
Pilot Study of Acupuncture’s Antispasmodic Effect on Upper Gastrointestinal Tract during Endoscopic Submucosal Dissection for Early Gastric Cancer: Controlled Clinical Trial

 , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Patients
- Those who were age >40 years and diagnosed as early-stage gastric cancer, irrespective of H. pylori infection. Early-stage gastric cancer was pathologically diagnosed using endoscopy prior to ESD [2]. The criteria of early-stage gastric cancer were: (1) An intramucosal intestinal-type cancer without ulcerative lesion, regardless of tumor size; (2) intramucosal intestinal-type cancer with ulcerative lesion, ≤3 cm in size; and (3) intramucosal diffuse type cancer ≤2 cm in size without ulcerative lesion.
- Those who were in stable condition without any symptoms of infectious diseases such as fever or respiratory symptoms, showed no rapid deterioration of cancer related symptoms and with no changes in the medication at least a week prior to the date of the ESD.
- Patients who had sufficient cognitive ability to understand the study protocol.
2.3. Patients Registration Assignment of the Subjects
2.4. ESD Procedure
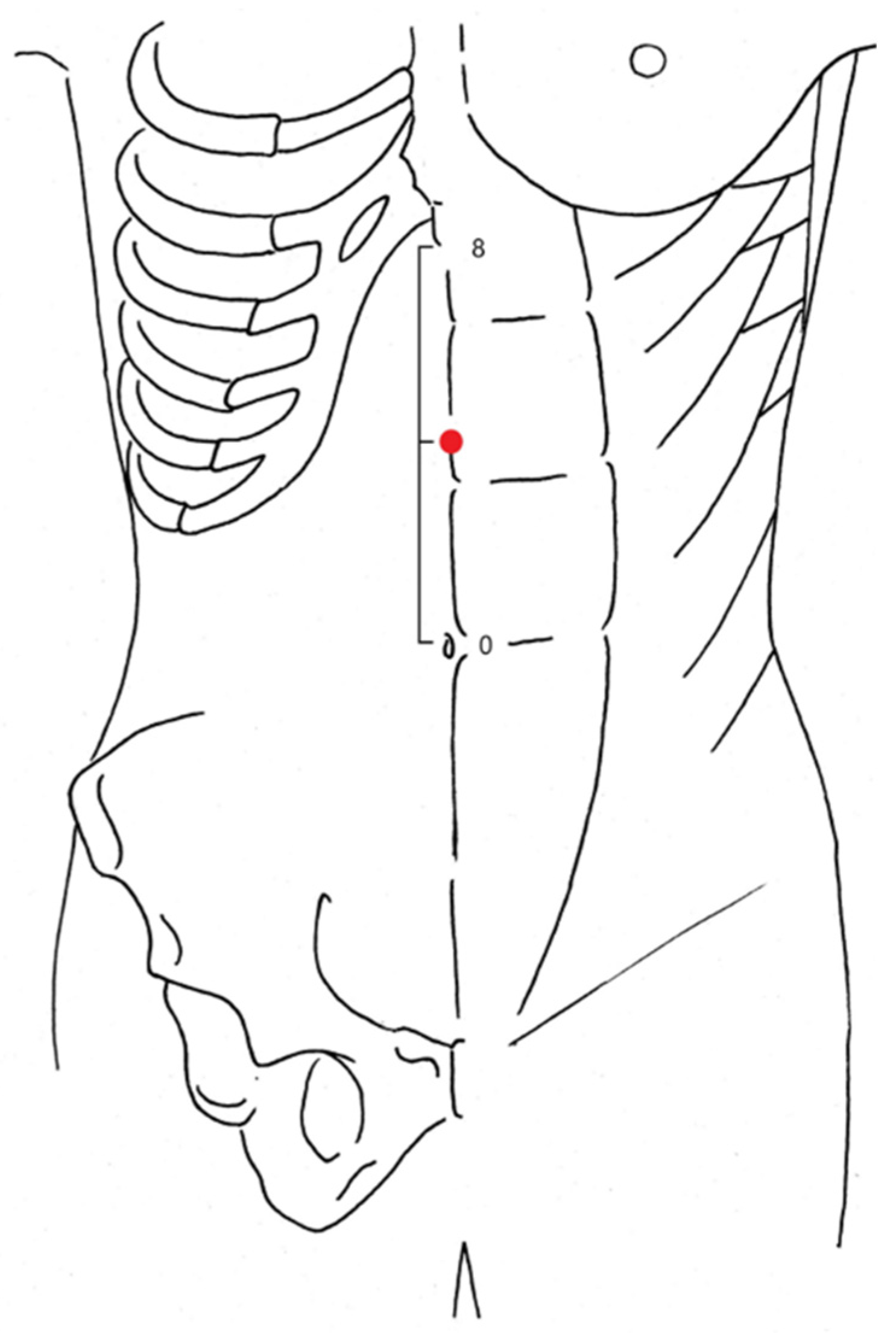
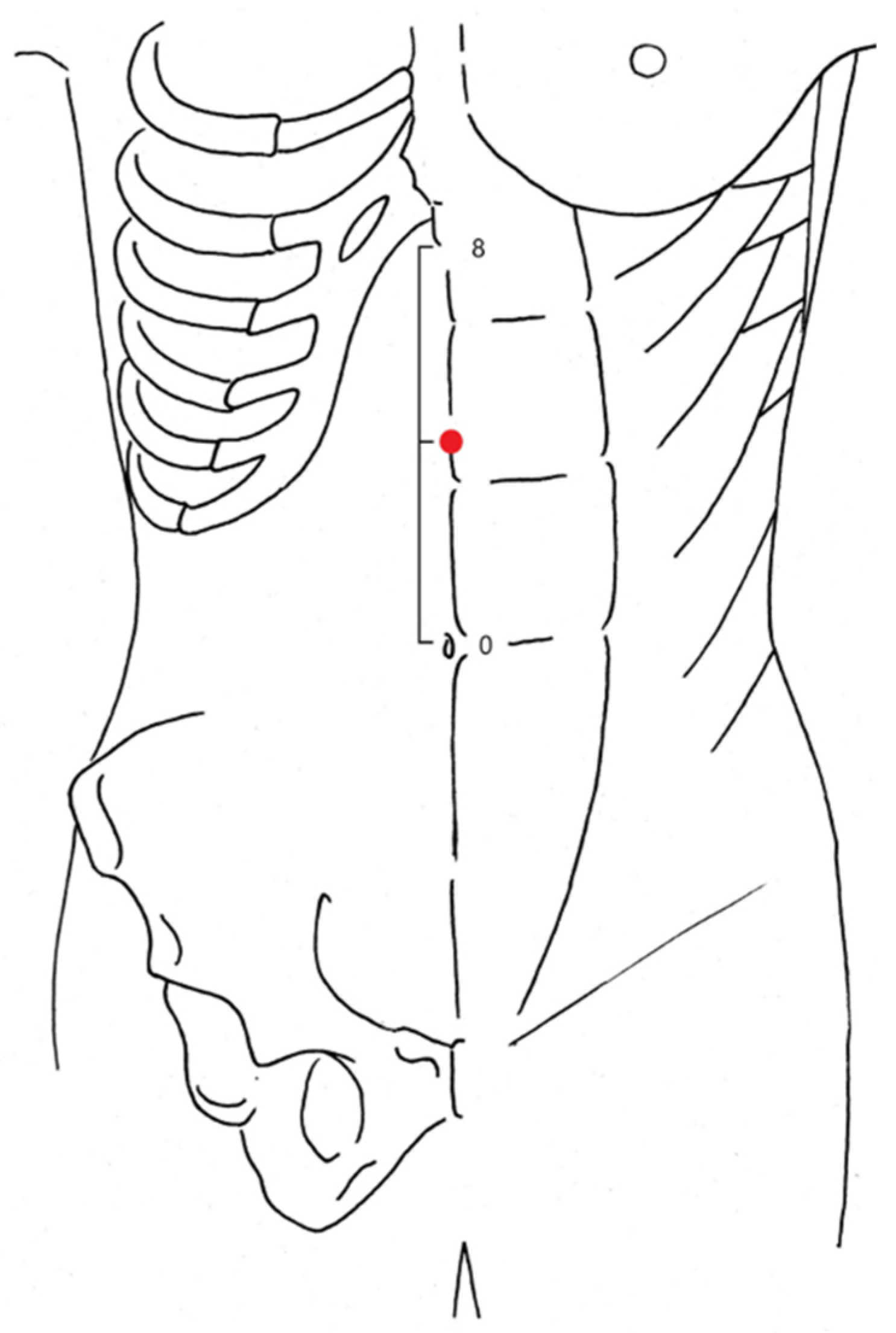
2.5. Interventiona and Blinding
2.6. Measures
2.6.1. Primary Outcome Measure
2.6.2. Secondary Outcome Measures
2.6.3. Other Outcome Measures
- Bleeding (intraoperative and postoperative), perforation (intraoperative and delay) due to ESD. Here, bleeding during the procedure is defined as when bleeding continued even after coagulation with normal hemostats, and when clipping or alcohol local injection had to be performed. Bleeding after treatment is defined as when hemostasis at the excised site had to be performed by upper gastrointestinal endoscopy because hematemesis, melena, or shock was observed.Perforation was defined as when a perforation was clearly confirmed during the operation and endoscopic clip closure was performed. Delayed perforation was defined as when peritonitis was suspected, and free air was found by abdominal X-ray or CT scan.
