
Coronal and Transverse Malalignment in Pediatric Patellofemoral Instability

Abstract
:1. Introduction
1.1. Patient History
1.2. Physical Exam
2. Imaging
3. Treatment
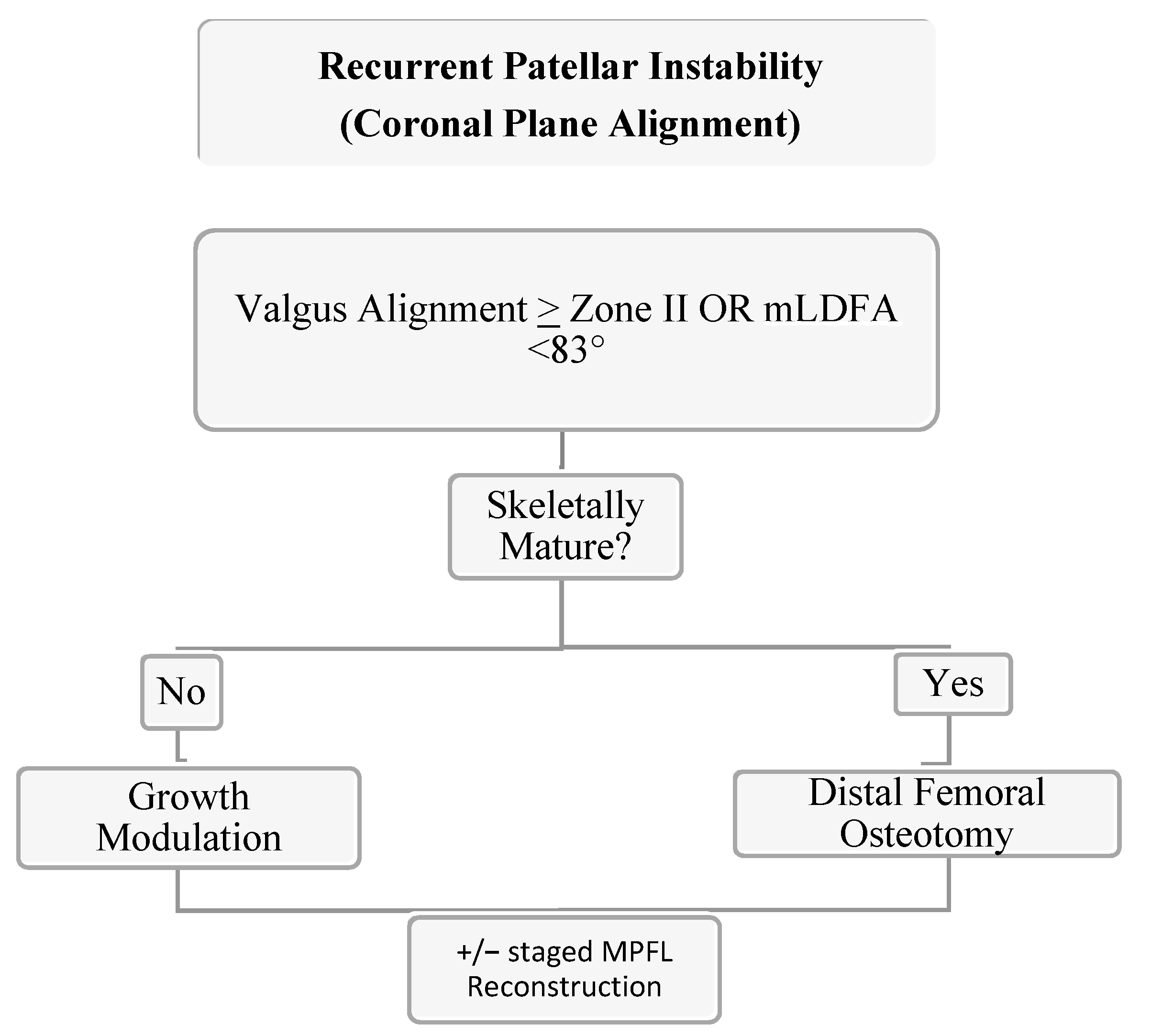
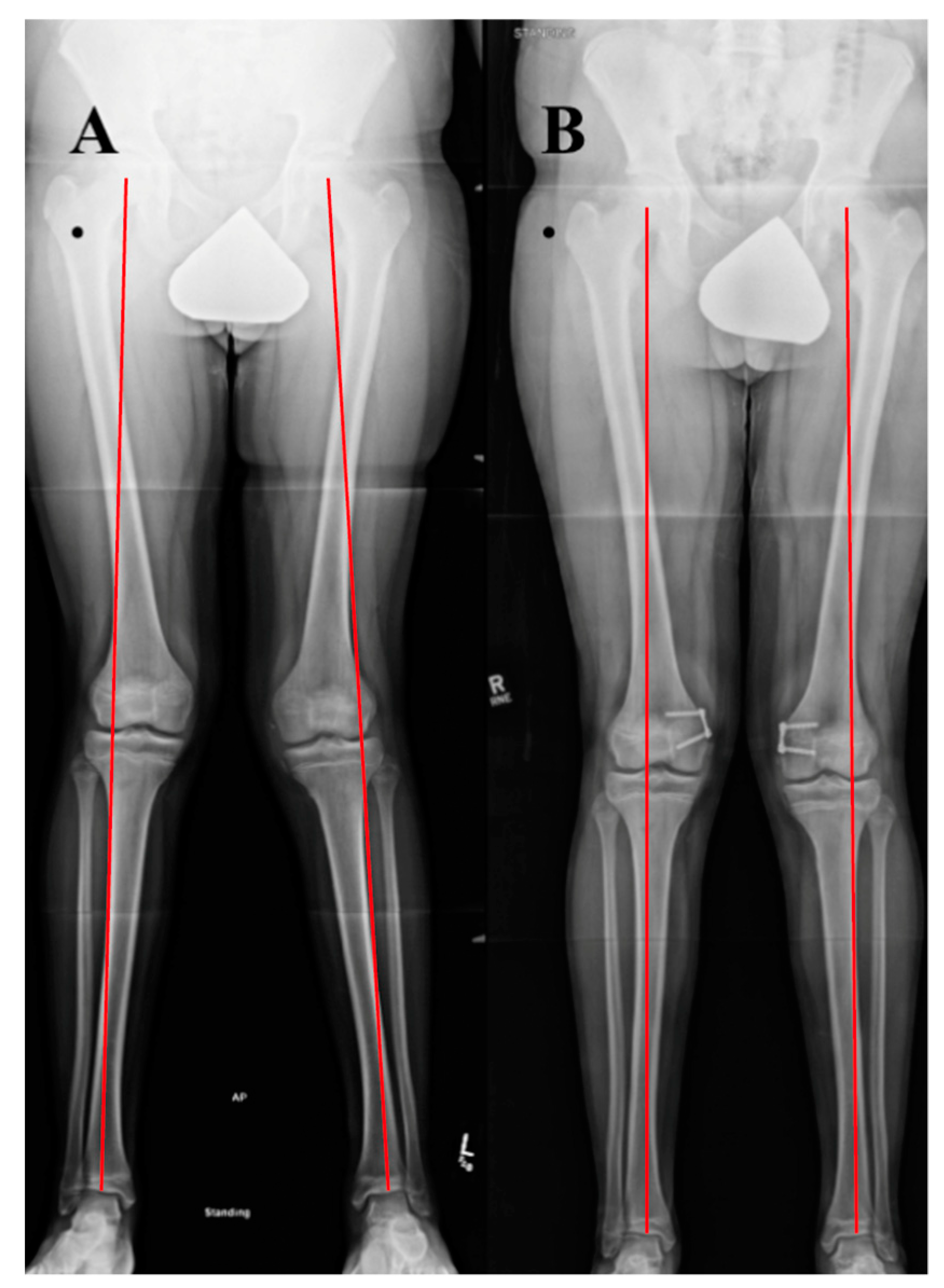
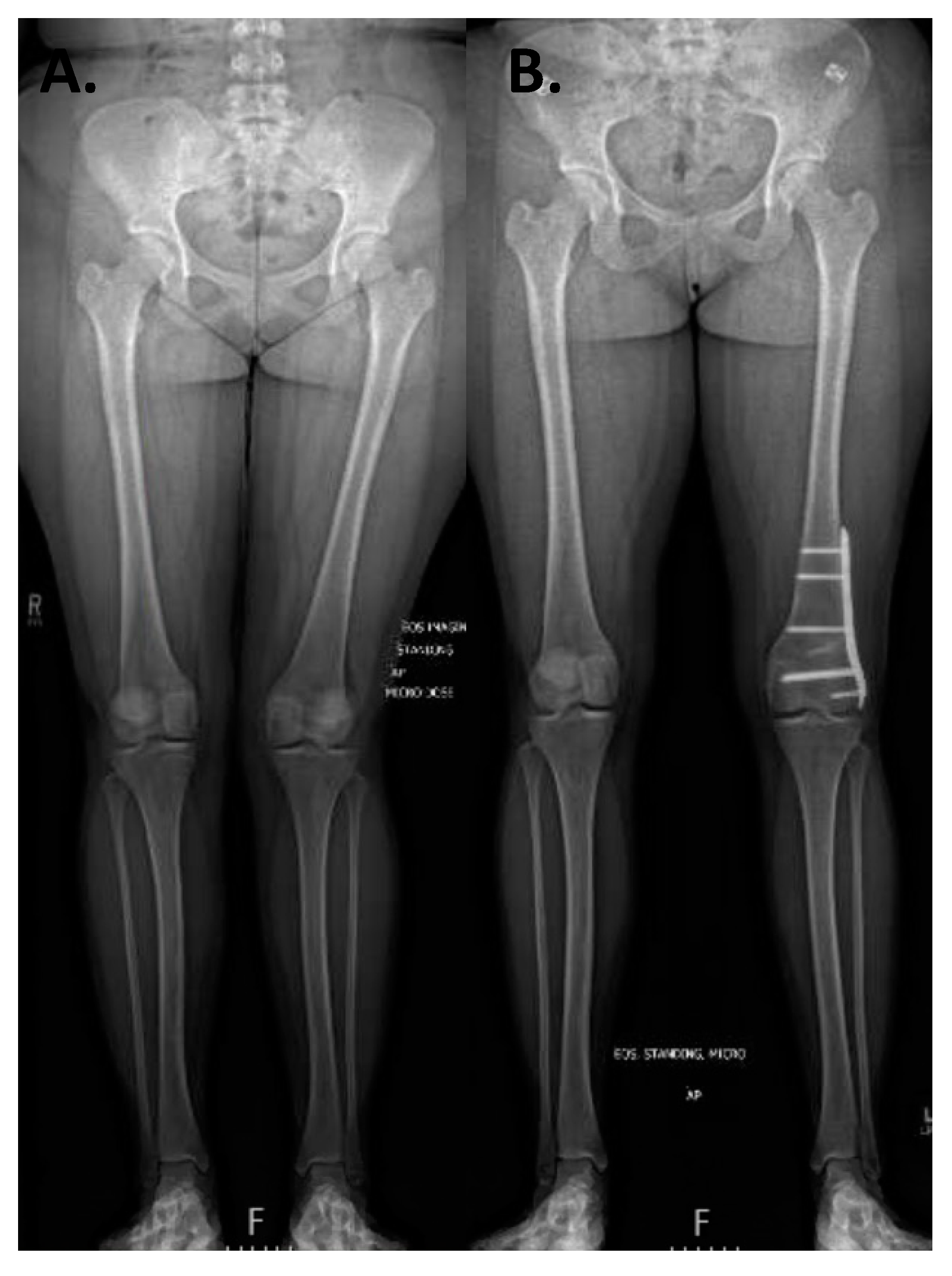
3.1. Coronal Plane Malalignment
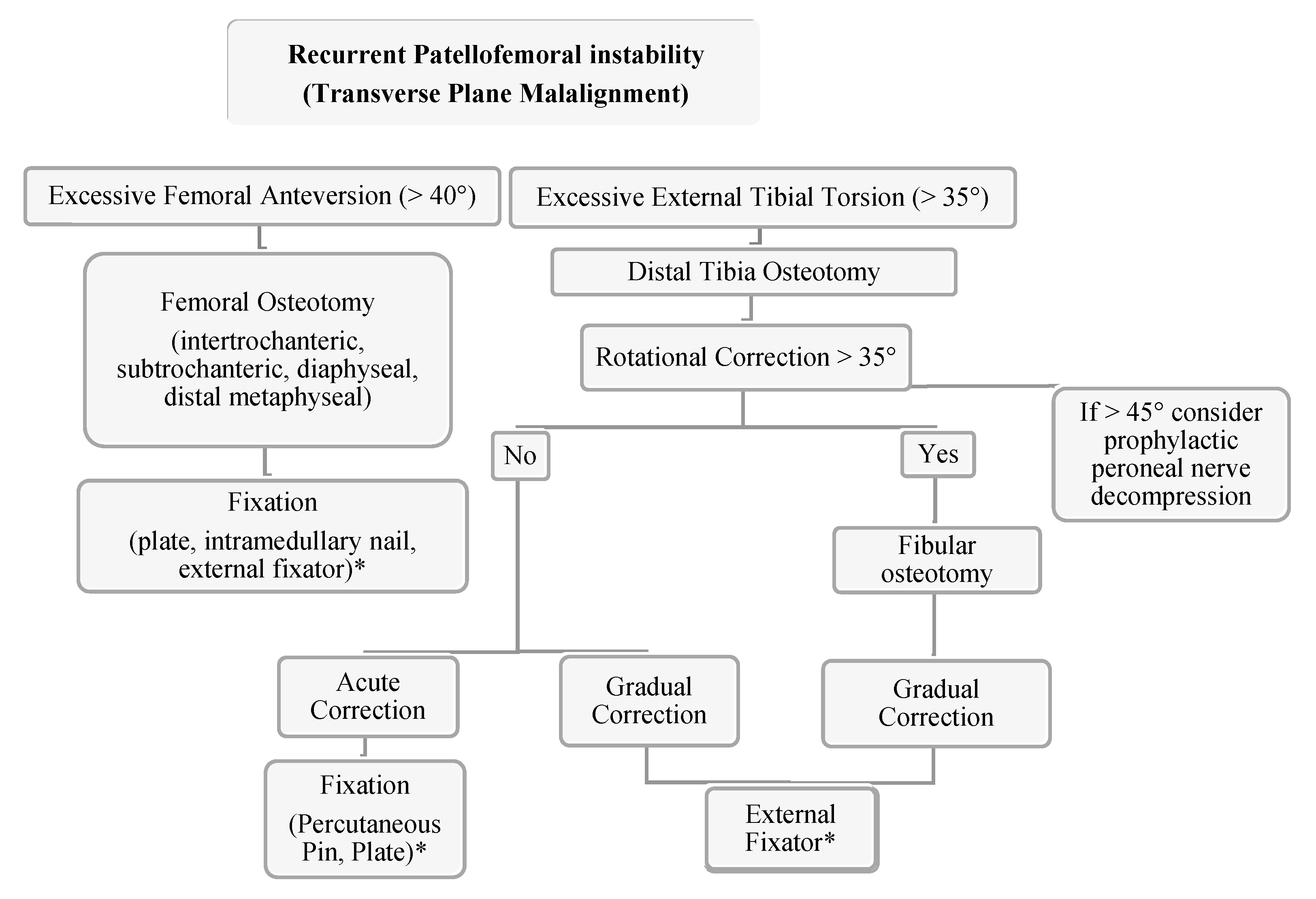
3.2. Transverse Plane Malalignment
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wilson, P.L.; Rathjen, K.E. Disorders of the Knee. In Tachdjian’s Pediatric Orthopaedics, 5th ed.; Herring, J.A., Ed.; Elservier: Saunders, PA, USA, 2014; pp. 702–710. [Google Scholar]
- Parikh, S.N.; Lykissas, M.G. Classification of Lateral Patellar Instability in Children and Adolescents. Orthop. Clin. N. Am. 2016, 47, 145–152. [Google Scholar] [CrossRef]
- Frosch, K.H.; Schmeling, A. A new classification system of patellar instability and patellar maltracking. Arch. Orthop. Trauma Surg. 2016, 136, 485–497. [Google Scholar] [CrossRef] [PubMed]
- Nietosvaara, Y. Acute Patellar Dislocation in Children Incidence and Associated Osteochondral Fractures. J. Pediatr. Orthop. 1994, 14, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Lewallen, L.W.; McIntosh, A.L.; Dahm, D.L. Predictors of recurrent instability after acute patellofemoral dislocation in pediatric and adolescent patients. Am. J. Sports Med. 2013, 41, 575–581. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, J.; Magnussen, R.A.; Collins, C.L.; Currie, D.W.; Best, T.M.; Comstock, R.D.; Flanigan, D.C. Epidemiology of Patellofemoral Instability Injuries Among High School Athletes in the United States. Am. J. Sports Med. 2015, 43, 1676–1682. [Google Scholar] [CrossRef] [PubMed]
- Fithian, D.C.; Paxton, E.W.; Stone, M.L.; Silva, P.; Davis, D.K.; Elias, D.A.; White, L.M. Epidemiology and natural history of acute patellar dislocation. Am. J. Sports Med. 2004, 32, 1114–1121. [Google Scholar] [CrossRef] [PubMed]
- Jaquith, B.P.; Parikh, S.N. Predictors of Recurrent Patellar Instability in Children and Adolescents After First-time Dislocation. J. Pediatr. Orthop. 2017, 37, 484–490. [Google Scholar] [CrossRef]
- Arendt, E.A.; Askenberger, M.; Agel, J.; Tompkins, M.A. Risk of Redislocation After Primary Patellar Dislocation: A Clinical Prediction Model Based on Magnetic Resonance Imaging Variables. Am. J. Sports Med. 2018, 46, 3385–3390. [Google Scholar] [CrossRef]
- Hevesi, M.; Heidenreich, M.J.; Camp, C.L.; Hewett, T.E.; Stuart, M.J.; Dahm, D.L.; Krych, A.J. The Recurrent Instability of the Patella Score: A Statistically Based Model for Prediction of Long-Term Recurrence Risk After First-Time Dislocation. Arthroscopy 2019, 35, 537–543. [Google Scholar] [CrossRef]
- Baumann, C.A.; Hinckel, B.B.; Tanaka, M.J. Update on Patellofemoral Anatomy and Biomehcanics. Oper. Tech. Sports Med. 2019, 27, 1–8. [Google Scholar] [CrossRef]
- Arendt, E.A.; England, K.; Agel, J.; Tompkins, M.A. An analysis of knee anatomic imaging factors associated with primary lateral patellar dislocations. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 3099–3107. [Google Scholar] [CrossRef] [PubMed]
- Askenberger, M.; Janarv, P.M.; Finnbogason, T.; Arendt, E.A. Morphology and Anatomic Patellar Instability Risk Factors in First-Time Traumatic Lateral Patellar Dislocations: A Prospective Magnetic Resonance Imaging Study in Skeletally Immature Children. Am. J. Sports Med. 2017, 45, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- James, S.L. Chondromalacia of the Patella in the Adolescent; Williams & Williams: Baltimore, MD, USA, 1979; pp. 205–251. [Google Scholar]
- Bruce, W.D.; Stevens, P.M. Surgical correction of miserable malalignment syndrome. J. Pediatr. Orthop. 2004, 24, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Somerville, E.W. Persistent foetal alignment of the hip. J. Bone Jt. Surg. Br. 1957, 39-B, 106–113. [Google Scholar] [CrossRef] [PubMed]
- Staheli, L.T.; Corbett, M.; Wyss, C.; King, H. Lower-extremity rotational problems in children. Normal values to guide management. J. Bone Jt. Surg. Br. 1985, 67, 39–47. [Google Scholar] [CrossRef]
