
The Impact of Age on Mortality in Chronic Haemodialysis Population with COVID-19

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
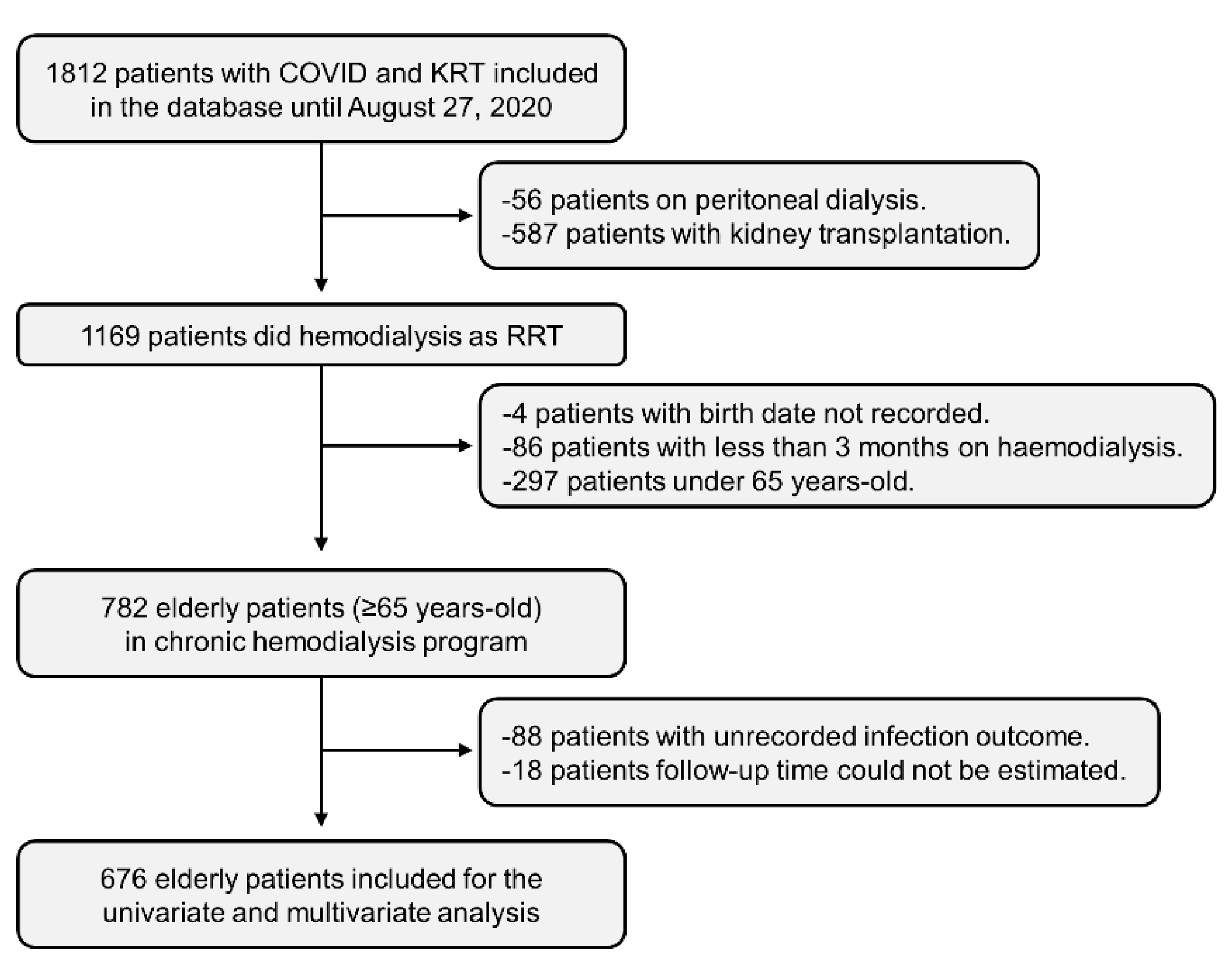
2.1. Data Source
2.2. Data Collection
2.3. Statistical Analysis
3. Results
3.1. Differences between Elderly and Non-Elderly Haemodialysis Populations
3.2. Mortality in Haemodialysis Patients
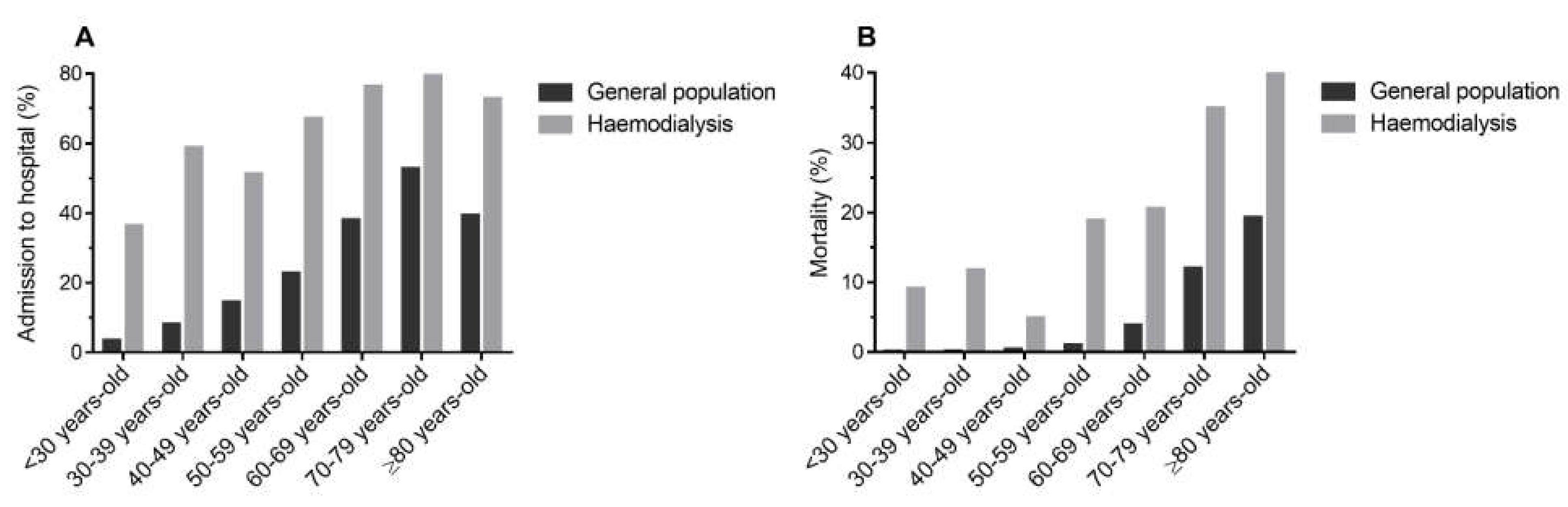
3.3. Mortality Compared to the General Population
3.4. Mortality Risk Factors in the Elderly Haemodialysis Population
3.5. Treatment of COVID-19 in the Elderly Haemodialysis Population
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. COVID-19 Weekly Epidemiological Update. 15 June 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---15-june-2021 (accessed on 21 June 2021).
