; Achana, F.A.; Gray, L.J.; Davies, M.J.; Khunti, K. Effects of Glucose-Lowering and Multifactorial Interventions on Cardiovascular and Mortality Outcomes: A Meta-Analysis of Randomized Control Trials. Diabet. Med. 2016, 33, 280–289. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Introduction: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S1–S2. [Google Scholar] [CrossRef] [PubMed]
- American Diabetes Association. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S125–S150. [Google Scholar] [CrossRef] [PubMed]
- Cosentino, F.; Grant, P.J.; Aboyans, V.; Bailey, C.J.; Ceriello, A.; Delgado, V.; Federici, M.; Filippatos, G.; Grobbee, D.E.; Hansen, T.B.; et al. 2019 ESC Guidelines on Diabetes, Pre-Diabetes, and Cardiovascular Diseases Developed in Collaboration with the EASD: The Task Force for Diabetes, Pre-Diabetes, and Cardiovascular Diseases of the European Society of Cardiology (ESC) and the European Association for the Study of Diabetes (EASD). Eur. Heart J. 2020, 41, 255–323. [Google Scholar] [CrossRef]
- World Health Organization. WHO Package of Essential Noncommunicable (PEN) Disease Interventions for Primary Health Care. Available online: https://apps.who.int/iris/bitstream/handle/10665/334186/9789240009226.eng.pdf?sequence=1&isAllowed=y (accessed on 21 July 2021).
- Fang, M.; Wang, D.; Coresh, J.; Selvin, E. Trends in Diabetes Treatment and Control in U.S. Adults, 1999–2018. N. Engl. J. Med. 2021, 384, 2219–2228. [Google Scholar] [CrossRef]
- Kim, B.-Y.; Won, J.C.; Lee, J.H.; Kim, H.-S.; Park, J.H.; Ha, K.H.; Won, K.C.; Kim, D.J.; Park, K.S. Diabetes Fact Sheets in Korea, 2018: An Appraisal of Current Status. Diabetes Metab. J. 2019, 43, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Khunti, K.; Ceriello, A.; Cos, X.; Block, C.D. Achievement of Guideline Targets for Blood Pressure, Lipid, and Glycaemic Control in Type 2 Diabetes: A Meta-Analysis. Diabetes Res. Clin. Pract. 2018, 137, 137–148. [Google Scholar] [CrossRef] [PubMed]
- Szwarcwald, C.L.; Malta, D.C.; de Souza, P.R.B.; da de Almeida, W.S.; Damacena, G.N.; Pereira, C.A.; Rosenfeld, L.G. Laboratory Exams of the National Health Survey: Methodology of Sampling, Data Collection and Analysis. Rev. Bras. Epidemiol. 2019, 22. [Google Scholar] [CrossRef]
- Szwarcwald, C.L.; Malta, D.C.; Pereira, C.A.; Vieira, M.L.F.P.; Conde, W.L.; de Souza Júnior, P.R.B.; Damacena, G.N.; Azevedo, L.O.; Azevedo E Silva, G.; Theme Filha, M.M.; et al. National Health Survey in Brazil: Design and methodology of application. Cienc. Saude Coletiva 2014, 19, 333–342. [Google Scholar] [CrossRef]
- Damacena, G.N.; Szwarcwald, C.L.; Malta, D.C.; de Souza Júnior, P.R.B.; Vieira, M.L.F.P.; Pereira, C.A.; de Morais Neto, O.L.; Silva Júnior, J.B. da O Processo de Desenvolvimento Da Pesquisa Nacional de Saúde No Brasil, 2013. Epidemiol. E Serv. Saúde 2015, 24, 197–206. [Google Scholar] [CrossRef]
- Kaptoge, S.; Pennells, L.; Bacquer, D.D.; Cooney, M.T.; Kavousi, M.; Stevens, G.; Riley, L.M.; Savin, S.; Khan, T.; Altay, S.; et al. World Health Organization Cardiovascular Disease Risk Charts: Revised Models to Estimate Risk in 21 Global Regions. Lancet Glob. Health 2019, 7, e1332–e1345. [Google Scholar] [CrossRef]
- Rao, J.N.K.; Scott, A.J. On Chi-Squared Tests for Multiway Contingency Tables with Cell Proportions Estimated from Survey Data. Ann. Stat. 1984, 12, 46–60. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2021. [Google Scholar]
- Lumley, T. Analysis of Complex Survey Samples. J. Stat. Softw. 2004, 9, 1–19. [Google Scholar] [CrossRef]
- Pesquisa Nacional de Saúde, 2013: Acesso e Utilização dos Serviços de Saúde, Acidentes e Violências: Brasil, Grandes Regiões e Unidades da Federação; Instituto Brasileiro de Geografia e Estatística-IBGE: Rio de Janeiro, Brazil, 2015; ISBN 978-85-240-4346-8.
