
Effects of Antidepressant Treatment on Neurotrophic Factors (BDNF and IGF-1) in Patients with Major Depressive Disorder (MDD)

Abstract
:1. Introduction
2. Materials and Methods
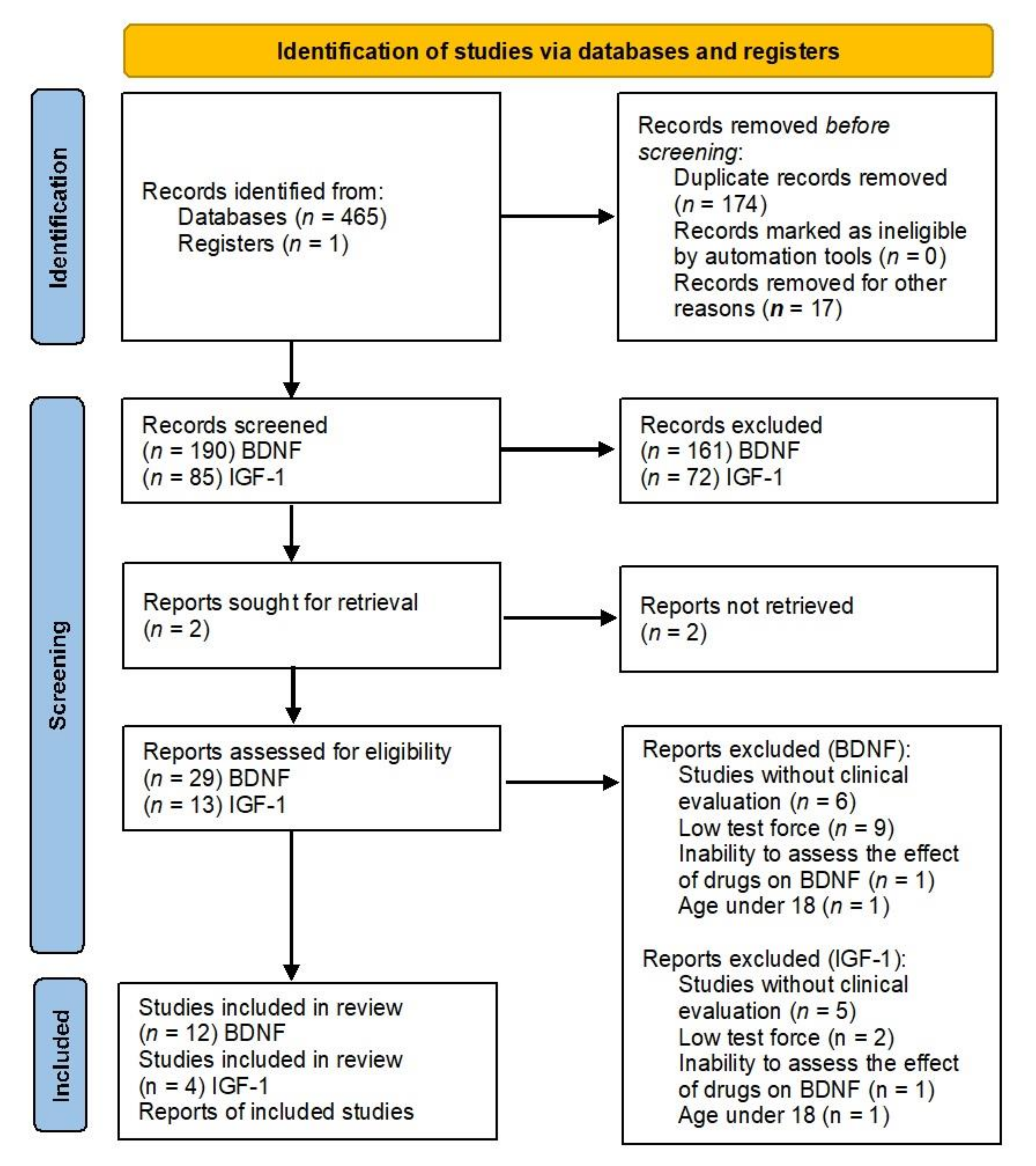
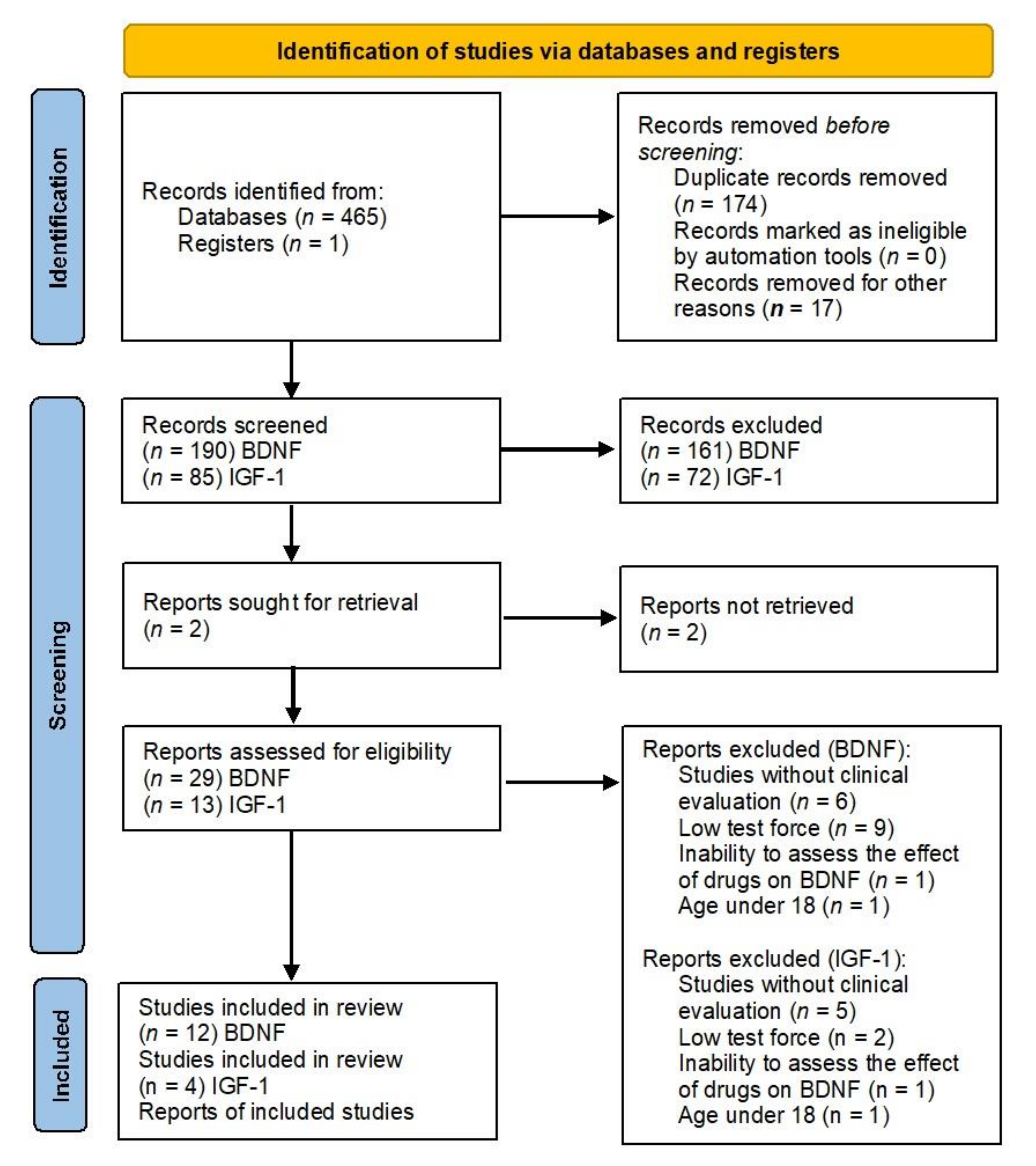
Search Strategy
Study Selection Strategy
3. Results
3.1. BDNF
3.2. IGF-1
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Blazer, D.G.; Kessler, R.C.; McGonagle, K.A.; Swartz, M.S. The prevalence and distribution of major depression in a national community sample: The National Comorbidity Survey. Am. J. Psychiatry 1994, 151, 979–986. [Google Scholar] [CrossRef]
- Barlow, D.; Durand, V. Abnormal Psychology, 1st ed.; Wadsworth/Thomson Learning: Belmont, CA, USA, 2007; pp. 292–295. [Google Scholar]
- Maes, M. Major Depression and Activation of The Inflammatory Response System. Adv. Exp. Med. Biol. 1999, 461, 25–46. [Google Scholar] [CrossRef]
- Maes, M.; Leonard, B.; Myint, A.; Kubera, M.; Verkerk, R. The new ‘5-HT’ hypothesis of depression: Cell-mediated immune activation induces indoleamine 2,3-dioxygenase, which leads to lower plasma tryptophan and an increased synthesis of detrimental tryptophan catabolites (TRYCATs), both of which contribute to the onset of depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2011, 35, 702–721. [Google Scholar] [CrossRef]
- Maes, M. Depression is an inflammatory disease, but cell-mediated immune activation is the key component of depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2011, 35, 664–675. [Google Scholar] [CrossRef]
- Capuron, L.; Dantzer, R. Cytokines and depression: The need for a new paradigm. Brain Behav. Immun. 2003, 17, 119–124. [Google Scholar] [CrossRef]
- Schiepers, O.J.G.; Wichers, M.C.; Maes, M. Cytokines and major depression. Prog. Neu-ro-Psychopharmacol. Biol. Psychiatry 2005, 29, 201–217. [Google Scholar] [CrossRef]
- Raison, C.L.; Capuron, L.; Miller, A.H. Cytokines sing the blues: Inflammation and the pathogenesis of depression. Trends Immunol. 2006, 27, 24–31. [Google Scholar] [CrossRef] [Green Version]
- Dowlati, Y.; Herrmann, N.; Swardfager, W.; Liu, H.; Sham, L.; Reim, E.K.; Lanctôt, K.L. A Meta-Analysis of Cytokines in Major Depression. Biol. Psychiatry 2010, 67, 446–457. [Google Scholar] [CrossRef] [PubMed]
- Torres-Aleman, I. Toward a comprehensive neurobiology of IGF-I. Dev. Neurobiol. 2010, 70, 384–396. [Google Scholar] [CrossRef] [PubMed]
- Raedler, T.J. Inflammatory mechanisms in major depressive disorder. Curr. Opin. Psychiatry 2011, 24, 519–525. [Google Scholar] [CrossRef] [PubMed]
- Behr, G.A.; Moreira, J.C.F.; Frey, B.N. Preclinical and Clinical Evidence of Antioxidant Effects of Antidepressant Agents: Implications for the Pathophysiology of Major Depressive Disorder. Oxidative Med. Cell. Longev. 2012, 2012, 609421. [Google Scholar] [CrossRef] [PubMed]
- Crupi, R.; Cuzzocrea, S. Neuroinflammation and Immunity: A New Pharmacological Target in Depression. CNS Neurol. Disord. Drug Targets 2016, 15, 464–476. [Google Scholar] [CrossRef] [PubMed]
- Gałecki, P.; Mossakowska-Wójcik, J.; Talarowska, M. The anti-inflammatory mechanism of antidepressants—SSRIs, SNRIs. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2018, 80, 291–294. [Google Scholar] [CrossRef] [PubMed]
- Gałecki, P.; Talarowska, M. Inflammatory theory of depression. Psychiatr. Polska 2018, 52, 437–447. [Google Scholar] [CrossRef]