- Additionally, blood pressure fluctuation was monitored during procedure. Blood pressure fluctuations were defined as greater than 30% increase or decrease from the baseline value (base line value is the blood pressure during a 10 min rest before the procedure) and such increase or decrease last for 3 min or more within 5 min after intervention with antispasmodics or acupuncture.
- Presence or absence of aspiration pneumonia after treatment was evaluated comprehensively by not only respiratory symptoms (cough, sputum, dyspnea, chest pain), and fever, but also findings by images of chest X-ray or chest CT, and sputum examination and blood culture.
- In accordance with the ASA Physical Status Classification System (ASA-PS) [15], the operation time, anesthesia time, total amount of sedative medication, and resection area were also evaluated. The resection area was calculated by ImageJ software, version 1.6.0 (NIH, Bethesda, MD, USA).
2.7. Sample Size and Statistical Analysis
3. Results
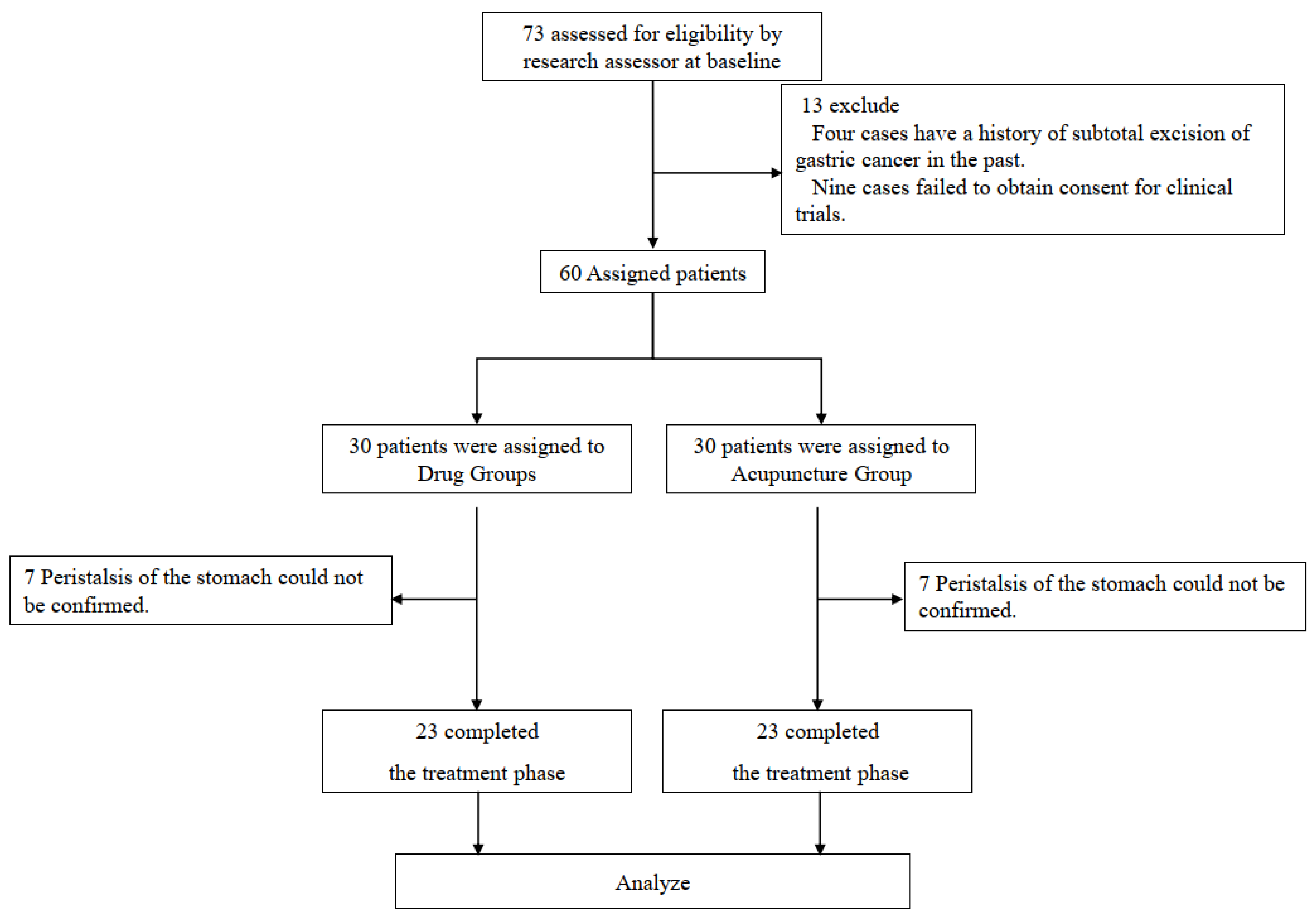
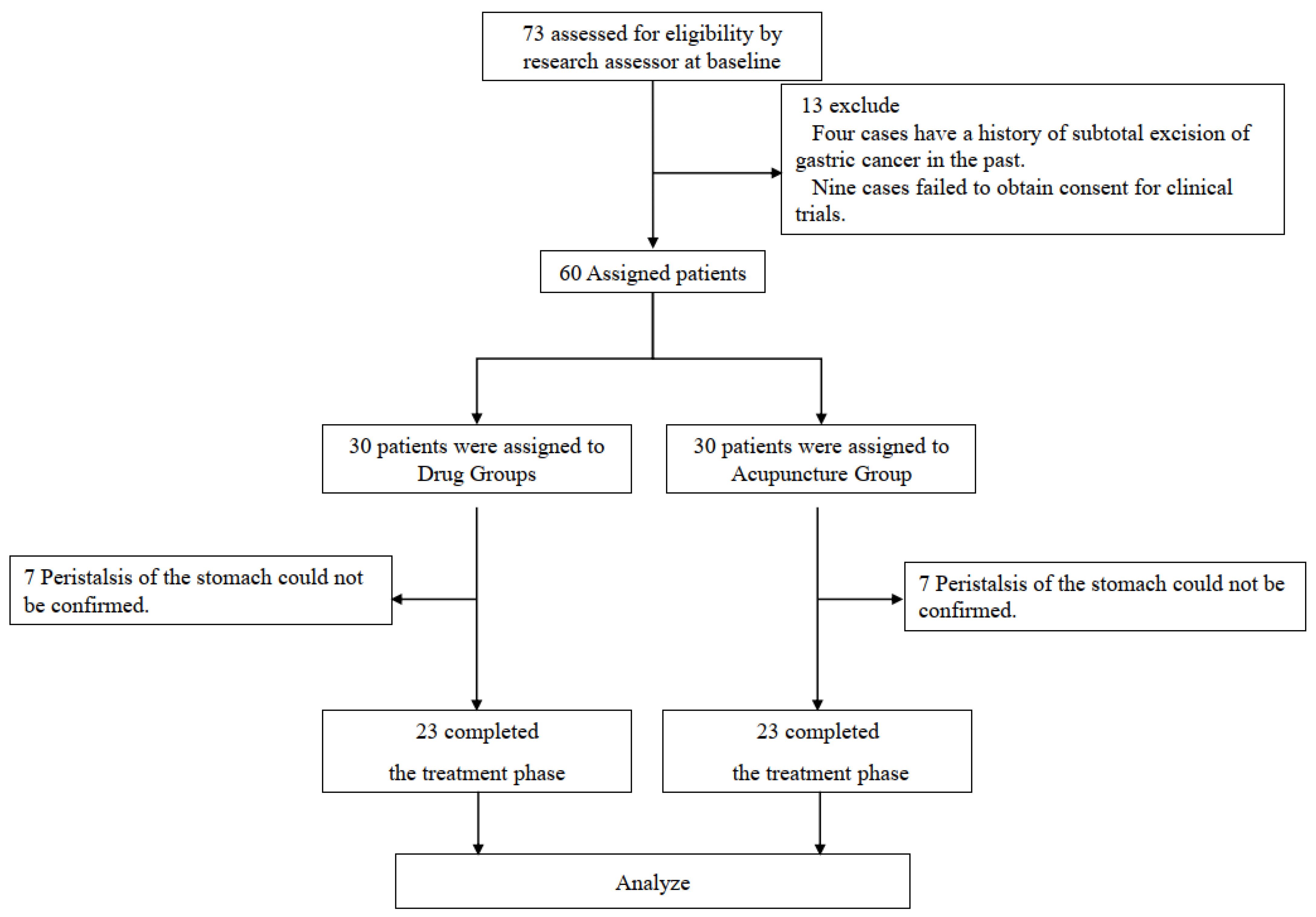
3.1. Study Population
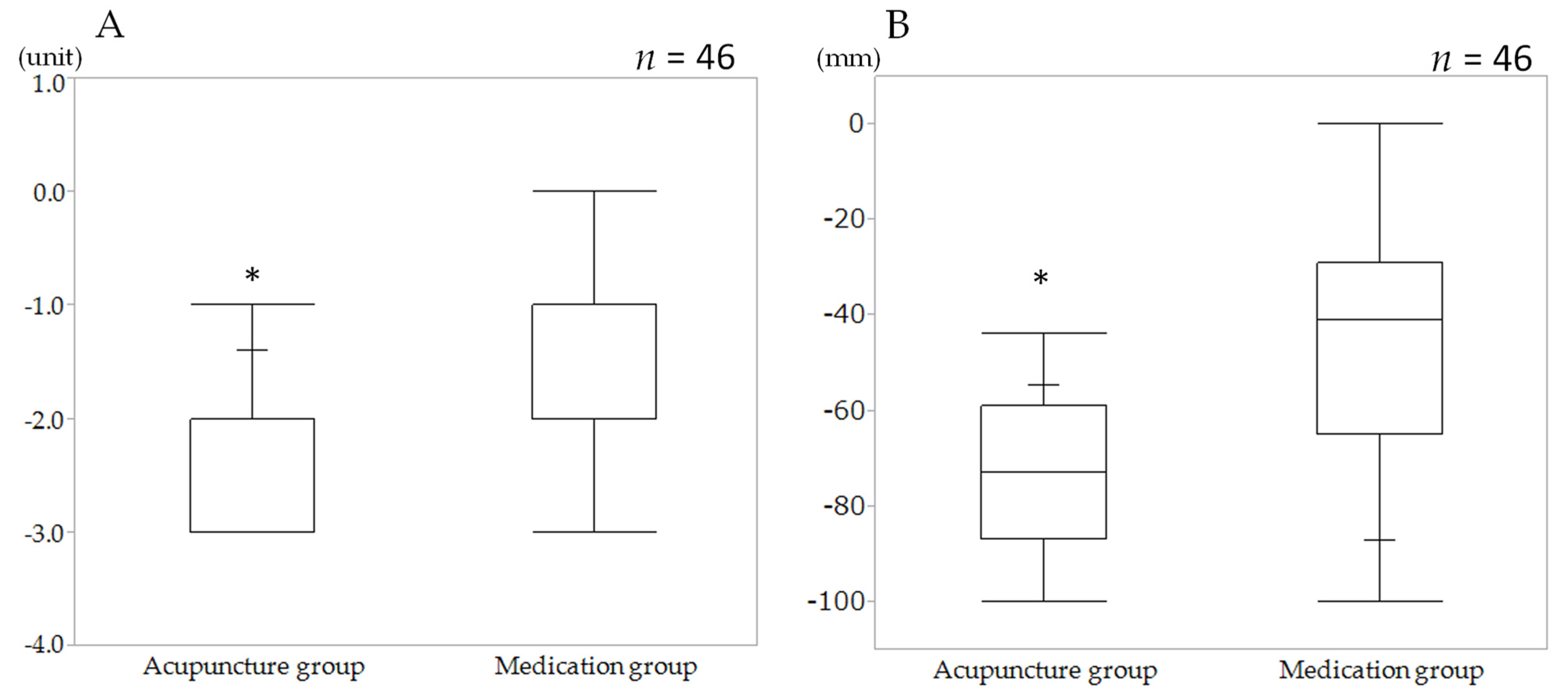
3.2. Primary Outcome (MNC)
3.3. Secondary Outcome (VAS)
3.4. Procedure Time and Area of Resected Specimen
3.5. Procedure Complications
4. Discussion
4.1. Antispasmodic Effect of Acupuncture Stimulation
4.2. Study Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sugimoto, M.; Jang, J.S.; Yoshizawa, Y.; Osawa, S.; Sugimoto, K.; Sato, Y.; Furuta, T. Proton Pump Inhibitor Therapy before and after Endoscopic Submucosal Dissection: A Review. Diagn. Ther. Endosc. 2012, 2012, 791873. [Google Scholar] [CrossRef] [Green Version]
- Ono, H.; Yao, K.; Fujishiro, M.; Oda, I.; Nimura, S.; Yahagi, N.; Iishi, H.; Oka, M.; Ajioka, Y.; Ichinose, M.; et al. Guidelines for endoscopic submucosal dissection and endoscopic mucosal resection for early gastric cancer. Dig. Endosc. 2016, 28, 3–15. [Google Scholar] [CrossRef] [Green Version]
