
Virtual Reality Interventions for Needle-Related Procedural Pain, Fear and Anxiety—A Systematic Review and Meta-Analysis

 , , ,
, , ,  , and
, and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
2.1. Electronic Searches
2.2. Study Selection
2.3. Outcomes
2.4. Data Extraction and Management
2.5. Assessment of Risk of Bias in Included Studies
2.6. Data Synthesis and Statistical Analysis
3. Results
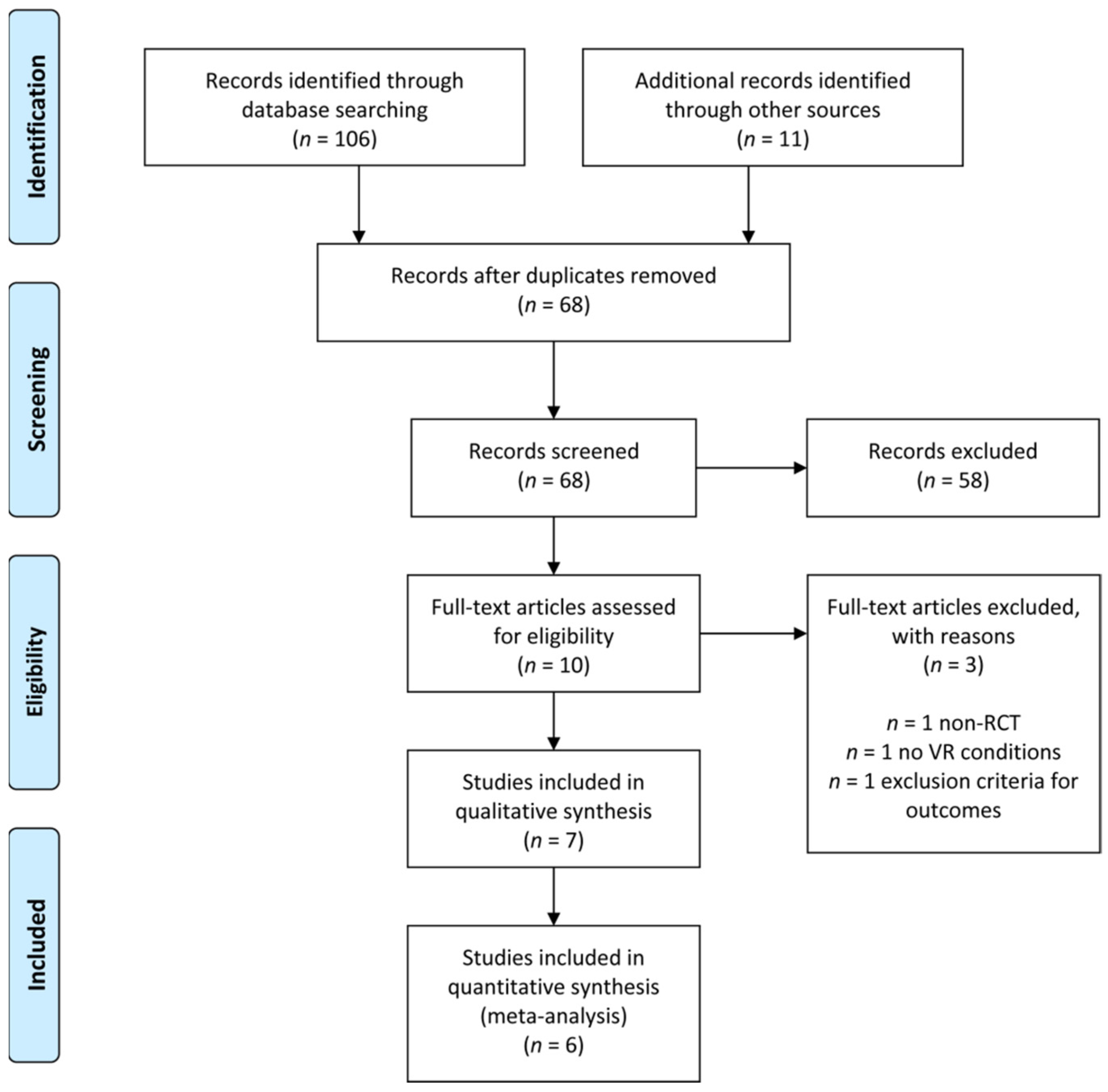
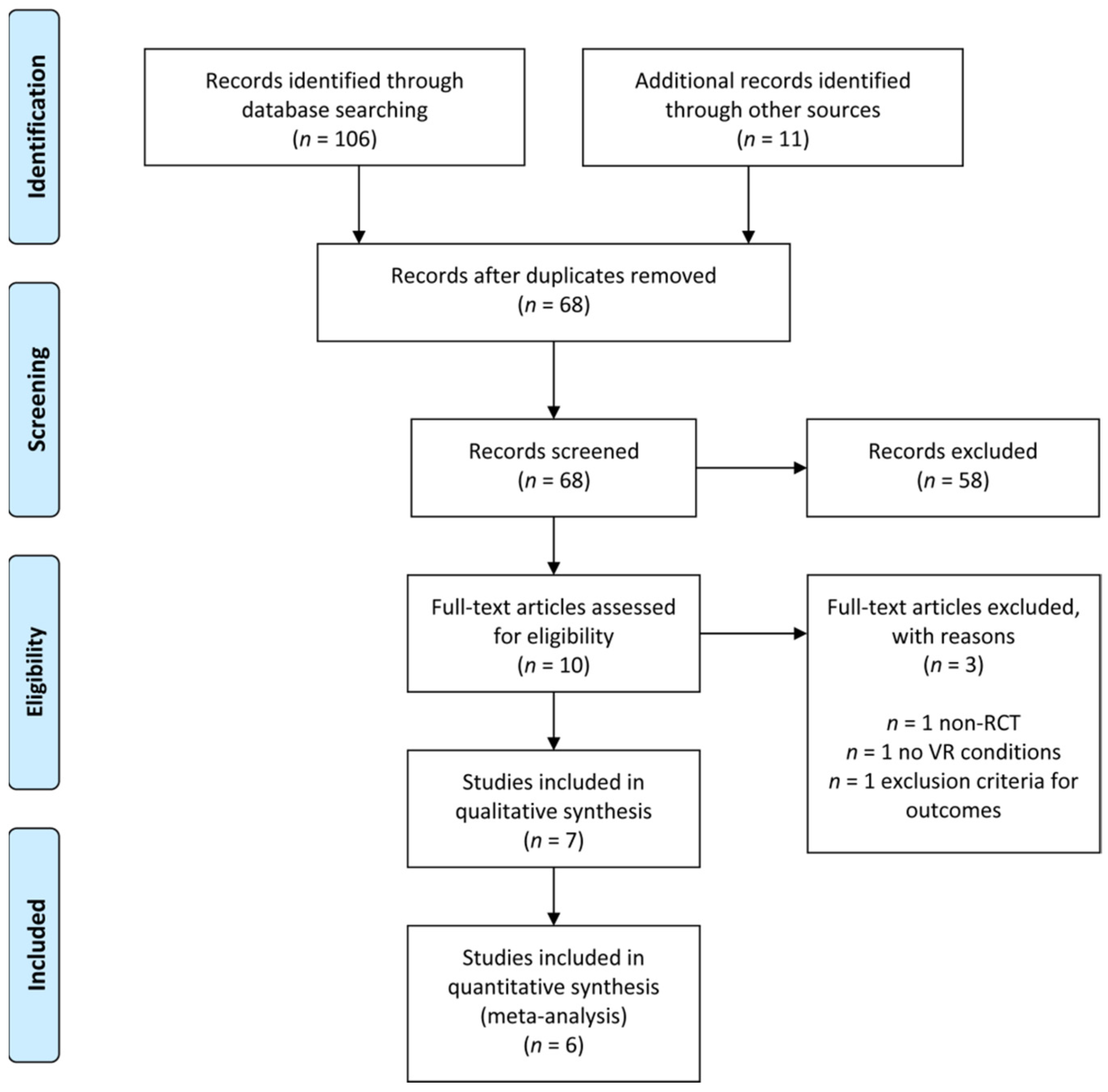
3.1. Included Studies
3.1.1. Characteristic of Included Studies
3.1.2. Effect Size of Included Studies
3.2. Excluded Studies
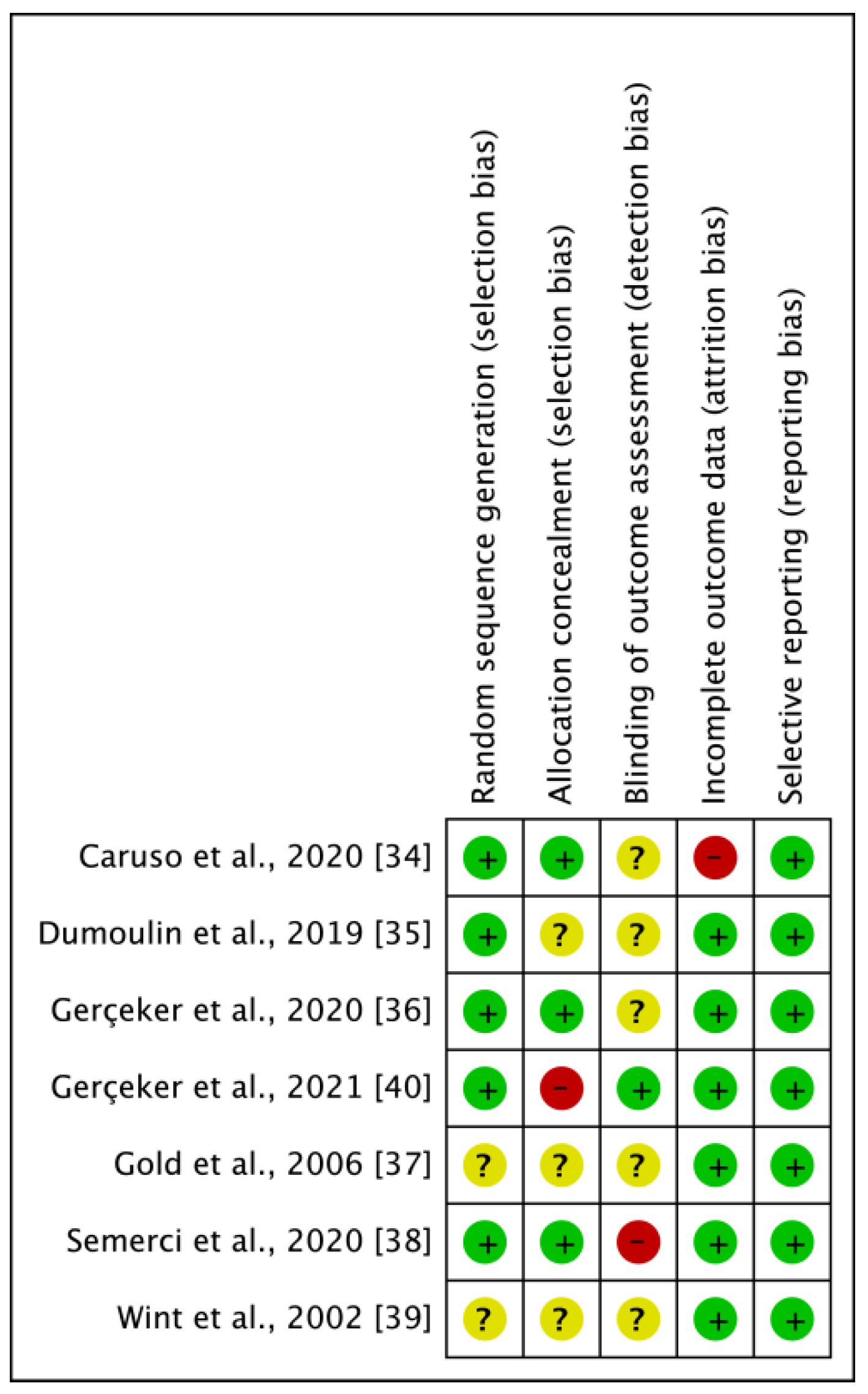
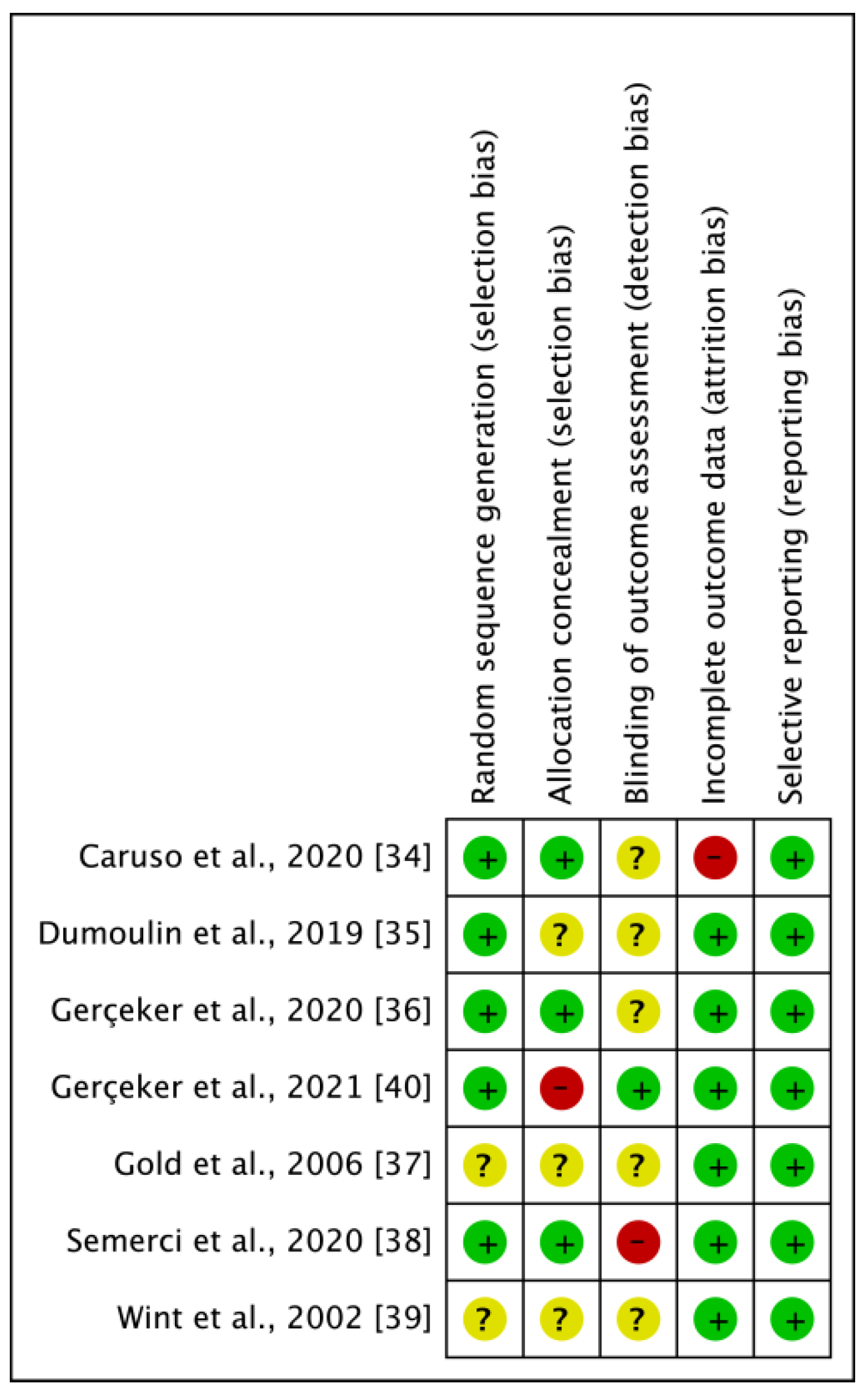
3.3. Risk of Bias of the Included Studies
3.4. Effects of Intervention
3.4.1. Comparison of VR Treatment and Standard Care. Outcome: Pain
3.4.2. Comparison of VR Treatment and Standard Care. Outcome: Fear
3.4.3. Comparison of VR Treatment and Standard Care. Outcome: Anxiety
3.4.4. Comparison of VR Treatment and Standard Care. Outcome: Satisfaction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Waddell, G.; Newton, M.; Henderson, I.; Somerville, D.; Main, C.J. A Fear-Avoidance Beliefs Questionnaire (FABQ) and the role of fear-avoidance beliefs in chronic low back pain and disability. Pain 1993, 52, 157–168. [Google Scholar] [CrossRef]
- Lyby, P.S.; Aslaksen, P.M.; Flaten, M.A. Variability in placebo analgesia and the role of fear of pain—An ERP study. Pain 2011, 152, 2405–2412. [Google Scholar] [CrossRef] [PubMed]
- Crombez, G.; Eccleston, C.; Van Damme, S.; Vlaeyen, J.W.; Karoly, P. Fear-avoidance model of chronic pain: The next generation. Clin. J. Pain 2012, 28, 475–483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Asmundson, G.J.; Parkerson, H.A.; Petter, M.; Noel, M. What is the role of fear and escape/avoidance in chronic pain? Models, structural analysis and future directions. Pain Manag. 2012, 2, 295–303. [Google Scholar] [CrossRef] [PubMed]