- Smits-Engelsman, B.; Klerks, M.; Kirby, A. Beighton score: A valid measure for generalized hypermobility in children. J. Pediatr. 2011, 158, 119–123, 123.e1–123.e4. [Google Scholar] [CrossRef]
- Carter, C.; Wilkinson, J. Persistent Joint Laxity and Congenital Dislocation of the Hip. J. Bone Jt. Surg. Br. 1964, 46, 40–45. [Google Scholar] [CrossRef]
- Sheehan, F.T.; Derasari, A.; Fine, K.M.; Brindle, T.J.; Alter, K.E. Q-angle and J-sign: Indicative of maltracking subgroups in patellofemoral pain. Clin. Orthop Relat. Res. 2010, 468, 266–275. [Google Scholar] [CrossRef] [Green Version]
- Dimon, J., III. Apprehension Test for Subluxation of the Patella. Clin. Orthop. Relat. Res. 1974, 103, 39. [Google Scholar] [CrossRef]
- Ikue, I.; Kazutomo, M.; Kimura, Y. Differences between the Craig’s test and copmuted tomography in measuring femoral anteversion in patients with anterior cruciate injuries. J. Phys. Ther. Sci. 2020, 32, 365–369. [Google Scholar]
- Huberti, H.; Hayes, W.C. Patellofemoral Contact Pressures the Influence of Q-angle and Tendofemoral Contact. J. Bone Jt. Surg. Br. 1984, 66, 715–724. [Google Scholar] [CrossRef]
- Brattstroem, H. Shape of the Intercondylar Groove Normally and in Recurrent Dislocation of Patella. A Clinical and X-Ray-Anatomical Investigation. Acta Orthop. Scand. Suppl. 1964, 68 (Suppl. 68), 61–148. [Google Scholar] [CrossRef] [Green Version]
- Woodland, L.H.; Francis, R.S. Parameters and comparisons of the quadriceps angle of college-aged men and women in the supine and standing positions. Am. J. Sports Med. 1992, 20, 208–211. [Google Scholar] [CrossRef]
- Kling, T. Angular and Torsional Deformities of the Lower Extremities. Clin. Orthop. Relat. Res. 1982, 176, 136–147. [Google Scholar]
- Magee, D.J. Hip. In Orthopedic Physical Assessment, 6th ed.; Elsevier: Saunders, PA, USA, 2014; pp. 710–711. [Google Scholar]
- Ruwe, P.A.; Gage, J.R.; Ozonoff, M.B.; DeLuca, P.A. Clinical determination of femoral anteversion. A comparison with established techniques. J. Bone Jt. Surg. Br. 1992, 74, 820–830. [Google Scholar] [CrossRef]
- Gelberman, R.H.; Cohen, M.S.; Desai, S.S.; Griffin, P.P.; Salamon, P.B.; O’Brien, T.M. Femoral anteversion. A clinical assessment of idiopathic intoeing gait in children. J. Bone Jt. Surg. Br. 1987, 69, 75–79. [Google Scholar] [CrossRef] [PubMed]
- Davids, J.R.; Benfanti, P.; Blackhurst, D.W.; Allen, B.L. Assessment of femoral anteversion in children with cerebral palsy: Accuracy of the trochanteric prominence angle test. J. Pediatr. Orthop. 2002, 22, 173–178. [Google Scholar] [CrossRef]
- Tan EW, C.A. Chapter 104 Patellar Instability, 6th ed.; Scott, W.N., Ed.; Elservier: Amsterdam, The Netherlands, 2018. [Google Scholar] [CrossRef]
- Tamari, K.; Tinley, P.; Briffa, K.; Breidahl, W. Validity and reliability of existing and modified clinical methods of measuring femoral and tibiofibular torsion in healthy subjects: Use of different reference axes may improve reliability. Clin. Anat. 2005, 18, 46–55. [Google Scholar] [CrossRef]
- Laurin, C.A.; Levesque, H.P.; Dussault, R.; Labelle, H.; Peides, J.P. The abnormal lateral patellofemoral angle: A diagnostic roentgenographic sign of recurrent patellar subluxation. J. Bone Jt. Surg. Br. 1978, 60, 55–60. [Google Scholar] [CrossRef]
- Merchant, A.C.; Mercer, R.L.; Jacobsen, R.H.; Cool, C.R. Roentgenographic analysis of patellofemoral congruence. J. Bone Jt. Surg. Br. 1974, 56, 1391–1396. [Google Scholar] [CrossRef]
- Dejour, D.; Walch, G.; Nove-Josserand, L. Factors of patellar instability: An anatomic radiographic study. Knee Surg. Sports Traumatol. Arthrosc. 1994, 2, 19–26. [Google Scholar] [CrossRef]
- Thevenin-Lemoine, C.; Ferrand, M.; Courvoisier, A.; Damsin, J.P.; Ducou le Pointe, H.; Vialle, R. Is the Caton-Deschamps index a valuable ratio to investigate patellar height in children? J. Bone Jt. Surg. Br. 2011, 93, e35. [Google Scholar] [CrossRef]
- Kazley, J.M.; Banerjee, S. Classifications in Brief: The Dejour Classification of Trochlear Dysplasia. Clin. Orthop. Relat. Res. 2019, 477, 2380–2386. [Google Scholar] [CrossRef]