- Instituto Brasileiro de Geografia e Estatística Nota Técnica—Dados dos Exames Laboratoriais da Pesquisa Nacional de Saúde—PNS. 2018. Available online: https://ftp.ibge.gov.br/PNS/2013/Divulgacoes/Outros/Exames/Nota_tecnica_Exames_Laboratoriais_PNS.pdf (accessed on 21 July 2021).
- Yu, N.-C.; Su, H.-Y.; Chiou, S.-T.; Yeh, M.C.; Yeh, S.-W.; Tzeng, M.-S.; Sheu, W.H.-H. Trends of ABC Control 2006–2011: A National Survey of Diabetes Health Promotion Institutes in Taiwan. Diabetes Res. Clin. Pract. 2013, 99, 112–119. [Google Scholar] [CrossRef] [PubMed]
- Portes, L.H.; Machado, C.V.; Turci, S.R.B. Trajetória Da Política de Controle Do Tabaco No Brasil de 1986 a 2016. Cad. Saúde Pública 2018, 34. [Google Scholar] [CrossRef]
- Navarro-Vidal, B.; Banegas, J.R.; León-Muñoz, L.M.; Rodríguez-Artalejo, F.; Graciani, A. Achievement of Cardiometabolic Goals among Diabetic Patients in Spain. A Nationwide Population-Based Study. PLoS ONE 2013, 8, e61549. [Google Scholar] [CrossRef] [PubMed]
- Mendes, A.B.V.; Fittipaldi, J.A.S.; Neves, R.C.S.; Chacra, A.R.; Moreira, E.D. Prevalence and Correlates of Inadequate Glycaemic Control: Results from a Nationwide Survey in 6,671 Adults with Diabetes in Brazil. Acta Diabetol. 2010, 47, 137–145. [Google Scholar] [CrossRef] [PubMed]
- Lopez Stewart, G.; Tambascia, M.; Rosas Guzmán, J.; Etchegoyen, F.; Ortega Carrión, J.; Artemenko, S. Control of Type 2 Diabetes Mellitus among General Practitioners in Private Practice in Nine Countries of Latin America. Rev. Panam. Salud Pública 2007, 22, 12–20. [Google Scholar] [CrossRef]
- American Diabetes Association. Facilitating Behavior Change and Well-Being to Improve Health Outcomes: Standards of Medical Care in Diabetes—2021. Diabetes Care 2021, 44, S53–S72. [Google Scholar] [CrossRef] [PubMed]
- Barua Rajat, S.; Rigotti Nancy, A.; Benowitz Neal, L.; Michael, C.K.; Mohammad-Ali, J.; Morris Pamela, B.; Ratchford Elizabeth, V.; Linda, S.; Stecker Eric, C.; Wiggins Barbara, S. ACC Expert Consensus Decision Pathway on Tobacco Cessation Treatment. J. Am. Coll. Cardiol. 2018, 72, 3332–3365. [Google Scholar] [CrossRef]