- Simons, L.E.; Kaczynski, K.J. The Fear Avoidance model of chronic pain: Examination for pediatric application. J. Pain 2012, 13, 827–835. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cavender, K.; Goff, M.D.; Hollon, E.C.; Guzzetta, C.E. Parents’ positioning and distracting children during venipuncture. Effects on children’s pain, fear, and distress. J. Holist. Nurs. 2004, 22, 32–56. [Google Scholar] [CrossRef] [PubMed]
- McLenon, J.; Rogers, M.A.M. The fear of needles: A systematic review and meta-analysis. J. Adv. Nurs. 2019, 75, 30–42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zeltzer, L.K.; Altman, A.; Cohen, D.; LeBaron, S.; Munuksela, E.L.; Schechter, N.L. American Academy of Pediatrics Report of the Subcommittee on the Management of Pain Associated with Procedures in Children with Cancer. Pediatrics 1990, 86, 826–831. [Google Scholar] [PubMed]
- Nguyen, T.N.; Nilsson, S.; Hellstrom, A.L.; Bengtson, A. Music therapy to reduce pain and anxiety in children with cancer undergoing lumbar puncture: A randomized clinical trial. J. Pediatr. Oncol. Nurs. 2010, 27, 146–155. [Google Scholar] [CrossRef]
- Post-White, J.; Fitzgerald, M.; Savik, K.; Hooke, M.C.; Hannahan, A.B.; Sencer, S.F. Massage therapy for children with cancer. J. Pediatr. Oncol. Nurs. 2009, 26, 16–28. [Google Scholar] [CrossRef]
- McKenna, K.; Gallagher, K.A.; Forbes, P.W.; Ibeziako, P. Ready, set, relax: Biofeedback-assisted relaxation training (BART) in a pediatric psychiatry consultation service. Psychosomatics 2015, 56, 381–389. [Google Scholar] [CrossRef]
- Manne, S.L.; Bakeman, R.; Jacobsen, P.B.; Gorfinkle, K.; Redd, W.H. An analysis of a behavioral intervention for children undergoing venipuncture. Health Psychol. 1994, 13, 556–566. [Google Scholar] [CrossRef]
- Erdogan, B.; Aytekin Ozdemir, A. The effect of three different methods on venipuncture pain and anxiety in children: Distraction cards, virtual reality, and Buzzy(R) (randomized controlled trial). J. Pediatr. Nurs. 2021. [Google Scholar] [CrossRef]