- Duman, R.S.; Gr Fau, H.; Nestler, E.J. A molecular and cellular theory of depression. Arch. Gen. Psychiatry 1997, 54, 597–607. [Google Scholar] [CrossRef]
- Duman, R.S.; Monteggia, L.M. A Neurotrophic Model for Stress-Related Mood Disorders. Biol. Psychiatry 2006, 59, 1116–1127. [Google Scholar] [CrossRef]
- Björkholm, C.; Monteggia, L.M. BDNF—A key transducer of antidepressant effects. Neuropharmacology 2016, 102, 72–79. [Google Scholar] [CrossRef] [Green Version]
- Brunoni, A.R.; Machado-Vieira, R.; Zarate, C.A.; Vieira, E.; Vanderhasselt, M.-A.; Nitsche, M.A.; Valiengo, L.; Benseñor, I.M.; Lotufo, P.; Gattaz, W.F.; et al. BDNF plasma levels after antidepressant treatment with sertraline and transcranial direct current stimulation: Results from a factorial, randomized, sham-controlled trial. Eur. Neuropsychopharmacol. 2014, 24, 1144–1151. [Google Scholar] [CrossRef] [Green Version]
- Molendijk, M.; Spinhoven, P.; Polak, M.; A A Bus, B.; Penninx, B.W.J.H.; Elzinga, B.M. Serum BDNF concentrations as peripheral manifestations of depression: Evidence from a systematic review and meta-analyses on 179 associations (N = 9484). Mol. Psychiatry 2013, 19, 791–800. [Google Scholar] [CrossRef]
- Wolkowitz, O.M.; Wolf, J.; Shelly, W.; Rosser, R.; Burke, H.M.; Lerner, G.K.; Reus, V.; Nelson, J.C.; Epel, E.S.; Mellon, S.H. Serum BDNF levels before treatment predict SSRI response in depression. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2011, 35, 1623–1630. [Google Scholar] [CrossRef] [Green Version]
- Brunoni, A.R.; Lopes, M.; Fregni, F. A systematic review and meta-analysis of clinical studies on major depression and BDNF levels: Implications for the role of neuroplasticity in depression. Int. J. Neuropsychopharmacol. 2008, 11, 1169–1180. [Google Scholar] [CrossRef]
- Shimitzu, E.; Hashimoto, K.; Iyo, M. Major depressive disorders and BDNF (brain-derived neu-rotrophic factor). Nihon Shinkei Seishin Yakurigaku Zasshi 2004, 24, 147–150. [Google Scholar]
- Zhang, J.; Yao, W.; Hashimoto, K. Brain-derived neurotrophic factor (BDNF)-TrkB signaling in inflammation-related depression and potential therapeutic targets. Curr. Neuropharmacol. 2016, 14, 721–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharma, A.N.; Silva, B.F.B.D.C.E.; Soares, J.C.; Carvalho, A.F.; Quevedo, J. Role of trophic factors GDNF, IGF-1 and VEGF in major depressive disorder: A comprehensive review of human studies. J. Affect. Disord. 2016, 197, 9–20. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mitre, M.; Mariga, A.; Chao, M. Neurotrophin signalling: Novel insights into mechanisms and pathophysiology. Clin. Sci. 2017, 131, 13–23. [Google Scholar] [CrossRef] [Green Version]
- Chen, B.; Dowlatshahi, D.; MacQueen, G.M.; Wang, J.-F.; Young, L. Increased hippocampal bdnf immunoreactivity in subjects treated with antidepressant medication. Biol. Psychiatry 2001, 50, 260–265. [Google Scholar] [CrossRef]
- Mondal, A.C.; Fatima, M. Direct and indirect evidences of BDNF and NGF as key modulators in depression: Role of antidepressants treatment. Int. J. Neurosci. 2019, 129, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Chen, M.; Zhang, L.; Jiang, Q. Peripheral IGF-1 in bipolar disorder and major depressive disorder: A systematic review and meta-analysis. Ann. Palliat. Med. 2020, 9, 4044–4053. [Google Scholar] [CrossRef] [PubMed]
