
Proximal Tibiofibular Dislocation in Closing-Wedge High Tibial Osteotomy Increases the Risk of Medium and Long-Term Total Knee Replacement

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Subjects
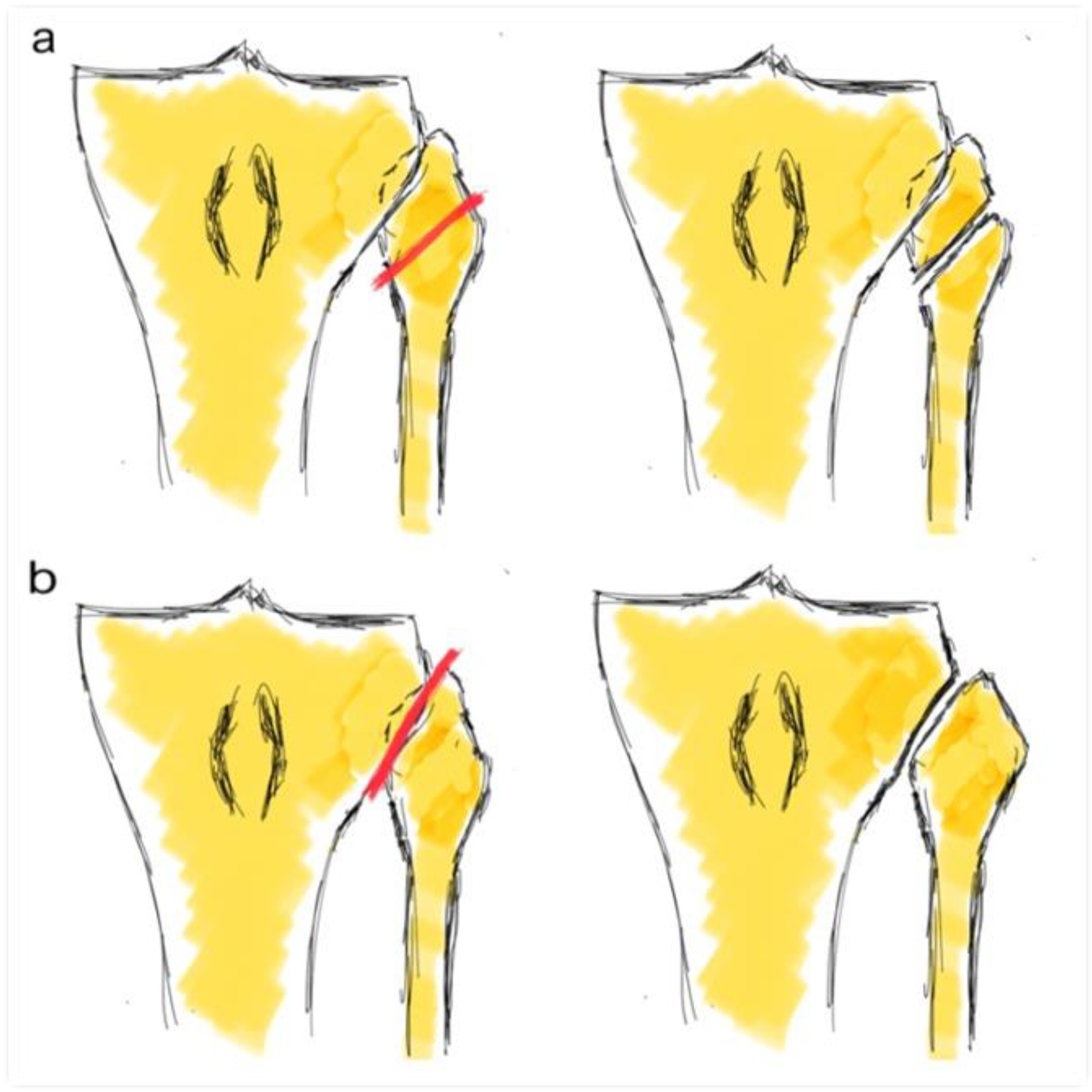
2.2. Surgical Procedure
2.3. Radiological Evaluation
2.4. Clinical Evaluation
2.5. Statistical Analysis
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Loia, M.C.; Vanni, S.; Rosso, F.; Bonasia, D.E.; Bruzzone, M.; Dettoni, F.; Rossi, R. High tibial osteotomy in varus knees: Indications and limits. Joints 2016, 4, 98–110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McNamara, I.; Birmingham, T.B.; Fowler, P.J.; Giffin, J.R. High tibial osteotomy: Evolution of research and clinical applica-tions—A Canadian experience. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Filho, R.B.; Xará-Leite, F.; Andrade, R.; Pereira, R.; Schott, V.; Neyret, P.; Espregueira-Mendes, J. Survivorship of high tibial osteotomy: Comparison between opening and closing wedge osteotomy. Ann. Jt. 2018, 3, 52. [Google Scholar] [CrossRef]
- Sabzevari, S.; Ebrahimpour, A.; Roudi, M.K.; Kachooei, A.R. High Tibial Osteotomy: A Systematic Review and Current Concept. Arch. Bone Jt. Surg. 2016, 4, 204–212. [Google Scholar] [PubMed]
- Brouwer, R.W.; Huizinga, M.R.; Duivenvoorden, T.; Van Raaij, T.M.; Verhagen, A.P.; A Bierma-Zeinstra, S.M.; Verhaar, J.A.N. Osteotomy for treating knee osteoarthritis. Cochrane Database Syst. Rev. 2014. [Google Scholar] [CrossRef]
- van Egmond, N.; van Grinsven, S.; van Loon, C.J.M.; Gaasbeek, R.D.; van Kampen, A. Better clinical results after closed- compared to open-wedge high tibial osteotomy in patients with medial knee osteoarthritis and varus leg alignment. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Bicer, E.K.; Basa, C.D.; Günay, H.; Aydogdu, S.; Sur, H. The fate of fibular osteotomies performed during high tibial osteotomy. Arch. Orthop. Trauma Surg. 2016, 136, 1085–1090. [Google Scholar] [CrossRef] [PubMed]