- Burns-Nader, S.; Joe, L.; Pinion, K. Computer tablet distraction reduces pain and anxiety in pediatric burn patients undergoing hydrotherapy: A randomized trial. Burns 2017, 43, 1203–1211. [Google Scholar] [CrossRef]
- Lee, D.W.; Chan, A.C.; Wong, S.K.; Fung, T.M.; Li, A.C.; Chan, S.K.; Mui, L.M.; Ng, E.K.; Chung, S.C. Can visual distraction decrease the dose of patient-controlled sedation required during colonoscopy? A prospective randomized controlled trial. Endoscopy 2004, 36, 197–201. [Google Scholar] [CrossRef]
- Li, A.; Montano, Z.; Chen, V.J.; Gold, J.I. Virtual reality and pain management: Current trends and future directions. Pain Manag. 2011, 1, 147–157. [Google Scholar] [CrossRef] [Green Version]
- Rutkowski, S. Management Challenges in Chronic Obstructive Pulmonary Disease in the COVID-19 Pandemic: Telehealth and Virtual Reality. J. Clin. Med. 2021, 10, 1261. [Google Scholar] [CrossRef] [PubMed]
- Matamala-Gomez, M.; Maselli, A.; Malighetti, C.; Realdon, O.; Mantovani, F.; Riva, G. Virtual Body Ownership Illusions for Mental Health: A Narrative Review. J. Clin. Med. 2021, 10, 139. [Google Scholar] [CrossRef]
- Szczepanska-Gieracha, J.; Cieslik, B.; Rutkowski, S.; Kiper, P.; Turolla, A. What can virtual reality offer to stroke patients? A narrative review of the literature. NeuroRehabilitation 2020, 47, 109–120. [Google Scholar] [CrossRef]
- Asl Aminabadi, N.; Erfanparast, L.; Sohrabi, A.; Ghertasi Oskouei, S.; Naghili, A. The Impact of Virtual Reality Distraction on Pain and Anxiety during Dental Treatment in 4-6 Year-Old Children: A Randomized Controlled Clinical Trial. J. Dent. Res. Dent. Clin. Dent. Prospect. 2012, 6, 117–124. [Google Scholar] [CrossRef]
- Custodio, N.B.; Costa, F.D.; Cadernartori, M.G.; da Costa, V.P.P.; Goettems, M.L. Effectiveness of Virtual Reality Glasses as a Distraction for Children During Dental Care. Pediatr. Dent. 2020, 42, 91–102. [Google Scholar]