- Szczęsny-Małysiak, E.; Ślusarczyk, J.; Głombik, K.; Budziszewska, B.; Kubera, M.; Lasoń, W.; Basta-Kaim, A. Possible contribution of IGF-1 to depressive disorder. Pharmacol. Rep. 2013, 65, 1622–1631. [Google Scholar] [CrossRef]
- Dyer, A.; Vahdatpour, C.; Sanfeliu, A.; Tropea, D. The role of Insulin-Like Growth Factor 1 (IGF-1) in brain development, maturation and neuroplasticity. Neuroscience 2016, 325, 89–99. [Google Scholar] [CrossRef] [PubMed]
- Levada, O.A.; Troyan, A. Major depressive disorder and accelerated aging from a peripheral IGF-1 overexpression perspective. Med. Hypotheses 2020, 138, 109610. [Google Scholar] [CrossRef] [PubMed]
- McCusker, R.H.; McCrea, K.; Zunich, S.; Dantzer, R.; Broussard, S.R.; Johnson, R.W.; Kelley, K.W. Insulin-like growth factor-I enhances the biological activity of brain-derived neurotrophic factor on cerebrocortical neurons. J. Neuroimmunol. 2006, 179, 186–190. [Google Scholar] [CrossRef]
- Karege, F.; Perret, G.; Bondolfi, G.; Schwald, M.; Bertschy, G.; Aubry, J.-M. Decreased serum brain-derived neurotrophic factor levels in major depressed patients. Psychiatry Res. 2002, 109, 143–148. [Google Scholar] [CrossRef]
- Lee, H.-Y.; Kim, Y.-K. Plasma Brain-Derived Neurotrophic Factor as a Peripheral Marker for the Action Mechanism of Antidepressants. Neuropsychobiology 2008, 57, 194–199. [Google Scholar] [CrossRef] [PubMed]
- Polyakova, M.; Stuke, K.; Schuemberg, K.; Mueller, K.; Schoenknecht, P.; Schroeter, M.L. BDNF as a biomarker for successful treatment of mood disorders: A systematic & quantitative meta-analysis. J. Affect. Disord. 2015, 174, 432–440. [Google Scholar] [CrossRef]
- Zhou, C.; Zhong, J.; Zou, B.; Fang, L.; Chen, J.-J.; Deng, X.; Zhang, L.; Zhao, X.; Qu, Z.; Lei, Y.; et al. Meta-analyses of comparative efficacy of antidepressant medications on peripheral BDNF concentration in patients with depression. PLoS ONE 2017, 12, e0172270. [Google Scholar] [CrossRef] [Green Version]
- Arumugam, V.; John, V.S.; Augustine, N.; Jacob, T.; Joy, S.M.; Sen, S.; Sen, T. The impact of antidepressant treatment on brain-derived neurotrophic factor level: An evidence-based approach through systematic review and meta-analysis. Indian J. Pharmacol. 2017, 49, 236–242. [Google Scholar] [CrossRef]
- Chiou, Y.-J.; Huang, T.-L. Serum Brain-Derived Neurotrophic Factors in Taiwanese Patients with Drug-Naïve First-Episode Major Depressive Disorder: Effects of Antidepressants. Int. J. Neuropsychopharmacol. 2016, 20, 213–218. [Google Scholar] [CrossRef] [Green Version]
- Gupta, R.; Gupta, K.; Tripathi, A.; Bhatia, M.; Gupta, L.K. Effect of Mirtazapine Treatment on Serum Levels of Brain-Derived Neurotrophic Factor and Tumor Necrosis Factor-a in Patients of Major Depressive Disorder with Severe Depression. Pharmacol. 2016, 97, 184–188. [Google Scholar] [CrossRef]
- Troyan, A.S.; Levada, O.A. The Diagnostic Value of the Combination of Serum Brain-Derived Neurotrophic Factor and Insulin-Like Growth Factor-1 for Major Depressive Disorder Diagnosis and Treatment Efficacy. Front. Psychiatry 2020, 11, 800. [Google Scholar] [CrossRef]
- Sagud, M.; Perkovic, M.N.; Vuksan-Cusa, B.; Maravic, A.; Strac, D.S.; Peles, A.M.; Zivkovic, M.; Kusevic, Z.; Pivac, N. A prospective, longitudinal study of platelet serotonin and plasma brain-derived neurotrophic factor concentrations in major depression: Effects of vortioxetine treatment. Psychopharmacology 2016, 233, 3259–3267. [Google Scholar] [CrossRef] [Green Version]
