
Landscape of Preterm Birth Therapeutics and a Path Forward

 ,
,  ,
,
Abstract
1. Introduction
2. Pathophysiology of PTB
3. The Earliest Tocolytic Agents: Betamimetics
4. Oxytocin Antagonism: Hope for Atosiban
- Institutional Review Boards, participants, and physicians have heightened concern when dealing with any drug that has a potential effect on the fetus and on the mother
- Can people give adequate informed consent during active labor?
- No templates of successful study design in tocolytic studies, since the only drugs previously approved by the FDA were approved under standards that are now deemed inadequate
- No tocolytic drug presented to the FDA has consistently shown neonatal benefit in controlled trials
- Lack of standardization for disease risk, severity, and progression for common diagnoses
- Small market: sales for ‘blockbuster drugs’ in the U.S. for 2004 (~$5 billion) versus annual sales for a tocolytic agent, estimated at <$500 million
5. Calcium Channel Blockers (CCBs): Low Cost and Favorable Safety Profile
6. Nonsteroidal Anti-Inflammatory Drugs as Tocolytic Agents: A Short-Term Prostaglandin Blockade
7. Magnesium Sulfate: A Classic Tocolytic, Called into Question
8. Addressing Infection: Trials of Antibiotics to Prevent PTB
9. Progesterone (P4) Analogs
10. Inhibiting Inflammation: Use of Broad-Spectrum Chemokine Inhibitors
11. Targeting the Prostaglandin F2 Alpha Receptor: OBE-022
12. Interleukin-1 Receptor Antagonism: Kineret and Rytvela
13. Nanoparticles
14. Challenges in Therapeutic Development
15. Pathway Forward toward New PTB Therapeutics
16. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Howson, C.P.; Kinney, M.V.; McDougall, L.; Lawn, J.E.; The Born Too Soon Preterm Birth Action Group. Born too soon: Preterm birth matters. Repro. Health 2013, 10 (Suppl. 1), 1–9. [Google Scholar] [CrossRef]
- Blencowe, H.; Cousens, S.; Oestergaard, M.Z.; Chou, D.; Moller, A.B.; Narwal, R.; Adler, A.; Vera Garcia, C.; Rohde, S.; Say, L.; et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: A systematic analysis and implications. Lancet 2012, 379, 2162–2172. [Google Scholar] [CrossRef]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm labor: One syndrome, many causes. Science 2014, 345, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Suman, V.; Luther, E.E. Preterm Labor. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Kramer, M.S.; Demissie, K.; Yang, H.; Platt, R.W.; Sauve, R.; Liston, R. The contribution of mild and moderate preterm birth to infant mortality. Fetal and Infant Health Study Group of the Canadian Perinatal Surveillance System. JAMA 2000, 284, 843–849. [Google Scholar] [CrossRef] [PubMed]
- Behrman, R.E.; Butler, A.S. Preterm Birth: Causes, Consequences, and Prevention; National Academies Press (US): Washington, DC, USA, 2007. [Google Scholar] [CrossRef]
- Vogel, J.P.; Nardin, J.M.; Dowswell, T.; West, H.M.; Oladapo, O.T. Combination of tocolytic agents for inhibiting preterm labour. Cochrane Database Syst. Rev. 2014, CD006169. [Google Scholar] [CrossRef]
- De Heus, R.; Mulder, E.J.; Visser, G.H. Management of preterm labor: Atosiban or nifedipine? Int. J. Womens Health 2010, 2, 137–142. [Google Scholar] [CrossRef]
- Papatsonis, D.N.; Flenady, V.; Liley, H.G. Maintenance therapy with oxytocin antagonists for inhibiting preterm birth after threatened preterm labour. Cochrane Database Syst. Rev. 2013, CD005938. [Google Scholar] [CrossRef]
- Dodd, J.M.; Crowther, C.A.; Middleton, P. Oral betamimetics for maintenance therapy after threatened preterm labour. Cochrane Database Syst. Rev. 2012, 12, CD003927. [Google Scholar] [CrossRef]
- Nanda, K.; Cook, L.A.; Gallo, M.F.; Grimes, D.A. Terbutaline pump maintenance therapy after threatened preterm labor for preventing preterm birth. Cochrane Database Syst. Rev. 2002, CD003933. [Google Scholar] [CrossRef]
- Naik Gaunekar, N.; Raman, P.; Bain, E.; Crowther, C.A. Maintenance therapy with calcium channel blockers for preventing preterm birth after threatened preterm labour. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Han, S.; Crowther, C.A.; Moore, V. Magnesium maintenance therapy for preventing preterm birth after threatened preterm labour. Cochrane Database Syst. Rev. 2013. [Google Scholar] [CrossRef]
- Chawanpaiboon, S.; Vogel, J.P.; Moller, A.B.; Lumbiganon, P.; Petzold, M.; Hogan, D.; Landoulsi, S.; Jampathong, N.; Kongwattanakul, K.; Laopaiboon, M.; et al. Global, regional, and national estimates of levels of preterm birth in 2014: A systematic review and modelling analysis. Lancet Glob. Health 2019, 7, e37–e46. [Google Scholar] [CrossRef]
- Walani, S.R. Global burden of preterm birth. Int. J. Gynaecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef]
- Flenady, V.; Reinebrant, H.E.; Liley, H.G.; Tambimuttu, E.G.; Papatsonis, D.N. Oxytocin receptor antagonists for inhibiting preterm labour. Cochrane Database Syst. Rev. 2014, CD004452. [Google Scholar] [CrossRef]
- Ples, L.; Sima, R.M.; Ricu, A.; Moga, M.A.; Ionescu, A.C. The efficacy of cervical cerclage combined with a pessary for the prevention of spontaneous preterm birth. J. Matern Fetal Neonatal Med. 2019, 1–5. [Google Scholar] [CrossRef]
- Care, A.; Jackson, R.; O’Brien, E.; Leigh, S.; Cornforth, C.; Haycox, A.; Whitworth, M.; Lavender, T.; Alfirevic, Z. Cervical cerclage, pessary, or vaginal progesterone in high-risk pregnant women with short cervix: A randomized feasibility study. J. Matern Fetal Neonatal Med. 2021, 34, 49–57. [Google Scholar] [CrossRef]
- Saccone, G.; Maruotti, G.M.; Giudicepietro, A.; Martinelli, P.; The Italian Preterm Birth Prevention Working Group. Effect of Cervical Pessary on Spontaneous Preterm Birth in Women With Singleton Pregnancies and Short Cervical Length: A Randomized Clinical Trial. JAMA 2017, 318, 2317–2324. [Google Scholar] [CrossRef]
- Adams Waldorf, K.M.; Singh, N.; Mohan, A.R.; Young, R.C.; Ngo, L.; Das, A.; Tsai, J.; Bansal, A.; Paolella, L.; Herbert, B.R.; et al. Uterine overdistention induces preterm labor mediated by inflammation: Observations in pregnant women and nonhuman primates. Am. J. Obstet. Gynecol. 2015, 213, 830.e1–830.e19. [Google Scholar] [CrossRef]
- Lye, S.J.; Mitchell, J.; Nashman, N.; Oldenhof, A.; Ou, R.; Shynlova, O.; Langille, L. Role of mechanical signals in the onset of term and preterm labor. Front. Horm Res. 2001, 27, 165–178. [Google Scholar]
- McLean, M.; Bisits, A.; Davies, J.; Woods, R.; Lowry, P.; Smith, R. A placental clock controlling the length of human pregnancy. Nat. Med. 1995, 1, 460–463. [Google Scholar] [CrossRef]