- Eijlers, R.; Utens, E.; Staals, L.M.; de Nijs, P.F.A.; Berghmans, J.M.; Wijnen, R.M.H.; Hillegers, M.H.J.; Dierckx, B.; Legerstee, J.S. Systematic Review and Meta-analysis of Virtual Reality in Pediatrics: Effects on Pain and Anxiety. Anesth. Analg. 2019, 129, 1344–1353. [Google Scholar] [CrossRef] [PubMed]
- Cieslik, B.; Mazurek, J.; Rutkowski, S.; Kiper, P.; Turolla, A.; Szczepanska-Gieracha, J. Virtual reality in psychiatric disorders: A systematic review of reviews. Complement. Med. 2020, 52, 102480. [Google Scholar] [CrossRef] [PubMed]
- Rutkowski, S.; Kiper, P.; Cacciante, L.; Cieslik, B.; Mazurek, J.; Turolla, A.; Szczepanska-Gieracha, J. Use of virtual reality-based training in different fields of rehabilitation: A systematic review and meta-analysis. J. Rehabil. Med. 2020. [Google Scholar] [CrossRef]
- Szczepanska-Gieracha, J.; Cieslik, B.; Serweta, A.; Klajs, K. Virtual Therapeutic Garden: A Promising Method Supporting the Treatment of Depressive Symptoms in Late-Life: A Randomized Pilot Study. J. Clin. Med. 2021, 10, 1942. [Google Scholar] [CrossRef]
- Rutkowski, S.; Szczegielniak, J.; Szczepanska-Gieracha, J. Evaluation of the efficacy of immersive virtual reality therapy as a method supporting pulmonary rehabilitation: A randomized controlled trial. J. Clin. Med. 2021, 10, 352. [Google Scholar] [CrossRef]
- Rutkowski, S.; Rutkowska, A.; Jastrzebski, D.; Racheniuk, H.; Pawelczyk, W.; Szczegielniak, J. Effect of Virtual Reality-Based Rehabilitation on Physical Fitness in Patients with Chronic Obstructive Pulmonary Disease. J. Hum. Kinet. 2019, 69, 149–157. [Google Scholar] [CrossRef] [Green Version]
- Jastrzebski, D.; Zebrowska, A.; Rutkowski, S.; Rutkowska, A.; Warzecha, J.; Ziaja, B.; Palka, A.; Czyzewska, B.; Czyzewski, D.; Ziora, D. Pulmonary Rehabilitation with a Stabilometric Platform after Thoracic Surgery: A Preliminary Report. J. Hum. Kinet. 2018, 65, 79–87. [Google Scholar] [CrossRef] [Green Version]