- Özcan, Ö.; Eroglu, M.; Boya, H.; Kaya, Y. Proximal tibiofibular joint pain versus peroneal nerve dysfunction: Clinical results of closed-wedge high tibial osteotomy performed with proximal tibiofibular joint disruption. Knee Surg. Sports Traumatol. Arthrosc. 2016, 25, 2936–2941. [Google Scholar] [CrossRef]
- Torres-Claramunt, R.; Sánchez-Soler, J.F.; Hinarejos, P.; Sala-Pujals, A.; Leal-Blanquet, J.; Monllau, J.C. Proximal Tibiofibular Dis-location in a Closing-Wedge High Tibial Osteotomy Causes Lateral Radiological Gapping of the Knee: A Prospective Ran-domized Study. J. Clin. Med. 2020, 9, 1622. [Google Scholar] [CrossRef]
- Sasaki, E.; Akimoto, H.; Iio, K.; Fujita, Y.; Saruga, T.; Kakizaki, H.; Ishibashi, Y. Long-term survival rate of closing wedge high tibial osteotomy with high valgus correction: A 15-year follow-up study. Knee Surg. Sports Traumatol. Arthrosc. 2020, 1–8. [Google Scholar] [CrossRef]
- Hui, C.; Salmon, L.J.; Kok, A.; Williams, H.A.; Hockers, N.; van der Tempel, W.M.; Chana, R.; Pinczewski, L.A. Long-term survival of high tibial osteotomy for medial compartment osteoarthritis of the knee. Am. J. Sports Med. 2011, 39, 64–70. [Google Scholar] [CrossRef] [PubMed]
- Polat, G.; Balcı, H.I.; Çakmak, M.F.; Demirel, M.; Şen, C.; Aşık, M. Long-term results and comparison of the three different high tibial osteotomy and fixation techniques in medial compartment arthrosis. J. Orthop. Surg. Res. 2017, 12, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Insall, J.N.; Dorr, L.D. Rationale of the Knee Society clinical rating system. Clin. Orthop. 1989, 248, 13. [Google Scholar] [CrossRef]
- Ares, O.; Castellet, E.; Maculé, F.; León, V.; Montañez, E.; Freire, A.; Hinarejos, P.; Montserrat, F.; Amillo, J.R. Translation and valida-tion of ’The Knee Society Clinical Rating System’ into Spanish. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 2618–2624. [Google Scholar] [CrossRef]