- Gravett, M.G.; Novy, M.J. Endocrine-immune interactions in pregnant non-human primates with intrauterine infection. Infect. Dis. Obstet. Gynecol. 1997, 5, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Hillier, S.L.; Krohn, M.A.; Kiviat, N.B.; Watts, D.H.; Eschenbach, D.A. Microbiologic causes and neonatal outcomes associated with chorioamnion infection. Am. J. Obstet. Gynecol. 1991, 165, 955–961. [Google Scholar] [CrossRef]
- Hillier, S.L.; Witkin, S.S.; Krohn, M.A.; Watts, D.H.; Kiviat, N.B.; Eschenbach, D.A. The relationship of amniotic fluid cytokines and preterm delivery, amniotic fluid infection, histologic chorioamnionitis, and chorioamnion infection. Obstet. Gynecol. 1993, 81, 941–948. [Google Scholar] [PubMed]
- Romero, R.; Sepulveda, W.; Kenney, J.S.; Archer, L.E.; Allison, A.C.; Sehgal, P.B. Interleukin 6 determination in the detection of microbial invasion of the amniotic cavity. Ciba Found. Symp. 1992, 167, 205–220, discussion 220–203. [Google Scholar]
- Yoon, B.H.; Romero, R.; Kim, C.J.; Jun, J.K.; Gomez, R.; Choi, J.H.; Syn, H.C. Amniotic fluid interleukin-6: A sensitive test for antenatal diagnosis of acute inflammatory lesions of preterm placenta and prediction of perinatal morbidity. Am. J. Obstet. Gynecol. 1995, 172, 960–970. [Google Scholar] [CrossRef]
- Rosen, T.; Kuczynski, E.; O’Neill, L.M.; Funai, E.F.; Lockwood, C.J. Plasma levels of thrombin-antithrombin complexes predict preterm premature rupture of the fetal membranes. J. Matern. Fetal Med. 2001, 10, 297–300. [Google Scholar] [CrossRef]
- Stephenson, C.D.; Lockwood, C.J.; Ma, Y.; Guller, S. Thrombin-dependent regulation of matrix metalloproteinase (MMP)-9 levels in human fetal membranes. J. Matern Fetal Neona 2005, 18, 17–22. [Google Scholar] [CrossRef]
- Chai, M.; Barker, G.; Menon, R.; Lappas, M. Increased oxidative stress in human fetal membranes overlying the cervix from term non-labouring and post labour deliveries. Placenta 2012, 33, 604–610. [Google Scholar] [CrossRef]
- Menon, R.; Fortunato, S.J.; Yu, J.; Milne, G.L.; Sanchez, S.; Drobek, C.O.; Lappas, M.; Taylor, R.N. Cigarette smoke induces oxidative stress and apoptosis in normal term fetal membranes. Placenta 2011, 32, 317–322. [Google Scholar] [CrossRef]
- Menon, R.; Yu, J.; Basanta-Henry, P.; Brou, L.; Berga, S.L.; Fortunato, S.J.; Taylor, R.N. Short fetal leukocyte telomere length and preterm prelabor rupture of the membranes. PLoS ONE 2012, 7, e31136. [Google Scholar] [CrossRef]
- Bredeson, S.; Papaconstantinou, J.; Deford, J.H.; Kechichian, T.; Syed, T.A.; Saade, G.R.; Menon, R. HMGB1 promotes a p38MAPK associated non-infectious inflammatory response pathway in human fetal membranes. PLoS ONE 2014, 9, e113799. [Google Scholar] [CrossRef]
- Menon, R. Oxidative stress damage as a detrimental factor in preterm birth pathology. Front. Immunol. 2014, 5, 567. [Google Scholar] [CrossRef]
- Menon, R.; Behnia, F.; Polettini, J.; Saade, G.R.; Campisi, J.; Velarde, M. Placental membrane aging and HMGB1 signaling associated with human parturition. Aging 2016, 8, 216–230. [Google Scholar] [CrossRef]
- Menon, R.; Boldogh, I.; Hawkins, H.K.; Woodson, M.; Polettini, J.; Syed, T.A.; Fortunato, S.J.; Saade, G.R.; Papaconstantinou, J.; Taylor, R.N. Histological evidence of oxidative stress and premature senescence in preterm premature rupture of the human fetal membranes recapitulated in vitro. Am. J. Pathol 2014, 184, 1740–1751. [Google Scholar] [CrossRef]
- Zhang, G.; Feenstra, B.; Bacelis, J.; Liu, X.; Muglia, L.M.; Juodakis, J.; Miller, D.E.; Litterman, N.; Jiang, P.P.; Russell, L.; et al. Genetic Associations with Gestational Duration and Spontaneous Preterm Birth. N. Engl. J. Med. 2017, 377, 1156–1167. [Google Scholar] [CrossRef]
- Bower, K.M.; Geller, R.J.; Perrin, N.A.; Alhusen, J. Experiences of Racism and Preterm Birth: Findings from a Pregnancy Risk Assessment Monitoring System, 2004 through 2012. Womens Health Issues 2018, 28, 495–501. [Google Scholar] [CrossRef]
- Krieger, N.; Van Wye, G.; Huynh, M.; Waterman, P.D.; Maduro, G.; Li, W.; Gwynn, R.C.; Barbot, O.; Bassett, M.T. Structural Racism, Historical Redlining, and Risk of Preterm Birth in New York City, 2013-2017. Am. J. Public Health 2020, 110, 1046–1053. [Google Scholar] [CrossRef]
- Mendez, D.D.; Hogan, V.K.; Culhane, J.F. Institutional racism, neighborhood factors, stress, and preterm birth. Ethn Health 2014, 19, 479–499. [Google Scholar] [CrossRef]
- Rich-Edwards, J.; Krieger, N.; Majzoub, J.; Zierler, S.; Lieberman, E.; Gillman, M. Maternal experiences of racism and violence as predictors of preterm birth: Rationale and study design. Paediatr. Perinat Epidemiol. 2001, 15 (Suppl. 2), 124–135. [Google Scholar] [CrossRef]
- Slaughter-Acey, J.C.; Sealy-Jefferson, S.; Helmkamp, L.; Caldwell, C.H.; Osypuk, T.L.; Platt, R.W.; Straughen, J.K.; Dailey-Okezie, R.K.; Abeysekara, P.; Misra, D.P. Racism in the form of micro aggressions and the risk of preterm birth among black women. Ann. Epidemiol. 2016, 26, 7–13.e11. [Google Scholar] [CrossRef]
- Cappelletti, M.; Della Bella, S.; Ferrazzi, E.; Mavilio, D.; Divanovic, S. Inflammation and preterm birth. J. Leukoc Biol. 2016, 99, 67–78. [Google Scholar] [CrossRef]
- Kemp, M.W. Preterm birth, intrauterine infection, and fetal inflammation. Front. Immunol. 2014, 5, 574. [Google Scholar] [CrossRef]
- Fortunato, S.J.; Menon, R.P.; Swan, K.F.; Menon, R. Inflammatory cytokine (interleukins 1, 6 and 8 and tumor necrosis factor-alpha) release from cultured human fetal membranes in response to endotoxic lipopolysaccharide mirrors amniotic fluid concentrations. Am. J. Obstet. Gynecol. 1996, 174, 1855–1861, discussion 1861–1852. [Google Scholar] [CrossRef]
- Menon, R.; Peltier, M.R.; Eckardt, J.; Fortunato, S.J. Diversity in cytokine response to bacteria associated with preterm birth by fetal membranes. Am. J. Obstet. Gynecol. 2009, 201, 306.e1–306.e6. [Google Scholar] [CrossRef]
- Romero, R.; Ceska, M.; Avila, C.; Mazor, M.; Behnke, E.; Lindley, I. Neutrophil attractant/activating peptide-1/interleukin-8 in term and preterm parturition. Am. J. Obstet. Gynecol. 1991, 165, 813–820. [Google Scholar] [CrossRef]
- Romero, R.; Gomez, R.; Ghezzi, F.; Yoon, B.H.; Mazor, M.; Edwin, S.S.; Berry, S.M. A fetal systemic inflammatory response is followed by the spontaneous onset of preterm parturition. Am. J. Obstet. Gynecol. 1998, 179, 186–193. [Google Scholar] [CrossRef]
- Romero, R.; Gomez, R.; Galasso, M.; Mazor, M.; Berry, S.M.; Quintero, R.A.; Cotton, D.B. The natural interleukin-1 receptor antagonist in the fetal, maternal, and amniotic fluid compartments: The effect of gestational age, fetal gender, and intrauterine infection. Am. J. Obstet. Gynecol. 1994, 171, 912–921. [Google Scholar] [CrossRef]