- Laver, K.E.; Lange, B.; George, S.; Deutsch, J.E.; Saposnik, G.; Crotty, M. Virtual reality for stroke rehabilitation. Cochrane. Database. Syst. Rev. 2017, 11, CD008349. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Group, P. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Int. J. Surg. 2010, 8, 336–341. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.; Altman, D.G.; Gotzsche, P.C.; Juni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Cohen, D. Statistical Power Analysis for the Behavioral Sciences; Routledge: New York, NY, USA, 1988. [Google Scholar] [CrossRef]
- Morris, S.B. Estimating effect sizes from pretest-posttest-control group designs. Organ. Res. Methods 2008, 11, 364–386. [Google Scholar] [CrossRef]
- Caruso, T.J.; George, A.; Menendez, M.; De Souza, E.; Khoury, M.; Kist, M.N.; Rodriguez, S.T. Virtual reality during pediatric vascular access: A pragmatic, prospective randomized, controlled trial. Paediatr. Anaesth. 2020, 30, 116–123. [Google Scholar] [CrossRef]
- Dumoulin, S.; Bouchard, S.; Ellis, J.; Lavoie, K.L.; Vézina, M.P.; Charbonneau, P.; Tardif, J.; Hajjar, A. A Randomized Controlled Trial on the Use of Virtual Reality for Needle-Related Procedures in Children and Adolescents in the Emergency Department. Games. Health J. 2019, 8, 285–293. [Google Scholar] [CrossRef]
- Ozalp Gerceker, G.; Ayar, D.; Ozdemir, E.Z.; Bektas, M. Effects of virtual reality on pain, fear and anxiety during blood draw in children aged 5–12 years old: A randomised controlled study. J. Clin. Nurs. 2020, 29, 1151–1161. [Google Scholar] [CrossRef]
- Gold, J.I.; Kim, S.H.; Kant, A.J.; Joseph, M.H.; Rizzo, A.S. Effectiveness of virtual reality for pediatric pain distraction during i.v. placement. Cyberpsychol. Behav. 2006, 9, 207–212. [Google Scholar] [CrossRef]
