
Swiss National Registry on Catheter Ablation Procedures: Changing Trends over the Last 20 Years

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
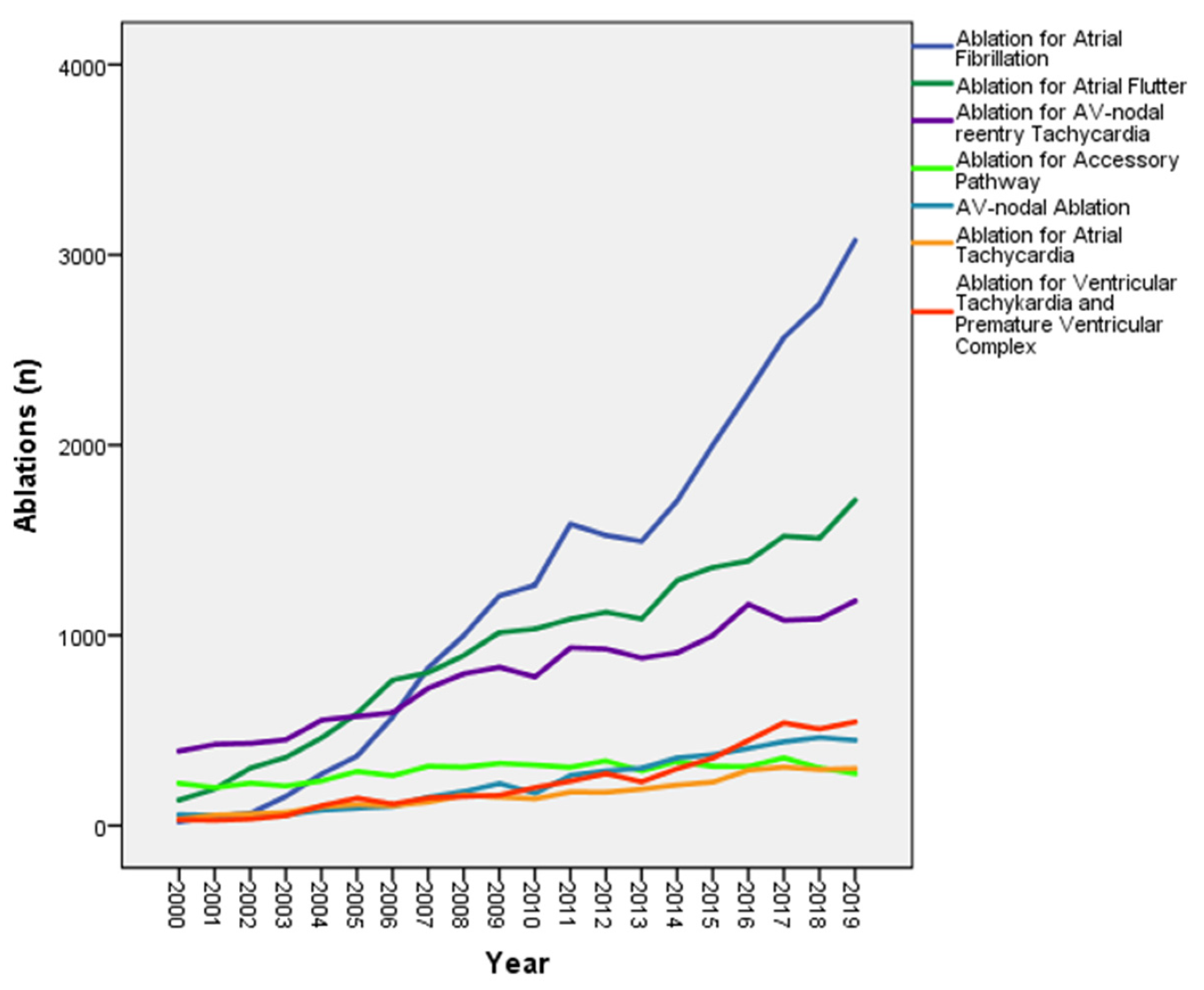
3.1. Ablation Indications
3.2. Concomitant Heart Disease
3.3. Age and Gender Distribution
3.4. Ablation Energy
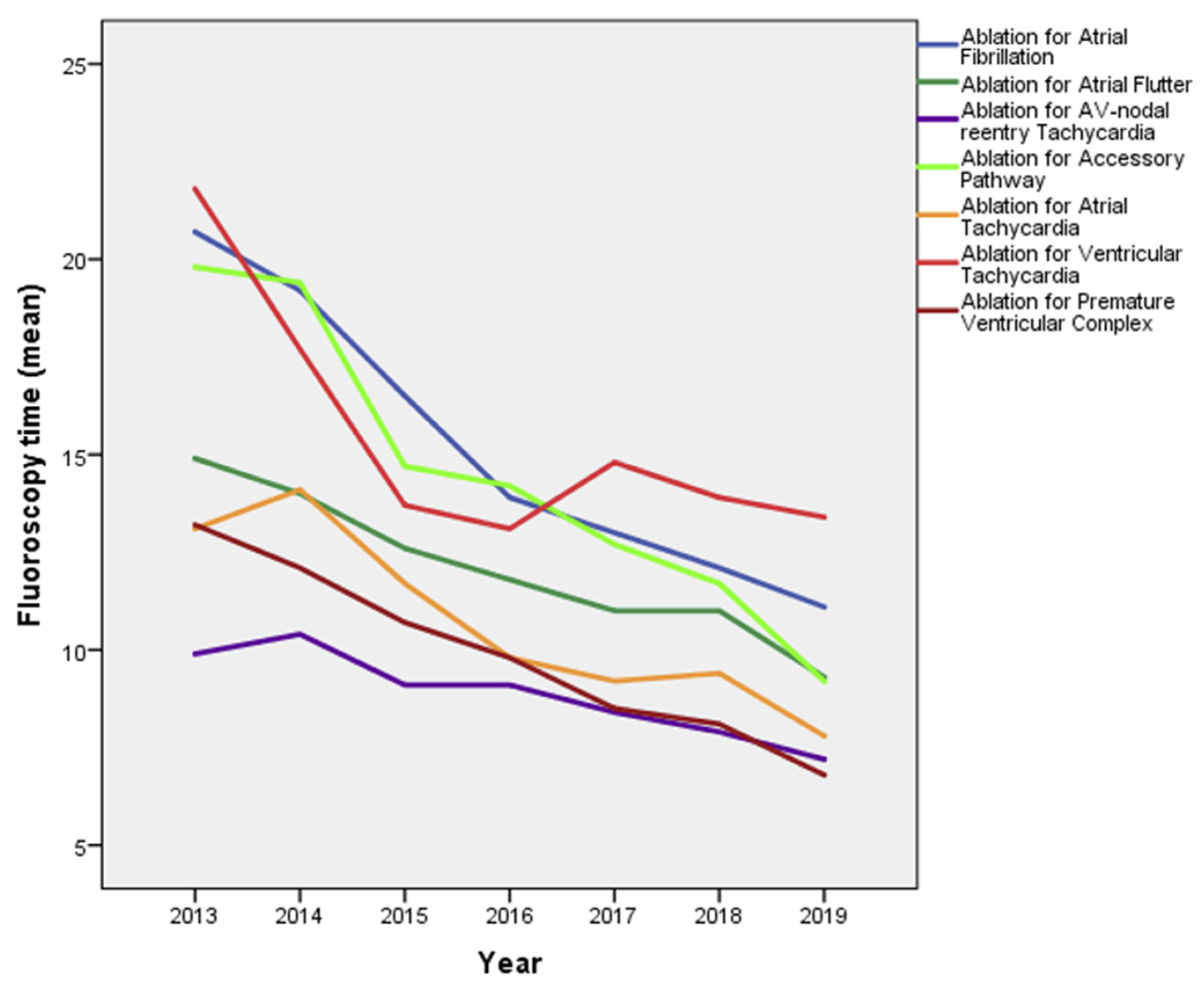
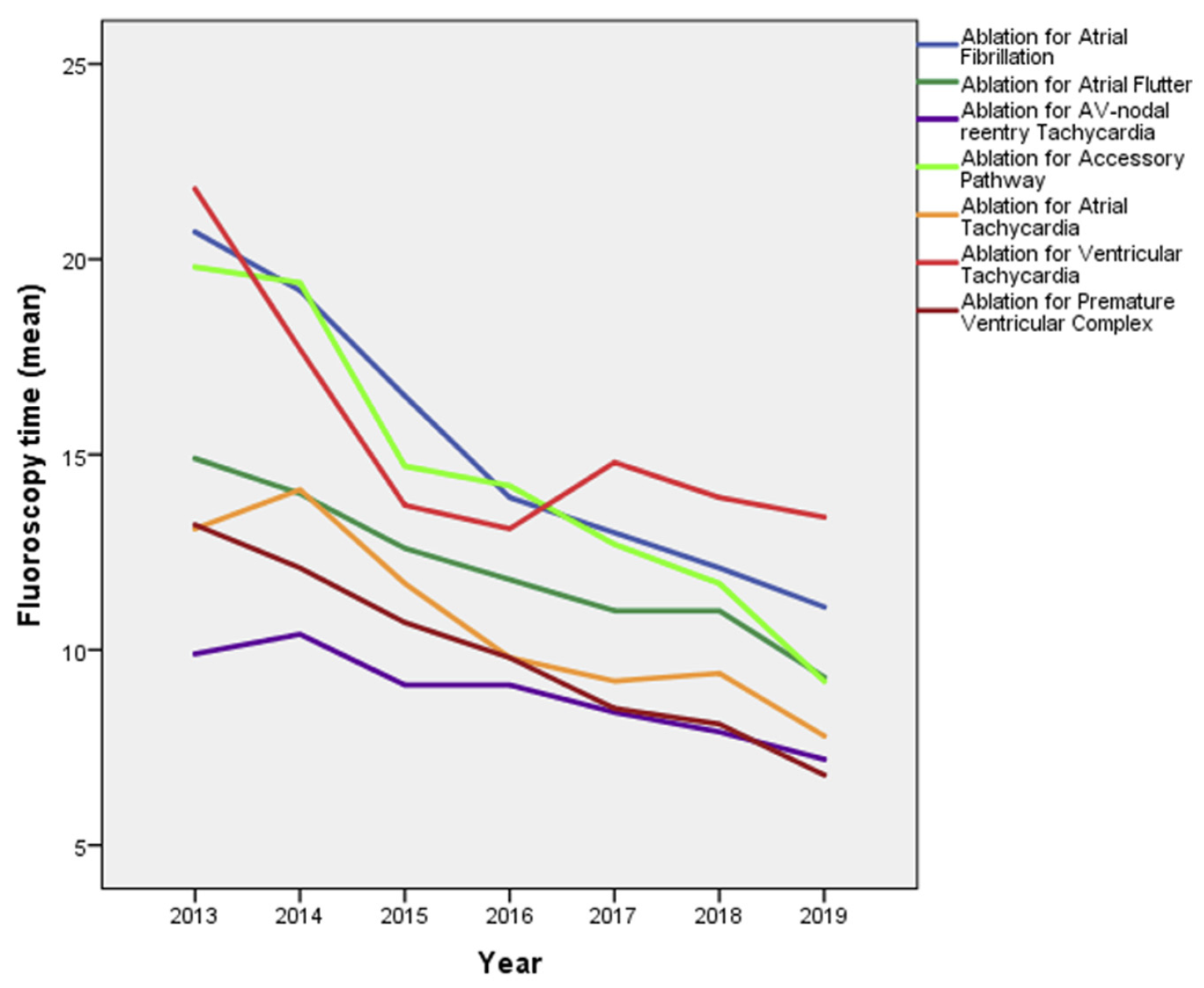
3.5. Fluoroscopy, Ablation and Procedure Durations, 3D Mapping System
3.6. Acute Procedural Success Rates
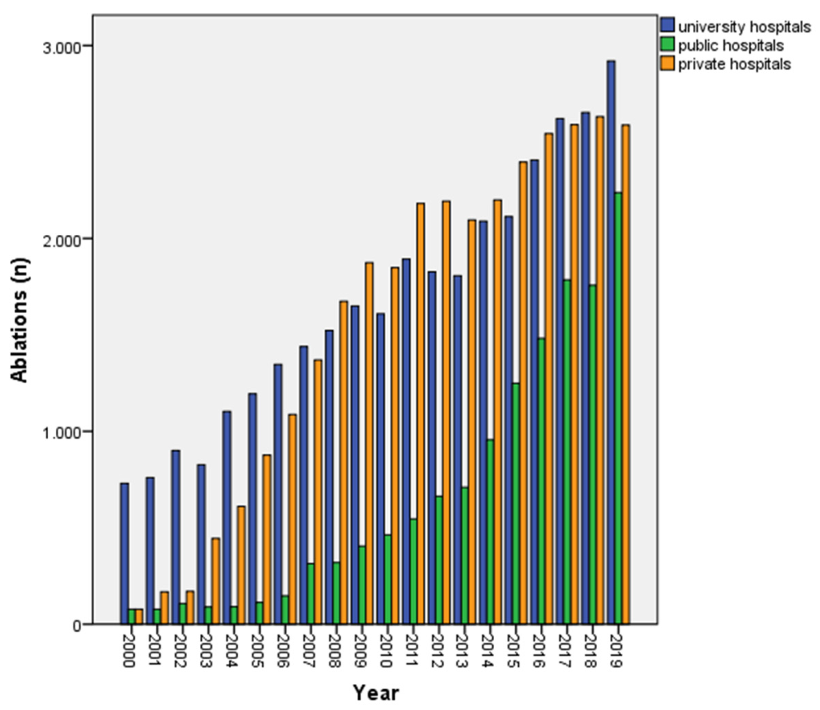
3.7. Location and Type of Ablation Centers
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Holmqvist, F.; Kesek, M.; Englund, A.; Blomström-Lundqvist, C.; Karlsson, L.O.; Kennebäck, G.; Poçi, D.; Samo-Ayou, R.; Sigurjónsdóttir, R.; Ringborn, M.; et al. A decade of catheter ablation of cardiac arrhythmias in Sweden: Ablation practices and outcomes. Eur. Heart J. 2019, 40, 820–830. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pallisgaard, J.L.; Gislason, G.H.; Hansen, J.; Johannessen, A.; Torp-Pedersen, C.; Rasmussen, P.V.; Hansen, M.L. Temporal trends in atrial fibrillation recurrence rates after ablation between 2005 and 2014: A nationwide Danish cohort study. Eur. Heart J. 2018, 39, 442–449. [Google Scholar] [CrossRef]
- Schnabel, R.B.; Yin, X.; Gona, P.; Larson, M.G.; Beiser, A.S.; McManus, D.D.; Newton-Cheh, C.; Lubitz, S.A.; Magnani, J.W.; Ellinor, P.T.; et al. 50 year trends in atrial fibrillation prevalence, incidence, risk factors, and mortality in the Framingham Heart Study: A cohort study. Lancet 2015, 386, 154–162. [Google Scholar] [CrossRef] [Green Version]