- Nadeau-Vallee, M.; Obari, D.; Quiniou, C.; Lubell, W.D.; Olson, D.M.; Girard, S.; Chemtob, S. A critical role of interleukin-1 in preterm labor. Cytokine Growth Factor Rev. 2016, 28, 37–51. [Google Scholar] [CrossRef]
- Gomez-Lopez, N.; Laresgoiti-Servitje, E.; Olson, D.M.; Estrada-Gutierrez, G.; Vadillo-Ortega, F. The role of chemokines in term and premature rupture of the fetal membranes: A review. Biol. Reprod 2010, 82, 809–814. [Google Scholar] [CrossRef]
- Vadillo-Ortega, F.; Estrada-Gutierrez, G. Role of matrix metalloproteinases in preterm labour. BJOG 2005, 112 (Suppl. 1), 19–22. [Google Scholar] [CrossRef] [PubMed]
- Keirse, M.J. The history of tocolysis. BJOG 2003, 110 (Suppl. 20), 94–97. [Google Scholar] [CrossRef]
- Elliott, J.P.; Morrison, J.C. The evidence regarding maintenance tocolysis. Obstet. Gynecol. Int. 2013, 2013, 708023. [Google Scholar] [CrossRef] [PubMed]
- Chawanpaiboon, S.; Laopaiboon, M.; Lumbiganon, P.; Sangkomkamhang, U.S.; Dowswell, T. Terbutaline pump maintenance therapy after threatened preterm labour for reducing adverse neonatal outcomes. Cochrane Database Syst. Rev. 2014, CD010800. [Google Scholar] [CrossRef] [PubMed]
- Creasy, R.K.; Golbus, M.S.; Laros, R.K., Jr.; Parer, J.T.; Roberts, J.M. Oral ritodrine maintenance in the treatment of preterm labor. Am. J. Obstet. Gynecol. 1980, 137, 212–219. [Google Scholar] [CrossRef]
- Chae, J.; Cho, G.J.; Oh, M.J.; Park, K.; Han, S.W.; Choi, S.J.; Oh, S.-Y.; Roh, C.R. In utero exposure to ritodrine during pregnancy and risk of autism in their offspring until 8 years of age. Sci. Rep. 2021. [Google Scholar] [CrossRef]
- Woyton, J.; Zimmer, M.; Fuchs, T. The use of Gynipral (hexoprenaline) in suppression of uterus contractions. Ginekol. Pol. 1999, 70, 896–900. [Google Scholar]
- Haas, D.M.; Benjamin, T.; Sawyer, R.; Quinney, S.K. Short-term tocolytics for preterm delivery—Current perspectives. Int. J. Womens Health 2014, 6, 343–349. [Google Scholar] [CrossRef]
- Neilson, J.P.; West, H.M.; Dowswell, T. Betamimetics for inhibiting preterm labour. Cochrane Database Syst Rev. 2014, CD004352. [Google Scholar] [CrossRef]
- Kosasa, T.S.; Nakayama, R.T.; Hale, R.W.; Rinzler, G.S.; Freitas, C.A. Ritodrine and terbutaline compared for the treatment of preterm labor. Acta Obstet. Gynecol. Scand. 1985, 64, 421–426. [Google Scholar] [CrossRef]
- Beall, M.H.; Edgar, B.W.; Paul, R.H.; Smith-Wallace, T. A comparison of ritodrine, terbutaline, and magnesium sulfate for the suppression of preterm labor. Am. J. Obstet. Gynecol. 1985, 153, 854–859. [Google Scholar] [CrossRef]
- Kopelman, J.N.; Duff, P.; Read, J.A. Randomized comparison of oral terbutaline and ritodrine for preventing recurrent preterm labor. J. Reprod Med. 1989, 34, 225–230. [Google Scholar] [PubMed]
- Weiss, M.A. Retrospective analysis of the effects of ritodrine and terbutaline in the management of preterm labor. Clin. Pharm. 1982, 1, 453–456. [Google Scholar] [PubMed]
- Caritis, S.N.; Toig, G.; Heddinger, L.A.; Ashmead, G. A double-blind study comparing ritodrine and terbutaline in the treatment of preterm labor. Am. J. Obstet. Gynecol. 1984, 150, 7–14. [Google Scholar] [CrossRef]
- Galik, M.; Gaspar, R.; Kolarovszki-Sipiczki, Z.; Falkay, G. Gestagen treatment enhances the tocolytic effect of salmeterol in hormone-induced preterm labor in the rat in vivo. Am. J. Obstet. Gynecol. 2008, 198, 319.e1–319.e5. [Google Scholar] [CrossRef]
- Gaspar, R.; Hajagos-Toth, J. Calcium channel blockers as tocolytics: Principles of their actions, adverse effects and therapeutic combinations. Pharmaceuticals 2013, 6, 689–699. [Google Scholar] [CrossRef]
- Perna, R.; Loughan, A.; Perkey, H.; Tyson, K. Terbutaline and Associated Risks for Neurodevelopmental Disorders. Child. Dev. Res. 2014, 2014. [Google Scholar] [CrossRef]
- Hayes, E.; Moroz, L.; Pizzi, L.; Baxter, J. A cost decision analysis of 4 tocolytic drugs. Am. J. Obstet. Gynecol. 2007, 197, 383.e1–383.e6. [Google Scholar] [CrossRef]
- Akerlund, M.; Carlsson, A.M.; Melin, P.; Trojnar, J. The effect on the human uterus of two newly developed competitive inhibitors of oxytocin and vasopressin. Acta Obstet. Gynecol. Scand. 1985, 64, 499–504. [Google Scholar] [CrossRef]
- Goodwin, T.M.; Paul, R.; Silver, H.; Spellacy, W.; Parsons, M.; Chez, R.; Hayashi, R.; Valenzuela, G.; Creasy, G.W.; Merriman, R. The effect of the oxytocin antagonist atosiban on preterm uterine activity in the human. Am. J. Obstet. Gynecol. 1994, 170, 474–478. [Google Scholar] [CrossRef]
- Goodwin, T.M.; Valenzuela, G.J.; Silver, H.; Creasy, G. Dose ranging study of the oxytocin antagonist atosiban in the treatment of preterm labor. Atosiban Study Group. Obstet. Gynecol. 1996, 88, 331–336. [Google Scholar] [CrossRef]
- Romero, R.; Sibai, B.M.; Sanchez-Ramos, L.; Valenzuela, G.J.; Veille, J.C.; Tabor, B.; Perry, K.G.; Varner, M.; Goodwin, T.M.; Lane, R.; et al. An oxytocin receptor antagonist (atosiban) in the treatment of preterm labor: A randomized, double-blind, placebo-controlled trial with tocolytic rescue. Am. J. Obstet. Gynecol. 2000, 182, 1173–1183. [Google Scholar] [CrossRef]
- Valenzuela, G.J.; Sanchez-Ramos, L.; Romero, R.; Silver, H.M.; Koltun, W.D.; Millar, L.; Hobbins, J.; Rayburn, W.; Shangold, G.; Wang, J.; et al. Maintenance treatment of preterm labor with the oxytocin antagonist atosiban. The Atosiban PTL-098 Study Group. Am. J. Obstet. Gynecol. 2000, 182, 1184–1190. [Google Scholar] [CrossRef]
- Greene, J.A.; Podolsky, S.H. Reform, regulation, and pharmaceuticals—The Kefauver-Harris Amendments at 50. N. Engl. J. Med. 2012, 367, 1481–1483. [Google Scholar] [CrossRef]
- Veiga, G.A.; Milazzotto, M.P.; Nichi, M.; Lucio, C.F.; Silva, L.C.; Angrimani, D.S.; Vannucchi, C.I. Gene expression of estrogen and oxytocin receptors in the uterus of pregnant and parturient bitches. Braz. J. Med. Biol. Res. 2015, 48, 339–343. [Google Scholar] [CrossRef][Green Version]
- Arthur, P.; Taggart, M.J.; Mitchell, B.F. Oxytocin and parturition: A role for increased myometrial calcium and calcium sensitization? Front. Biosci. 2007, 12, 619–633. [Google Scholar] [CrossRef][Green Version]
- Kim, S.H.; Riaposova, L.; Ahmed, H.; Pohl, O.; Chollet, A.; Gotteland, J.P.; Hanyaloglu, A.; Bennett, P.R.; Terzidou, V. Oxytocin Receptor Antagonists, Atosiban and Nolasiban, Inhibit Prostaglandin F2alpha-induced Contractions and Inflammatory Responses in Human Myometrium. Sci. Rep. 2019, 9, 5792. [Google Scholar] [CrossRef]