- Cavero-Redondo, I.; Peleteiro, B.; Álvarez-Bueno, C.; Rodriguez-Artalejo, F.; Martínez-Vizcaíno, V. Glycated Haemoglobin A1c as a Risk Factor of Cardiovascular Outcomes and All-Cause Mortality in Diabetic and Non-Diabetic Populations: A Systematic Review and Meta-Analysis. BMJ Open 2017, 7, e015949. [Google Scholar] [CrossRef]
- Yudkin, J.S.; Richter, B.; Gale, E.A.M. Intensified Glucose Lowering in Type 2 Diabetes: Time for a Reappraisal. Diabetologia 2010, 53, 2079–2085. [Google Scholar] [CrossRef]
- Scicali, R.; Di Pino, A.; Ferrara, V.; Urbano, F.; Piro, S.; Rabuazzo, A.M.; Purrello, F. New Treatment Options for Lipid-Lowering Therapy in Subjects with Type 2 Diabetes. Acta Diabetol. 2018, 55, 209–218. [Google Scholar] [CrossRef]
- Chou, R.; Dana, T.; Blazina, I.; Daeges, M.; Jeanne, T.L. Statins for Prevention of Cardiovascular Disease in Adults: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2016, 316, 2008. [Google Scholar] [CrossRef]
- Bundy, J.D.; Li, C.; Stuchlik, P.; Bu, X.; Kelly, T.N.; Mills, K.T.; He, H.; Chen, J.; Whelton, P.K.; He, J. Systolic Blood Pressure Reduction and Risk of Cardiovascular Disease and Mortality: A Systematic Review and Network Meta-Analysis. JAMA Cardiol. 2017, 2, 775–781. [Google Scholar] [CrossRef] [PubMed]
- Arnett, D.K.; Blumenthal, R.S.; Albert, M.A.; Buroker, A.B.; Goldberger, Z.D.; Hahn, E.J.; Himmelfarb, C.D.; Khera, A.; Lloyd-Jones, D.; McEvoy, J.W.; et al. 2019 ACC/AHA Guideline on the Primary Prevention of Cardiovascular Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2019, 140, e596–e646. [Google Scholar] [CrossRef] [PubMed]
- Scicali, R.; Rosenbaum, D.; Di Pino, A.; Giral, P.; Cluzel, P.; Redheuil, A.; Piro, S.; Rabuazzo, A.M.; Purrello, F.; Bruckert, E.; et al. An Increased Waist-to-Hip Ratio Is a Key Determinant of Atherosclerotic Burden in Overweight Subjects. Acta Diabetol. 2018, 55, 741–749. [Google Scholar] [CrossRef] [PubMed]
- Seidu, S.; Cos, X.; Brunton, S.; Harris, S.B.; Jansson, S.P.O.; Mata-Cases, M.; Neijens, A.M.J.; Topsever, P.; Khunti, K. A Disease State Approach to the Pharmacological Management of Type 2 Diabetes in Primary Care: A Position Statement by Primary Care Diabetes Europe. Prim. Care Diabetes 2021, 15, 31–51. [Google Scholar] [CrossRef] [PubMed]