- Petrilli, C.M.; Jones, S.A.; Yang, J.; Rajagopalan, H.; O’Donnell, L.; Chernyak, Y.; Tobin, K.A.; Cerfolio, R.J.; Francois, F.; Horwitz, L.I. Factors associated with hospital admission and critical illness among 5279 people with coronavirus disease 2019 in New York City: Prospective cohort study. BMJ 2020, 369. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Cheng, Y.; Luo, R.; Wang, K.; Zhang, M.; Wang, Z.; Dong, L.; Li, J.; Yao, Y.; Ge, S.; Xu, G. Kidney disease is associated with in-hospital death of patients with COVID-19. Kidney Int. 2020, 97, 829–838. [Google Scholar] [CrossRef]
- Palaiodimos, L.; Kokkinidis, D.G.; Li, W.; Karamanis, D.; Ognibene, J.; Arora, S.; Southern, W.N.; Mantzoros, C.S. Severe obesity is associated with higher in-hospital mortality in a cohort of patients with COVID-19 in the Bronx, New York. Metabolism 2020, 108. [Google Scholar] [CrossRef] [PubMed]
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. OpenSAFELY: Factors associated with COVID-19 death in 17 million patients. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Registro Español de Enfermos Renales (REER) Informe de Diálisis y Trasplante 2019. Available online: https://www.senefro.org/contents/webstructure/INFORME_REER_SEN_2020_WEB_SEN.pdf (accessed on 31 December 2020).
- REER Registro Español de Enfermos Renales. Available online: http://www.registrorenal.es/ (accessed on 30 December 2020).
- Sánchez-Álvarez, J.E.; Pérez Fontán, M.; Jiménez Martín, C.; Blasco Pelícano, M.; Cabezas Reina, C.J.; Sevillano Prieto, Á.M.; Melilli, E.; Crespo Barrios, M.; Macía Heras, M.; del Pino y Pino, M.D. Situación de la infección por SARS-CoV-2 en pacientes en tratamiento renal sustitutivo. Informe del Registro COVID-19 de la Sociedad Española de Nefrología (SEN). Nefrología 2020, 40, 272–278. [Google Scholar] [CrossRef] [PubMed]
- Red Nacional de Vigilancia Epidemiológica. Informe COVID-19 No33. Ministerio de Ciencia e Innovación. 2020. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/INFORMES/Informes%20COVID-19/Informe%20n%c2%ba%2033.%20An%c3%a1lisis%20de%20los%20casos%20de%20COVID-19%20hasta%20el%2010%20de%20mayo%20en%20Espa%c3%b1a%20a%2029%20de%20mayo%20de%202020.pdf (accessed on 1 July 2021).
- Red Nacional de Vigilancia Epidemiológica. Informe COVID-19 No41. Ministerio de Ciencia e Innovación. 2020. Available online: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/INFORMES/Informes%20COVID-19/Informe%20COVID-19.%20N%c2%ba%2041_27agosto2020_ISCIII.pdf (accessed on 1 July 2021).
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Valeri, A.M.; Robbins-Juarez, S.Y.; Stevens, J.S.; Ahn, W.; Rao, M.K.; Radhakrishnan, J.; Gharavi, A.G.; Mohan, S.; Husain, S.A. Presentation and Outcomes of Patients with ESKD and COVID-19. J. Am. Soc. Nephrol. 2020, 31, ASN.2020040470. [Google Scholar] [CrossRef]