- Moutquin, J.M.; Sherman, D.; Cohen, H.; Mohide, P.T.; Hochner-Celnikier, D.; Fejgin, M.; Liston, R.M.; Dansereau, J.; Mazor, M.; Shalev, E.; et al. Double-blind, randomized, controlled trial of atosiban and ritodrine in the treatment of preterm labor: A multicenter effectiveness and safety study. Am. J. Obstet. Gynecol. 2000, 182, 1191–1199. [Google Scholar] [CrossRef]
- Papatsonis, D.; Flenady, V.; Cole, S.; Liley, H. Oxytocin receptor antagonists for inhibiting preterm labour. Cochrane Database Syst. Rev. 2005, CD004452. [Google Scholar] [CrossRef]
- Fullerton, M.B.G.M.; Shetty, A.; Bhattacharya, S. Atosiban in the Management of Preterm Labor. Clin. Med. Insights: Women’s Health 2011, 4. [Google Scholar] [CrossRef]
- Sanchez-Ramos, L. A double-blind placebo-controlled trial of oxytocin receptor antagonist (antocin) maintenance therapy in patients with preterm labor. Pediatric Res. 1997, 41. [Google Scholar] [CrossRef]
- Taira, N. Nifedipine: A novel vasodilator. Drugs 2006, 66, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Conde-Agudelo, A.; Romero, R.; Kusanovic, J.P. Nifedipine in the management of preterm labor: A systematic review and metaanalysis. Am. J. Obstet. Gynecol. 2011, 204, 134.e1–134.e20. [Google Scholar] [CrossRef] [PubMed]
- Le Ray, C.; Maillard, F.; Carbonne, B.; Verspyck, E.; Cabrol, D.; Goffinet, F.; EVAPRIMA Group. Nifedipine or nicardipine in management of threatened preterm delivery: An observational population-based study. J. Gynecol. Obstet. Biol. Reprod 2010, 39, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Papatsonis, D.N.; Van Geijn, H.P.; Ader, H.J.; Lange, F.M.; Bleker, O.P.; Dekker, G.A. Nifedipine and ritodrine in the management of preterm labor: A randomized multicenter trial. Obstet. Gynecol. 1997, 90, 230–234. [Google Scholar] [CrossRef]
- Habli, M.; Clifford, C.C.; Brady, T.M.; Rodriguez, Z.; Eschenbacher, M.; Wu, M.; DeFranco, E.; Gresh, J.; Kamath-Rayne, B.D. Antenatal exposure to nonsteroidal anti-inflammatory drugs and risk of neonatal hypertension. J. Clin. Hypertens 2018, 20, 1334–1341. [Google Scholar] [CrossRef]
- Abramson, S.; Korchak, H.; Ludewig, R.; Edelson, H.; Haines, K.; Levin, R.I.; Herman, R.; Rider, L.; Kimmel, S.; Weissmann, G. Modes of action of aspirin-like drugs. Proc. Natl. Acad. Sci. USA 1985, 82, 7227–7231. [Google Scholar] [CrossRef]
- Orlando, B.J.; Lucido, M.J.; Malkowski, M.G. The structure of ibuprofen bound to cyclooxygenase-2. J. Struct. Biol. 2015, 189, 62–66. [Google Scholar] [CrossRef]
- Al-Mondhiri, H.M.A.; Spaet, T.H. Acetylation of human platelets by aspirin. Fed. Proc. 1969, 28, 576. [Google Scholar]
- Mitchell, J.A.; Akarasereenont, P.; Thiemermann, C.; Flower, R.J.; Vane, J.R. Selectivity of nonsteroidal antiinflammatory drugs as inhibitors of constitutive and inducible cyclooxygenase. Proc. Natl. Acad. Sci. USA 1993, 90, 11693–11697. [Google Scholar] [CrossRef]
- Sadovsky, Y.; Nelson, D.M.; Muglia, L.J.; Gross, G.A.; Harris, K.C.; Koki, A.; Masferrer, J.L.; Olson, L.M. Effective diminution of amniotic prostaglandin production by selective inhibitors of cyclooxygenase type 2. Am. J. Obstet. Gynecol. 2000, 182, 370–376. [Google Scholar] [CrossRef]
- Gross, G.; Imamura, T.; Vogt, S.K.; Wozniak, D.F.; Nelson, D.M.; Sadovsky, Y.; Muglia, L.J. Inhibition of cyclooxygenase-2 prevents inflammation-mediated preterm labor in the mouse. Am. J. Physiol. Regul. Integr. Comp. Physiol. 2000, 278, R1415–R1423. [Google Scholar] [CrossRef]
- Yousif, M.H.; Thulesius, O. Tocolytic effect of the cyclooxygenase-2 inhibitor, meloxicam: Studies on uterine contractions in the rat. J. Pharm. Pharmacol. 1998, 50, 681–685. [Google Scholar] [CrossRef]
- Hirst, J.J.; Mijovic, J.E.; Zakar, T.; Olson, D.M. Prostaglandin endoperoxide H synthase-1 and -2 mRNA levels and enzyme activity in human decidua at term labor. J. Soc. Gynecol. Investig. 1998, 5, 13–20. [Google Scholar] [CrossRef]
- Hirst, J.J.; Teixeira, F.J.; Zakar, T.; Olson, D.M. Prostaglandin endoperoxide-H synthase-1 and -2 messenger ribonucleic acid levels in human amnion with spontaneous labor onset. J. Clin. Endocrinol. Metab. 1995, 80, 517–523. [Google Scholar] [CrossRef]
- Hirst, J.J.; Teixeira, F.J.; Zakar, T.; Olson, D.M. Prostaglandin H synthase-2 expression increases in human gestational tissues with spontaneous labour onset. Reprod. Fertil. Dev. 1995, 7, 633–637. [Google Scholar] [CrossRef]
- Mijovic, J.E.; Zakar, T.; Nairn, T.K.; Olson, D.M. Prostaglandin-endoperoxide H synthase-2 expression and activity increases with term labor in human chorion. Am. J. Physiol. 1997, 272, E832–E840. [Google Scholar] [CrossRef]
- Mijovic, J.E.; Zakar, T.; Angelova, J.; Olson, D.M. Prostaglandin endoperoxide H synthase mRNA expression in the human amnion and decidua during pregnancy and in the amnion at preterm labour. Mol. Hum. Reprod. 1999, 5, 182–187. [Google Scholar] [CrossRef]
- Khanprakob, T.; Laopaiboon, M.; Lumbiganon, P.; Sangkomkamhang, U.S. Cyclo-oxygenase (COX) inhibitors for preventing preterm labour. Cochrane Database Syst. Rev. 2012, 10, CD007748. [Google Scholar] [CrossRef]
- Reinebrant, H.E.; Pileggi-Castro, C.; Romero, C.L.; Dos Santos, R.A.; Kumar, S.; Souza, J.P.; Flenady, V. Cyclo-oxygenase (COX) inhibitors for treating preterm labour. Cochrane Database Syst. Rev. 2015, CD001992. [Google Scholar] [CrossRef]
- Groom, K.M.; Shennan, A.H.; Jones, B.A.; Seed, P.; Bennett, P.R. TOCOX--a randomised, double-blind, placebo-controlled trial of rofecoxib (a COX-2-specific prostaglandin inhibitor) for the prevention of preterm delivery in women at high risk. BJOG 2005, 112, 725–730. [Google Scholar] [CrossRef]
- Rolnik, D.L.; Wright, D.; Poon, L.C.; O’Gorman, N.; Syngelaki, A.; de Paco Matallana, C.; Akolekar, R.; Cicero, S.; Janga, D.; Singh, M.; et al. Aspirin versus Placebo in Pregnancies at High Risk for Preterm Preeclampsia. N. Engl. J. Med. 2017, 377, 613–622. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, M.K.; Goudar, S.S.; Kodkany, B.S.; Metgud, M.; Somannavar, M.; Okitawutshu, J.; Lokangaka, A.; Tshefu, A.; Bose, C.L.; Mwapule, A.; et al. Low-dose aspirin for the prevention of preterm delivery in nulliparous women with a singleton pregnancy (ASPIRIN): A randomised, double-blind, placebo-controlled trial. Lancet 2020, 395, 285–293. [Google Scholar] [CrossRef]
- Henderson, J.T.; Whitlock, E.P.; O’Connor, E.; Senger, C.A.; Thompson, J.H.; Rowland, M.G. Low-dose aspirin for prevention of morbidity and mortality from preeclampsia: A systematic evidence review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2014, 160, 695–703. [Google Scholar] [CrossRef] [PubMed]
- Andrikopoulou, M.; Purisch, S.E.; Handal-Orefice, R.; Gyamfi-Bannerman, C. Low-dose aspirin is associated with reduced spontaneous preterm birth in nulliparous women. Am. J. Obstet. Gynecol. 2018, 219, 399.e1–399.e6. [Google Scholar] [CrossRef]