- Brugada, J.; Katritsis, D.G.; Arbelo, E.; Arribas, F.; Bax, J.J.; Blomstrom-Lundqvist, C.; Calkins, H.; Corrado, D.; Deftereos, S.G.; Diller, G.P.; et al. 2019 ESC Guidelines for the management of patients with supraventricular tachycardiaThe Task Force for the management of patients with supraventricular tachycardia of the European Society of Cardiology (ESC). Eur. Heart J. 2020, 41, 655–720. [Google Scholar] [CrossRef] [Green Version]
- Hindricks, G.; Potpara, T.; Dagres, N.; Arbelo, E.; Bax, J.J.; Blomström-Lundqvist, C.; Boriani, G.; Castella, M.; Dan, G.A.; Dilaveris, P.E.; et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2020, 42, 373–498. [Google Scholar] [CrossRef]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castella, M.; Diener, H.C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [Green Version]
- Kirchhof, P.; Camm, A.J.; Goette, A.; Brandes, A.; Eckardt, L.; Elvan, A.; Fetsch, T.; Van Gelder, I.C.; Haase, D.; Haegeli, L.M.; et al. Early Rhythm-Control Therapy in Patients with Atrial Fibrillation. N. Engl. J. Med. 2020, 383, 1305–1316. [Google Scholar] [CrossRef]
- Brachmann, J.; Lewalter, T.; Kuck, K.H.; Andresen, D.; Willems, S.; Spitzer, S.G.; Straube, F.; Schumacher, B.; Eckardt, L.; Danilovic, D.; et al. Long-termsymptom improvement and patient satisfaction following catheter ablation of supraventricular tachycardia: Insights from the German ablation registry. Eur. Heart J. 2017, 38, 1317–1326. [Google Scholar] [CrossRef]
- Latchamsetty, R.; Yokokawa, M.; Morady, F.; Kim, H.M.; Mathew, S.; Tilz, R.; Kuck, K.-H.; Nagashima, K.; Tedrow, U.; Stevenson, W.G.; et al. Multicenter outcomes for catheter ablation of idiopathic premature ventricular complexes. JACC Clin. Electrophysiol. 2015, 1, 116–123. [Google Scholar] [CrossRef]