- Stepanovich, M.; Bomar, J.D.; Pennock, A.T. Are the Current Classifications and Radiographic Measurements for Trochlear Dysplasia Appropriate in the Skeletally Immature Patient? Orthop. J. Sports Med. 2016, 4, 2325967116669490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Heyworth, B.E.; Osei, D.A.; Fabricant, P.D.; Schneider, R.; Doyle, S.M.; Green, D.W.; Widmann, R.F.; Lyman, S.; Burke, S.W.; Scher, D.M. The shorthand bone age assessment: A simpler alternative to current methods. J. Pediatr. Orthop. 2013, 33, 569–574. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.J.; Hall, E.J. Computed tomography--an increasing source of radiation exposure. N. Engl. J. Med. 2007, 357, 2277–2284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Paley, D.; Tetsworth, K. Mechanical axis deviation of the lower limbs. Preoperative planning of uniapical angular deformities of the tibia or femur. Clin. Orthop. Relat. Res. 1992, 48–64. [Google Scholar]
- Shearman, C.M.; Brandser, E.A.; Kathol, M.H.; Clark, W.A.; Callaghan, J.J. An easy linear estimation of the mechanical axis on long-leg radiographs. AJR Am. J. Roentgenol. 1998, 170, 1220–1222. [Google Scholar] [CrossRef] [Green Version]
- Paley, D. Principles of Deformity Correction; Springer: Berlin/Heidelberg, Germany, 2002. [Google Scholar]
- Stiebel, M.P.D. Derotational Osteotomies of the Femur and Tibia for Recurrent Patellar Instability. Oper. Tech. Sports Med. 2019, 27. [Google Scholar] [CrossRef]
- Mahboubi, S.; Horstmann, H. Femoral torsion: CT measurement. Radiology 1986, 160, 843–844. [Google Scholar] [CrossRef]
- Parikh, S.; Noyes, F.R. Patellofemoral disorders: Role of computed tomography and magnetic resonance imaging in defining abnormal rotational lower limb alignment. Sports Health 2011, 3, 158–169. [Google Scholar] [CrossRef] [Green Version]
- Weiner, D.S.; Cook, A.J.; Hoyt, W.A., Jr.; Oravec, C.E. Computed tomography in the measurement of femoral anteversion. Orthopedics 1978, 1, 299–306. [Google Scholar] [CrossRef]
- Murphy, S.B.; Simon, S.R.; Kijewski, P.K.; Wilkinson, R.H.; Griscom, N.T. Femoral anteversion. J. Bone Jt. Surg. Br. 1987, 69, 1169–1176. [Google Scholar] [CrossRef]
- Eckhoff, D.G.; Johnson, K.K. Three-dimensional computed tomography reconstruction of tibial torsion. Clin. Orthop. Relat. Res. 1994, 302, 42–46. [Google Scholar] [CrossRef]
- Kaiser, P.; Attal, R.; Kammerer, M.; Thauerer, M.; Hamberger, L.; Mayr, R.; Schmoelz, W. Significant differences in femoral torsion values depending on the CT measurement technique. Arch. Orthop. Trauma Surg. 2016, 136, 1259–1264. [Google Scholar] [CrossRef] [Green Version]
- Yoshioka, Y.; Cooke, T.D. Femoral anteversion: Assessment based on function axes. J. Orthop. Res. 1987, 5, 86–91. [Google Scholar] [CrossRef]
- Waidelich, H.A.; Strecker, W.; Schneider, E. Computed tomographic torsion-angle and length measurement of the lower extremity. The methods, normal values and radiation load. Rofo 1992, 157, 245–251. [Google Scholar] [CrossRef]
- Schmaranzer, F.; Lerch, T.D.; Siebenrock, K.A.; Tannast, M.; Steppacher, S.D. Differences in Femoral Torsion Among Various Measurement Methods Increase in Hips With Excessive Femoral Torsion. Clin. Orthop. Relat. Res. 2019, 477, 1073–1083. [Google Scholar] [CrossRef]
- Jarrett, D.Y.; Oliveira, A.M.; Zou, K.H.; Snyder, B.D.; Kleinman, P.K. Axial Oblique CT to Assess Femoral Anteversion. Am. J. Roentgenol. 2010, 194, 1230–1233. [Google Scholar] [CrossRef]
- Rosskopf, A.B.; Ramseier, L.E.; Sutter, R.; Pfirrmann, C.W.; Buck, F.M. Femoral and tibial torsion measurement in children and adolescents: Comparison of 3D models based on low-dose biplanar radiography and low-dose CT. AJR Am. J. Roentgenol. 2014, 202, W285–W291. [Google Scholar] [CrossRef]
- Rosskopf, A.B.; Buck, F.M.; Pfirrmann, C.W.; Ramseier, L.E. Femoral and tibial torsion measurements in children and adolescents: Comparison of MRI and 3D models based on low-dose biplanar radiographs. Skeletal Radiol. 2017, 46, 469–476. [Google Scholar] [CrossRef]
