
Atypia and Follicular Lesions of Undetermined Significance in Subsequent Biopsy Result: What Clinicians Need to Know

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
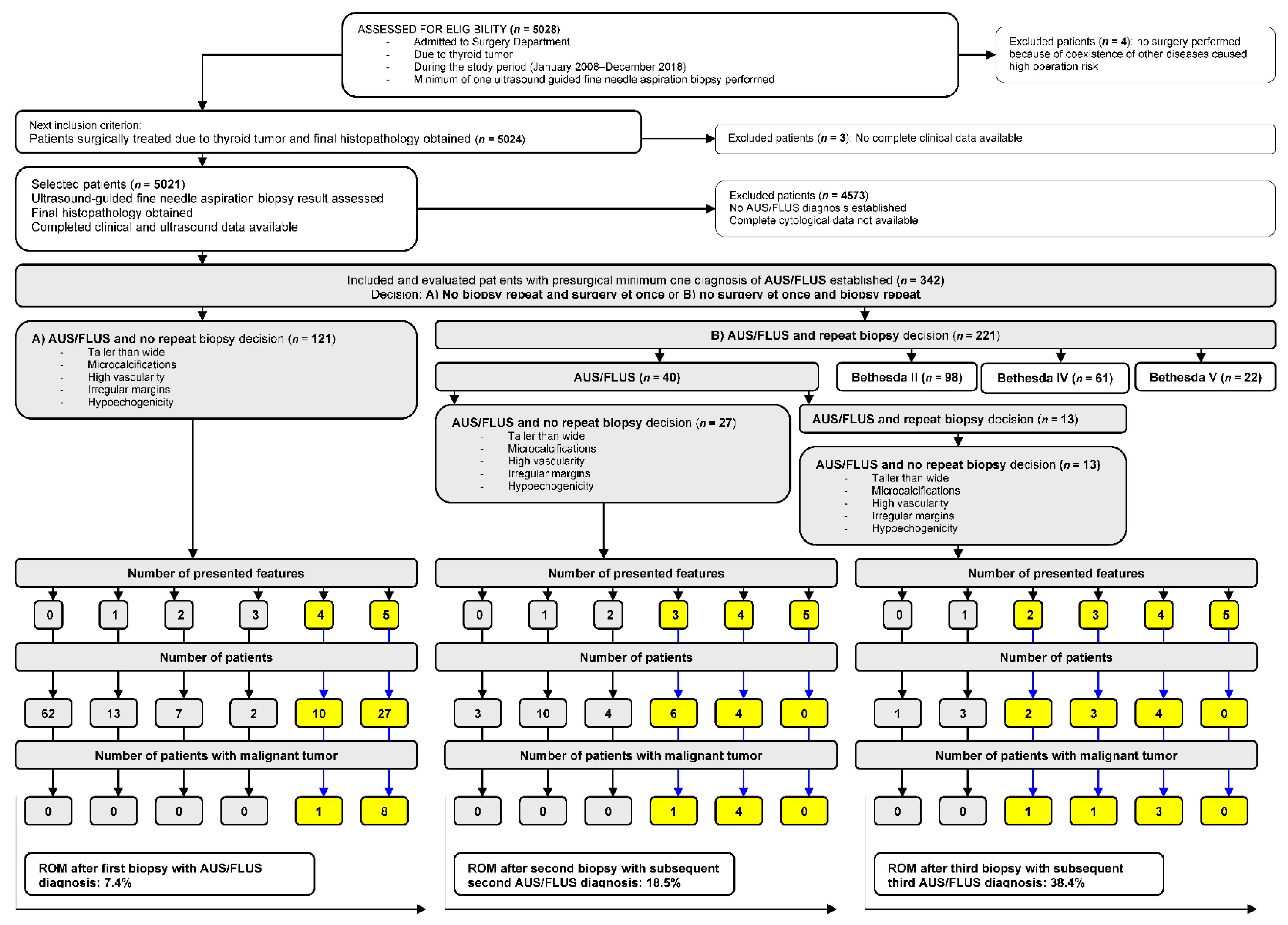
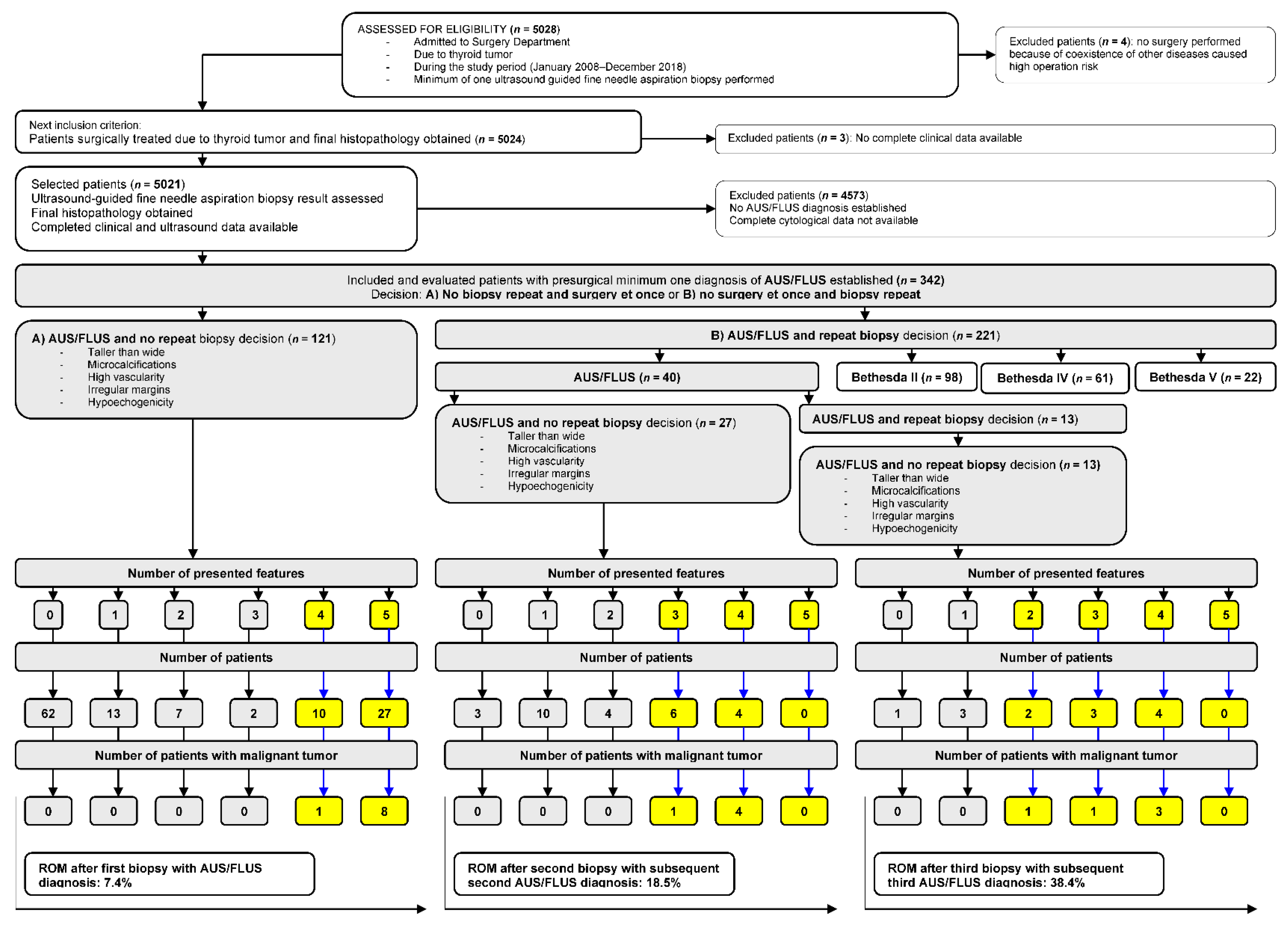
2.1. Study Population
2.2. Statistical Analysis
3. Results
3.1. Patients’ Characteristic
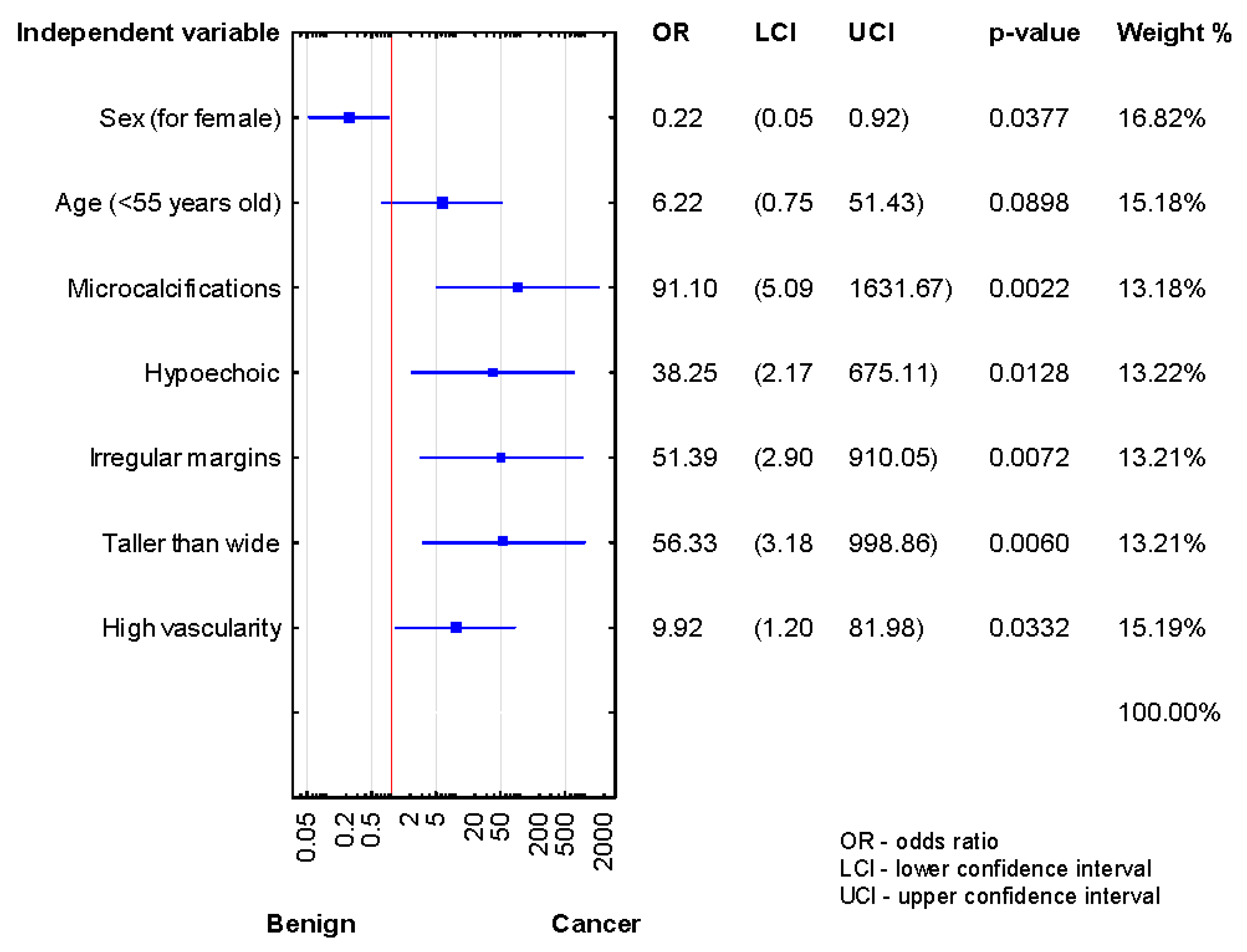
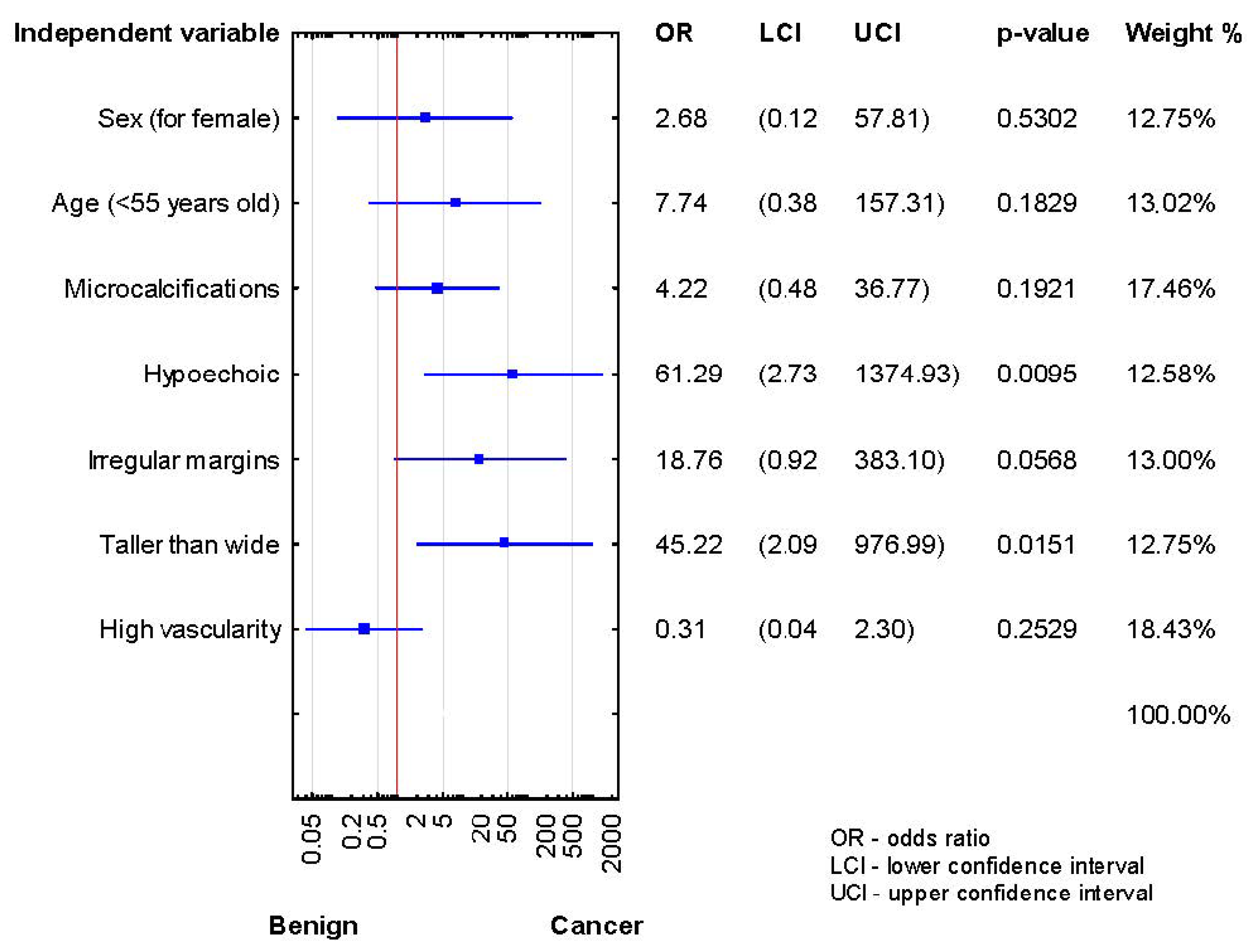
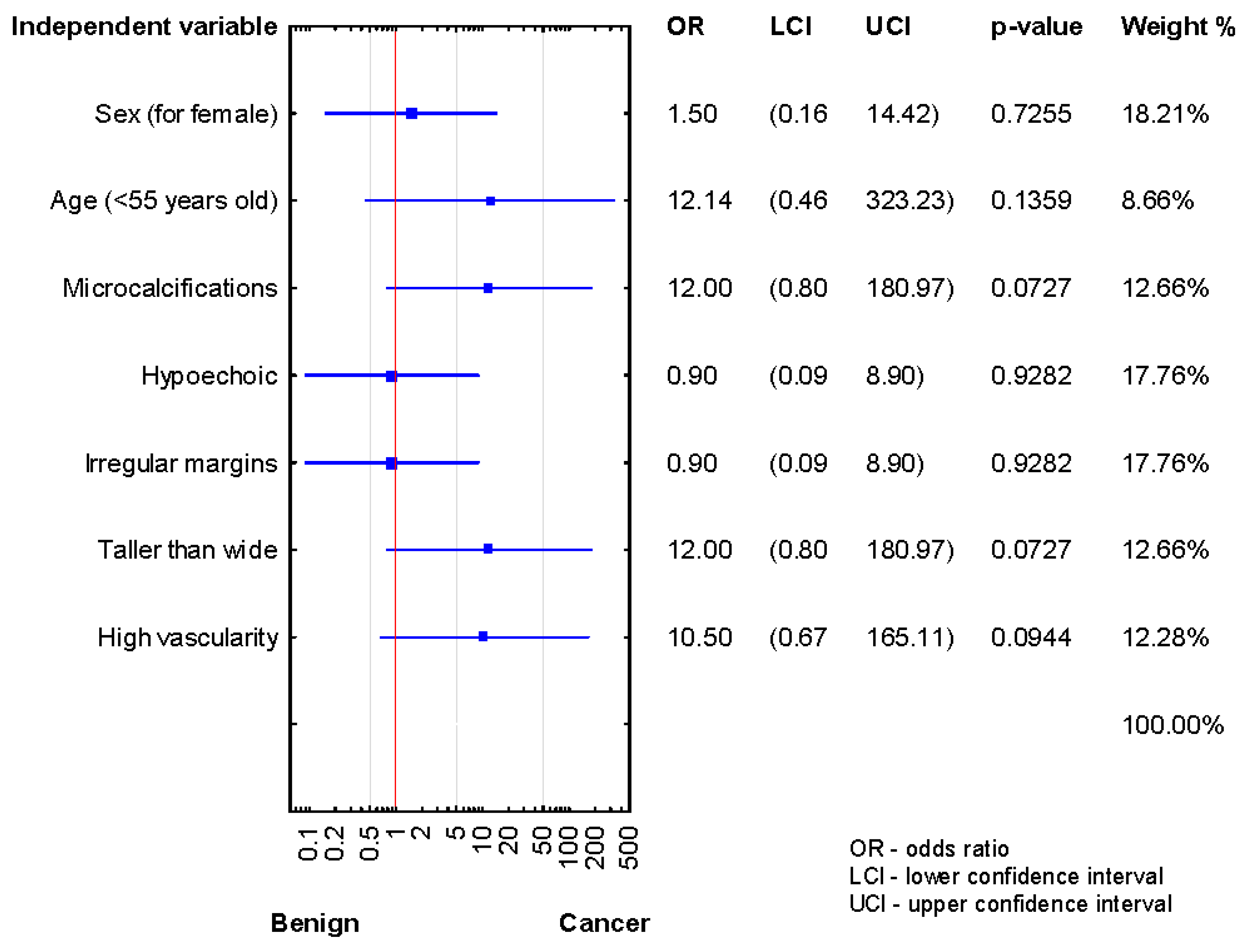
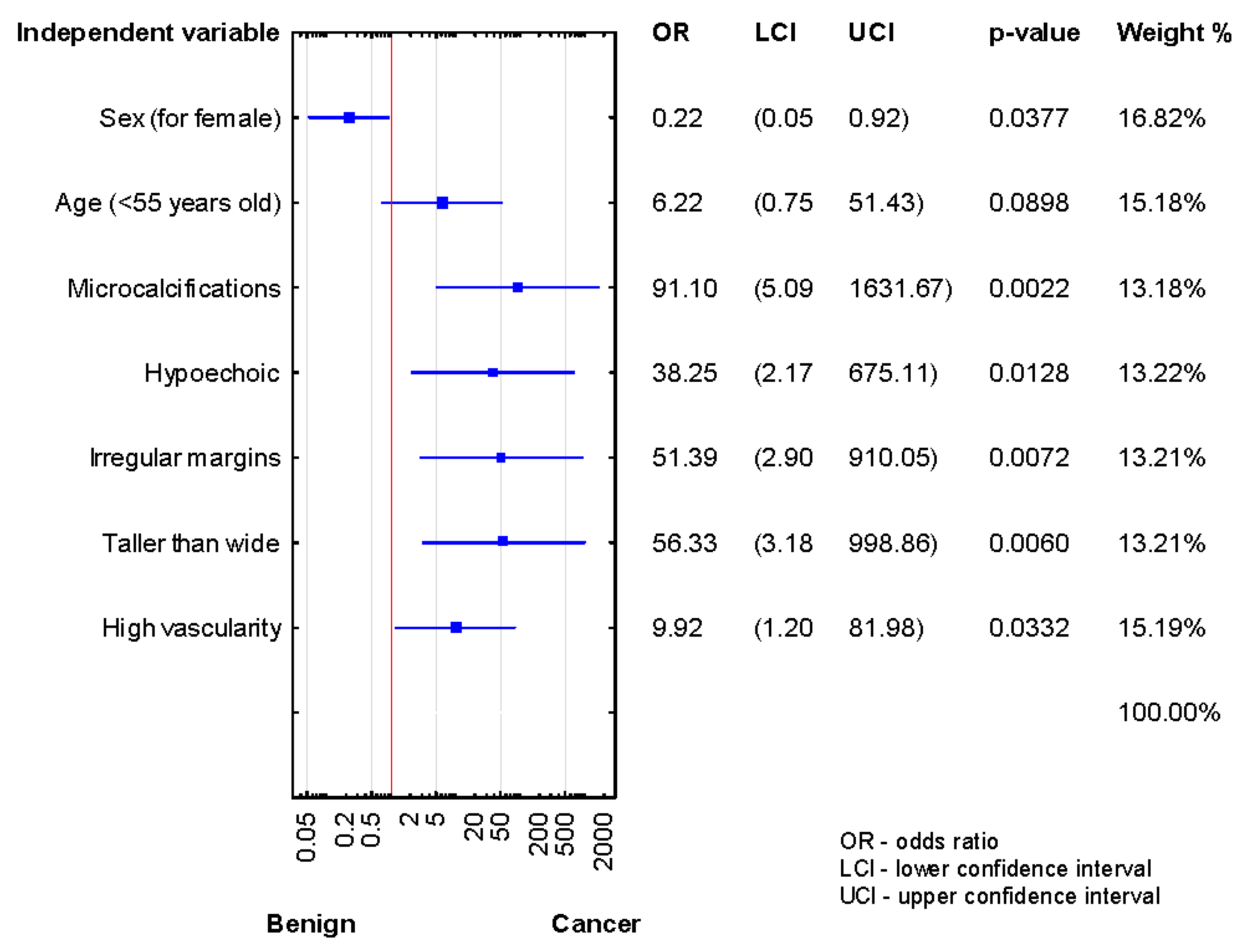
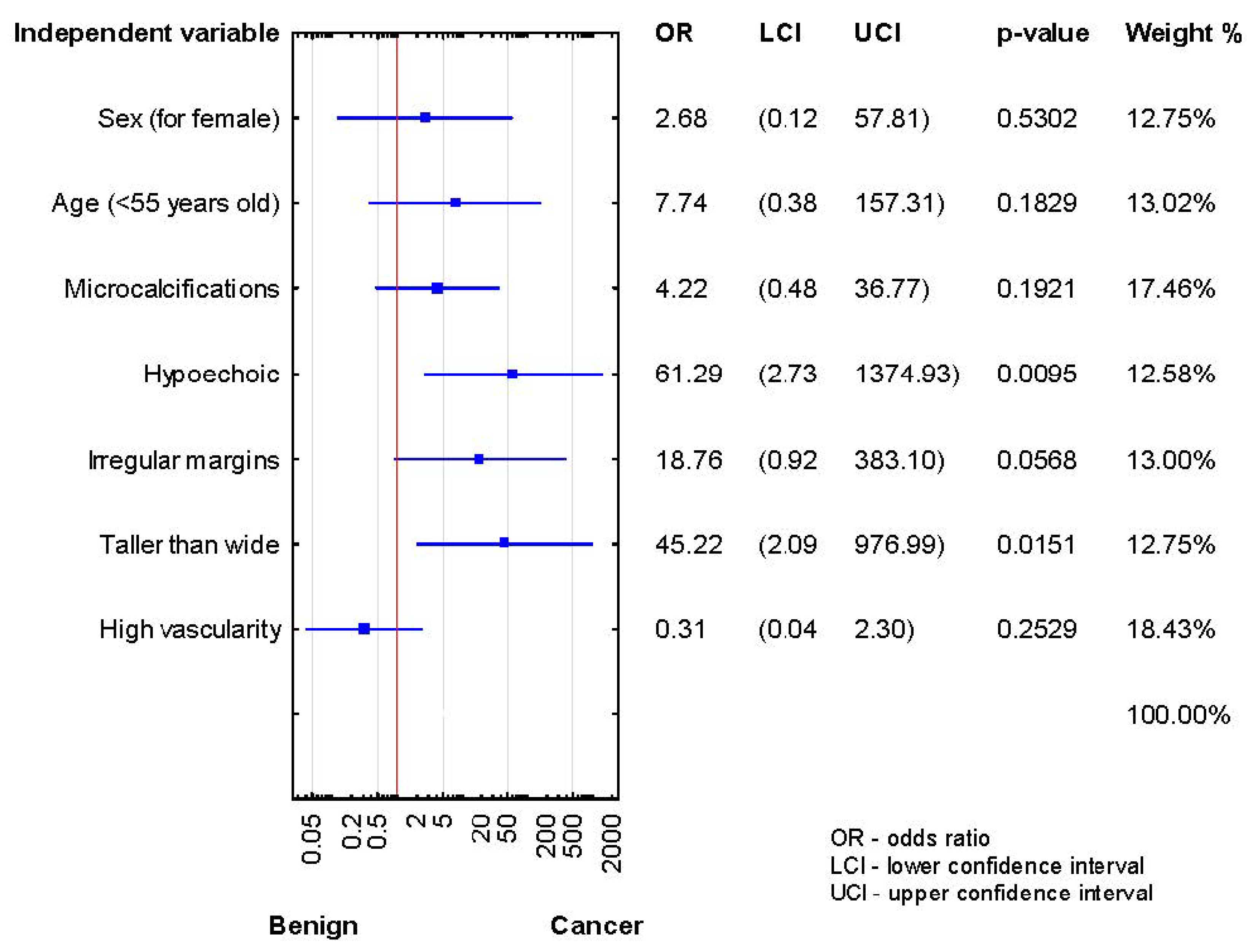
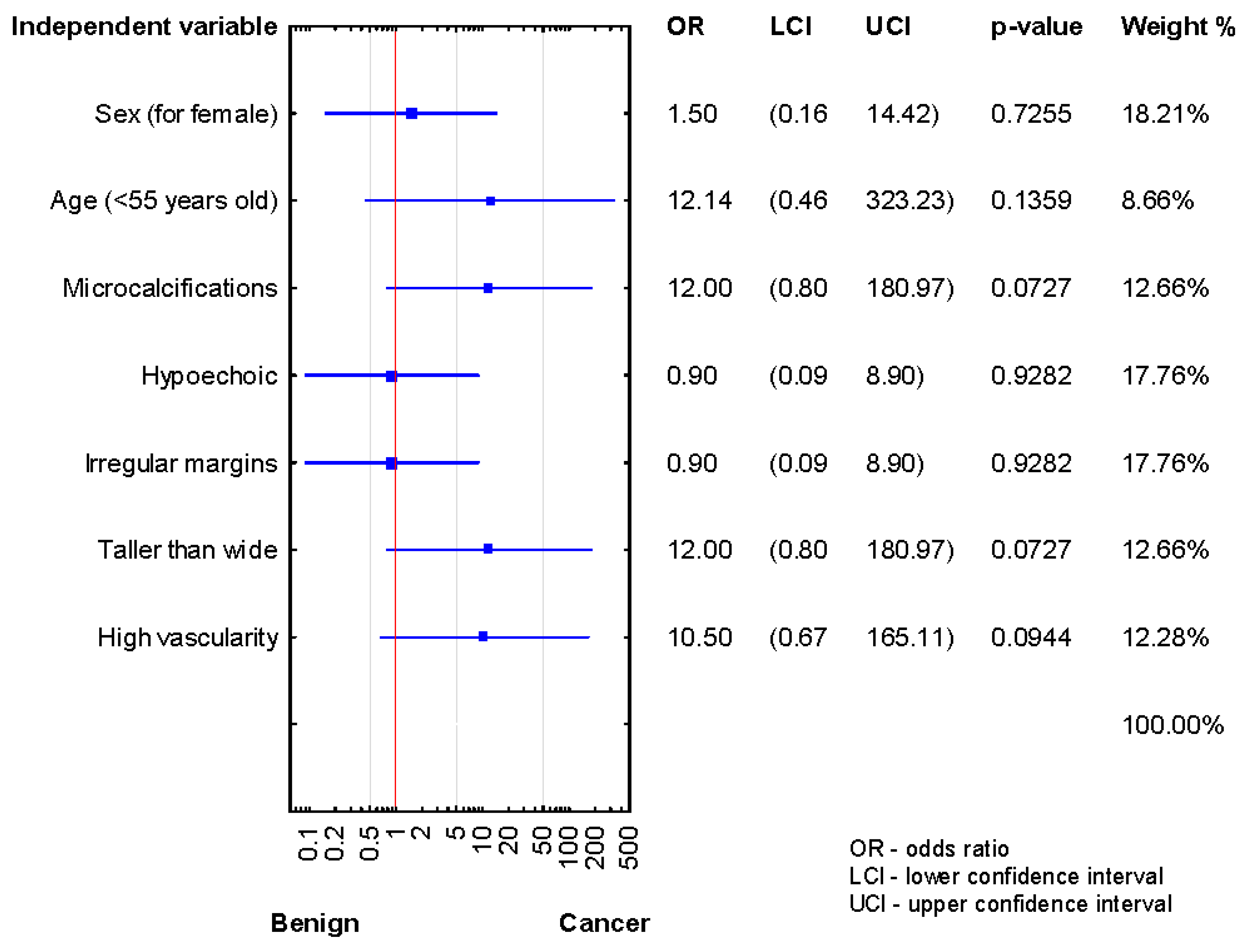
3.2. Association between Age, Sex, and US Features, and Occurrence of TN Malignancy
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| TN | thyroid nodule |
| AUS | atypia of undetermined significance |
| FLUS | follicular lesion of undetermined significance |
| US | ultrasound |
| ROM | risk of malignancy |
| UG-FNAB | ultrasound-guided fine-needle aspiration biopsy |
| ATA | American Thyroid Association |
| TBSRTC | The Bethesda System for Reporting Thyroid Cytopathology |
| NIFTP | noninvasive follicular neoplasms with papillary-like feature |
| SD | standard deviation |
| PTC | papillary thyroid cancer |
| FTC | follicular thyroid cancer |
| KTIDS | Korean Thyroid Imaging Reporting and Data System |
References
- Gao, L.Y.; Wang, Y.; Jiang, Y.X.; Yang, X.; Liu, R.; Xi, X.; Zhu, S.; Zhao, R.; Lai, X.; Zhang, X.; et al. Ultrasound is helpful to differentiate Bethesda class III thyroid nodules: A PRISMA-compliant systematic review and meta-analysis. Medicine 2017, 96, e6564. [Google Scholar] [CrossRef]