- Likert, R. A technique for the measurement of attitudes. Arch. Psychol. 1932, 140, 1–55. [Google Scholar]
- Yang, Z.Y.; Chen, W.; Li, C.X.; Wang, J.; Shao, D.C.; Hou, Z.Y.; Gao, S.J.; Wang, F.; Li, J.D.; Hao, J.D.; et al. Medial compartment decompression by fibular osteotomy to treat medial compartment knee osteoarthritis: A Pilot Study. Orthopedics 2015, 38, e1110–e1114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zou, G.; Lan, W.; Zeng, Y.; Xie, J.; Chen, S.; Qiu, Y. Early clinical effect of proximal fibular osteotomy on knee osteoarthritis. Bio-Med. Res. 2017, 28, 9291–9294. [Google Scholar]
- Wang, X.; Wei, L.; Lv, Z.; Zhao, B.; Duan, Z.; Wu, W.; Zhang, B.; Wei, X. Proximal fibular osteotomy: A new surgery for pain relief and improvement of joint function in patients with knee osteoarthritis. J. Int. Med. Res. 2017, 45, 282–289. [Google Scholar] [CrossRef] [Green Version]
- Lu, Z.K.; Huang, C.; Wang, F.; Miao, S.; Zeng, L.; He, S.; Ye, X.; Chen, W. Combination of Proximal Fibulectomy with Arthroscopic Partial Meniscectomy for Medial Compartment Osteoarthritis Accompanied by Medial Meniscal Tear. J. Clin. Diagn. Res. 2018, 12, 1–3. [Google Scholar] [CrossRef]
- Liu, B.; Chen, W.; Zhang, Q.; Yan, X.; Zhang, F.; Dong, T.; Yang, G.; Zhang, Y. Proximal fibular osteotomy to treat medial compart-ment knee osteoarthritis: Preoperational factors for short-term prognosis. PLoS ONE 2018, 13, e0197980. [Google Scholar]
- Nie, Y.; Ma, J.; Huang, Z.; Xu, B.; Tang, S.; Shen, B.; Kraus, V.B.; Pei, F. Upper partial fibulectomy improves knee biomechanics and function and decreases knee pain of osteoarthritis: A pilot and biomechanical study. J. Biomech. 2018, 71, 22–29. [Google Scholar] [CrossRef]