- Semerci, R.; Akgun Kostak, M.; Eren, T.; Avci, G. Effects of Virtual Reality on Pain During Venous Port Access in Pediatric Oncology Patients: A Randomized Controlled Study. J. Pediatr. Oncol. Nurs. 2021, 38, 142–151. [Google Scholar] [CrossRef]
- Sander Wint, S.; Eshelman, D.; Steele, J.; Guzzetta, C.E. Effects of distraction using virtual reality glasses during lumbar punctures in adolescents with cancer. Oncol. Nurs. Forum 2002, 29, E8–E15. [Google Scholar] [CrossRef]
- Gerceker, G.O.; Bektas, M.; Aydinok, Y.; Oren, H.; Ellidokuz, H.; Olgun, N. The effect of virtual reality on pain, fear, and anxiety during access of a port with huber needle in pediatric hematology-oncology patients: Randomized controlled trial. Eur. J. Oncol. Nurs. 2021, 50, 101886. [Google Scholar] [CrossRef]
- Nilsson, S.; Finnstrom, B.; Kokinsky, E.; Enskar, K. The use of Virtual Reality for needle-related procedural pain and distress in children and adolescents in a paediatric oncology unit. Eur. J. Oncol. Nurs. 2009, 13, 102–109. [Google Scholar] [CrossRef]
- Ebrahimpour, F.; Sadeghi, N.; Najafi, M.; Iraj, B.; Shahrokhi, A. Effect of Playing Interactive Computer Game on Distress of Insulin Injection Among Type 1 Diabetic Children. Iran. J. Pediatr. 2015, 25, e427. [Google Scholar] [CrossRef] [Green Version]
- Dunn, A.; Patterson, J.; Biega, C.F.; Grishchenko, A.; Luna, J.; Stanek, J.R.; Strouse, R. A Novel Clinician-Orchestrated Virtual Reality Platform for Distraction During Pediatric Intravenous Procedures in Children With Hemophilia: Randomized Controlled Trial. JMIR Serious Games 2019, 7, e10902. [Google Scholar] [CrossRef]
- Lopez-Valverde, N.; Muriel-Fernandez, J.; Lopez-Valverde, A.; Valero-Juan, L.F.; Ramirez, J.M.; Flores-Fraile, J.; Herrero-Payo, J.; Blanco-Antona, L.A.; Macedo-de-Sousa, B.; Bravo, M. Use of Virtual Reality for the Management of Anxiety and Pain in Dental Treatments: Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 3086. [Google Scholar] [CrossRef]
- Seligman, L.D.; Hovey, J.D.; Chacon, K.; Ollendick, T.H. Dental anxiety: An understudied problem in youth. Clin. Psychol. Rev. 2017, 55, 25–40. [Google Scholar] [CrossRef] [PubMed]