- Haugen, B.R.; Alexander, E.K.; Bible, K.C.; Doherty, G.M.; Mandel, S.J.; Nikiforov, Y.E.; Pacini, F.; Randolph, G.W.; Sawka, A.M.; Schlumberger, M.; et al. 2015 American Thyroid Association Management Guidelines for Adult Patients with Thyroid Nodules and Differentiated Thyroid Cancer: The American Thyroid Association Guidelines Task Force on Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 2016, 26, 1–133. [Google Scholar] [CrossRef] [Green Version]
- Cibas, E.S.; Ali, S.Z. The Bethesda System for Reporting Thyroid Cytopathology. Am. J. Clin. Pathol. 2009, 132, 658–665. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cibas, E.S.; Ali, S.Z. The 2017 Bethesda System for Reporting Thyroid Cytopathology. Thyroid 2017, 27, 1341–1346. [Google Scholar] [CrossRef] [PubMed]
- Krane, J.F.; Nayar, R.; Renshaw, A.A. Atypia of undetermined significance/follicular lesion of undetermined significance. In The Bethesda System for Reporting Thyroid Cytopathology: Definitions, Criteria, and Explanatory Notes, 2nd ed.; Ali, S.Z., Cibas, E.S., Eds.; Springer Nature: Dordrecht, The Netherlands, 2018; pp. 49–70. [Google Scholar]
- Crescenzi, A.; Palermo, A.; Trimboli, P. Cancer prevalence in the subcategories of the indeterminate class III (AUS/FLUS) of the Bethesda system for thyroid cytology: A meta-analysis. J. Endocrinol. Investig. 2021, 44, 1343–1351. [Google Scholar] [CrossRef] [PubMed]
- López Vázquez, Y.L.; Penín Álvarez, M.; San Miguel Fraile, P.; Pérez, M.B. Risk of malignancy in thyroid nodules with atipia of undetermined significance. Endocrinol. Nutr. 2015, 62, 507–510. [Google Scholar] [CrossRef] [PubMed]