- Qin, D.; Chen, W.; Wang, J.; Lv, H.; Ma, W.; Dong, T.; Zhang, Y. Mechanism and influencing factors of proximal fibular osteotomy for treatment of medial compartment knee osteoarthritis: A prospective study. J. Int. Med. Res. 2018, 46, 3114–3123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Utomo, D.N.; Mahyudin, F.; Wijaya, A.M.; Widhiyanto, L. Proximal fibula osteotomy as an alternative to TKA and HTO in late-stage varus type of knee osteoarthritis. J. Orthop. 2018, 15, 858–861. [Google Scholar] [CrossRef] [PubMed]
- Yazdi, H.; Mallakzadeh, M.; Mohtajeb, M.; Farshidfar, S.S.; Baghery, A.; Givehchian, B. The effect of partial fibulectomy on contact pressure of the knee: A cadaveric study. Eur. J. Orthop. Surg. Traumatol. 2014, 24, 1285–1289. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Lin, Z.; Zeng, X.; Ma, L.; Chen, L.; Xia, H.; Zhang, Y. Kinematic characteristics of an osteotomy of the proximal aspect of the fibula during walking: A case report. JBJS Case Connect. 2017, 7, e43. [Google Scholar] [CrossRef]
- Baldini, T.; Roberts, J.; Hao, J.; Hunt, K.; Dayton, M.; Hogan, C. Medial compartment decompression by proximal fibular osteot-omy: A biomechanical cadaver study. Orthopedics 2018, 41, e496–e501. [Google Scholar] [CrossRef]
- Wang, J.; Lv, H.; Chen, W.; Fan, M.; Li, M.; Zhang, Y. Anatomical Adaptation of Fibula and its Mechanism of Proximal Partial Fibulectomy Associated with Medial Compartment Knee Osteoarthritis. Orthop. Surg. 2019, 11, 204–211. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Title | Group 1. FHO (n 105) | Group 2. TFJD (n 125) | p-Value |
|---|---|---|---|
| Age (years) | 53.2 (SD 9.2) | 54.9 (SD 8.4) | n.s. |
| Biological sex (male/female) | 70/35 | 81/44 | n.s. |
| Body mass index (Kg/m2) | 30.2 (SD 7.4) | 29.2 (SD 4.6) | n.s. |
| Side (right/left) | 47/58 | 64/61 | n.s. |
| Previous FTA | 170.9° (SD 3.6) | 171.6° (SD 2.3) | n.s. |