- Lunt, C.C.; Satin, A.J.; Barth, W.H., Jr.; Hankins, G.D. The effect of indomethacin tocolysis on maternal coagulation status. Obstet. Gynecol. 1994, 84, 820–822. [Google Scholar]
- Shah, A.A.; Thjodleifsson, B.; Murray, F.E.; Kay, E.; Barry, M.; Sigthorsson, G.; Gudjonsson, H.; Oddsson, E.; Price, A.B.; Fitzgerald, D.J.; et al. Selective inhibition of COX-2 in humans is associated with less gastrointestinal injury: A comparison of nimesulide and naproxen. Gut 2001, 48, 339–346. [Google Scholar] [CrossRef]
- Ungprasert, P.; Cheungpasitporn, W.; Crowson, C.S.; Matteson, E.L. Individual non-steroidal anti-inflammatory drugs and risk of acute kidney injury: A systematic review and meta-analysis of observational studies. Eur. J. Intern. Med. 2015, 26, 285–291. [Google Scholar] [CrossRef]
- American College of Obstetricians and Gynecologists; Committee on Practice Bulletins—Obstetrics. Practice Bulletin No. 171: Management of Preterm Labor. Obstet. Gynecol. 2016, 128, e155–e164. [Google Scholar] [CrossRef]
- Moise, K.J., Jr. Effect of advancing gestational age on the frequency of fetal ductal constriction in association with maternal indomethacin use. Am. J. Obstet. Gynecol. 1993, 168, 1350–1353. [Google Scholar] [CrossRef]
- Sawdy, R.J.; Lye, S.; Fisk, N.M.; Bennett, P.R. A double-blind randomized study of fetal side effects during and after the short-term maternal administration of indomethacin, sulindac, and nimesulide for the treatment of preterm labor. Am. J. Obstet. Gynecol. 2003, 188, 1046–1051. [Google Scholar] [CrossRef]
- Moise, K.J., Jr.; Huhta, J.C.; Sharif, D.S.; Ou, C.N.; Kirshon, B.; Wasserstrum, N.; Cano, L. Indomethacin in the treatment of premature labor. Effects on the fetal ductus arteriosus. N. Engl. J. Med. 1988, 319, 327–331. [Google Scholar] [CrossRef]
- Dudley, D.K.; Hardie, M.J. Fetal and neonatal effects of indomethacin used as a tocolytic agent. Am. J. Obstet. Gynecol. 1985, 151, 181–184. [Google Scholar] [CrossRef]
- Niebyl, J.R.; Witter, F.R. Neonatal outcome after indomethacin treatment for preterm labor. Am. J. Obstet. Gynecol. 1986, 155, 747–749. [Google Scholar] [CrossRef]
- Abarbanel, A.R. The spasmolysant action of magnesium ions on the tetanically contracting human gravid uterus. Am. J. Obstet. Gynecol. 1945, 473–483. [Google Scholar] [CrossRef]
- Hall, D.G. Serum magnesium in pregnancy. Obstet. Gynecol. 1957, 9, 158–162. [Google Scholar]
- Gordon, M.C.; Iams, J.D. Magnesium sulfate. Clin. Obstet. Gynecol. 1995, 38, 706–712. [Google Scholar] [CrossRef]
- Elliott, J.P.; Morrison, J.C.; Bofill, J.A. Risks and Benefits of Magnesium Sulfate Tocolysis in Preterm Labor (PTL). AIMS Public Health 2016, 3, 348–356. [Google Scholar] [CrossRef]
- Mercer, B.M.; Merlino, A.A.; Society for Maternal-Fetal Medicine. Magnesium sulfate for preterm labor and preterm birth. Obstet. Gynecol. 2009, 114, 650–668. [Google Scholar] [CrossRef]
- Crowther, C.A.; Brown, J.; McKinlay, C.J.; Middleton, P. Magnesium sulphate for preventing preterm birth in threatened preterm labour. Cochrane Database Syst. Rev. 2014, CD001060. [Google Scholar] [CrossRef]
- Hall, D.G.; Mc, G.H., Jr.; Corey, E.L.; Thornton, W.N., Jr. The effects of magnesium therapy on the duration of labor. Am. J. Obstet. Gynecol. 1959, 78, 27–32. [Google Scholar] [CrossRef]
- Fomin, V.P.; Gibbs, S.G.; Vanam, R.; Morimiya, A.; Hurd, W.W. Effect of magnesium sulfate on contractile force and intracellular calcium concentration in pregnant human myometrium. Am. J. Obstet. Gynecol. 2006, 194, 1384–1390. [Google Scholar] [CrossRef]
- Phillippe, M. Cellular mechanisms underlying magnesium sulfate inhibition of phasic myometrial contractions. Biochem. Biophys. Res. Commun. 1998, 252, 502–507. [Google Scholar] [CrossRef]
- Tica, V.I.; Tica, A.A.; Carlig, V.; Banica, O.S. Magnesium ion inhibits spontaneous and induced contractions of isolated uterine muscle. Gynecol. Endocrinol. 2007, 23, 368–372. [Google Scholar] [CrossRef]
- Lewis, D.F. Magnesium sulfate: The first-line tocolytic. Obstet. Gynecol. Clin. North. Am. 2005, 32, 485–500. [Google Scholar] [CrossRef]
- Han, S.; Crowther, C.A.; Moore, V. Magnesium maintenance therapy for preventing preterm birth after threatened preterm labour. Cochrane Database Syst. Rev. 2010. [Google Scholar] [CrossRef]
- Committee Opinion No. 455: Magnesium sulfate before anticipated preterm birth for neuroprotection. Obstet. Gynecol. 2010, 115, 669–671. [CrossRef]
- McNamara, H.C.; Crowther, C.A.; Brown, J. Different treatment regimens of magnesium sulphate for tocolysis in women in preterm labour. Cochrane Database Syst. Rev. 2015, CD011200. [Google Scholar] [CrossRef]
- Haas, D.M.; Caldwell, D.M.; Kirkpatrick, P.; McIntosh, J.J.; Welton, N.J. Tocolytic therapy for preterm delivery: Systematic review and network meta-analysis. BMJ 2012, 345, e6226. [Google Scholar] [CrossRef]
- Makrides, M.; Crosby, D.D.; Bain, E.; Crowther, C.A. Magnesium supplementation in pregnancy. Cochrane Database Syst. Rev. 2014, CD000937. [Google Scholar] [CrossRef]
- Crowther, C.A.; Hiller, J.E.; Doyle, L.W.; Haslam, R.R.; Australasian Collaborative Trial of Magnesium Sulphate Collaborative Group. Effect of magnesium sulfate given for neuroprotection before preterm birth: A randomized controlled trial. JAMA 2003, 290, 2669–2676. [Google Scholar] [CrossRef]
- Rouse, D.J.; Hirtz, D.G.; Thom, E.; Varner, M.W.; Spong, C.Y.; Mercer, B.M.; Iams, J.D.; Wapner, R.J.; Sorokin, Y.; Alexander, J.M.; et al. A randomized, controlled trial of magnesium sulfate for the prevention of cerebral palsy. N. Engl. J. Med. 2008, 359, 895–905. [Google Scholar] [CrossRef] [PubMed]
- Marret, S.; Marpeau, L.; Follet-Bouhamed, C.; Cambonie, G.; Astruc, D.; Delaporte, B.; Bruel, H.; Guillois, B.; Pinquier, D.; Zupan-Simunek, V.; et al. Effect of magnesium sulphate on mortality and neurologic morbidity of the very-preterm newborn (of less than 33 weeks) with two-year neurological outcome: Results of the prospective PREMAG trial. Gynecol. Obstet. Fertil. 2008, 36, 278–288. [Google Scholar] [CrossRef] [PubMed]
- Marret, S.; Marpeau, L.; Zupan-Simunek, V.; Eurin, D.; Leveque, C.; Hellot, M.F.; Benichou, J.; PREMAG Trial Group. Magnesium sulphate given before very-preterm birth to protect infant brain: The randomised controlled PREMAG trial*. BJOG 2007, 114, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Doyle, L.W.; Crowther, C.A.; Middleton, P.; Marret, S.; Rouse, D. Magnesium sulphate for women at risk of preterm birth for neuroprotection of the fetus. Cochrane Database Syst. Rev. 2009, CD004661. [Google Scholar] [CrossRef]