- Santangeli, P.; Frankel, D.S.; Marchlinski, F.E. Advances in Arrhythmia and Electrophysiology End Points for Ablation of Scar-Related Ventricular Tachycardia. Circulation 2014, 7, 949–960. [Google Scholar]
- Ghanbari, H.; Baser, K.; Yokokawa, M.; Stevenson, W.; Della Bella, P.; Vergara, P.; Deneke, T.; Kuck, K.H.; Kottkamp, H.; Fei, S.; et al. Noninducibility in Postinfarction Ventricular Tachycardia as an End Point for Ventricular Tachycardia Ablation and Its Effects on Outcomes. Circulation 2014, 7, 677–683. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanner, H.; Hindricks, G.; Volkmer, M.; Furniss, S.; Kühlkamp, V.; Lacroix, D.; De Chillou, C.; Almendral, J.; Caponi, D.; Kuck, K.-H.; et al. Catheter Ablation of Recurrent Scar-Related Ventricular Tachycardia Using Electroanatomical Mapping and Irrigated Ablation Technology: Results of the Prospective Multicenter Euro-VT-Study. J. Cardiovasc. Electrophysiol. 2009, 21, 47–53. [Google Scholar] [CrossRef]
- Calkins, H.; Epstein, A.; Packer, D.; Arria, A.; Hummel, J.; Gilligan, D.M.; Trusso, J.; Carlson, M.; Luceri, R.; Kopelman, H.; et al. Catheter Ablation of Ventricular Tachycardia in Patients With Structural Heart Disease Using Cooled Radiofrequency Energy Results of a Prospective Multicenter Study. J. Am. Coll. Cardiol. 2000, 35, 1905–1914. [Google Scholar] [CrossRef] [Green Version]
- Stevenson, W.G.; Wilber, D.J.; Natale, A.; Jackman, W.M.; Marchlinski, F.E.; Talbert, T.; Gonzalez, M.D.; Worley, S.J.; Daoud, E.G.; Hwang, C.; et al. Irrigated Radiofrequency Catheter Ablation Guided by Electroanatomic Mapping for Recurrent Ventricular. Circulation 2008, 118, 2773–2782. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kuck, K.H.; Schaumann, A.; Eckardt, L.; Willems, S.; Ventura, R.; Delacrétaz, E.; Pitschner, H.F.; Kautzner, J.; Schumacher, B.; Hansen, P.S.; et al. Catheter ablation of stable ventricular tachycardia before defi brillator implantation in patients with coronary heart disease (VTACH): A multicentre randomised controlled trial. Lancet 2010, 375, 31–40. [Google Scholar] [CrossRef]
- Quesada, A.; Cózar, R.; Anguera, I. Spanish Catheter Ablation Registry. 19th Official Report of the Heart Rhythm Association of the Spanish Society of Cardiology (2019). Rev. Española Cardiol. 2020, 73, 1049–1060. [Google Scholar] [CrossRef] [PubMed]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter ablation for atrial fibrillation with heart failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef] [PubMed]
- Curley, M.; Berger, M.; Roth, J.; Benjamin, I.; Rubenstein, J. Predictors of Mortality and Major In-Hospital Adverse Events Associated With Electrophysiology Catheter Ablation. JAMA Intern. Med. 2014, 174, 815–817. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bohnen, M.; Stevenson, W.G.; Tedrow, U.B.; Michaud, G.F.; John, R.M.; Epstein, L.M.; Albert, C.M.; Koplan, B.A. Incidence and predictors of major complications from contemporary catheter ablation to treat cardiac arrhythmias. Heart Rhythm. 2011, 8, 1661–1666. [Google Scholar] [CrossRef] [PubMed]
- Suenari, K.; Hu, Y.F.; Tsao, H.M.; Tai, C.T.; Chiang, C.E.; Lin, Y.J.; Chang, S.L.; Lo, L.W.; Ta-Chuan, T.U.A.N.; Lee, P.C.; et al. Gender Differences in the Clinical Characteristics and Atrioventricular Nodal Conduction Properties in Patients With Atrioventricular Nodal Reentrant Tachycardia. J. Cardiovasc. Electrophysiol. 2010, 21, 1114–1119. [Google Scholar] [CrossRef] [PubMed]