| Ahlbäck preop | 1.9 (SD 0.3) | 2.1 (SD 0.4) | n.s. |
| KSS knee | 53.9 | 54.7 | n.s. |
| KSS function | 69.8 | 71.3 | n.s. |
| Title | Group 1. FHO (n 105) | Group 2. TFJD (n 125) | p-Value |
|---|---|---|---|
| Infection | 7 | 9 | n.s. |
| Osteotomy failure | 3 | 4 | n.s. |
| Title | Group 1. FHO (n 105) | Group 2. TFJD (n 125) | p-Value |
|---|---|---|---|
| Mean Follow-Up (FU) | 109.8 months (SD 45.6) | 87.3 months (SD 32.3) | 0.01 |
| KSS R | 86.5 (SD 15.9) | 84.3 (SD 15.8) | 0.33 |
| KSS F | 79.7 (SD 23.2) | 77.6 (SD 20.6) | 0.31 |
| FTA 1y FU | 178.9° (SD 4.8) | 179.9° (SD 3.8) | 0.12 |
| FTA final FU | 178.7° (SD 4.9) | 179.5° (SD 4.2) | 0.11 |
| Undercorrected FTA ≤ 180° | 52 (49.5%) | 58 (46.4%) | 0.13 |
| Ahlbäck 1y FU | 2.07 (SD 0.6) | 2.27 (SD 0.4) | 0.06 |
| Ahlbäck final FU | 2.21 (SD 0.5) | 2.55 (0.5) | 0.02 * |
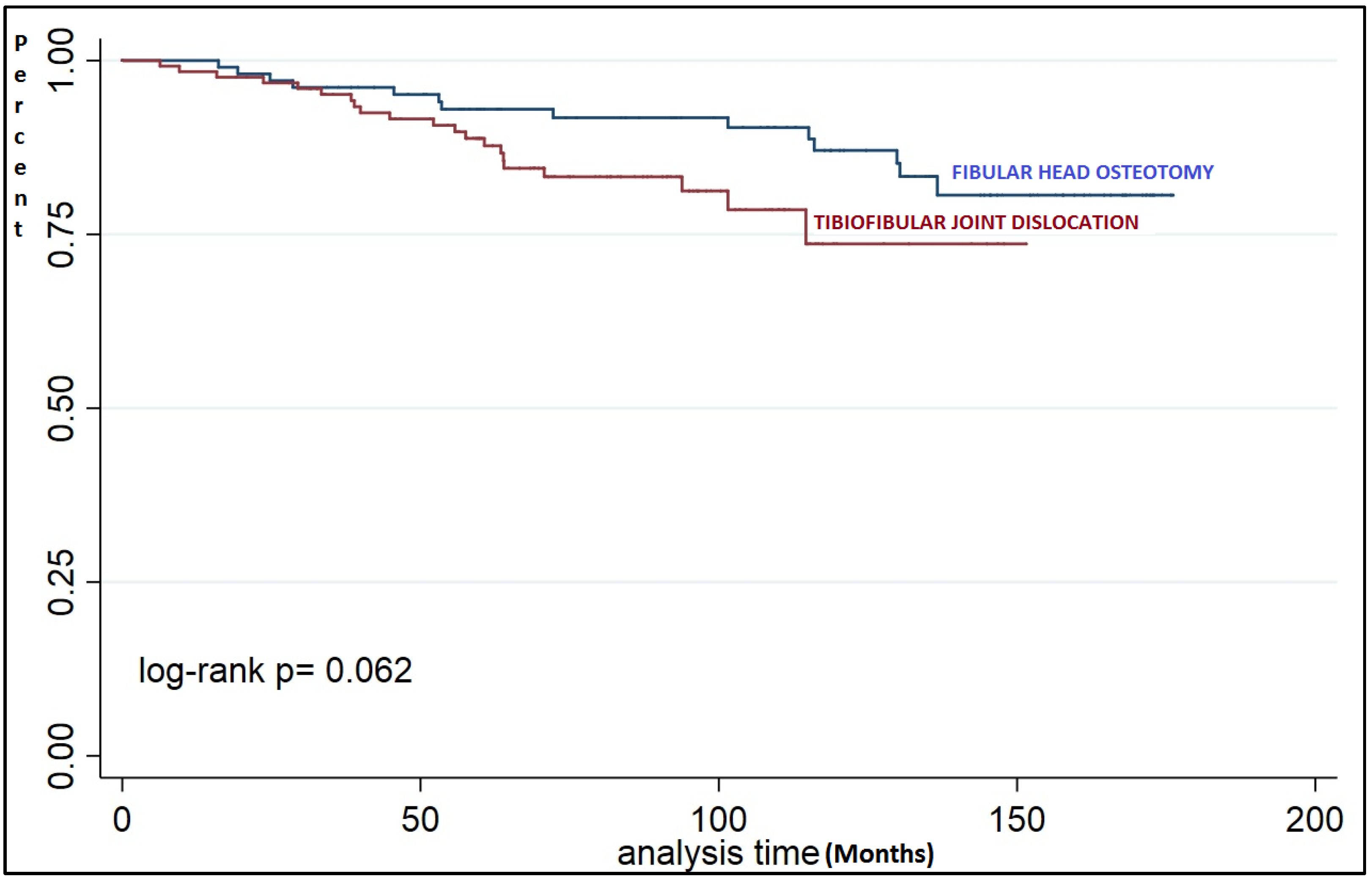
| TKR final FU | 14 (13.3%) | 21 (16.8%) | 0.58 |
| Time to TKR | 74.4 months (SD 45.5) | 61.36 months (SD 28.6) | 0.16 |
| Satisfaction (Likert 1–5) | 3.8 (SD 1.1) | 3.8 (SD 1.2) | 0.97 |
| Would you repeat surgery? (yes/no) | 90/15 (85.7%) | 102/23 (81.6%) | 0.55 |
| Time Follow-Up (Months) | Group 1. FHO (n 105) | Group 2. TFJD (n 125) | p-Value |
|---|---|---|---|
| 24 | 98% | 96.8% | 0.53 |
| 36 | 96.1% | 95.1% | 0.71 |
| 48 | 95.1% | 91.6% | 0.29 |
| 60 | 93% | 88.8% | 0.28 |
| 120 | 87% | 73.6% | 0.07 |
| Title | Group 1. FHO (n 52) | Group 2. TFJD (n 58) | p-Value |
|---|---|---|---|
| KSS R | 86.9 (SD 15.7) | 83.3 (SD 17.4) | 0.4 |
| KSS F | 80.7 (SD 24.8) | 78.1 (SD 20.9) | 0.33 |
| FTA 1y FU | 176.1° (SD 3.7) | 177.1° (SD 2.9) | 0.24 |
| FTA final FU | 175.6° (SD 3.9) | 176.5° (SD 4.2) | 0.48 |
| Ahlbäck 1y FU | 2.11 (SD 0.6) | 2.25 (SD 0.5) | 0.32 |
| Ahlbäck final FU | 2.27 (SD 0.5) | 2.6 (0.5) | 0.04 * |
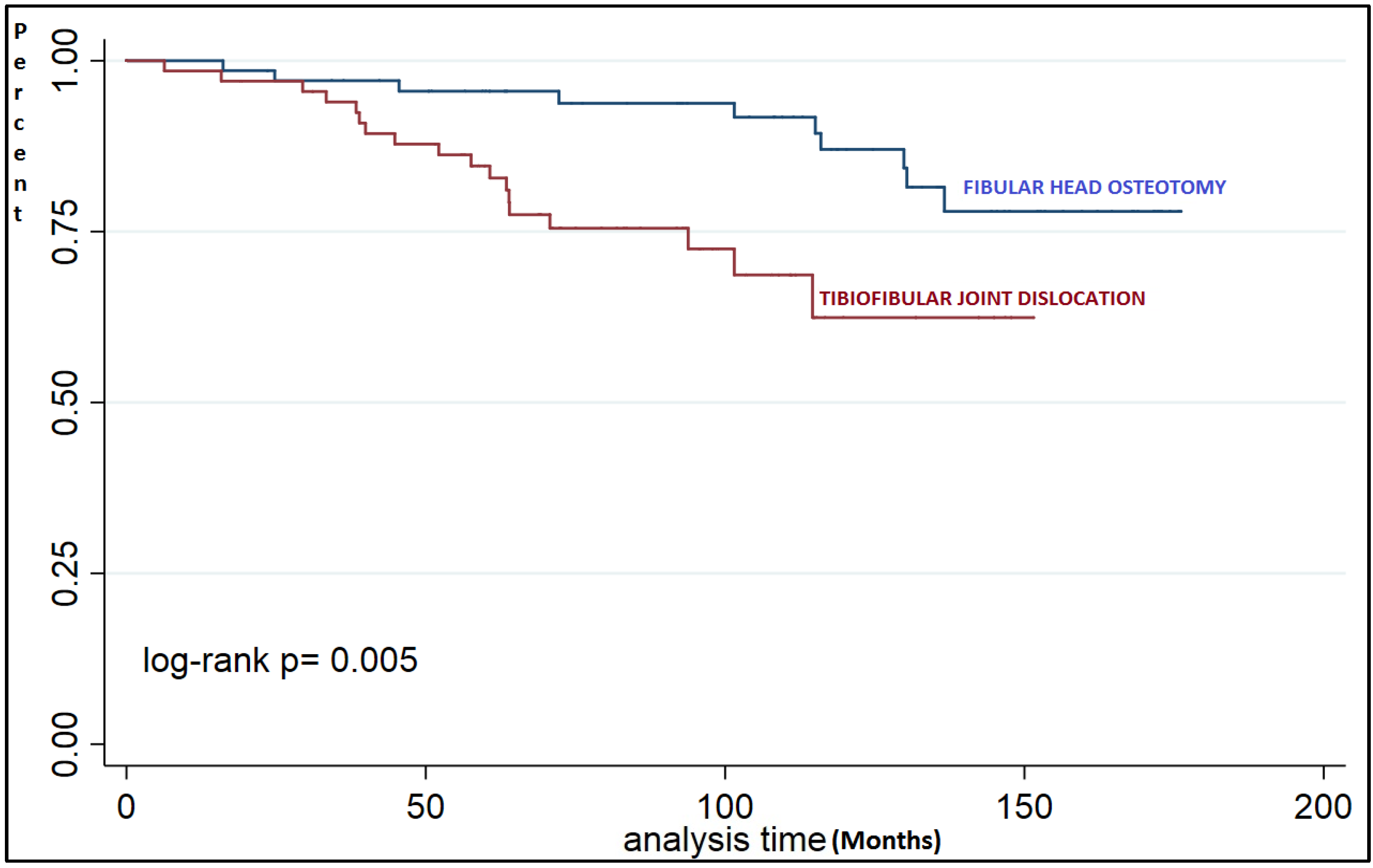
| TKR final FU | 9 (17.3%) | 18 (31%) | 0.04 * |