- Akselrod, S.; Bloomfield, A.; Marmot, M.; Moran, A.E.; Nishtar, S.; Placella, E. Mobilising Society to Implement Solutions for Non-Communicable Diseases. BMJ 2019, 365, l360. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, M.I.; Bracco, P.; Canhada, S.; Guimarães, J.M.N.; Barreto, S.M.; Chor, D.; Griep, R.; Yudkin, J.S.; Duncan, B.B. Regression to the Mean Contributes to the Apparent Improvement in Glycemia 3.8 Years After Screening: The ELSA-Brasil Study. Diabetes Care 2021, 44, 81–88. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | A1C (%) | p Value † | ||||
|---|---|---|---|---|---|---|
| Overall | <7 | 7 to <8 | 8 to <9 | ≥9 | ||
| Overall, n (%) | 465 (100) | 225 (46.0) | 73 (19.8) | 60 (14.1) | 107 (20.1) | |
| Sex, n (%) | 0.12 | |||||
| Female | 308 (61.5) | 158 (49.9) | 40 (15.9) | 37 (12.8) | 73 (21.4) | |
| Male | 157 (38.5) | 67 (39.6) | 33 (26.0) | 23 (16.3) | 34 (18.1) | |
| Age group (years), n (%) | 0.005 | |||||
| 18–44 | 53 (11.5) | 25 (25.3) | 6 (26.7) | 4 (15.7) | 18 (32.3) | |
| 45–59 | 168 (38.1) | 70 (40.4) | 24 (16.4) | 18 (13.7) | 56 (29.5) | |
| 60+ | 244 (50.4) | 130 (54.9) | 43 (20.8) | 38 (14.1) | 33 (10.2) | |
| Race, n (%) | 0.31 | |||||
| White | 191 (52.1) | 96 (48.3) | 36 (22.4) | 23 (12.5) | 36 (16.9) | |
| Black or Brown | 274 (47.9) | 129 (43.5) | 37 (17.0) | 37 (15.9) | 71 (23.6) | |
| Education, n (%) | 0.97 | |||||
| Elementary or less | 345 (70.3) | 158 (45.3) | 56 (19.7) | 49 (14.1) | 82 (20.9) | |
| Above elementary school | 120 (29.7) | 67 (47.5) | 17 (19.9) | 11 (14.3) | 25 (18.3) | |
| Region, n (%) | 0.03 | |||||
| North | 64 (3.5) | 30 (46.1) | 8 (12.7) | 9 (15.3) | 17 (25.9) | |
| Northeast | 145 (20.1) | 70 (48.3) | 23 (15.8) | 16 (11.2) | 36 (24.7) | |
| Southeast | 125 (55.0) | 61 (45.4) | 28 (25.1) | 18 (15.1) | 18 (14.4) | |
| South | 59 (13.0) | 26 (42.0) | 7 (11.7) | 10 (17.2) | 16 (29.0) | |
| Center-West | 72 (8.4) | 38 (50.1) | 7 (9.9) | 7 (9.6) | 20 (30.4) | |