- Porter, M.J.; Morton, J.B.; Denman, R.; Lin, A.C.; Tierney, S.; Santucci, P.A.; Cai, J.J.; Madsen, N.; Wilber, D.J. Influence of age and gender on the mechanism of supraventricular tachycardia. Heart Rhythm. 2004, 1, 393–396. [Google Scholar] [CrossRef] [PubMed]
- Go, A.S.; Hylek, E.M.; Phillips, K.A.; Chang, Y.; Henault, L.E.; Selby, J.V.; Singer, D.E. Prevalence of Diagnosed Atrial Fibrillation in Adults. JAMA 2001, 285, 2370. [Google Scholar] [CrossRef]
- Patel, N.; Deshmukh, A.; Thakkar, B.; Coffey, J.O.; Agnihotri, K.; Patel, A.; Ainani, N.; Nalluri, N.; Patel, N.; Patel, N.; et al. Gender, Race, and Health Insurance Status in Patients Undergoing Catheter Ablation for Atrial Fibrillation. Am. J. Cardiol. 2016, 117, 1117–1126. [Google Scholar] [CrossRef]
- Patel, D.; Mohanty, P.; Di Biase, L.; Sanchez, J.E.; Shaheen, M.H.; Burkhardt, J.D.; Bassouni, M.; Cummings, J.; Wang, Y.; Lewis, W.R.; et al. Outcomes and complications of catheter ablation for atrial fibrillation in females. Heart Rhythm. 2010, 7, 167–172. [Google Scholar] [CrossRef]
- Verma, A.; Jiang, C.-Y.; Betts, T.R.; Chen, J.; Deisenhofer, I.; Mantovan, R.; Macle, L.; Morillo, C.A.; Haverkamp, W.; Weerasooriya, R.; et al. Approaches to Catheter Ablation for Persistent Atrial Fibrillation. N. Engl. J. Med. 2015, 372, 1812–1822. [Google Scholar] [CrossRef] [PubMed]
- Zylla, M.M.; Brachmann, J.; Lewalter, T.; Hoffmann, E.; Kuck, K.-H.; Andresen, D.; Willems, S.; Eckardt, L.; Tebbenjohanns, J.; Spitzer, S.G.; et al. Sex-related outcome of atrial fibrillation ablation: Insights from the German Ablation Registry. Heart Rhythm. 2016, 13, 1837–1844. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Year | Number of Ablations (Absolute Numbers) | Number of Ablations per 100,000 Inhabitants |