- Hilbrands, L.B.; Duivenvoorden, R.; Vart, P.; Franssen, C.F.M.; Hemmelder, M.H.; Jager, K.J.; Kieneker, L.M.; Noordzij, M.; Pena, M.J.; de Vries, H.; et al. COVID-19-related mortality in kidney transplant and dialysis patients: Results of the ERACODA collaboration. Nephrol. Dial. Transplant. 2020, 35, 1973–1983. [Google Scholar] [CrossRef] [PubMed]
- Jager, K.J.; Kramer, A.; Chesnaye, N.C.; Couchoud, C.; Sánchez-Álvarez, J.E.; Garneata, L.; Collart, F.; Hemmelder, M.H.; Ambühl, P.; Kerschbaum, J.; et al. Results from the ERA-EDTA Registry indicate a high mortality due to COVID-19 in dialysis patients and kidney transplant recipients across Europe. Kidney Int. 2020, 98. [Google Scholar] [CrossRef] [PubMed]
- Gansevoort, R.T.; Hilbrands, L.B. CKD is a key risk factor for COVID-19 mortality. Nat. Rev. Nephrol. 2020, 16, 705–706. [Google Scholar] [CrossRef]
- Goicoechea, M.; Sánchez Cámara, L.A.; Macías, N.; Muñoz de Morales, A.; Rojas, Á.G.; Bascuñana, A.; Arroyo, D.; Vega, A.; Abad, S.; Verde, E.; et al. COVID-19: Clinical course and outcomes of 36 hemodialysis patients in Spain. Kidney Int. 2020, 98, 27–34. [Google Scholar] [CrossRef] [PubMed]
- Anguiano, L.; Riera, M.; Pascual, J.; Valdivielso, J.M.; Barrios, C.; Betriu, A.; Mojal, S.; Fernández, E.; Soler, M.J.; Faura, A.; et al. Circulating angiotensin-converting enzyme 2 activity in patients with chronic kidney disease without previous history of cardiovascular disease. Nephrol. Dial. Transplant. 2015, 30, 1176–1185. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crespo, M.; Mazuecos, A.; Rodrigo, E.; Gavela, E.; Villanego, F.; Sánchez-Alvarez, E.; González-Monte, E.; Jiménez-Martín, C.; Melilli, E.; Diekman, F.; et al. Respiratory and Gastrointestinal COVID-19 Phenotypes in Kidney Transplant Recipients. Transplantation 2020, 104, 2225–2233. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Murthy, S.; Diaz, J.V.; Slutsky, A.S.; Villar, J.; Angus, D.C.; Annane, D.; Azevedo, L.C.P.; Berwanger, O.; Cavalcanti, A.B.; et al. Association between Administration of Systemic Corticosteroids and Mortality among Critically Ill Patients with COVID-19: A Meta-analysis. JAMA J. Am. Med. Assoc. 2020, 324, 1330–1341. [Google Scholar] [CrossRef]
- Ramiro, S.; Mostard, R.L.M.; Magro-Checa, C.; Van Dongen, C.M.P.; Dormans, T.; Buijs, J.; Gronenschild, M.; De Kruif, M.D.; Van Haren, E.H.J.; Van Kraaij, T.; et al. Historically controlled comparison of glucocorticoids with or without tocilizumab versus supportive care only in patients with COVID-19-associated cytokine storm syndrome: Results of the CHIC study. Ann. Rheum. Dis. 2020, 79, 1143–1151. [Google Scholar] [CrossRef] [PubMed]
- Horby, P.; Lim, W.; Emberson, J.; Mafham, M.; Bell, J. Dexamethasone in Hospitalized Patients with Covid-19. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef] [PubMed]