- Fujishiro, M.; Yahagi, N.; Kakushima, N.; Kodashima, S.; Muraki, Y.; Ono, S.; Kobayashi, K.; Hashimoto, T.; Yamamichi, N.; Tateishi, A.; et al. Successful nonsurgical management of perforation complicating endoscopic submucosal dissection of gastrointestinal epithelial neoplasms. Endoscopy 2006, 38, 1001–1006. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Ono, H.; Hasuike, N.; Takizawa, K. Endoscopic submucosal dissection of early gastric cancer. Digestion 2008, 77, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Lim, J.H.; Kim, S.G.; Choi, J.; Im, P.J.; Kim, J.S.; Jung, H.C. Risk factors of delayed ulcer healing after gastric endoscopic submucosal dissection. Surg. Endosc. 2015, 29, 3666–3673. [Google Scholar] [CrossRef] [PubMed]
- Furuta, T.; Kato, M.; Itoh, T.; Inaba, T.; Komura, N.; Katanuma, A.; Shimizu, S.; Hiyama, T.; Matsuda, K.; Yasuda, I.; et al. Sixth National Survey Report on Gastrointestinal Endoscopic Incidents 5 Years from 2008 to 2012. Gastroenterol. Endosc. 2016, 58, 1466–1491. (In Japanese) [Google Scholar]
- Schneider, A.; Streitberger, K.; Joos, S. Acupuncture treatment in gastrointestinal diseases: A systematic review. World J. Gastroenterol. 2007, 13, 3417–3424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Imai, K. Effects of acupuncture on electrogastrogram, instantaneous heart rate and sympathetic skin response with pharmacological analysis to elucidate the neural mechanisms in humans. Meiji Acupunct. Med. 1996, 19, 45–55. (In Japanese) [Google Scholar]
- Sato, A.; Sato, Y.; Suzuki, A.; Uchida, S. Neural mechanisms of the reflex inhibition and excitation of gastric motility elicited by acupuncture-like stimulation in anesthetized rats. Neurosci. Res. 1993, 18, 53–62. [Google Scholar] [CrossRef]
- Hugh MacPherson, H.; Altman, G.D.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.; Moher, D.; STRICTA Revision Group. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT Statement. PLoS Med. 2010, 8, e1000261. [Google Scholar] [CrossRef] [Green Version]