- Ling, J.; Li, W.; Lalwani, N. Atypia of undetermined significance/follicular lesions of undetermined significance: What radiologists need to know. Neuroradiol. J. 2021, 34, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Marin, F.; Murillo, R.; Diego, C.; Jodar, E.; Acevedo, A. The impact of repeat fine-needle aspiration in thyroid nodules categorized as atypia of undetermined significance or follicular lesion of undetermined significance: A single center experience. Diagn. Cytopathol. 2021, 49, 412–417. [Google Scholar] [CrossRef]
- Elomami, A.; Elhag, S.A.; Alseddeeqi, E. Cytological Sub-Classification of Atypia of Undetermined Significance May Predict Malignancy Risk in Thyroid Nodules. Acta Cytol. 2021, 1, 1–8. [Google Scholar]
- Özkara, S.K.; Bayrak, B.Y.; Turan, G. High risk of malignancy in cases with atypia of undetermined significance on fine needle aspiration of thyroid nodules even after exclusion of NIFTP. Diagn. Cytopathol. 2020, 48, 986–997. [Google Scholar] [CrossRef]
- Evranos, B.; Polat, S.B.; Baser, H.; Ozdemir, D.; Kilicarslan, A.; Yalcin, A.; Ersoy, R.; Cakir, B. Bethesda classification is a valuable guide for fine needle aspiration reports and highly predictive especially for diagnosing aggressive variants of papillary thyroid carcinoma. Cytopathology 2016, 28, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Guleria, P.; Agarwal, S.; Iyer, V.K.; Jain, D.; Mathur, S.R.; Yadav, D. Subcategorisation of AUS/FLUS thyroid lesions as per the 2017 Bethesda System for Reporting Thyroid Cytopathology: A retrospective study from a tertiary care centre analysing risk of malignancy (ROM) of the different subcategories. J. Clin. Pathol. 2019, 72, 771–777. [Google Scholar] [CrossRef]