- Zheng, W.; Zhou, Y.-L.; Wang, C.-Y.; Lan, X.-F.; Zhang, B.; Zhou, S.-M.; Yan, S.; Ning, Y.-P. Plasma BDNF concentrations and the antidepressant effects of six ketamine infusions in unipolar and bipolar depression. PeerJ 2021, 9, e10989. [Google Scholar] [CrossRef]
- Bot, M.; Milaneschi, Y.; Penninx, B.W.; Drent, M.L. Plasma insulin-like growth factor I levels are higher in depressive and anxiety disorders, but lower in antidepressant medication users. Psychoneuroendocrinology 2016, 68, 148–155. [Google Scholar] [CrossRef]
- Levada, O.A.; Troyan, A.S.; Pinchuk, I. Serum insulin-like growth factor-1 as a potential marker for MDD diagnosis, its clinical characteristics, and treatment efficacy validation: Data from an open-label vortioxetine study. BMC Psychiatry 2020, 20, 208. [Google Scholar] [CrossRef] [PubMed]
- Kopczak, A.; Stalla, G.K.; Uhr, M.; Lucae, S.; Hennings, J.; Ising, M.; Holsboer, F.; Kloiber, S. IGF-I in major depression and antidepressant treatment response. Eur. Neuropsychopharmacol. 2015, 25, 864–872. [Google Scholar] [CrossRef]
- Rush, A.J.; Trivedi, M.H.; Wisniewski, S.R.; Nierenberg, A.A.; Stewart, J.W.; Warden, D. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: A STAR*D report. Am. J. Psychiatry 2006, 163, 1905–1917. [Google Scholar] [CrossRef] [PubMed]
- Weilburg, J.B. An overview of SSRI and SNRI therapies for depression. Manag. Care 2004, 13, 25–33. [Google Scholar]
- Baldwin, D.S. Serotonin noradrenaline reuptake inhibitors: A new generation of treatment for anxiety disorders. Int. J. Psychiatry Clin. Pract. 2006, 10, 12–15. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Faries, D.; Herrera, J.; Rayamajhi, J.; DeBrota, D.; Demitrack, M.; Potter, W.Z. The responsive-ness of the Hamilton Depression Rating Scale. J Psychiatr. Res. 2000, 34, 3–10. [Google Scholar] [CrossRef]
- Nibuya, M.; Morinobu, S.; Duman, R.S. Regulation of BDNF and trkB mRNA in rat brain by chronic electroconvulsive seizure and antidepressant drug treatments. J. Neurosci. 1995, 15, 7539–7547. [Google Scholar] [CrossRef] [PubMed]
- Nibuya, M.; Nestler, E.; Duman, R. Chronic antidepressant administration increases the expression of cAMP response element binding protein (CREB) in rat hippocampus. J. Neurosci. 1996, 16, 2365–2372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siwek, J.; Gourlay, M.L.; Slawson, D.C.; Shaughnessy, A.F. How to write an evidence-based clinical review article. Am. Fam. Physician 2002, 65, 11820489. [Google Scholar]
- Matrisciano, F.; Bonaccorso, S.; Ricciardi, A.; Scaccianoce, S.; Panaccione, I.; Wang, L.; Ruberto, A.; Tatarelli, R.; Nicoletti, F.; Girardi, P.; et al. Changes in BDNF serum levels in patients with major depression disorder (MDD) after 6 months treatment with sertraline, escitalopram, or venlafaxine. J. Psychiatr. Res. 2009, 43, 247–254. [Google Scholar] [CrossRef] [Green Version]
- Başterzi, A.D.; Yazici, K.; Aslan, E.; Delialioğlu, N.; Tasdelen, B.; Acar, Ş.T.; Yazici, A. Effects of fluoxetine and venlafaxine on serum brain derived neurotrophic factor levels in depressed patients. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2009, 33, 281–285. [Google Scholar] [CrossRef] [PubMed]
- Hellweg, R.; Ziegenhorn, A.; Heuser, I.; Deuschle, M. Serum Concentrations of Nerve Growth Factor and Brain-Derived Neurotrophic Factor in Depressed Patients before and after Antidepressant Treatment. Pharmacopsychiatry 2008, 41, 66–71. [Google Scholar] [CrossRef]