- Uman, L.S.; Birnie, K.A.; Noel, M.; Parker, J.A.; Chambers, C.T.; McGrath, P.J.; Kisely, S.R. Psychological interventions for needle-related procedural pain and distress in children and adolescents. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klassen, J.A.; Liang, Y.; Tjosvold, L.; Klassen, T.P.; Hartling, L. Music for pain and anxiety in children undergoing medical procedures: A systematic review of randomized controlled trials. Ambul. Pediatr. 2008, 8, 117–128. [Google Scholar] [CrossRef] [PubMed]
- Luo, H.; Cao, C.; Zhong, J.; Chen, J.; Cen, Y. Adjunctive virtual reality for procedural pain management of burn patients during dressing change or physical therapy: A systematic review and meta-analysis of randomized controlled trials. Wound Repair Regen. 2019, 27, 90–101. [Google Scholar] [CrossRef] [Green Version]
- Hughes, S.W.; Zhao, H.; Auvinet, E.J.; Strutton, P.H. Attenuation of capsaicin-induced ongoing pain and secondary hyperalgesia during exposure to an immersive virtual reality environment. Pain Rep. 2019, 4, e790. [Google Scholar] [CrossRef]
- Hoffman, H.G.; Richards, T.L.; Coda, B.; Bills, A.R.; Blough, D.; Richards, A.L.; Sharar, S.R. Modulation of thermal pain-related brain activity with virtual reality: Evidence from fMRI. Neuroreport 2004, 15, 1245–1248. [Google Scholar] [CrossRef]
- Buhle, J.T.; Stevens, B.L.; Friedman, J.J.; Wager, T.D. Distraction and placebo: Two separate routes to pain control. Psychol. Sci. 2012, 23, 246–253. [Google Scholar] [CrossRef] [Green Version]
- Aydin, D.; Sahiner, N.C.; Ciftci, E.K. Comparison of the effectiveness of three different methods in decreasing pain during venipuncture in children: Ball squeezing, balloon inflating and distraction cards. J. Clin. Nurs. 2016, 25, 2328–2335. [Google Scholar] [CrossRef]