- Diederichs, G.; Kohlitz, T.; Kornaropoulos, E.; Heller, M.O.; Vollnberg, B.; Scheffler, S. Magnetic resonance imaging analysis of rotational alignment in patients with patellar dislocations. Am. J. Sports Med. 2013, 41, 51–57. [Google Scholar] [CrossRef]
- Sung, K.H.; Youn, K.; Chung, C.Y.; Kitta, M.I.; Kumara, H.C.; Min, J.J.; Lee, J.; Park, M.S. Development and Validation of a Mobile Application for Measuring Femoral Anteversion in Patients With Cerebral Palsy. J. Pediatr. Orthop. 2020, 40, e516–e521. [Google Scholar] [CrossRef]
- Maine, S.T.; O’Gorman, P.; Barzan, M.; Stockton, C.A.; Lloyd, D.; Carty, C.P. Rotational Malalignment of the Knee Extensor Mechanism: Defining Rotation of the Quadriceps and Its Role in the Spectrum of Patellofemoral Joint Instability. JB JS Open Access 2019, 4. [Google Scholar] [CrossRef] [Green Version]
- Clementz, B.G. Assessment of tibial torsion and rotational deformity with a new fluoroscopic technique. Clin. Orthop. Relat. Res. 1989, 245, 199–209. [Google Scholar] [CrossRef]
- Jend, H.H.; Heller, M.; Dallek, M.; Schoettle, H. Measurement of tibial torsion by computer tomography. Acta Radiol. Diagn. 1981, 22, 271–276. [Google Scholar] [CrossRef]
- Liodakis, E.; Doxastaki, I.; Chu, K.; Krettek, C.; Gaulke, R.; Citak, M.; Kenawey, M. Reliability of the assessment of lower limb torsion using computed tomography: Analysis of five different techniques. Skeletal Radiol. 2012, 41, 305–311. [Google Scholar] [CrossRef]
- Richmond, C.G.; Shea, K.G.; Burlile, J.F.; Heyer, A.M.; Ellis, H.B.; Wilson, P.L.; Arendt, E.A.; Tompkins, M.A. Patellar-Trochlear Morphology in Pediatric Patients From 2 to 11 Years of Age: A Descriptive Analysis Based on Computed Tomography Scanning. J. Pediatr. Orthop. 2020, 40, e96–e102. [Google Scholar] [CrossRef]
- Goutallier, D.; Bernageau, J.; Lecudonnec, B. The measurement of the tibial tuberosity. Patella groove distanced technique and results (author’s transl). Rev. Chir. Orthop. Reparatrice Appar. Mot. 1978, 64, 423–428. [Google Scholar]
- Schoettle, P.B.; Zanetti, M.; Seifert, B.; Pfirrmann, C.W.; Fucentese, S.F.; Romero, J. The tibial tuberosity-trochlear groove distance; a comparative study between CT and MRI scanning. Knee 2006, 13, 26–31. [Google Scholar] [CrossRef]
- Camp, C.L.; Stuart, M.J.; Krych, A.J.; Levy, B.A.; Bond, J.R.; Collins, M.S.; Dahm, D.L. CT and MRI measurements of tibial tubercle-trochlear groove distances are not equivalent in patients with patellar instability. Am. J. Sports Med. 2013, 41, 1835–1840. [Google Scholar] [CrossRef]
- Ho, C.P.; James, E.W.; Surowiec, R.K.; Gatlin, C.C.; Ellman, M.B.; Cram, T.R.; Dornan, G.J.; LaPrade, R.F. Systematic technique-dependent differences in CT versus MRI measurement of the tibial tubercle-trochlear groove distance. Am. J. Sports Med. 2015, 43, 675–682. [Google Scholar] [CrossRef]
- Hinckel, B.B.; Gobbi, R.G.; Kihara Filho, E.N.; Demange, M.K.; Pecora, J.R.; Rodrigues, M.B.; Camanho, G.L. Why are bone and soft tissue measurements of the TT-TG distance on MRI different in patients with patellar instability? Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 3053–3060. [Google Scholar] [CrossRef]
- Dickens, A.J.; Morrell, N.T.; Doering, A.; Tandberg, D.; Treme, G. Tibial tubercle-trochlear groove distance: Defining normal in a pediatric population. J. Bone Jt. Surg. Br. 2014, 96, 318–324. [Google Scholar] [CrossRef]
- Seitlinger, G.; Scheurecker, G.; Hogler, R.; Labey, L.; Innocenti, B.; Hofmann, S. Tibial tubercle-posterior cruciate ligament distance: A new measurement to define the position of the tibial tubercle in patients with patellar dislocation. Am. J. Sports Med. 2012, 40, 1119–1125. [Google Scholar] [CrossRef] [PubMed]
- Chassaing, V.; Zeitoun, J.M.; Camara, M.; Blin, J.L.; Marque, S.; Chancelier, M.D. Tibial tubercle torsion, a new factor of patellar instability. Orthop. Traumatol. Surg. Res. 2017, 103, 1173–1178. [Google Scholar] [CrossRef] [PubMed]