- Umene-Nakano, W.; Yoshimura, R.; Ueda, N.; Suzuki, A.; Ikenouchi-Sugita, A.; Hori, H.; Otani, K.; Nakamura, J. Predictive factors for responding to sertraline treatment: Views from plasma catecholamine metabolites and serotonin transporter polymorphism. J. Psychopharmacol. 2009, 24, 1764–1771. [Google Scholar] [CrossRef]
- Gonul, A.S.; Akdeniz, F.; Taneli, F.; Donat, O.; Eker, M.C.; Vahip, S. Effect of treatment on serum brain–derived neurotrophic factor levels in depressed patients. Eur. Arch. Psychiatry Clin. Neurosci. 2005, 255, 381–386. [Google Scholar] [CrossRef]
- Aydemir, C.; Yalcin, E.S.; Aksaray, S.; Kisa, C.; Yildirim, S.G.; Uzbay, T.; Goka, E. Brain-derived neurotrophic factor (BDNF) changes in the serum of depressed women. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2006, 30, 1256–1260. [Google Scholar] [CrossRef]
- Yoshimura, R.; Mitoma, M.; Sugita, A.; Hori, H.; Okamoto, T.; Umene, W.; Ueda, N.; Nakamura, J. Effects of paroxetine or milnacipran on serum brain-derived neurotrophic factor in depressed patients. Prog. Neuro-Psychopharmacol. Biol. Psychiatry 2007, 31, 1034–1037. [Google Scholar] [CrossRef]
- Ghosh, R.; Gupta, R.; Bhatia, M.; Tripathi, A.; Gupta, L. Comparison of efficacy, safety and brain derived neurotrophic factor (BDNF) levels in patients of major depressive disorder, treated with fluoxetine and desvenlafaxine. Asian J. Psychiatry 2015, 18, 37–41. [Google Scholar] [CrossRef]
- Katsuki, A.; Yoshimura, R.; Kishi, T.; Hori, H.; Umene-Nakano, W.; Ikenouchi-Sugita, A.; Hayashi, K.; Atake, K.; Iwata, N.; Nakamura, J. Serum levels of brain-derived neurotrophic factor (BDNF), BDNF gene Val66Met polymorphism, or plasma catecholamine metabolites, and response to mirtazapine in Japanese patients with major depressive disorder (MDD). CNS Spectrums 2012, 17, 155–163. [Google Scholar] [CrossRef]
- Deuschle, M.; Gilles, M.; Scharnholz, B.; Lederbogen, F.; Lang, U.E.; Hellweg, R. Changes of Serum Concentrations of Brain-Derived Neurotrophic Factor (BDNF) during Treatment with Venlafaxine and Mirtazapine: Role of Medication and Response to Treatment. Pharmacopsychiatry 2012, 46, 54–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mikoteit, T.; Beck, J.; Eckert, A.; Hemmeter, U.; Brand, S.; Bischof, R.; Holsboer-Trachsler, E.; Delini-Stula, A. High baseline BDNF serum levels and early psychopathological improvement are predictive of treatment outcome in major depression. Psychopharmacol. 2014, 231, 2955–2965. [Google Scholar] [CrossRef]
- Fornaro, M.; Rocchi, G.; Escelsior, A.; Contini, P.; Martino, M. Might different cytokine trends in depressed patients receiving duloxetine indicate differential biological backgrounds. J. Affect. Disord. 2013, 145, 300–307. [Google Scholar] [CrossRef] [PubMed]
- Pezet, S.; Malcangio, M.; McMahon, S.B. BDNF: A neuromodulator in nociceptive pathways? Brain Res. Rev. 2002, 40, 240–249. [Google Scholar] [CrossRef]
- Rauti, R.; Cellot, G.; D’Andrea, P.; Colliva, A.; Scaini, D.; Tongiorgi, E.; Ballerini, L. BDNF impact on synaptic dynamics: Extra or intracellular long-term release differently regulates cultured hippocampal synapses. Mol. Brain 2020, 13, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Sharma, T.; Guski, L.S.; Freund, N.; Gøtzsche, P.C. Suicidality and aggression during antidepressant treatment: Systematic review and meta-analyses based on clinical study reports. BMJ 2016, 352, i65. [Google Scholar] [CrossRef] [Green Version]