- Obara, K.; Haruma, K.; Irisawa, A.; Kaise, M.; Gotoda, T.; Sugiyama, M.; Tanabe, S.; Horiuchi, A.; Fujita, N.; Ozaki, M.; et al. Guidelines for sedation in gastroenterological endoscopy. Dig. Endosc. 2015, 27, 435–449. [Google Scholar] [CrossRef]
- Niwa, H.; Nakamura, T.; Fujino, M. Endoscopic observation on gastric peristalsis and pyloric movement. Gastroenterol. Endosc. 1975, 17, 236–242. (In Japanese) [Google Scholar]
- World Health Organization (WHO) Western Pacific Region. WHO Standard Acupuncture Point Locations in the Western Pacific Region; WHO Press Western Pacific: Manila, Philippines, 2008; ISBN 978-9290613831. [Google Scholar]
- Fukuzawa, M.; Kawai, T.; Sugimoto, H. Effects on the gastric peristaltic movement of glucagon using a nasal endoscope. Prog. Med. 2012, 32, 573–576. (In Japanese) [Google Scholar]
- Abouleish, A.E.; Leib, M.L.; Cohen, N.H. ASA provides examples to each ASA physical status class. ASA Monit. 2015, 79, 38–39. [Google Scholar]
- Matsumoto, J.; Ishizaki, N.; Ono, K.; Yano, T.; Yamamura, Y. The effect of acupuncture for inhibition of gastric peristalsis during gastroscopy. J. JSAM 2004, 54, 779–784. (In Japanese) [Google Scholar]
- Stunkard, A.J.; Van, I.T.B.; Reis, B.B. The mechanism of satiety: Effect of glucagon on gastric hunger contractions in man. Proc. Soc. Exp. Biol. Med. 1955, 89, 258–261. [Google Scholar] [CrossRef] [PubMed]
- Chernish, S.M.; Miller, R.E.; Rosenak, B.D.; Scholzet, N.E. Hypotonic duodenography with the use of glucagon. Gastroenterology 1972, 63, 392–398. [Google Scholar] [CrossRef]
- Itoh, Z.; Takeuchi, S.; Aizawa, I.; Mori, K.; Taminato, T.; Seino, Y.; Imura, H.; Yanaihara, N. Changes in plasma motilin concentration and gastrointestinal contractile activity in conscious dogs. Am. J. Dig. Dis. 1978, 23, 929–935. [Google Scholar] [CrossRef]
- Takahashi, T. Mechanism of Interdigestive Migrating Motor Complex. J. Neurogastroenterol. Motil. 2012, 18, 246–257. [Google Scholar] [CrossRef]