| Time to TKR (months) | 88.8 (SD 45.7) | 54.9 (SD 28.3) | 0.03 * |
| Satisfaction (Likert 1–5) | 3.9 (SD 1.1) | 3.7 (SD 1.3) | 0.67 |
| Would you repeat surgery? (yes/no) | 58/12 (82.8%) | 55/12 (82%) | 0.59 |
| Time Follow-Up (Months) | Group 1. FHO (n 52) | Group 2. TFJD (n 58) | p-Value |
|---|---|---|---|
| 24 | 98.5 | 97 | 0.54 |
| 36 | 97 | 93.9 | 0.38 |
| 48 | 95.5 | 87.8 | 0.14 |
| 60 | 95.5 | 84.6 | 0.03 |
| 120 | 82.6 | 62.4 | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-Soler, J.; Coelho, A.; Torres-Claramunt, R.; Gasol, B.; Fontanellas, A.; Perelli, S.; Hinarejos, P.; Monllau, J.C. Proximal Tibiofibular Dislocation in Closing-Wedge High Tibial Osteotomy Increases the Risk of Medium and Long-Term Total Knee Replacement. J. Clin. Med. 2021, 10, 2743. https://doi.org/10.3390/jcm10132743
Sánchez-Soler J, Coelho A, Torres-Claramunt R, Gasol B, Fontanellas A, Perelli S, Hinarejos P, Monllau JC. Proximal Tibiofibular Dislocation in Closing-Wedge High Tibial Osteotomy Increases the Risk of Medium and Long-Term Total Knee Replacement. Journal of Clinical Medicine. 2021; 10(13):2743. https://doi.org/10.3390/jcm10132743
Chicago/Turabian StyleSánchez-Soler, Juan, Alex Coelho, Raúl Torres-Claramunt, Berta Gasol, Albert Fontanellas, Simone Perelli, Pedro Hinarejos, and Joan Carles Monllau. 2021. "Proximal Tibiofibular Dislocation in Closing-Wedge High Tibial Osteotomy Increases the Risk of Medium and Long-Term Total Knee Replacement" Journal of Clinical Medicine 10, no. 13: 2743. https://doi.org/10.3390/jcm10132743
APA StyleSánchez-Soler, J., Coelho, A., Torres-Claramunt, R., Gasol, B., Fontanellas, A., Perelli, S., Hinarejos, P., & Monllau, J. C. (2021). Proximal Tibiofibular Dislocation in Closing-Wedge High Tibial Osteotomy Increases the Risk of Medium and Long-Term Total Knee Replacement. Journal of Clinical Medicine, 10(13), 2743. https://doi.org/10.3390/jcm10132743