- Phillips, M.L.; Chase, H.W.; Sheline, Y.I.; Etkin, A.; Almeida, J.R.; Deckersbach, T.; Trivedi, M.H. Identifying Predictors, Moderators, and Mediators of Antidepressant Response in Major Depressive Disorder: Neuroimaging Approaches. Am. J. Psychiatry 2015, 172, 124–138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Belzeaux, R.; Lin, C.-W.; Ding, Y.; Bergon, A.; Ibrahim, E.C.; Turecki, G.; Tseng, G.; Sibille, E. Predisposition to treatment response in major depressive episode: A peripheral blood gene coexpression network analysis. J. Psychiatr. Res. 2016, 81, 119–126. [Google Scholar] [CrossRef]
- Jacobs, B.L.; Fornal, C.A. Chronic fluoxetine treatment increases hippocampal neurogenesis in rats: A novel theory of depression. Soc. Neurosci. Abstr. 1999, 25, 714. [Google Scholar]
- Mahar, I.; Bambico, F.R.; Mechawar, N.; Nobrega, J.N. Stress, serotonin, and hippocampal neurogenesis in relation to depression and antidepressant effects. Neurosci. Biobehav. Rev. 2014, 38, 173–192. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Study | Year of Study | Grading System by Siwek et al. [54] | Type of Study | Patient Group (n) | Duration of Study (Weeks) | Markers | Medication | Influence of Drugs on Markers | Results |
|---|---|---|---|---|---|---|---|---|---|
| Polyakova et al. [36] | 2014 | A | Meta-Analysis | n = 2298 | 2–8 | serum BDNF | Paroxetine, Escitalopram, Citalopram, Sertraline, Fluoxetine, Venlafaxine, Duloxetine Mirtazapine, Tranylcypromine, Amitriptyline, Clomipramine | YES | Serum BDNF was significantly decreased in patients in a depressive state compared with controls. The BDNF levels increased upon treatment in remitters and responders, whereas in the non-responders they remained stable. Serum BDNF changes in remitters and responders were significantly larger than in the non-responders. |
| Zhou et al. [37] | 2017 | A | Meta-Analysis | n = 633 | serum and plasma BDNF | venlafaxine, paroxetine, sertraline, esciltalopram | +/− | Significant decreased HDRS score. Sertraline—statistically significant effect on the serum BDNF levels pre- and post-antidepressant treatment. Plasma BDNF—no effect. | |
| Arumugam et al. [38] | 2017 | A | Meta-Analysis | n = 154 | 5–12 | serum BDNF | Venlafaxine, Fluoxetine, Paroxetine, Citalopram, Sertraline, Milnacipran | +/− | Antidepressant therapy is associated with a change in BDNF level, but did not produce any significant impact on it. HDRS score signified a positive antidepressant treatment outcome. |
| Chiou et al. [39] | 2017 | A | Longitudinal study | n = 142 (drug-naïve first-episode MDD = 71 healthy controls = (71) | 4 | serum BDNF | escitalopram fluoxetine mirtazapine paroxetine venlafaxine | NO | The serum BDNF levels post-treatment were not significantly elevated. |
| Brunoni et al. [19] | 2014 | A | Randomized Controlled Trial | n = 103 (73 had their baseline and endpoint BDNF plasma levels analyzed) | 6 | plasma BDNF | sertraline, | NO | Sertraline did not change BDNF plasma levels over time and according to clinical improvement. There were no significant correlations between MADRS or HDRS scores changes with BDNF plasma changes. |