- Guleria, P.; Mani, K.; Agarwal, S. Indian experience of AUS/FLUS diagnosis: Is it different from rest of Asia and the West?—A systematic review and meta-analysis. Gland. Surg. 2020, 9, 1797–1812. [Google Scholar] [CrossRef]
- Kakudo, K.; Higuchi, M.; Hirokawa, M.; Satoh, S.; Jung, C.K.; Bychkov, A. Thyroid FNA cytology in Asian practice-Active surveillance for indeterminate thyroid nodules reduces overtreatment of thyroid carcinomas. Cytopatholgoy 2017, 28, 455–466. [Google Scholar] [CrossRef]
- Zhou, B.; Zhai, Y.F.; Zhang, D.Y.; Wang, D.Q.; Wei, L.; Qin, J.W. The role of combined BRAFV600E gene detection in the diagnosis of thyroid nodule determined as Bethesda III by fine-needle aspiration. Zhonghua Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2020, 55, 1057–1062. [Google Scholar] [PubMed]
- Park, V.; Kim, E.-K.; Kwak, J.Y.; Yoon, J.H.; Moon, H.J. Malignancy risk and characteristics of thyroid nodules with two consecutive results of atypia of undetermined significance or follicular lesion of undetermined significance on cytology. Eur. Radiol. 2015, 25, 2601–2607. [Google Scholar] [CrossRef]
- Sullivan, P.S.; Hirschowitz, S.L.; Fung, P.C.; Apple, S.K. The impact of atypia/follicular lesion of undetermined significance and repeat fine-needle aspiration: 5 years before and after implementation of the Bethesda System. Cancer Cytopathol. 2014, 122, 866–872. [Google Scholar] [CrossRef] [PubMed]
- Kuru, B.; Atmaca, A.; Kefeli, M. Malignancy rate associated with Bethesda category III (AUS/FLUS) with and without repeat fine needle aspiration biopsy. Diagn. Cytopathol. 2016, 44, 394–398. [Google Scholar] [CrossRef] [PubMed]