- Takahashi, T. Mechanism of acupuncture on neuromodulation in the gut-a review. Neuromodulation 2011, 14, 8–12. [Google Scholar] [CrossRef]
- Su, Y.S.; Yang, Z.K.; Xin, J.J.; He, W.; Shi, H.; Wang, X.Y.; Hu, L.; Jing, X.H.; Zhu, B. Somatosensory Nerve Fibers Mediated Generation of De-qi in Manual Acupuncture and Local Moxibustion-Like Stimuli-Modulated Gastric Motility in Rats. Evid. Based Complement. Altern. Med. 2014, 2014, 673239. [Google Scholar] [CrossRef] [PubMed]
- Tada, H.; Fujita, M.; Harris, M.; Tatewaki, M.; Nakagawa, K.; Yamamura, T.; Pappas, T.N.; Takahashi, T. Neural mechanism of acupuncture-induced gastric relaxations in rats. Dig. Dis. Sci. 2003, 48, 59–68. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
| Evaluation | Class | State of Peristalsis |
|---|---|---|
| Very easy to operation | I | No peristaltic movement found and no problem with endoscopic operation. Equivalent to degree I (no peristaltic movement). |
| Easy to operation | II | Slight peristaltic movement found but no problem with endoscopic operation. Equivalent to degree II (slight peristaltic movement). |
| operation is slightly difficult | III | Some, although light, peristaltic movement found and some problem with endoscopic operation. Equivalent to degree III (mild peristaltic movement). |
| operation is difficult | IV | Peristaltic movement found and hard to perform endoscopic operation. Equivalent to degree IV (strong peristaltic movement). |
| MG (n = 30) | AG (n = 30) | p Value | |
|---|---|---|---|
| Gender (M/F) | 20/10 | 23/7 | 0.39 |
| Age yr (IQR) | 77.50 (72.3 to 82.0) | 76.00 (67.0 to 81.5) | 0.45 |
| Height (m) (IQR) | 154.40 (150.2 to 170.0) | 158.80 (148.6 to 166.2) | 0.31 |
| Body Weight (kg) (IQR) | 58.70 (48.9 to 66.5) | 59.95 (52.3 to 65.5) | 0.61 |
| Body Mass Index (Kg/m2) (IQR) | 23.90 (21.5 to 25.9) | 23.70 (21.5 to 25.7) | 0.63 |
| Brinkman index (IQR) | 161.00 (0.0 to 480.3) | 0.00 (0.0 to 560.0) | 0.67 |
| ASA-PS n (%) | |||
| Class I | 18 (60.0) | 23 (76.7) | 0.46 |
| Class II | 7 (23.3) | 4 (13.3) | |