- Hertanto, D.M.; Sutanto, H.; Wungu, C.D.; K. Wungu, C.D.; Mayjen Moestopo No, J. Immunomodulation as a Potent COVID-19 Pharmacotherapy: Past, Present and Future. Preprints 2021. [Google Scholar] [CrossRef]
- Kramer, A.; Pippias, M.; Noordzij, M.; Stel, V.S.; Afentakis, N.; Ambühl, P.M.; Andrusev, A.M.; Fuster, E.A.; Arribas Monzón, F.E.; Åsberg, A.; et al. The European Renal Association—European Dialysis and Transplant Association (ERA-EDTA) Registry Annual Report 2015: A summary. Clin. Kidney J. 2018, 11, 108–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
{kind=link}
{kind=link}
| Variables | <65 Years-Old (n = 254) | ≥65 Years-Old (n = 676) | p-Value |
|---|---|---|---|
| Mean follow-up time (days) | 20 (IQR: 13–30) | 16 (IQR: 8–28) | NA |
| Age | 53.5 ± 10.7 | 78.3 ± 7.2 | <0.001 |
| Male sex | 165 (65.0%) | 431 (63.8%) | 0.733 |
| Primary kidney disease: | |||
| Diabetic kidney disease | 69 (27.2%) | 188 (27.8%) | 0.582 |
| Primary glomerular disease | 50 (19.7%) | 68 (10.1%) | <0.001 |
| Interstitial nephropathy | 15 (5.9%) | 40 (5.9%) | 0.643 |
| Polycystic kidney disease | 13 (5.1%) | 22 (3.3%) | 0.294 |
| Nephrosclerosis | 18 (7.1%) | 121 (17.9%) | <0.001 |
| Systemic disease | 8 (3.2%) | 14 (2.1%) | 0.430 |
| Others or unknown | 81 (31.8%) | 223 (32.9%) | NA |
| Time on hemodialysis (years) | 2.4 (IQR: 1.1–5.3) | 3.1 (IQR: 1.5–5.8) | 0.335 |
| Chronic haemodialysis performed in a hospital | 120 (47.2%) | 287 (42.5%) | 0.389 |
| Clinical presentation: | |||
| Asymptomatic | 44 (17.3%) | 90 (13.3%) | 0.087 |
| Fever | 163 (64.2%) | 431 (63.8%) | 0.912 |
| Respiratory symptoms a | 138 (54.3%) | 373 (55.2%) | 0.933 |
| Dyspnea | 72 (28.4%) | 257 (38.0%) | 0.022 |
| Gastrointestinal symptoms b | 42 (16.5%) | 97 (14.4%) | 0.641 |
| Pneumonia | 131 (51.6%) | 435 (64.4%) | <0.001 |
| Lymphopenia | 160 (63.0%) | 481 (71.2%) | 0.002 |
| Hospitalization | 166 (65.4%) | 515 (76.2%) | 0.002 |
| Admission to ICU | 25 (9.8%) | 9 (1.3%) | <0.001 |
| Mechanical ventilation | 27 (10.6%) | 50 (7.4%) | 0.177 |
| Mortality | 40 (15.8%) | 239 (35.4%) | <0.001 |
| Variables | Haemodialysis Population (n = 930) | General Population (n = 438,469) | p-Value |
|---|---|---|---|
| Age | 71.6 ± 13.8 | 50.8 ± 23.5 | <0.001 |
| Male sex | 596 (64.1%) | 201,018 (45.8%) | <0.001 |
| Hospitalization | 681 (74.0%) | 101,277 (23.1%) | <0.001 |
| Admission to ICU | 34 (5.2%) | 8329 (1.9%) | <0.001 |
| Mortality | 279 (30.0%) | 21,325 (4.9%) | <0.001 |
| Variables | Total (n = 676) | Survivors (n = 437) | Non-Survivors (n = 239) | HR (95% CI) | p-Value |
|---|---|---|---|---|---|
| Mean follow-up time (days) | 16 (IQR: 8–28) | 20 (IQR: 14–36) | 7 (IQR: 3–13) | NA | NA |
| Age | 78.3 ± 7.2 | 77.7 ± 7.0 | 79.5 ± 7.4 | 1.35 (1.13–1.62) c | 0.001 |
| Male sex | 431 (63.8%) | 265 (60.6%) | 166 (69.5%) | 1.36 (1.03–1.79) | 0.029 |