- Kaya, C.; Bozkurt, E.; Mut, D.T.; Mihmanli, M.; Uludağ, M. Which factors are associated with malignancy in thyroid nodules classified as Bethesda category 3 (Aus/FLUS) and how do they influence the patient’s management? Acta Endocrinol. 2019, 15, 491–496. [Google Scholar] [CrossRef]
- Jan, I.-S.; Lee, Y.-T.; Wang, C.-M.; Cheng, T.-Y.; Wang, C.-Y.; Chang, T.-C.; Shih, S.-R. The surgery and repeat aspiration outcomes of the atypia of undetermined significance/follicular lesion of undetermined significance category in The Bethesda System for Reporting Thyroid Cytopathology. Asian J. Surg. 2019, 42, 144–147. [Google Scholar] [CrossRef]
- Hong, S.-H.; Lee, H.; Cho, M.-S.; Lee, J.E.; Sung, Y.-A.; Hong, Y.S. Malignancy Risk and Related Factors of Atypia of Undetermined Significance/Follicular Lesion of Undetermined Significance in Thyroid Fine Needle Aspiration. Int. J. Endocrinol. 2018, 2018, 4521984. [Google Scholar] [CrossRef] [PubMed]
- Gweon, H.M.; Son, E.J.; Youk, J.H.; Kim, J.-A. Thyroid Nodules with Bethesda System III Cytology: Can Ultrasonography Guide the Next Step? Ann. Surg. Oncol. 2013, 20, 3083–3088. [Google Scholar] [CrossRef]
- Ryu, Y.J.; Jung, Y.S.; Yoon, H.C.; Hwang, M.J.; Shin, S.H.; Cho, J.S.; Lee, J.S.; Kim, H.K.; Kang, H.C.; Lim, H.S.; et al. Atypia of undetermined significance on thyroid fine needle aspiration: Surgical outcome and risk factors for malignancy. Ann. Surg. Treat. Res. 2014, 86, 109–114. [Google Scholar] [CrossRef] [Green Version]