- Hughston, J.C. Subluxation of the patella. J. Bone Jt. Surg. Br. 1968, 50, 1003–1026. [Google Scholar] [CrossRef]
- Insall, J.; Bullough, P.G.; Burstein, A.H. Proximal "tube" realignment of the patella for chondromalacia patellae. Clin. Orthop. Relat. Res. 1979, 144, 63–69. [Google Scholar] [CrossRef]
- Andrish, J. The management of recurrent patellar dislocation. Orthop. Clin. N. Am. 2008, 39, 313–327. [Google Scholar] [CrossRef]
- Panagopoulos, A.; van Niekerk, L.; Triantafillopoulos, I.K. MPFL reconstruction for recurrent patella dislocation: A new surgical technique and review of the literature. Int. J. Sports Med. 2008, 29, 359–365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Redler, L.H.; Wright, M.L. Surgical Management of Patellofemoral Instability in the Skeletally Immature Patient. J. Am. Acad Orthop. Surg. 2018, 26, e405–e415. [Google Scholar] [CrossRef] [PubMed]
- Maenpaa, H.; Huhtala, H.; Lehto, M.U. Recurrence after patellar dislocation. Redislocation in 37/75 patients followed for 6-24 years. Acta Orthop. Scand. 1997, 68, 424–426. [Google Scholar] [CrossRef] [PubMed]
- Miler, M. Patellofemoral Instability and Other Common Knee Issues in the Skeletally Immature Athlete. In Orthopaedic Knowledge Update: Sports Medicine 5, 5th ed.; Milewski, M., Ed.; American Academy of Orthopaedic Surgeons: Rosemont, IL, USA, 2016; pp. 667–670. [Google Scholar]
- Hennrikus, W.; Pylawka, T. Patellofemoral instability in skeletally immature athletes. Instr. Course Lect. 2013, 62, 445–453. [Google Scholar] [PubMed]
- Cootjans, K.; Dujardin, J.; Vandenneucker, H.; Bellemans, J. A surgical algorithm for the treatment of recurrent patellar dislocation. Results at 5 year follow-up. Acta Orthop. Belg. 2013, 79, 318–325. [Google Scholar]
- Gruskay, J.A.; Gomoll, A.H.; Arendt, E.A.; Dejour, D.H.; Strickland, S.M. Patellar Instability and Dislocation: Optimizing Surgical Treatment and How to Avoid Complications. Instr. Course Lect. 2020, 69, 671–692. [Google Scholar]
- Liu, J.N.; Steinhaus, M.E.; Kalbian, I.L.; Post, W.R.; Green, D.W.; Strickland, S.M.; Shubin Stein, B.E. Patellar Instability Management: A Survey of the International Patellofemoral Study Group. Am. J. Sports Med. 2018, 46, 3299–3306. [Google Scholar] [CrossRef]
- Tompkins, M.A.; Arendt, E.A. Patellar instability factors in isolated medial patellofemoral ligament reconstructions--What does the literature tell us? A systematic review. Am. J. Sports Med. 2015, 43, 2318–2327. [Google Scholar] [CrossRef]
- Puzzitiello, R.N.; Waterman, B.; Agarwalla, A.; Zuke, W.; Cole, B.J.; Verma, N.N.; Yanke, A.B.; Forsythe, B. Primary Medial Patellofemoral Ligament Repair Versus Reconstruction: Rates and Risk Factors for Instability Recurrence in a Young, Active Patient Population. Arthroscopy 2019, 35, 2909–2915. [Google Scholar] [CrossRef]
- Previtali, D.; Milev, S.R.; Pagliazzi, G.; Filardo, G.; Zaffagnini, S.; Candrian, C. Recurrent Patellar Dislocations Without Untreated Predisposing Factors: Medial Patellofemoral Ligament Reconstruction Versus Other Medial Soft-Tissue Surgical Techniques-A Meta-analysis. Arthroscopy 2020, 36, 1725–1734. [Google Scholar] [CrossRef]
- Kumar, N.; Bastrom, T.P.; Dennis, M.M.; Pennock, A.T.; Edmonds, E.W. Adolescent Medial Patellofemoral Ligament Reconstruction: A Comparison of the Use of Autograft Versus Allograft Hamstring. Orthop. J. Sports Med. 2018, 6, 2325967118774272. [Google Scholar] [CrossRef] [Green Version]
- Lemaire, M. Reinforcement of tendons and ligaments with carbon fibers. Four years, 1300 cases. Clin. Orthop. Relat. Res. 1985, 196, 169–174. [Google Scholar]
- Ellera Gomes, J.L. Medial patellofemoral ligament reconstruction for recurrent dislocation of the patella: A preliminary report. Arthroscopy 1992, 8, 335–340. [Google Scholar] [CrossRef]
- Kearney, S.P.; Mosca, V.S. Selective hemiepiphyseodesis for patellar instability with associated genu valgum. J. Orthop. 2015, 12, 17–22. [Google Scholar] [CrossRef] [Green Version]