| Receiving cash transfer, n (%) | 0.84 | |||||
| No | 431 (94.2) | 208 (46.4) | 71 (20.0) | 57 (14.0) | 95 (19.6) | |
| Yes | 34 (5.8) | 17 (39.3) | 2 (16.2) | 3 (17.1) | 12 (27.4) | |
| Private health insurance, n (%) | 0.21 | |||||
| No | 329 (68.4) | 148 (45.7) | 51 (17.0) | 43 (14.5) | 87 (22.8) | |
| Yes | 136 (31.6) | 77 (46.6) | 22 (25.8) | 17 (13.3) | 20 (14.3) | |
| Body mass index group (kg/m2), n (%) | <0.001 | |||||
| <25 | 98 (21.3) | 55 (50.9) | 6 (6.0) | 17 (22.4) | 20 (20.8) | |
| 25–29.9 | 168 (34.6) | 75 (44.0) | 25 (17.8) | 21 (12.9) | 47 (25.3) | |
| 30–34.9 | 127 (29.2) | 67 (52.8) | 23 (20.7) | 13 (10.8) | 24 (15.7) | |
| ≥35 | 72 (14.9) | 28 (30.0) | 19 (42.5) | 9 (11.7) | 16 (15.8) | |
| Current smoker, n (%) | 0.33 | |||||
| No | 416 (90.3) | 205 (45.9) | 61 (19.3) | 56 (15.1) | 94 (19.7) | |
| Yes | 49 (9.7) | 20 (46.5) | 12 (24.4) | 4 (4.9) | 13 (24.2) | |
| Years since diabetes diagnosis, n (%) | 0.13 | |||||
| 0–1 | 35 (5.8) | 20 (59.4) | 7 (21.5) | 1 (1.2) | 7 (18.0) | |
| 1–10 | 217 (46.0) | 117 (50.5) | 34 (20.0) | 22 (10.9) | 44 (18.6) | |
| 10+ | 213 (48.3) | 88 (40.0) | 32 (19.4) | 37 (18.8) | 56 (21.8) | |
| Current antidiabetic medication, n (%) | <0.001 | |||||
| None | 38 (7.9) | 10 (20.8) | 8 (24.7) | 6 (13.2) | 14 (41.3) | |
| Oral antidiabetic drugs alone | 341 (71.2) | 193 (55.8) | 45 (17.7) | 41 (12.0) | 62 (14.5) | |
| Insulin alone | 19 (6.0) | 8 (38.1) | 3 (12.9) | 2 (25.4) | 6 (23.6) | |
| Both insulin and oral antidiabetic drugs | 67 (14.9) | 14 (15.7) | 17 (30.0) | 11 (20.2) | 25 (34.1) | |
| History of cardiovascular disease, n (%) | 0.21 | |||||
| No | 381 (82.2) | 181 (44.6) | 59 (18.8) | 48 (14.5) | 93 (22.1) | |
| Yes | 84 (17.8) | 44 (52.3) | 14 (24.4) | 12 (12.4) | 14 (11.0) | |
| Characteristic | Overall | High CVD Risk | Low CVD Risk | p Value † |
|---|---|---|---|---|
| (n = 465) | (n = 97) | (n = 368) | ||
| Mean (SD) | Mean (SD) | Mean (SD) | ||
| A1C (%) | 7.62 (1.86) | 7.17 (1.76) | 7.73 (1.87) | 0.01 |
| Systolic BP (mmHg) | 136.8 (21.2) | 141.0 (27.4) | 135.8 (19.2) | 0.13 |
| Diastolic BP (mmHg) | 80.4 (11.8) | 78.6 (12.7) | 80.8 (11.5) | 0.23 |