- Grimes, D.A.; Nanda, K. Magnesium sulfate tocolysis: Time to quit. Obstet. Gynecol. 2006, 108, 986–989. [Google Scholar] [CrossRef]
- Klauser, C.K.; Briery, C.M.; Keiser, S.D.; Martin, R.W.; Kosek, M.A.; Morrison, J.C. Effect of antenatal tocolysis on neonatal outcomes. J. Matern Fetal Neonatal Med. 2012, 25, 2778–2781. [Google Scholar] [CrossRef]
- Nassar, A.H.; Sakhel, K.; Maarouf, H.; Naassan, G.R.; Usta, I.M. Adverse maternal and neonatal outcome of prolonged course of magnesium sulfate tocolysis. Acta Obstet. Gynecol. Scand. 2006, 85, 1099–1103. [Google Scholar] [CrossRef]
- Mittendorf, R.; Covert, R.; Boman, J.; Khoshnood, B.; Lee, K.S.; Siegler, M. Is tocolytic magnesium sulphate associated with increased total paediatric mortality? Lancet 1997, 350, 1517–1518. [Google Scholar] [CrossRef]
- Romero, R.; Espinoza, J.; Kusanovic, J.P.; Gotsch, F.; Hassan, S.; Erez, O.; Chaiworapongsa, T.; Mazor, M. The preterm parturition syndrome. BJOG 2006, 113 (Suppl. 3), 17–42. [Google Scholar] [CrossRef]
- Hillier, S.L.; Krohn, M.A.; Cassen, E.; Easterling, T.R.; Rabe, L.K.; Eschenbach, D.A. The role of bacterial vaginosis and vaginal bacteria in amniotic fluid infection in women in preterm labor with intact fetal membranes. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1995, 20 (Suppl. 2), S276–S278. [Google Scholar] [CrossRef]
- DiGiulio, D.B.; Romero, R.; Kusanovic, J.P.; Gomez, R.; Kim, C.J.; Seok, K.S.; Gotsch, F.; Mazaki-Tovi, S.; Vaisbuch, E.; Sanders, K.; et al. Prevalence and diversity of microbes in the amniotic fluid, the fetal inflammatory response, and pregnancy outcome in women with preterm pre-labor rupture of membranes. Am. J. Reprod. Immunol. 2010, 64, 38–57. [Google Scholar] [CrossRef]
- Romero, R.; Espinoza, J.; Goncalves, L.F.; Kusanovic, J.P.; Friel, L.; Hassan, S. The role of inflammation and infection in preterm birth. Semin. Reprod. Med. 2007, 25, 21–39. [Google Scholar] [CrossRef]
- Flenady, V.; Hawley, G.; Stock, O.M.; Kenyon, S.; Badawi, N. Prophylactic antibiotics for inhibiting preterm labour with intact membranes. Cochrane Database Syst. Rev. 2013, CD000246. [Google Scholar] [CrossRef]
- Kenyon, S.L.; Taylor, D.J.; Tarnow-Mordi, W. Broad-spectrum antibiotics for spontaneous preterm labour: The ORACLE II randomised trial. ORACLE Collaborative Group. Lancet 2001, 357, 989–994. [Google Scholar] [CrossRef]
- Stetzer, B.P.; Mercer, B.M. Antibiotics and preterm labor. Clin. Obstet. Gynecol. 2000, 43, 809–817. [Google Scholar] [CrossRef]
- Kenyon, S.; Pike, K.; Jones, D.R.; Brocklehurst, P.; Marlow, N.; Salt, A.; Taylor, D.J. Childhood outcomes after prescription of antibiotics to pregnant women with spontaneous preterm labour: 7-year follow-up of the ORACLE II trial. Lancet 2008, 372, 1319–1327. [Google Scholar] [CrossRef]
- Goldenberg, R.L.; Culhane, J.F.; Iams, J.D.; Romero, R. Epidemiology and causes of preterm birth. Lancet 2008, 371, 75–84. [Google Scholar] [CrossRef]
- Menon, R.; Fortunato, S.J. Infection and the role of inflammation in preterm premature rupture of the membranes. Best Pract. Res. Clin. Obstet. Gynaecol. 2007, 21, 467–478. [Google Scholar] [CrossRef]
- Lannon, S.M.; Vanderhoeven, J.P.; Eschenbach, D.A.; Gravett, M.G.; Adams Waldorf, K.M. Synergy and interactions among biological pathways leading to preterm premature rupture of membranes. Reprod. Sci. 2014, 21, 1215–1227. [Google Scholar] [CrossRef]
- Ehsanipoor, R. ACOG Practice Bulletin No. 188: Prelabor Rupture of Membranes. Obstet. Gynecol. 2018, 131, e1–e14. [Google Scholar] [CrossRef]
- Prelabor Rupture of Membranes: ACOG Practice Bulletin, Number 217. Obstet. Gynecol. 2020, 135, e80–e97. [CrossRef]
- Mercer, B.M.; Miodovnik, M.; Thurnau, G.R.; Goldenberg, R.L.; Das, A.F.; Ramsey, R.D.; Rabello, Y.A.; Meis, P.J.; Moawad, A.H.; Iams, J.D.; et al. Antibiotic therapy for reduction of infant morbidity after preterm premature rupture of the membranes. A randomized controlled trial. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. JAMA J. Am. Med. Assoc. 1997, 278, 989–995. [Google Scholar] [CrossRef]
- Kenyon, S.L.; Taylor, D.J.; Tarnow-Mordi, W. Broad-spectrum antibiotics for preterm, prelabour rupture of fetal membranes: The ORACLE I randomised trial. ORACLE Collaborative Group. Lancet 2001, 357, 979–988. [Google Scholar] [CrossRef]
- Lee, J.; Romero, R.; Kim, S.M.; Chaemsaithong, P.; Park, C.W.; Park, J.S.; Jun, J.K.; Yoon, B.H. A new anti-microbial combination prolongs the latency period, reduces acute histologic chorioamnionitis as well as funisitis, and improves neonatal outcomes in preterm PROM. J. Matern Fetal Neonatal Med. 2016, 29, 707–720. [Google Scholar] [CrossRef]
- Mackeen, A.D.; Seibel-Seamon, J.; Muhammad, J.; Baxter, J.K.; Berghella, V. Tocolytics for preterm premature rupture of membranes. Cochrane Database Syst. Rev. 2014, CD007062. [Google Scholar] [CrossRef]
- Lorthe, E.; Goffinet, F.; Marret, S.; Vayssiere, C.; Flamant, C.; Quere, M.; Benhammou, V.; Ancel, P.Y.; Kayem, G. Tocolysis after preterm premature rupture of membranes and neonatal outcome: A propensity-score analysis. Am. J. Obstet. Gynecol. 2017, 217, 212.e1–212.e12. [Google Scholar] [CrossRef]
- Hillier, S.L.; Krohn, M.A.; Rabe, L.K.; Klebanoff, S.J.; Eschenbach, D.A. The normal vaginal flora, H2O2-producing lactobacilli, and bacterial vaginosis in pregnant women. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 1993, 16 (Suppl. 4), S273–S281. [Google Scholar] [CrossRef]
- Hillier, S.L.; Martius, J.; Krohn, M.; Kiviat, N.; Holmes, K.K.; Eschenbach, D.A. A case-control study of chorioamnionic infection and histologic chorioamnionitis in prematurity. N. Engl. J. Med. 1988, 319, 972–978. [Google Scholar] [CrossRef] [PubMed]
- Hillier, S.L.; Nugent, R.P.; Eschenbach, D.A.; Krohn, M.A.; Gibbs, R.S.; Martin, D.H.; Cotch, M.F.; Edelman, R.; Pastorek, J.G., 2nd; Rao, A.V.; et al. Association between bacterial vaginosis and preterm delivery of a low-birth-weight infant. The Vaginal Infections and Prematurity Study Group. N. Engl. J. Med. 1995, 333, 1737–1742. [Google Scholar] [CrossRef] [PubMed]
- Hitti, J.; Hillier, S.L.; Agnew, K.J.; Krohn, M.A.; Reisner, D.P.; Eschenbach, D.A. Vaginal indicators of amniotic fluid infection in preterm labor. Obstet. Gynecol. 2001, 97, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Hitti, J.; Lapidus, J.A.; Lu, X.; Reddy, A.P.; Jacob, T.; Dasari, S.; Eschenbach, D.A.; Gravett, M.G.; Nagalla, S.R. Noninvasive diagnosis of intraamniotic infection: Proteomic biomarkers in vaginal fluid. Am. J. Obstet. Gynecol. 2010, 203, 32.e1–32.e8. [Google Scholar] [CrossRef][Green Version]