| Class III | 4 (13.3) | 3 (10.0) | |
| Class IV | 1 (3.3) | 0 (0) | |
| Class V | 0 (0) | 0 (0) | |
| Complications n (%) | |||
| Hypertension | 17.00 (56.7) | 18.00 (60.0) | 0.79 |
| Hyperlipidemia | 3.00 (10.0) | 6.00 (20.0) | 0.28 |
| Diabetes mellitus | 5.00 (16.7) | 9.00 (30.0) | 0.22 |
| Location n (%) | |||
| Cardia | 1 (3.3) | 1.00 (3.3) | 0.99 |
| Body | 7 (23.3) | 6 (20.0) | |
| Incisura | 6 (20.0) | 6 (20.0) | |
| Anterum | 16 (53.3) | 17 (56.7) | |
| Macroscopic type, n (%) | |||
| Type 0-I | 3 (10.0) | 2 (6.7) | 0.92 |
| Type 0-IIa | 8 (26.7) | 6 (20.0) | |
| Type 0-IIb | 1 (3.3) | 1 (3.3) | |
| Type 0-IIc | 9 (30.0) | 14 (46.7) | |
| Type 0-IIa + IIc | 5 (16.7) | 4 (13.3) | |
| Type 0-IIc + IIa | 2 (6.7) | 2 (6.7) | |
| Type 0-IIa + IIb | 2 (6.67) | 1 (3.3) |
| Baseline | After | Change from Baseline to Post Treatment Measurements | p Value | |
|---|---|---|---|---|
| MNC (unit) | ||||
| AG (n 23) (IQR) | 4.00 (3.0 to 4.0) | 1.00 (1.0 to 1.0) | −2.00 (−3.0 to −2.0) | <0.0001 |
| MG (n 23) (IQR) | 4.00 (3.0 to 4.0) | 2.00 (2.0 to 3.0) | −1.00 (−2.0 to −1.0) | |
| VAS (mm) | ||||
| AG (n 23) (IQR) | 96.00 (77.5 to 100) | 15.00 (7.0 to 23.0) | −73.00 (−87.0 to −59.0) | <0.0001 |
| MG (n 23) (IQR) | 80.00 (72.5 to 89.5) | 29.00 (16.5 to 52.0) | −41.00 (−65.0 to −29.0) |
| MG (n = 23) | AG (n = 23) | p Value | |
|---|---|---|---|
| Procedure time (minute) (IQR) | 53.00 (44.0 to 76.0) | 93.00 (70.5 to 138.0) | 0.005 |
| Anesthesia time (minute) (IQR) | 51.00 (40.0 to 72.0) | 85.00 (65.5 to 132.0) | 0.003 |
| Resected specimen area (mm2) (IQR) | 480.00 (358.5 to 621.0) | 598.00 (428.0 to 820.5) | 0.09 |
| Resection en bloc (%) | 23 (100) | 23 (100) | N.A |
| Sedative medication | |||
| Midazolam (mg) (IQR) | 16.00 (14.0 to 20.0) | 18.00 (14.0 to 20.0) | 0.25 |
| Propofol (mg) (IQR) | 0.00 (0.0 to 6.5) | 0.00 (0.0 to 9.0) | 0.61 |
| Pentazocine (mg) (IQR) | 1.00 (0.5 to 1.0) | 1.00 (0.5 to 1.0) | 0.89 |
| Procedure Complications n (%) | |||
| Bleeding | |||