| LDL-C (mg/dL) | 104.2 (34.3) | 95.7 (33.6) | 106.4 (34.2) | 0.02 |
| BP (mmHg) | n (%) | n (%) | n (%) | 0.01 |
| <130/80 | 153 (30.4) | 24 (28.4) | 129 (31.0) | |
| 130/80 to <140/90 | 120 (25.9) | 25 (24.4) | 95 (26.3) | |
| 140/90 to <160/100 | 119 (27.9) | 19 (18.7) | 100 (30.2) | |
| ≥160/100 | 73 (15.8) | 29 (28.6) | 44 (12.5) | |
| LDL-C (mg/dL) | n (%) | n (%) | n (%) | 0.15 |
| <100 | 214 (47.0) | 56 (59.0) | 158 (43.9) | |
| 100–129 | 151 (33.3) | 25 (28.2) | 126 (34.6) | |
| 130–159 | 70 (12.8) | 12 (7.1) | 58 (14.3) | |
| ≥160 | 30 (6.8) | 4 (5.6) | 26 (7.1) | |
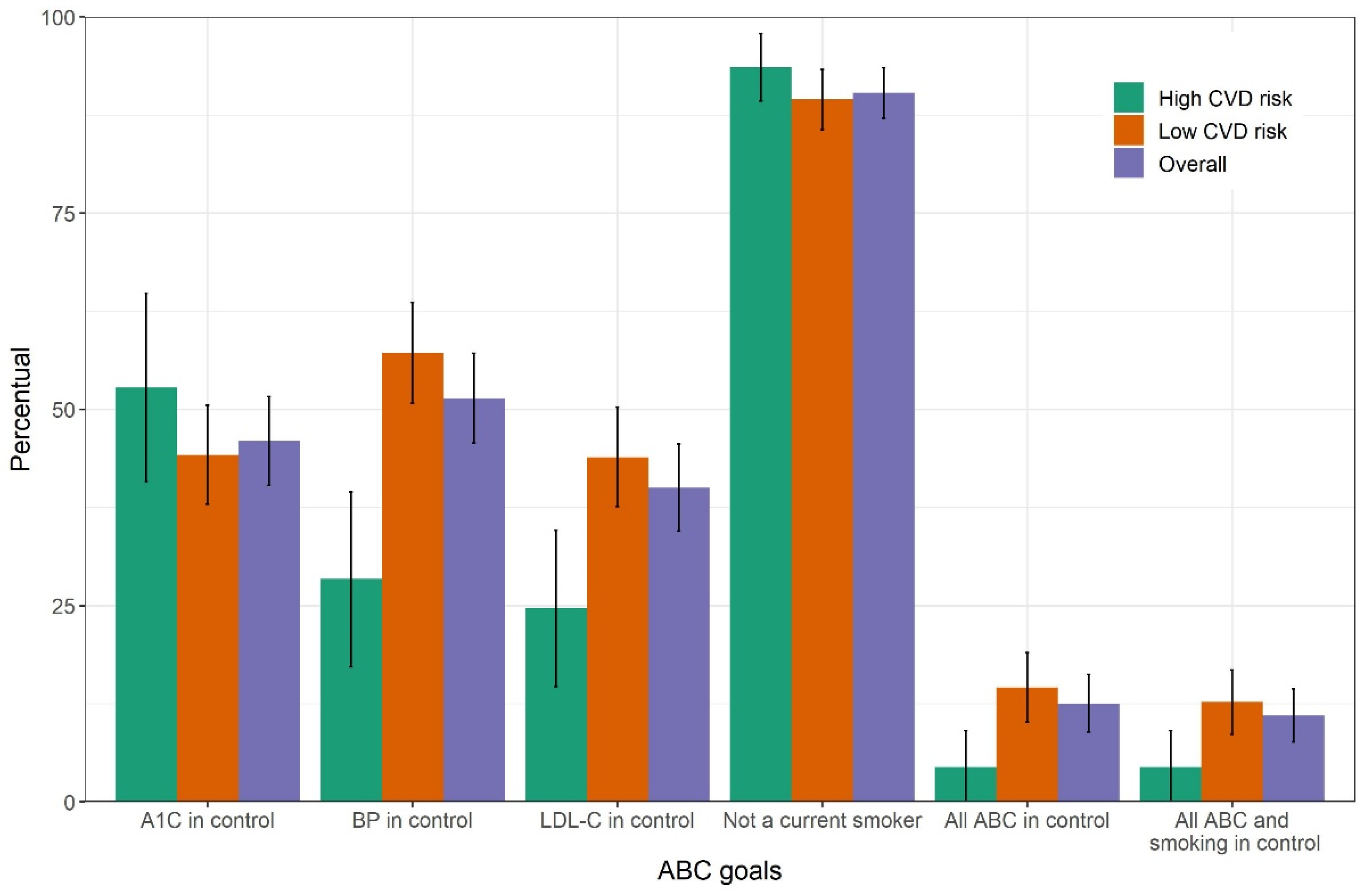
| Attained control | n (%; 95%CI) | n (%; 95%CI) | n (%; 95%CI) | |
| A1C | 225 (46.0; 40.3–51.6) | 49 (52.8; 40.8–64.8) | 176 (44.2; 37.9–50.5) | 0.22 |
| BP | 248 (51.4; 45.7–57.1) | 24 (28.4; 17.2–39.5) | 224 (57.2; 50.8–63.6) | <0.001 |
| LDL-C | 183 (40.0; 34.5–45.6) | 25 (24.7; 14.7–34.6) | 158 (43.9; 37.6–50.3) | 0.004 |
| Non-smoking | 416 (90.3; 87.1–93.5) | 87 (93.6; 89.3–97.9) | 329 (89.5; 85.6–93.3) | 0.19 |
| Characteristic | A1C < 7% | Achieving ≥ 2 Goals | ||
|---|---|---|---|---|
| Model 1 | Model 2 | Model 1 | Model 2 | |
| PR (95% CI) | PR (95% CI) | PR (95% CI) | PR (95% CI) | |
| Sex (reference: Female) | ||||
| Male | 0.84 (0.64–1.08) | 0.79 (0.61–1.01) | 0.87 (0.66–1.14) | 0.79 (0.60–1.03) |
| Age (increase of 10 years) | 1.18 (1.08–1.29) | 1.24 (1.14–1.35) | 1.03 (0.94–1.14) | 1.05 (0.95–1.15) |
| Race (reference: White) | ||||
| Black or Brown | 0.97 (0.77–1.23) | 0.94 (0.75–1.19) | 0.81 (0.63–1.05) | 0.80 (0.62–1.02) |
| Education (reference: Elementary or less) | ||||
| Above elementary school | 1.23 (0.95–1.58) | 1.24 (0.97–1.59) | 1.27 (0.97–1.67) | 1.29 (0.98–1.68) |
| Region (reference: Southeast) | ||||
| North | 1.12 (0.79–1.59) | 1.12 (0.78–1.62) | 0.97 (0.68–1.38) | 1.08 (0.75–1.56) |
| Northeast | 1.04 (0.81–1.34) | 1.04 (0.80–1.35) | 0.83 (0.62–1.10) | 0.84 (0.62–1.12) |
| South | 1.01 (0.71–1.44) | 0.97 (0.68–1.39) | 0.96 (0.66–1.39) | 0.90 (0.62–1.32) |
| Center-West | 1.18 (0.88–1.59) | 1.15 (0.86–1.55) | 1.28 (0.95–1.72) | 1.37 (1.03–1.83) |