- Lin, K.M.; Fabricant, P.D. CORR Synthesis: Can Guided Growth for Angular Deformity Correction Be Applied to Management of Pediatric Patellofemoral Instability? Clin. Orthop. Relat. Res. 2020, 478, 2231–2238. [Google Scholar] [CrossRef] [PubMed]
- Bachmann, M.; Rutz, E.; Brunner, R.; Gaston, M.S.; Hirschmann, M.T.; Camathias, C. Temporary hemiepiphysiodesis of the distal medial femur: MPFL in danger. Arch. Orthop. Trauma Surg. 2014, 134, 1059–1064. [Google Scholar] [CrossRef]
- Metaizeau, J.P.; Wong-Chung, J.; Bertrand, H.; Pasquier, P. Percutaneous epiphysiodesis using transphyseal screws (PETS). J. Pediatr. Orthop. 1998, 18, 363–369. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.N.; Redman, C.; Gopinathan, N.R. Simultaneous treatment for patellar instability and genu valgum in skeletally immature patients: A preliminary study. J. Pediatr. Orthop. B 2019, 28, 132–138. [Google Scholar] [CrossRef]
- Frings, J.; Krause, M.; Akoto, R.; Wohlmuth, P.; Frosch, K.H. Combined distal femoral osteotomy (DFO) in genu valgum leads to reliable patellar stabilization and an improvement in knee function. Knee Surg. Sports Traumatol. Arthrosc. 2018, 26, 3572–3581. [Google Scholar] [CrossRef]
- Wilson, P.L.; Black, S.R.; Ellis, H.B.; Podeszwa, D.A. Distal Femoral Valgus and Recurrent Traumatic Patellar Instability: Is an Isolated Varus Producing Distal Femoral Osteotomy a Treatment Option? J. Pediatr. Orthop. 2018, 38, e162–e167. [Google Scholar] [CrossRef]
- Fabry, G.; MacEwen, G.D.; Shands, A.R., Jr. Torsion of the femur. A follow-up study in normal and abnormal conditions. J. Bone Jt. Surg. Br. 1973, 55, 1726–1738. [Google Scholar] [CrossRef]
- Eckhoff, D.G.; Montgomery, W.K.; Kilcoyne, R.F.; Stamm, E.R. Femoral morphometry and anterior knee pain. Clin. Orthop. Relat. Res. 1994, 64–68. [Google Scholar] [CrossRef]
- Eckhoff, D.G.; Brown, A.W.; Kilcoyne, R.F.; Stamm, E.R. Knee version associated with anterior knee pain. Clin. Orthop. Relat. Res. 1997, 10, 152–155. [Google Scholar] [CrossRef]
- Cameron, J.C.; Saha, S. External tibial torsion: An underrecognized cause of recurrent patellar dislocation. Clin. Orthop. Relat. Res. 1996, 177–184. [Google Scholar] [CrossRef]
- Eckhoff, D.G.; Kramer, R.C.; Alongi, C.A.; VanGerven, D.P. Femoral anteversion and arthritis of the knee. J. Pediatr. Orthop. 1994, 14, 608–610. [Google Scholar] [CrossRef]
- Cooke, T.D.; Price, N.; Fisher, B.; Hedden, D. The inwardly pointing knee. An unrecognized problem of external rotational malalignment. Clin. Orthop. Relat. Res. 1990, 260, 56–60. [Google Scholar] [CrossRef]
- Teitge, R.A. The power of transverse plane limb mal-alignment in the genesis of anterior knee pain—clinical relevance. Ann. Jt. 2018, 3, 70. [Google Scholar] [CrossRef]
- Nelitz, M. Femoral Derotational Osteotomies. Curr. Rev. Musculoskelet. Med. 2018, 11, 272–279. [Google Scholar] [CrossRef] [PubMed]
- Herzenberg, J.E.; Smith, J.D.; Paley, D. Correcting torsional deformities with Ilizarov’s apparatus. Clin. Orthop. Relat. Res. 1994, 302, 36–41. [Google Scholar]
- Teitge, R.A. Osteotomy in the Treatment of Patellofemoral Instability. Tech. Knee Surg. 2006, 5, 2–18. [Google Scholar] [CrossRef]
- Imhoff, F.B.; Beitzel, K.; Zakko, P.; Obopilwe, E.; Voss, A.; Scheiderer, B.; Morikawa, D.; Mazzocca, A.D.; Arciero, R.A.; Imhoff, A.B. Derotational Osteotomy of the Distal Femur for the Treatment of Patellofemoral Instability Simultaneously Leads to the Correction of Frontal Alignment: A Laboratory Cadaveric Study. Orthop. J. Sports Med. 2018, 6, 2325967118775664. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, P.; Schmoelz, W.; Schottle, P.B.; Heinrichs, C.; Zwierzina, M.; Attal, R. Isolated medial patellofemoral ligament reconstruction for patella instability is insufficient for higher degrees of internal femoral torsion. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 758–765. [Google Scholar] [CrossRef]
- Ateschrang, A.; Freude, T.; Grunwald, L.; Schaffler, A.; Stockle, U.; Schroter, S. Patella dislocation: An algorithm for diagnostic and treatment considering the rotation. Z. Orthop. Unfall. 2014, 152, 59–67. [Google Scholar] [CrossRef] [Green Version]