| Primary kidney disease: | |||||
| Diabetic kidney disease | 188 (27.8%) | 117 (26.8%) | 71 (29.7%) | 1.44 (1.07–1.94) | 0.016 |
| Primary glomerular disease | 68 (10.1%) | 48 (11.0%) | 20 (8.4%) | 0.87 (0.55–1.39) | 0.566 |
| Interstitial nephropathy | 40 (5.9%) | 34 (7.8%) | 6 (2.5%) | 0.38 (0.17–0.86) | 0.020 |
| Polycystic kidney disease | 22 (3.3%) | 15 (3.4%) | 7 (2.9%) | 0.95 (0.44–2.01) | 0.884 |
| Nephrosclerosis | 121 (17.9%) | 84 (19.2%) | 37 (15.5%) | 0.94 (0.66–1.36) | 0.754 |
| Systemic disease | 14 (2.1%) | 7 (1.6%) | 7 (2.9%) | 1.84 (0.86–3.92) | 0.114 |
| Others or unknown | 223 (32.9%) | 132 (30.2%) | 91 (38.1%) | NA | NA |
| Time on KRT (years) | 3.1 (IQR: 1.5–5.8) | 3.1 (IQR: 1.4–5.6) | 3.1 (IQR: 1.6–6.0) | 1.00 (0.99–1.02) d | 0.838 |
| Chronic haemodialysis performed in a hospital | 287 (42.5%) | 204 (46.7%) | 83 (34.7%) | 0.73 (0.55–0.98) | 0.034 |
| Received treatments prior to infection: | |||||
| Angiotensin converting enzyme inhibitors (ACEi) | 58 (8.6%) | 36 (8.2%) | 22 (9.2%) | 1.16 (0.75–1.80) | 0.501 |
| Angiotensin receptor blockers (ARB) | 84 (12.4%) | 62 (14.2%) | 22 (9.2%) | 0.69 (0.45–1.08) | 0.101 |
| ACEi or ARB | 138 (20.4%) | 95 (21.7%) | 43 (18.0%) | 0.87 (0.62–1.21) | 0.407 |
| Non-steroidal anti-inflammatory drugs | 23 (3.4%) | 16 (3.7%) | 7 (2.9%) | 0.79 (0.37–1.68) | 0.542 |
| Clinical presentation: | |||||
| Asymptomatic | 90 (13.3%) | 82 (18.8%) | 8 (3.4%) | 0.19 (0.09–0.39) | <0.001 |
| Fever | 431 (63.8%) | 253 (57.9%) | 178 (74.5%) | 1.86 (1.36–2.54) | <0.001 |
| Respiratory symptoms a | 373 (55.2%) | 218 (49.9%) | 155 (64.9%) | 1.55 (1.18–2.03) | 0.002 |
| Dyspnea | 257 (38.0%) | 128 (29.3%) | 129 (54.0%) | 2.34 (1.79–3.06) | <0.001 |
| Gastrointestinal symptoms b | 97 (14.4%) | 65 (14.9%) | 32 (13.4%) | 0.87 (0.59–1.26) | 0.451 |
| Pneumonia | 435 (64.4%) | 237 (54.2%) | 198 (82.9%) | 3.96 (2.70–5.82) | <0.001 |
| Lymphopenia | 481 (71.2%) | 281 (64.3%) | 200 (83.7%) | 3.56 (2.27–5.59) | <0.001 |
| Hospitalization | 515 (76.2%) | 291 (66.6%) | 224 (93.7%) | 7.38 (4.12–13.20) | <0.001 |
| Hospitalization days | 11 (IQR: 7–17) | 14 (IQR: 9.5–21.5) | 8 (IQR: 4–12) | 0.60 (0.53–0.68) e | <0.001 |
| Admission to ICU | 9 (1.3%) | 1 (0.2%) | 8 (3.4%) | 2.29 (1.13–4.64) | 0.022 |
| Mechanical ventilation | 50 (7.4%) | 5 (1.1%) | 45 (18.8%) | 3.83 (2.72–5.39) | <0.001 |
| Variable | Model 1 | Model 2 | Model 3 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| HR | 95% CI | p-Value | HR | 95% CI | p-Value | HR | 95% CI | p-Value | |
| Age | 1.59 b | 1.31–1.93 b | <0.001 | 1.87 b | 1.48–2.37 b | <0.001 | 1.48 b | 1.21–1.82 b | <0.001 |
| Male sex | 1.21 | 0.90–1.63 | 0.210 | 1.19 | 0.85–1.66 | 0.324 | 1.16 | 0.84–1.60 | 0.369 |
| Clinical presentation: | |||||||||
| Asymptomatic | 0.96 | 0.39–2.35 | 0.931 | 1.47 | 0.53–4.07 | 0.461 | 1.31 | 0.53–3.26 | 0.562 |