| Gupta et al. [40] | 2017 | B | Clinical Trial | n = 60 (agomelatine = 30 fluoxetine = 30) | 12 | serum BDNF | Fluoxetine, Agomelatine | YES | Agomelatine responders—serum BDNF level significantly increased at 12 weeks after treatment. Fluoxetine responders group—serum BDNF level significantly increased after 12 weeks of treatment. |
| Troyan & Levada. [45] | 2020 | B | Clinical Trial | n = 73 (treatment group = 30 healthy controls HC = 32 MDD = 41) | 8 | serum BDNF (sBDNF) | Vortioxetin | YES | BDNF levels were significantly higher post-treatment; moreover, they were prominently higher than in healthy controls (HC). Prominent inverse relationships was estabilished between BDNF concentrations and MDD status. |
| Sagud et al. [42] | 2016 | B | Longitudinal study | n = 88 (healthy controls = 44, MDD = 44) | 4 | plasma BDNF | Vortioxetine | YES | Vortioxetine treatment significantly increased plasma BDNF concentration in depressed patients compared to their baseline values. |
| Zheng et al. [43] | 2021 | C | Clinical Trial | n = 94 | 26 days | plasma BDNF | Ketamine | YES | Correlation and regression analyses showed significant associations between pBDNF concentrations at baseline and MADRS scores at 13 d and 26 d in depressed patients. |
| Study | Year of Study | Grading System by Siwek et al. [54] | Type of Study | Patient Group (n) | Duration of Study (Weeks) | Markers | Medication | Influence of Drugs on Markers | Results |
|---|---|---|---|---|---|---|---|---|---|
| Troyan & Levada. [42] | 2020 | B | Clinical Trial | n = 73 (treatment group = 30 healthy controls HC = 32 MDD = 41) | 8 | serum IGF-1 | Vortioxetin | YES | IGF-1 concentrations in MDD group post-treatment were significantly lower than pre-treatment and not significantly different from HC. Positive correlation was found between IGF-1 level and MDD status. |
| Bot et al. [45] | 2016 | B | Clinical Trial | n = 2714 (HC = 602) | 2 years | Serum IGF-1 | Fluoxetine Citalopram, Paroxetine, Sertraline Fluvoxamine, Venlafaxine, Clomipramine, Amitriptyline, Mirtazapine | YES | IGF-1 concentrations in MDD group post-treatment were significantly lower than pre-treatment and not significantly different from HC. Positive correlation was found between IGF-1 level and MDD status. |
| Levada et al. [46] | 2020 | B | Clinical Trial | completed = 48 (MDD = 78 HC = 47) | 8 | serum IGF-1 | Vortioxetine | YES | Vortioxetine treatment significantly attenuated IGF-1 levels and improved all psychopathological and neuropsychological parameters. MDD patients had significantly higher serum IGF-1 levels than controls. IGF-1 had a good diagnostic value for predicting MDD in the whole sample with AUC. IGF-1 level has decreased after vortixetine treatment. |
| Kopczak et al. [47] | 2015 | B | Clinical Trial | n = 170 (MDD = 78 HC = 92) | 6 | Serum IGF-1 | SSRI (selective serotonin reuptake inhibitors) SNRI (serotonin–norepinephrine reuptake inhibitor) TCA (tricyclic antidepressants) Mirtazapine | YES | IGF-I levels were significantly higher in patients at admission and in week 6 compared to HC. |
| Group of Antideoressants | Medication | Study | Duration of the Study (Weeks) | Patient Group (n) | Effect * |
|---|---|---|---|---|---|
| BDNF | |||||
| SSRI | Sertraline | Wolkowitz et al. [21] | 8 | n = 10 | ↑ |
| Brunoni et al. [19] | 6 | n = 18 | ↓ | ||
| Umene-Nakano et al. [58] | 8 | n = 59 | ↑ (responders only) | ||
| Matrisciano et al. [54] | 6 months | n = 7 | ↑ | ||
| Gonul et al. [59] | 8 | n = 8 | ↑ | ||