- Hinterwimmer, S.; Rosenstiel, N.; Lenich, A.; Waldt, S.; Imhoff, A.B. Femoral osteotomy for patellofemoral instability. Unfallchirurg 2012, 115, 410–416. [Google Scholar] [CrossRef]
- Lee, S.Y.; Jeong, J.; Lee, K.; Chung, C.Y.; Lee, K.M.; Kwon, S.S.; Choi, Y.; Kim, T.G.; Lee, J.I.; Lee, J.; et al. Unexpected angular or rotational deformity after corrective osteotomy. BMC Musculoskelet. Disord. 2014, 15, 175. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, S.S. Three-dimensional Effect of the Single Plane Proximal Femur Osteotomy. Hip Pelvis 2015, 27, 23–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelitz, M.; Wehner, T.; Steiner, M.; Durselen, L.; Lippacher, S. The effects of femoral external derotational osteotomy on frontal plane alignment. Knee Surg. Sports Traumatol. Arthrosc. 2014, 22, 2740–2746. [Google Scholar] [CrossRef]
- Kaiser, P.; Konschake, M.; Loth, F.; Plaikner, M.; Attal, R.; Liebensteiner, M.; Schlumberger, M. Derotational femoral osteotomy changes patella tilt, patella engagement and tibial tuberosity trochlear groove distance. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 926–933. [Google Scholar] [CrossRef]
- Hoekstra, H.; Rosseels, W.; Sermon, A.; Nijs, S. Corrective limb osteotomy using patient specific 3D-printed guides: A technical note. Injury 2016, 47, 2375–2380. [Google Scholar] [CrossRef] [PubMed]
- Zheng, P.; Xu, P.; Yao, Q.; Tang, K.; Lou, Y. 3D-printed navigation template in proximal femoral osteotomy for older children with developmental dysplasia of the hip. Sci. Rep. 2017, 7, 44993. [Google Scholar] [CrossRef] [PubMed]
- Victor, J.; Premanathan, A. Virtual 3D planning and patient specific surgical guides for osteotomies around the knee: A feasibility and proof-of-concept study. Bone Jt. J. 2013, 95-B, 153–158. [Google Scholar] [CrossRef]
- Hankemeier, S.; Hufner, T.; Wang, G.; Kendoff, D.; Zeichen, J.; Zheng, G.; Krettek, C. Navigated open-wedge high tibial osteotomy: Advantages and disadvantages compared to the conventional technique in a cadaver study. Knee Surg. Sports Traumatol. Arthrosc. 2006, 14, 917–921. [Google Scholar] [CrossRef] [PubMed]
- Imhoff, F.B.; Schnell, J.; Magana, A.; Diermeier, T.; Scheiderer, B.; Braun, S.; Imhoff, A.B.; Arciero, R.A.; Beitzel, K. Single cut distal femoral osteotomy for correction of femoral torsion and valgus malformity in patellofemoral malalignment-proof of application of new trigonometrical calculations and 3D-printed cutting guides. BMC Musculoskelet. Disord. 2018, 19, 215. [Google Scholar] [CrossRef]
- Merle, R.; Descamps, L. Plane oblique osteotomy in correction of deformities of the extremities. Mem. Acad. Chir. 1952, 78, 271–276. [Google Scholar]
- Wilkens, K.J.; Nicolaou, D.A.; Lee, M.A. Novel venting technique for intramedullary rod fixation of pathologic fractures. Orthopedics 2011, 34, 776–779. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martin, R.; Leighton, R.K.; Petrie, D.; Ikejiani, C.; Smyth, B. Effect of proximal and distal venting during intramedullary nailing. Clin. Orthop. Relat. Res. 1996, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Weisz, G.M.; Rang, M.; Salter, R.B. Posttraumatic fat embolism in children: Review of the literature and of experience in the Hospital for Sick Children, Toronto. J. Trauma 1973, 13, 529–534. [Google Scholar] [CrossRef]
- Edwards, K.J.; Cummings, R.J. Fat embolism as a complication of closed femoral shortening. J. Pediatr. Orthop. 1992, 12, 542–543. [Google Scholar] [CrossRef] [PubMed]
- Blondel, B.; Violas, P.; Launay, F.; Sales de Gauzy, J.; Kohler, R.; Jouve, J.L.; Bollini, G. Fat embolism during limb lengthening with a centromedullary nail: Three cases. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2008, 94, 510–514. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Pape, H.C.; Cohen, A.P.; Krettek, C.; Smith, R.M. Review: Systemic effects of femoral nailing: From Kuntscher to the immune reactivity era. Clin. Orthop. Relat. Res. 2002, 404, 378–386. [Google Scholar] [CrossRef]