| Receiving cash transfer (reference: No) | ||||
| Yes | 1.01 (0.56–1.84) | 0.94 (0.52–1.70) | 0.94 (0.53–1.66) | 0.81 (0.46–1.42) |
| Private health insurance (reference: No) | ||||
| Yes | 0.99 (0.77–1.27) | 0.93 (0.72–1.21) | 1.24 (0.96–1.60) | 1.15 (0.88–1.51) |
| Body mass index (increase of 5 kg/m2) | 0.93 (0.83–1.03) | 0.91 (0.82–1.02) | 0.85 (0.76–0.95) | 0.82 (0.73–0.92) |
| Current smoker (reference: No) | ||||
| Yes | 0.88 (0.60–1.31) | 0.92 (0.64–1.33) | 0.83 (0.57–1.21) | 0.90 (0.64–1.27) |
| Years since diabetes diagnosis (reference: 1–10) | ||||
| 0–1 | 1.22 (0.86–1.73) | 1.20 (0.84–1.72) | 0.69 (0.39–1.20) | 0.68 (0.41–1.12) |
| 10+ | 0.68 (0.53–0.88) | 0.67 (0.53–0.86) | 0.79 (0.60–1.04) | 0.76 (0.59–0.98) |
| History of cardiovascular disease (reference: No) | ||||
| Yes | 1.05 (0.79–1.40) | 1.09 (0.83–1.43) | 0.76 (0.53–1.10) | 0.79 (0.55–1.13) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
dos Reis, R.C.P.; Duncan, B.B.; Szwarcwald, C.L.; Malta, D.C.; Schmidt, M.I. Control of Glucose, Blood Pressure, and Cholesterol among Adults with Diabetes: The Brazilian National Health Survey. J. Clin. Med. 2021, 10, 3428. https://doi.org/10.3390/jcm10153428
dos Reis RCP, Duncan BB, Szwarcwald CL, Malta DC, Schmidt MI. Control of Glucose, Blood Pressure, and Cholesterol among Adults with Diabetes: The Brazilian National Health Survey. Journal of Clinical Medicine. 2021; 10(15):3428. https://doi.org/10.3390/jcm10153428
Chicago/Turabian Styledos Reis, Rodrigo Citton P., Bruce B. Duncan, Célia Landmann Szwarcwald, Deborah Carvalho Malta, and Maria Inês Schmidt. 2021. "Control of Glucose, Blood Pressure, and Cholesterol among Adults with Diabetes: The Brazilian National Health Survey" Journal of Clinical Medicine 10, no. 15: 3428. https://doi.org/10.3390/jcm10153428
APA Styledos Reis, R. C. P., Duncan, B. B., Szwarcwald, C. L., Malta, D. C., & Schmidt, M. I. (2021). Control of Glucose, Blood Pressure, and Cholesterol among Adults with Diabetes: The Brazilian National Health Survey. Journal of Clinical Medicine, 10(15), 3428. https://doi.org/10.3390/jcm10153428