|---|---|---|
| 2019 | 7745 | 90.37 |
| 2018 | 7041 | 82.40 |
| 2017 | 6996 | 82.46 |
| 2016 | 6431 | 76.38 |
| 2015 | 5758 | 69.15 |
| 2014 | 5244 | 63.66 |
| 2013 | 4612 | 56.66 |
| 2012 | 4683 | 58.25 |
| 2011 | 4620 | 58.08 |
| 2010 | 3920 | 49.81 |
| 2009 | 3929 | 50.46 |
| 2008 | 3517 | 45.66 |
| 2007 | 3123 | 41.13 |
| 2006 | 2581 | 34.37 |
| 2005 | 2185 | 29.29 |
| 2004 | 1805 | 24.34 |
| 2003 | 1362 | 18.50 |
| 2002 | 1178 | 16.11 |
| 2001 | 1006 | 13.86 |
| 2000 | 886 | 12.30 |
| Type of Ablation | Male Age Mean (SD) | Female Age Mean (SD) | Difference of Mean Age between Sexes (p-Value) | Male N (%) | Female N (%) | All Ablations Single and Combined Investigations (n) | Ablation Single Approach (n) | Ablation Using Cryo-Energy (n) | Redo- Intervention N (%) | Without CM N (%) | Acute Success (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| AF | 61 (+/− 0.8) | 65.7 (+/− 1.1) | <0.001 | 8515 (69.3) | 3769 (30.7) | 15,859 | 12,365 | 1754 | 3007 (24.3) | 8023 (64.9) | 99.17 |
| AFL | 67 (+/− 0.8) | 68.4 (+/− 1.1) | 0.025 | 5158 (78.6) | 1406 (21.4) | 9863 | 6582 | 21 | 546 (8.3) | 3147 (47.8) | 96.82 |
| AVNRT | 58 (+/− 1.6) | 54 (+/− 1.1) | 0.001 | 3013 (44.4) | 3780 (55.6) | 7295 | 6809 | 19 | 387 (5.7) | 5858 (86.0) | 98.93 |
| AP | 35.7 (+/− 1.3) | 39.6 (+/− 1.5) | 0.001 | 1256 (62.0) | 796 (38.0) | 2177 | 2060 | 29 | 302 (14.7) | 1938 (94.0) | 92.51 |
| AT | 58 (+/− 2.6) | 58 (+/− 2.3) | 0.906 | 596 (46.7) | 679 (53.3) | 1825 | 1280 | 0 | 204 (15.9) | 855 (66.8) | 86.31 |
| AVN | 74.1 (+/− 1.5) | 77.6 (+/− 0.8) | <0.001 | 1254 (48.2) | 1350 (51.8) | 2789 | 2617 | 0 | 144 (5.5) | 683 (26.1) | - |