- Krohn, M.A.; Hillier, S.L.; Lee, M.L.; Rabe, L.K.; Eschenbach, D.A. Vaginal Bacteroides species are associated with an increased rate of preterm delivery among women in preterm labor. J. Infect. Dis. 1991, 164, 88–93. [Google Scholar] [CrossRef]
- Krohn, M.A.; Hillier, S.L.; Nugent, R.P.; Cotch, M.F.; Carey, J.C.; Gibbs, R.S.; Eschenbach, D.A. The genital flora of women with intraamniotic infection. Vaginal Infection and Prematurity Study Group. J. Infect. Dis. 1995, 171, 1475–1480. [Google Scholar] [CrossRef]
- Meis, P.J.; Goldenberg, R.L.; Mercer, B.; Moawad, A.; Das, A.; McNellis, D.; Johnson, F.; Iams, J.D.; Thom, E.; Andrews, W.W. The preterm prediction study: Significance of vaginal infections. National Institute of Child Health and Human Development Maternal-Fetal Medicine Units Network. Am. J. Obstet. Gynecol. 1995, 173, 1231–1235. [Google Scholar] [CrossRef]
- Carey, J.C.; Klebanoff, M.A.; Hauth, J.C.; Hillier, S.L.; Thom, E.A.; Ernest, J.M.; Heine, R.P.; Nugent, R.P.; Fischer, M.L.; Leveno, K.J.; et al. Metronidazole to prevent preterm delivery in pregnant women with asymptomatic bacterial vaginosis. National Institute of Child Health and Human Development Network of Maternal-Fetal Medicine Units. N. Engl. J. Med. 2000, 342, 534–540. [Google Scholar] [CrossRef]
- Joesoef, M.R.; Hillier, S.L.; Wiknjosastro, G.; Sumampouw, H.; Linnan, M.; Norojono, W.; Idajadi, A.; Utomo, B. Intravaginal clindamycin treatment for bacterial vaginosis: Effects on preterm delivery and low birth weight. Am. J. Obstet. Gynecol. 1995, 173, 1527–1531. [Google Scholar] [CrossRef]
- McGregor, J.A.; French, J.I.; Jones, W.; Milligan, K.; McKinney, P.J.; Patterson, E.; Parker, R. Bacterial vaginosis is associated with prematurity and vaginal fluid mucinase and sialidase: Results of a controlled trial of topical clindamycin cream. Am. J. Obstet. Gynecol. 1994, 170, 1048–1059, discussion 1059–1060. [Google Scholar] [CrossRef]
- US Preventive Services Task Force; Owens, D.K.; Davidson, K.W.; Krist, A.H.; Barry, M.J.; Cabana, M.; Caughey, A.B.; Donahue, K.; Doubeni, C.A.; Epling, J.W., Jr.; et al. Screening for Bacterial Vaginosis in Pregnant Persons to Prevent Preterm Delivery: US Preventive Services Task Force Recommendation Statement. JAMA 2020, 323, 1286–1292. [Google Scholar] [CrossRef]
- Kahwati, L.C.; Clark, R.; Berkman, N.; Urrutia, R.; Patel, S.V.; Zeng, J.; Viswanathan, M. Screening for Bacterial Vaginosis in Pregnant Adolescents and Women to Prevent Preterm Delivery: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2020, 323, 1293–1309. [Google Scholar] [CrossRef]
- Subtil, D.; Brabant, G.; Tilloy, E.; Devos, P.; Canis, F.; Fruchart, A.; Bissinger, M.C.; Dugimont, J.C.; Nolf, C.; Hacot, C.; et al. Early clindamycin for bacterial vaginosis in pregnancy (PREMEVA): A multicentre, double-blind, randomised controlled trial. Lancet 2018, 392, 2171–2179. [Google Scholar] [CrossRef]
- Mitchell, C.; Balkus, J.; Agnew, K.; Lawler, R.; Hitti, J. Changes in the vaginal microenvironment with metronidazole treatment for bacterial vaginosis in early pregnancy. J. Women’s Health 2009, 18, 1817–1824. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, C.M.; Hitti, J.E.; Agnew, K.J.; Fredricks, D.N. Comparison of oral and vaginal metronidazole for treatment of bacterial vaginosis in pregnancy: Impact on fastidious bacteria. BMC Infect. Dis. 2009, 9, 89. [Google Scholar] [CrossRef] [PubMed]
- Hummelen, R.; Fernandes, A.D.; Macklaim, J.M.; Dickson, R.J.; Changalucha, J.; Gloor, G.B.; Reid, G. Deep sequencing of the vaginal microbiota of women with HIV. PLoS ONE 2010, 5, e12078. [Google Scholar] [CrossRef]
- Gomez, L.M.; Sammel, M.D.; Appleby, D.H.; Elovitz, M.A.; Baldwin, D.A.; Jeffcoat, M.K.; Macones, G.A.; Parry, S. Evidence of a gene-environment interaction that predisposes to spontaneous preterm birth: A role for asymptomatic bacterial vaginosis and DNA variants in genes that control the inflammatory response. Am. J. Obstet. Gynecol. 2010, 202, 386.e1–386.e6. [Google Scholar] [CrossRef]
- Andrews, W.W.; Klebanoff, M.A.; Thom, E.A.; Hauth, J.C.; Carey, J.C.; Meis, P.J.; Caritis, S.N.; Leveno, K.J.; Wapner, R.J.; Varner, M.W.; et al. Midpregnancy genitourinary tract infection with Chlamydia trachomatis: Association with subsequent preterm delivery in women with bacterial vaginosis and Trichomonas vaginalis. Am. J. Obstet. Gynecol. 2006, 194, 493–500. [Google Scholar] [CrossRef]
- Meis, P.J.; Michielutte, R.; Peters, T.J.; Wells, H.B.; Sands, R.E.; Coles, E.C.; Johns, K.A. Factors associated with preterm birth in Cardiff, Wales. I. Univariable and multivariable analysis. Am. J. Obstet. Gynecol. 1995, 173, 590–596. [Google Scholar] [CrossRef]
- Meis, P.J.; Michielutte, R.; Peters, T.J.; Wells, H.B.; Sands, R.E.; Coles, E.C.; Johns, K.A. Factors associated with preterm birth in Cardiff, Wales. II. Indicated and spontaneous preterm birth. Am. J. Obstet. Gynecol. 1995, 173, 597–602. [Google Scholar] [CrossRef]
- Tilton, R.C.; Steingrimsson, O.; Ryan, R.W. Susceptibilities of Pseudomonas species to tetracycline, minocycline, gentamicin, and tobramycin. Am. J. Clin. Pathol 1978, 69, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Burtin, P.; Taddio, A.; Ariburnu, O.; Einarson, T.R.; Koren, G. Safety of metronidazole in pregnancy: A meta-analysis. Am. J. Obstet. Gynecol. 1995, 172, 525–529. [Google Scholar] [CrossRef]
- Klebanoff, M.A.; Carey, J.C.; Hauth, J.C.; Hillier, S.L.; Nugent, R.P.; Thom, E.A.; Ernest, J.M.; Heine, R.P.; Wapner, R.J.; Trout, W.; et al. Failure of metronidazole to prevent preterm delivery among pregnant women with asymptomatic Trichomonas vaginalis infection. N. Engl. J. Med. 2001, 345, 487–493. [Google Scholar] [CrossRef]
- Schuster, H.J.; de Jonghe, B.A.; Limpens, J.; Budding, A.E.; Painter, R.C. Asymptomatic vaginal Candida colonization and adverse pregnancy outcomes including preterm birth: A systematic review and meta-analysis. Am. J. Obstet. Gynecol. MFM 2020, 2, 100163. [Google Scholar] [CrossRef]
- Norwitz, E.R.; Caughey, A.B. Progesterone supplementation and the prevention of preterm birth. Rev. Obstet. Gynecol. 2011, 4, 60–72. [Google Scholar]
- Mesiano, S.A.; Peters, G.A.; Amini, P.; Wilson, R.A.; Tochtrop, G.P.; van Den Akker, F. Progestin therapy to prevent preterm birth: History and effectiveness of current strategies and development of novel approaches. Placenta 2019, 79, 46–52. [Google Scholar] [CrossRef]