| Inoperative | 2.00 (8.70) | 1.00 (4.35) | 0.55 |
| Postoperative | 0 (0) | 0 (0) | N.A |
| Perforation | |||
| Intraoperative | 1.00 (4.35) | 0 (0) | 0.31 |
| delay | 0 (0) | 0 (0) | 1.00 |
| Blood pressure fluctuation | 14.00 (60.86) | 2.00 (8.70) | 0.001 |
| Emergency surgery | 0 (0) | 0 (0) | N.A |
| Aspiration pneumonia | 0 (0) | 0 (0) | N.A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, M.; Ishizaki, N.; Kayo, T.; Furuta, T.; Igarashi, R.; Maki, T.; Hoshi, K.; Yamabe, A.; Fujisawa, M.; Funakubo, A.; et al. Pilot Study of Acupuncture’s Antispasmodic Effect on Upper Gastrointestinal Tract during Endoscopic Submucosal Dissection for Early Gastric Cancer: Controlled Clinical Trial. J. Clin. Med. 2021, 10, 3050. https://doi.org/10.3390/jcm10143050
Suzuki M, Ishizaki N, Kayo T, Furuta T, Igarashi R, Maki T, Hoshi K, Yamabe A, Fujisawa M, Funakubo A, et al. Pilot Study of Acupuncture’s Antispasmodic Effect on Upper Gastrointestinal Tract during Endoscopic Submucosal Dissection for Early Gastric Cancer: Controlled Clinical Trial. Journal of Clinical Medicine. 2021; 10(14):3050. https://doi.org/10.3390/jcm10143050
Chicago/Turabian StyleSuzuki, Masao, Naoto Ishizaki, Takumi Kayo, Taiga Furuta, Ryo Igarashi, Takumi Maki, Koki Hoshi, Akane Yamabe, Mariko Fujisawa, Akira Funakubo, and et al. 2021. "Pilot Study of Acupuncture’s Antispasmodic Effect on Upper Gastrointestinal Tract during Endoscopic Submucosal Dissection for Early Gastric Cancer: Controlled Clinical Trial" Journal of Clinical Medicine 10, no. 14: 3050. https://doi.org/10.3390/jcm10143050
APA StyleSuzuki, M., Ishizaki, N., Kayo, T., Furuta, T., Igarashi, R., Maki, T., Hoshi, K., Yamabe, A., Fujisawa, M., Funakubo, A., Mitsuma, T., Irisawa, A., & Shibukawa, G. (2021). Pilot Study of Acupuncture’s Antispasmodic Effect on Upper Gastrointestinal Tract during Endoscopic Submucosal Dissection for Early Gastric Cancer: Controlled Clinical Trial. Journal of Clinical Medicine, 10(14), 3050. https://doi.org/10.3390/jcm10143050