| VT | 63.6 (+/− 1.5) | 55.4 (+/− 3.0) | <0.001 | 1155 (78.5) | 316 (21.5) | 1561 | 1489 | 0 | 364 (24.4) | 407 (27.3) | 48.75 |
| PVC | 58 (+/− 1.5) | 51 (+/− 2.4) | <0.001 | 740 (58.0) | 535 (42.0) | 1361 | 1286 | 0 | 159 (12.4) | 781 (60.7) | 85.28 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Molitor, N.; Yalcinkaya, E.; Auricchio, A.; Burri, H.; Delacretaz, E.; Kühne, M.; Menafoglio, A.; Reek, S.; Reichlin, T.; Herrera-Siklody, C.; et al. Swiss National Registry on Catheter Ablation Procedures: Changing Trends over the Last 20 Years. J. Clin. Med. 2021, 10, 3021. https://doi.org/10.3390/jcm10143021
Molitor N, Yalcinkaya E, Auricchio A, Burri H, Delacretaz E, Kühne M, Menafoglio A, Reek S, Reichlin T, Herrera-Siklody C, et al. Swiss National Registry on Catheter Ablation Procedures: Changing Trends over the Last 20 Years. Journal of Clinical Medicine. 2021; 10(14):3021. https://doi.org/10.3390/jcm10143021
Chicago/Turabian StyleMolitor, Nadine, Emre Yalcinkaya, Angelo Auricchio, Haran Burri, Etienne Delacretaz, Michael Kühne, Andrea Menafoglio, Sven Reek, Tobias Reichlin, Claudia Herrera-Siklody, and et al. 2021. "Swiss National Registry on Catheter Ablation Procedures: Changing Trends over the Last 20 Years" Journal of Clinical Medicine 10, no. 14: 3021. https://doi.org/10.3390/jcm10143021
APA StyleMolitor, N., Yalcinkaya, E., Auricchio, A., Burri, H., Delacretaz, E., Kühne, M., Menafoglio, A., Reek, S., Reichlin, T., Herrera-Siklody, C., Zimmerli, M., Sticherling, C., & Duru, F. (2021). Swiss National Registry on Catheter Ablation Procedures: Changing Trends over the Last 20 Years. Journal of Clinical Medicine, 10(14), 3021. https://doi.org/10.3390/jcm10143021