| Escitalopram | Wolkowitz et al. [21] | 8 | n = 15 | ↑ | |
| Matrisciano et al. [54] | 6 months | n = 7 | ↑ | ||
| Aydemir et al. [60] | 6 | n = 20 | ↑ | ||
| Chiou et al. [39] | 4 | n = 2 | ↓ | ||
| Paroxetine | Yoshimura et al. [61] | 8 | n = 21 | ↑ | |
| Gonul et al. [59] | 8 | n = 3 | ↑ | ||
| Chiou et al. [39] | 4 | n = 7 | ↓ | ||
| Hellweg et al. [56] | 36 days | n = 20 | ↓ | ||
| Fluoxetine | Başterzi et al. [55] | 6 | n = 22 | ↑/↓ | |
| Gupta et al. [40] | 12 | n = 30 | ↑ | ||
| Gonul et al. [59] | 8 | n = 5 | ↑ | ||
| Ghosh et al. [62] | 12 | n = 30 | ↑ | ||
| Chiou et al. [39] | 44 | n = 21 | ↓ | ||
| SNRI | Vortixetine | Troyan et al. [41] | 8 | n = 30 | ↑ |
| Sagud et al. [42] | 4 | n = 44 | ↑ | ||
| Venlafaxine | Başterzi et al. [55] | 6 | n = 21 | ↓ | |
| Matrisciano et al. [54] | 6 months | n = 7 | ↑ (after 6 months of treatment) | ||
| Katsuki et al. [63] | 4 | n = 48 | ↑ | ||
| Gonul et al. [59] | 8 | n = 10 | ↑ | ||
| Chiou et al. [39] | 4 | n = 8 | ↓ | ||
| Deuschle et al. (2012) [64] | 28 days | n = 27 | ↔ | ||
| Duloxetine | Mikoteit et al. [65] | 6 | n = 21 | ↑ | |
| Other | Mirtazapine | Fornaro et al. [66] | 12 | n = 30 | ↑ early non-responders, ↔ early responders |
| Deuschle et al. (2012) [64] | 28 days | n = 29 | ↑ | ||
| Chiou et al. [39] | 4 | n = 3 | ↓ | ||
| Ketamine | Zheng et al. [43] | 26 days | n = 94 | ↑ | |
| Milnacipran | Yoshimura et al. [61] | 8 | n = 21 | ↑ | |
| Amitryptyline | Hellweg et al. [56] | 36 days | n = 20 | ↑ | |
| IGF-1 | |||||
| SSRI | N/A | Kopczak et al. [46] | 6 | n = 13 | ↓ |
| Fluoxetine Citalopram Paroxetine Sertraline Fluvoxamine | Bot et al. [44] | N/A | n = 52 n= 96 n = 195 n = 40 n = 38 | ↓ ↓ ↓ ↓ ↓ | |
| SNRI | N/A | Kopczak et al. [46] | 6 | n = 12 | ↓ |
| Vortioxetine | Troyan et al. [41] | 8 | n = 41 | ↓ | |
| Levada et al. [45] | 8 | n = 48 | ↓ | ||
| Venlafaxine | Bot et al. [44] | N/A | n = 95 | ↓ | |
| TCA | Clomipramine Amitriptyline | Bot et al. [44] | N/A | n = 26 n = 21 | ↓ ↓ (not statistically significant) |
| N/A | Kopczak et al. [46] | 6 | n = 14 | ↓ | |
| Other | Mirtazapine | Kopczak et al. [46] | 6 | n = 8 | ↓ |
| Bot et al. [44] | N/A | n = 33 | ↓ (not statistically significant) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mosiołek, A.; Mosiołek, J.; Jakima, S.; Pięta, A.; Szulc, A. Effects of Antidepressant Treatment on Neurotrophic Factors (BDNF and IGF-1) in Patients with Major Depressive Disorder (MDD). J. Clin. Med. 2021, 10, 3377. https://doi.org/10.3390/jcm10153377
Mosiołek A, Mosiołek J, Jakima S, Pięta A, Szulc A. Effects of Antidepressant Treatment on Neurotrophic Factors (BDNF and IGF-1) in Patients with Major Depressive Disorder (MDD). Journal of Clinical Medicine. 2021; 10(15):3377. https://doi.org/10.3390/jcm10153377
Chicago/Turabian StyleMosiołek, Anna, Jadwiga Mosiołek, Sławomir Jakima, Aleksandra Pięta, and Agata Szulc. 2021. "Effects of Antidepressant Treatment on Neurotrophic Factors (BDNF and IGF-1) in Patients with Major Depressive Disorder (MDD)" Journal of Clinical Medicine 10, no. 15: 3377. https://doi.org/10.3390/jcm10153377
APA StyleMosiołek, A., Mosiołek, J., Jakima, S., Pięta, A., & Szulc, A. (2021). Effects of Antidepressant Treatment on Neurotrophic Factors (BDNF and IGF-1) in Patients with Major Depressive Disorder (MDD). Journal of Clinical Medicine, 10(15), 3377. https://doi.org/10.3390/jcm10153377