- Birnie, K.A.; Noel, M.; Parker, J.A.; Chambers, C.T.; Uman, L.S.; Kisely, S.R.; McGrath, P.J. Systematic review and meta-analysis of distraction and hypnosis for needle-related pain and distress in children and adolescents. J. Pediatr. Psychol. 2014, 39, 783–808. [Google Scholar] [CrossRef] [Green Version]
- Liu, Q.; Zhou, Y.; Xie, X.Y.; Xue, Q.; Zhu, K.H.; Wan, Z.H.; Wu, H.; Zhang, J.J.; Song, R.R. The prevalence of behavioral problems among school-aged children in home quarantine during the COVID-19 pandemic in china. J. Affect. Disord. 2021, 279, 412–416. [Google Scholar] [CrossRef]
- de Lima, C.V.C.; Candido, E.L.; da Silva, J.A.; Albuquerque, L.V.; Soares, L.D.; do Nascimento, M.M.; de Oliveira, S.A.; Neto, M.L.R. Effects of quarantine on mental health of populations affected by Covid-19. J. Affect. Disord. 2020, 275, 253–254. [Google Scholar] [CrossRef]





Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Czech, O.; Wrzeciono, A.; Rutkowska, A.; Guzik, A.; Kiper, P.; Rutkowski, S. Virtual Reality Interventions for Needle-Related Procedural Pain, Fear and Anxiety—A Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 3248. https://doi.org/10.3390/jcm10153248
Czech O, Wrzeciono A, Rutkowska A, Guzik A, Kiper P, Rutkowski S. Virtual Reality Interventions for Needle-Related Procedural Pain, Fear and Anxiety—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(15):3248. https://doi.org/10.3390/jcm10153248
Chicago/Turabian StyleCzech, Oliver, Adam Wrzeciono, Anna Rutkowska, Agnieszka Guzik, Paweł Kiper, and Sebastian Rutkowski. 2021. "Virtual Reality Interventions for Needle-Related Procedural Pain, Fear and Anxiety—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 15: 3248. https://doi.org/10.3390/jcm10153248
APA StyleCzech, O., Wrzeciono, A., Rutkowska, A., Guzik, A., Kiper, P., & Rutkowski, S. (2021). Virtual Reality Interventions for Needle-Related Procedural Pain, Fear and Anxiety—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 10(15), 3248. https://doi.org/10.3390/jcm10153248