| Fever | 1.16 | 0.81–1.67 | 0.419 | 1.36 | 0.88–2.12 | 0.165 | 1.26 | 0.84–1.90 | 0.263 |
| Respiratory symptoms a | 0.97 | 0.70–1.34 | 0.853 | 0.97 | 0.67–1.42 | 0.881 | 0.92 | 0.65–1.30 | 0.619 |
| Dyspnea | 1.51 | 1.11–2.04 | 0.008 | 1.57 | 1.10–2.25 | 0.013 | 1.63 | 1.17–2.26 | 0.004 |
| Pneumonia | 1.74 | 1.10–2.73 | 0.017 | 1.79 | 1.03–3.11 | 0.040 | 2.32 | 1.38–3.90 | 0.002 |
| Lymphopenia | 1.44 | 0.87–2.38 | 0.155 | 1.58 | 0.84–2.97 | 0.152 | 1.40 | 0.81–2.43 | 0.230 |
| Hospitalization | 4.00 | 1.83–8.70 | <0.001 | 4.43 | 1.77–11.11 | 0.001 | 6.69 | 2.59–17.30 | <0.001 |
| Primary kidney disease: | |||||||||
| Diabetic kidney disease | 1.57 | 0.98–2.53 | 0.063 | ||||||
| Primary glomerular disease | 1.07 | 0.58–2.00 | 0.826 | ||||||
| Interstitial nephropathy | 0.56 | 0.23–1.37 | 0.205 | ||||||
| Polycystic kidney disease | 1.57 | 0.67–3.66 | 0.295 | ||||||
| Nephrosclerosis | 1.03 | 0.61–1.74 | 0.922 | ||||||
| Systemic disease | 2.50 | 1.06–5.94 | 0.035 | ||||||
| Treatments received for infection: | |||||||||
| Lopinavir/Ritonavir | 0.94 | 0.67–1.32 | 0.711 | ||||||
| Hydroxychloroquine | 0.71 | 0.45–1.10 | 0.127 | ||||||
| Interferon beta | 1.56 | 0.82–2.98 | 0.174 | ||||||
| Tocilizumab | 0.87 | 0.42–1.82 | 0.712 | ||||||
| Glucocorticoids | 0.68 | 0.48–0.96 | 0.027 | ||||||
| Azithromycin | 0.85 | 0.62–1.18 | 0.336 | ||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vergara, A.; Molina-Van den Bosch, M.; Toapanta, N.; Villegas, A.; Sánchez-Cámara, L.; Sequera, P.d.; Manrique, J.; Shabaka, A.; Aragoncillo, I.; Ruiz, M.C.; et al. The Impact of Age on Mortality in Chronic Haemodialysis Population with COVID-19. J. Clin. Med. 2021, 10, 3022. https://doi.org/10.3390/jcm10143022
Vergara A, Molina-Van den Bosch M, Toapanta N, Villegas A, Sánchez-Cámara L, Sequera Pd, Manrique J, Shabaka A, Aragoncillo I, Ruiz MC, et al. The Impact of Age on Mortality in Chronic Haemodialysis Population with COVID-19. Journal of Clinical Medicine. 2021; 10(14):3022. https://doi.org/10.3390/jcm10143022
Chicago/Turabian StyleVergara, Ander, Mireia Molina-Van den Bosch, Néstor Toapanta, Andrés Villegas, Luis Sánchez-Cámara, Patricia de Sequera, Joaquín Manrique, Amir Shabaka, Inés Aragoncillo, María Carmen Ruiz, and et al. 2021. "The Impact of Age on Mortality in Chronic Haemodialysis Population with COVID-19" Journal of Clinical Medicine 10, no. 14: 3022. https://doi.org/10.3390/jcm10143022
APA StyleVergara, A., Molina-Van den Bosch, M., Toapanta, N., Villegas, A., Sánchez-Cámara, L., Sequera, P. d., Manrique, J., Shabaka, A., Aragoncillo, I., Ruiz, M. C., Benito, S., Sánchez, E., & Soler, M. J. (2021). The Impact of Age on Mortality in Chronic Haemodialysis Population with COVID-19. Journal of Clinical Medicine, 10(14), 3022. https://doi.org/10.3390/jcm10143022