- Kuru, B.; Atmaca, A.; Tarim, I.; Kefeli, M.; Topgul, K.; Yoruker, S.; Elmali, M.; Danaci, M. Risk factors associated with malignancy and with triage to surgery in thyroid nodules classified as Bethesda category III (AUS/FLUS). Eur. J. Surg. Oncol. (EJSO) 2016, 42, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Hong, M.J.; Na, D.G.; Baek, J.H.; Sung, J.Y.; Kim, J.-H. Cytology-Ultrasonography Risk-Stratification Scoring System Based on Fine-Needle Aspiration Cytology and the Korean-Thyroid Imaging Reporting and Data System. Thyroid 2017, 27, 953–959. [Google Scholar] [CrossRef] [PubMed]
- Schneider, D.F.; Stafford, L.M.C.; Brys, N.; Greenberg, C.C.; Balentine, C.J.; Elfenbein, D.M.; Pitt, S.C. Gauging The Extent Of Thyroidectomy For Indeterminate Thyroid Nodules: An Oncologic Perspective. Endocr. Pract. 2017, 23, 442–450. [Google Scholar] [CrossRef] [Green Version]
- Saftencu, M.; Braicu, C.; Cojocneanu, R.; Buse, M.; Irimie, A.; Piciu, D.; Berindan-Neagoe, I. Gene Expression Patterns Unveil New Insights in Papillary Thyroid Cancer. Medicine 2019, 55, 500. [Google Scholar] [CrossRef] [Green Version]
- Karapanou, O. The role of molecular genetics in the pre-surgical management of thyroid nodules. Minerva Endocrinol. 2020, 46, 21–34. [Google Scholar]
- Al-Salam, S.; Sharma, C.; Abu Sa’a, M.T.; Afandi, B.; Aldahmani, K.M.; Al Dhaheri, A.; Yahya, H.; Al Naqbi, D.; Al Zuraiqi, E.; Mohamed, B.K.; et al. Ultrasound-guided fine needle aspiration cytology and ultrasound examination of thyroid nodules in the UAE: A comparison. PLoS ONE 2021, 16, e0247807. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | n (%) or Mean ± SD | |
|---|---|---|