- Eriksson, E.A.; Rickey, J.; Leon, S.M.; Minshall, C.T.; Fakhry, S.M.; Schandl, C.A. Fat embolism in pediatric patients: An autopsy evaluation of incidence and etiology. J. Crit. Care 2015, 30, 221.e1–221.e5. [Google Scholar] [CrossRef]
- Teitge, R. Patellofemoral Disorders: Correction of Rotational Malalignment of the Lower Extremity. In Noyes’ Knee Disorders: Surgery, Rehabilitation, Clinical Outcomes, 2nd ed.; Noyes, F., Ed.; Elsevier: Saunders, PA, USA, 2017; pp. 1014–1035. [Google Scholar] [CrossRef]
- Krengel, W.F., 3rd; Staheli, L.T. Tibial rotational osteotomy for idiopathic torsion. A comparison of the proximal and distal osteotomy levels. Clin. Orthop. Relat. Res. 1992, 283, 285–289. [Google Scholar]
- Delgado, E.D.; Schoenecker, P.L.; Rich, M.M.; Capelli, A.M. Treatment of severe torsional malalignment syndrome. J. Pediatric Orthop. 1996, 16, 484–488. [Google Scholar] [CrossRef]
- Tetsworth, K.D.; Thorsell, J.D. Combined techniques for the safe correction of very large tibial rotational deformities in adults. J. Limb Lengthen. Reconstr. 2015, 1, 6–13. [Google Scholar] [CrossRef]
- Nogueira, M.P.; Hernandez, A.J.; Pereira, C.A.M.; Paley, D.; Bhave, A. Surgical decompression of the peroneal nerve in the correction of lower limb deformities: A cadaveric study. J. Limb Lengthen. Reconstr. 2016, 2, 76–81. [Google Scholar] [CrossRef]
- Nogueira, M.P.; Paley, D.; FRCSC. Prophylactic and Therapeutic Peroneal Nerve Decompression for Deformity Correction and Lengthening. Oper. Tech. Orthop. 2011, 21, 180–183. [Google Scholar] [CrossRef] [Green Version]
- Galardi, G.; Comi, G.; Lozza, L.; Marchettini, P.; Novarina, M.; Facchini, R.; Paronzini, A. Peripheral nerve damage during limb lengthening. Neurophysiology in five cases of bilateral tibial lengthening. J. Bone Jt. Surg. Br. 1990, 72, 121–124. [Google Scholar] [CrossRef]
- Turner, M.S. The association between tibial torsion and knee joint pathology. Clin. Orthop Relat Res. 1994, 302, 47–51. [Google Scholar] [CrossRef]
- Staheli, L.T. Torsion--treatment indications. Clin. Orthop. Relat. Res. 1989, 247, 61–66. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Physical Exam Finding | Points (1 Point for Each Side, 9 Total) |
|---|---|
| Knee hyperextension (>10 degrees) | 2 |
| Elbow hyperextension (>10 degrees) | 2 |
| Metacarpophalangeal joint extension >90° | 2 |
| Ability to flex thumb to forearm | 2 |
| Place palms flat on floor on forward bend | 1 |
| Dejour Type | Lateral Radiograph Findings | Significance |
|---|---|---|
| Type A | Crossing sign | Shallow trochlea; trochlear groove lies in same plane as anterior border of lateral condyle |
| Type B | Crossing sign, supratrochlear spur | Flat/convex trochlea; spurring about proximal aspect of trochlea |
| Type C | Crossing sign, double contour | Trochlear facet asymmetry (convex lateral facet, hypoplastic medial facet); anterior border of lateral condyle lies anterior to anterior border of medial condyle |
| Type D | Crossing sign, double contour, supratrochlear spur | All 3 findings present with characteristic “cliff” pattern (lateral trochlear vertical sloping) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Palmer, R.C.; Podeszwa, D.A.; Wilson, P.L.; Ellis, H.B. Coronal and Transverse Malalignment in Pediatric Patellofemoral Instability. J. Clin. Med. 2021, 10, 3035. https://doi.org/10.3390/jcm10143035
Palmer RC, Podeszwa DA, Wilson PL, Ellis HB. Coronal and Transverse Malalignment in Pediatric Patellofemoral Instability. Journal of Clinical Medicine. 2021; 10(14):3035. https://doi.org/10.3390/jcm10143035
Chicago/Turabian StylePalmer, Robert C., David A. Podeszwa, Philip L. Wilson, and Henry B. Ellis. 2021. "Coronal and Transverse Malalignment in Pediatric Patellofemoral Instability" Journal of Clinical Medicine 10, no. 14: 3035. https://doi.org/10.3390/jcm10143035
APA StylePalmer, R. C., Podeszwa, D. A., Wilson, P. L., & Ellis, H. B. (2021). Coronal and Transverse Malalignment in Pediatric Patellofemoral Instability. Journal of Clinical Medicine, 10(14), 3035. https://doi.org/10.3390/jcm10143035