| Sex | Female | 284 (83.0) |
| Male | 58 (17.0) | |
| Age (years old) | 51.26 ± 15.41 | |
| Age | <55 years | 191 (55.8) |
| >55 years | 151 (44.2) | |
| Histopathological diagnosis | Goiter | 197 (57.6) |
| Adenoma | 54 (15.8) | |
| Thyroiditis | 44 (12.9) | |
| PTC | 46 (13.4) | |
| FTC | 1 (0.3) | |
| Nodule size (cm) (median, IQR) | 2.00 (1.5–2.6) | |
| ≤1.0 cm | 39 (11.4) | |
| >1.0 ≤ 2.0 cm | 139 (40.6) | |
| >2.0 ≤ 4.0 cm | 150 (43.9) | |
| >4.0 cm | 14 (4.1) | |
| Ultrasound features | n (%) | |
| Microcalcifications | Yes | 72 (21.1) |
| No | 270 (78.9) | |
| Echogenicity | Hypoechoic | 125 (36.5) |
| Hyperechoic | 217 (63.5) | |
| Irregular margin | Yes | 132 (38.6) |
| No | 210 (61.4) | |
| Taller-than-wide | Yes | 111 (32.5) |
| No | 231 (67.5) | |
| High vascularity | Yes | 118 (34.5) |
| No | 224 (65.5) | |
| Independent Variables | Benign (n = 142) | Cancer (n = 19) | p-Value (Fisher Exact Test) | OR (+95% CI) | p-Value (Wald Test) | |
|---|---|---|---|---|---|---|
| N (%) | N (%) | |||||
| Sex: | Female | 117 (82.4) | 13 (68.4) | 0.210 | 0.46 (0.15–1.34) | 0.154 |
| Male | 25 (17.6) | 6 (31.6) | ||||
| Age: | <55 years | 76 (53.5) | 15 (79.0) | 0.047 * | 3.26 (1.02–10.38) | 0.044 * |
| >55 years | 66 (46.5) | 4 (21.0) | ||||
| Nodule size: | <2 cm | 67 (47.2) | 19 (100.0) | <0.0001 * | - | - |
| >2 cm | 75 (52.8) | 0 (0.0) | ||||
| Microcalcifications: | Yes | 24 (16.9) | 15 (79.0) | <0.0001 * | 18.43 (5.57–60.98) | <0.0001 * |
| No | 118 (83.1) | 4 (21.0) | ||||
| Echogenicity: | Hypoechoic | 45 (31.7) | 17 (89.5) | <0.0001 * | 18.32 (4.01–83.67) | 0.0002 * |
| Hyperechoic | 97 (68.3) | 2 (10.5) | ||||
| Irregular margins: | Yes | 43 (30.3) | 17 (89.5) | <0.0001 * | 19.56 (4.28–89.46) | 0.0001 * |
| No | 99 (69.7) | 2 (10.5) | ||||
| Taller-than-wide: | Yes | 34 (23.9) | 18 (94.7) | <0.0001 * | 57.17 (7.24–451.32) | 0.0001 * |
| No | 108 (76.1) | 1 (5.3) | ||||
| High vascularity: | Yes | 66 (46.5) | 13 (68.4) | 0.089 | 2.49 (0.89–6.98) | 0.079 |
| No | 76 (53.5) | 6 (31.6) | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kaliszewski, K.; Diakowska, D.; Rzeszutko, M.; Nowak, Ł.; Tokarczyk, U.; Rudnicki, J. Atypia and Follicular Lesions of Undetermined Significance in Subsequent Biopsy Result: What Clinicians Need to Know. J. Clin. Med. 2021, 10, 3082. https://doi.org/10.3390/jcm10143082
Kaliszewski K, Diakowska D, Rzeszutko M, Nowak Ł, Tokarczyk U, Rudnicki J. Atypia and Follicular Lesions of Undetermined Significance in Subsequent Biopsy Result: What Clinicians Need to Know. Journal of Clinical Medicine. 2021; 10(14):3082. https://doi.org/10.3390/jcm10143082
Chicago/Turabian StyleKaliszewski, Krzysztof, Dorota Diakowska, Marta Rzeszutko, Łukasz Nowak, Urszula Tokarczyk, and Jerzy Rudnicki. 2021. "Atypia and Follicular Lesions of Undetermined Significance in Subsequent Biopsy Result: What Clinicians Need to Know" Journal of Clinical Medicine 10, no. 14: 3082. https://doi.org/10.3390/jcm10143082
APA StyleKaliszewski, K., Diakowska, D., Rzeszutko, M., Nowak, Ł., Tokarczyk, U., & Rudnicki, J. (2021). Atypia and Follicular Lesions of Undetermined Significance in Subsequent Biopsy Result: What Clinicians Need to Know. Journal of Clinical Medicine, 10(14), 3082. https://doi.org/10.3390/jcm10143082