- Da Fonseca, E.B.; Bittar, R.E.; Carvalho, M.H.; Zugaib, M. Prophylactic administration of progesterone by vaginal suppository to reduce the incidence of spontaneous preterm birth in women at increased risk: A randomized placebo-controlled double-blind study. Am. J. Obstet. Gynecol. 2003, 188, 419–424. [Google Scholar] [CrossRef]
- Meis, P.J.; Klebanoff, M.; Thom, E.; Dombrowski, M.P.; Sibai, B.; Moawad, A.H.; Spong, C.Y.; Hauth, J.C.; Miodovnik, M.; Varner, M.W.; et al. Prevention of recurrent preterm delivery by 17 alpha-hydroxyprogesterone caproate. N. Engl. J. Med. 2003, 348, 2379–2385. [Google Scholar] [CrossRef]
- Choi, S.J. Use of progesterone supplement therapy for prevention of preterm birth: Review of literatures. Obstet. Gynecol. Sci. 2017, 60, 405–420. [Google Scholar] [CrossRef]
- Chang, C.Y.; Nguyen, C.P.; Wesley, B.; Guo, J.; Johnson, L.L.; Joffe, H.V. Withdrawing Approval of Makena—A Proposal from the FDA Center for Drug Evaluation and Research. N. Engl. J. Med. 2020, 383, e131. [Google Scholar] [CrossRef]
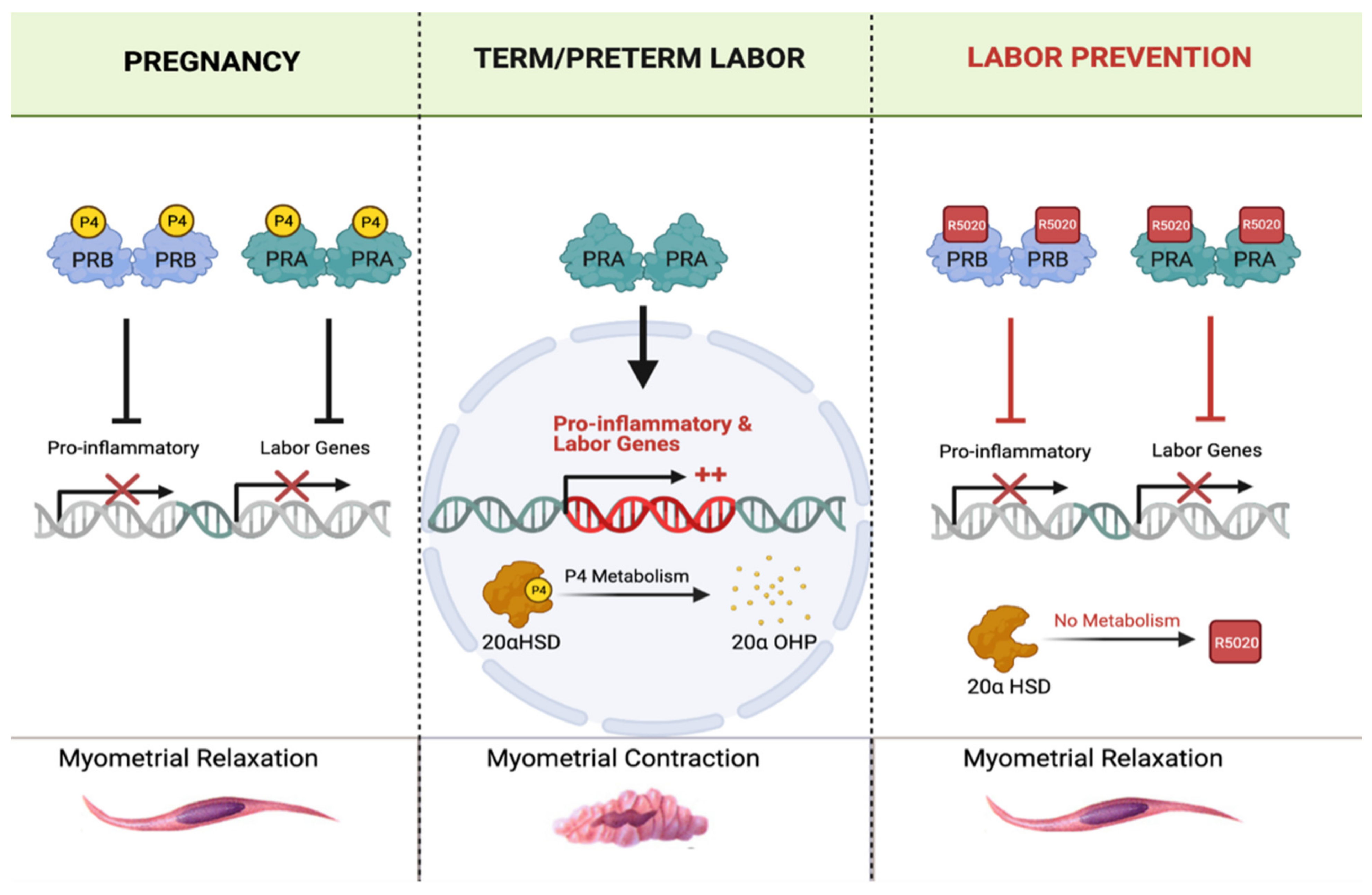
- Astle, S.; Slater, D.M.; Thornton, S. The involvement of progesterone in the onset of human labour. Eur. J. Obstet. Gynecol. Reprod. Biol. 2003, 108, 177–181. [Google Scholar] [CrossRef]
- Brown, A.G.; Leite, R.S.; Strauss, J.F., 3rd. Mechanisms underlying “functional” progesterone withdrawal at parturition. Ann. N. Y. Acad. Sci. 2004, 1034, 36–49. [Google Scholar] [CrossRef]
- Mesiano, S.; Chan, E.C.; Fitter, J.T.; Kwek, K.; Yeo, G.; Smith, R. Progesterone withdrawal and estrogen activation in human parturition are coordinated by progesterone receptor A expression in the myometrium. J. Clin. Endocrinol. Metab. 2002, 87, 2924–2930. [Google Scholar] [CrossRef]
- Nadeem, L.; Shynlova, O.; Matysiak-Zablocki, E.; Mesiano, S.; Dong, X.; Lye, S. Molecular evidence of functional progesterone withdrawal in human myometrium. Nat. Commun. 2016, 7, 11565. [Google Scholar] [CrossRef]
- Nadeem, L.; Shynlova, O.; Mesiano, S.; Lye, S. Progesterone Via its Type-A Receptor Promotes Myometrial Gap Junction Coupling. Sci. Rep. 2017, 7, 13357. [Google Scholar] [CrossRef]
- Hassan, S.S.; Romero, R.; Vidyadhari, D.; Fusey, S.; Baxter, J.K.; Khandelwal, M.; Vijayaraghavan, J.; Trivedi, Y.; Soma-Pillay, P.; Sambarey, P.; et al. Vaginal progesterone reduces the rate of preterm birth in women with a sonographic short cervix: A multicenter, randomized, double-blind, placebo-controlled trial. Ultrasound. Obstet. Gynecol. 2011, 38, 18–31. [Google Scholar] [CrossRef]
- Norman, J.E.; Marlow, N.; Messow, C.M.; Shennan, A.; Bennett, P.R.; Thornton, S.; Robson, S.C.; McConnachie, A.; Petrou, S.; Sebire, N.J.; et al. Vaginal progesterone prophylaxis for preterm birth (the OPPTIMUM study): A multicentre, randomised, double-blind trial. Lancet 2016, 387, 2106–2116. [Google Scholar] [CrossRef]
- O’Brien, J.M.; Adair, C.D.; Lewis, D.F.; Hall, D.R.; Defranco, E.A.; Fusey, S.; Soma-Pillay, P.; Porter, K.; How, H.; Schackis, R.; et al. Progesterone vaginal gel for the reduction of recurrent preterm birth: Primary results from a randomized, double-blind, placebo-controlled trial. Ultrasound Obstet. Gynecol. 2007, 30, 687–696. [Google Scholar] [CrossRef]
- Romero, R.; Nicolaides, K.; Conde-Agudelo, A.; Tabor, A.; O’Brien, J.M.; Cetingoz, E.; Da Fonseca, E.; Creasy, G.W.; Klein, K.; Rode, L.; et al. Vaginal progesterone in women with an asymptomatic sonographic short cervix in the midtrimester decreases preterm delivery and neonatal morbidity: A systematic review and metaanalysis of individual patient data. Am. J. Obstet. Gynecol. 2012, 206, 124.e1–124.e19. [Google Scholar] [CrossRef]
- Fonseca, E.B.; Celik, E.; Parra, M.; Singh, M.; Nicolaides, K.H.; Fetal Medicine Foundation Second Trimester Screening, G. Progesterone and the risk of preterm birth among women with a short cervix. N. Engl. J. Med. 2007, 357, 462–469. [Google Scholar] [CrossRef]
- Nelson, D.B.; McIntire, D.D.; McDonald, J.; Gard, J.; Turrichi, P.; Leveno, K.J. 17-alpha Hydroxyprogesterone caproate did not reduce the rate of recurrent preterm birth in a prospective cohort study. Am. J. Obstet. Gynecol. 2017, 216, 600.e1–600.e9. [Google Scholar] [CrossRef]
- Blackwell, S.C.; Gyamfi-Bannerman, C.; Biggio, J.R., Jr.; Chauhan, S.P.; Hughes, B.L.; Louis, J.M.; Manuck, T.A.; Miller, H.S.; Das, A.F.; Saade, G.R.; et al. 17-OHPC to Prevent Recurrent Preterm Birth in Singleton Gestations (PROLONG Study): A Multicenter, International, Randomized Double-Blind Trial. Am. J. Perinatol. 2020, 37, 127–136. [Google Scholar] [CrossRef]
- Romero, R.; Conde-Agudelo, A.; El-Refaie, W.; Rode, L.; Brizot, M.L.; Cetingoz, E.; Serra, V.; Da Fonseca, E.; Abdelhafez, M.S.; Tabor, A.; et al. Vaginal progesterone decreases preterm birth and neonatal morbidity and mortality in women with a twin gestation and a short cervix: An updated meta-analysis of individual patient data. Ultrasound Obstet. Gynecol. 2017, 49, 303–314. [Google Scholar] [CrossRef]
- Shambhavi, S.; Bagga, R.; Bansal, P.; Kalra, J.; Kumar, P. A randomised trial to compare 200 mg micronised progesterone effervescent vaginal tablet daily with 250 mg intramuscular 17 alpha hydroxy progesterone caproate weekly for prevention of recurrent preterm birth. J. Obstet. Gynaecol. 2018, 38, 800–806. [Google Scholar] [CrossRef] [PubMed]
- American College of Obstetricians and Gynecologists. Practice bulletin no. 130: Prediction and prevention of preterm birth. Obstet. Gynecol. 2012, 120, 964–973. [Google Scholar] [CrossRef] [PubMed]
- How, H.Y.; Sibai, B.M. Progesterone for the prevention of preterm birth: Indications, when to initiate, efficacy and safety. Ther. Clin. Risk Manag. 2009, 5, 55–64. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Ahn, K.H.; Bae, N.Y.; Hong, S.C.; Lee, J.S.; Lee, E.H.; Jee, H.J.; Cho, G.J.; Oh, M.J.; Kim, H.J. The safety of progestogen in the prevention of preterm birth: Meta-analysis of neonatal mortality. J. Perinat Med. 2017, 45, 11–20. [Google Scholar] [CrossRef]
- Kuon, R.J.; Shi, S.Q.; Maul, H.; Sohn, C.; Balducci, J.; Maner, W.L.; Garfield, R.E. Pharmacologic actions of progestins to inhibit cervical ripening and prevent delivery depend on their properties, the route of administration, and the vehicle. Am. J. Obstet. Gynecol. 2010, 202, 455.e1–455.e9. [Google Scholar] [CrossRef]
- Grainger, D.J.; Lever, A.M. Blockade of chemokine-induced signalling inhibits CCR5-dependent HIV infection in vitro without blocking gp120/CCR5 interaction. Retrovirology 2005, 2, 23. [Google Scholar] [CrossRef]
- Larena, M.; Regner, M.; Lobigs, M. The Chemokine Receptor CCR5, a Therapeutic Target for HIV/AIDS Antagonists, Is Critical for Recovery in a Mouse Model of Japanese Encephalitis. PLoS ONE 2012, 7, 10. [Google Scholar] [CrossRef]
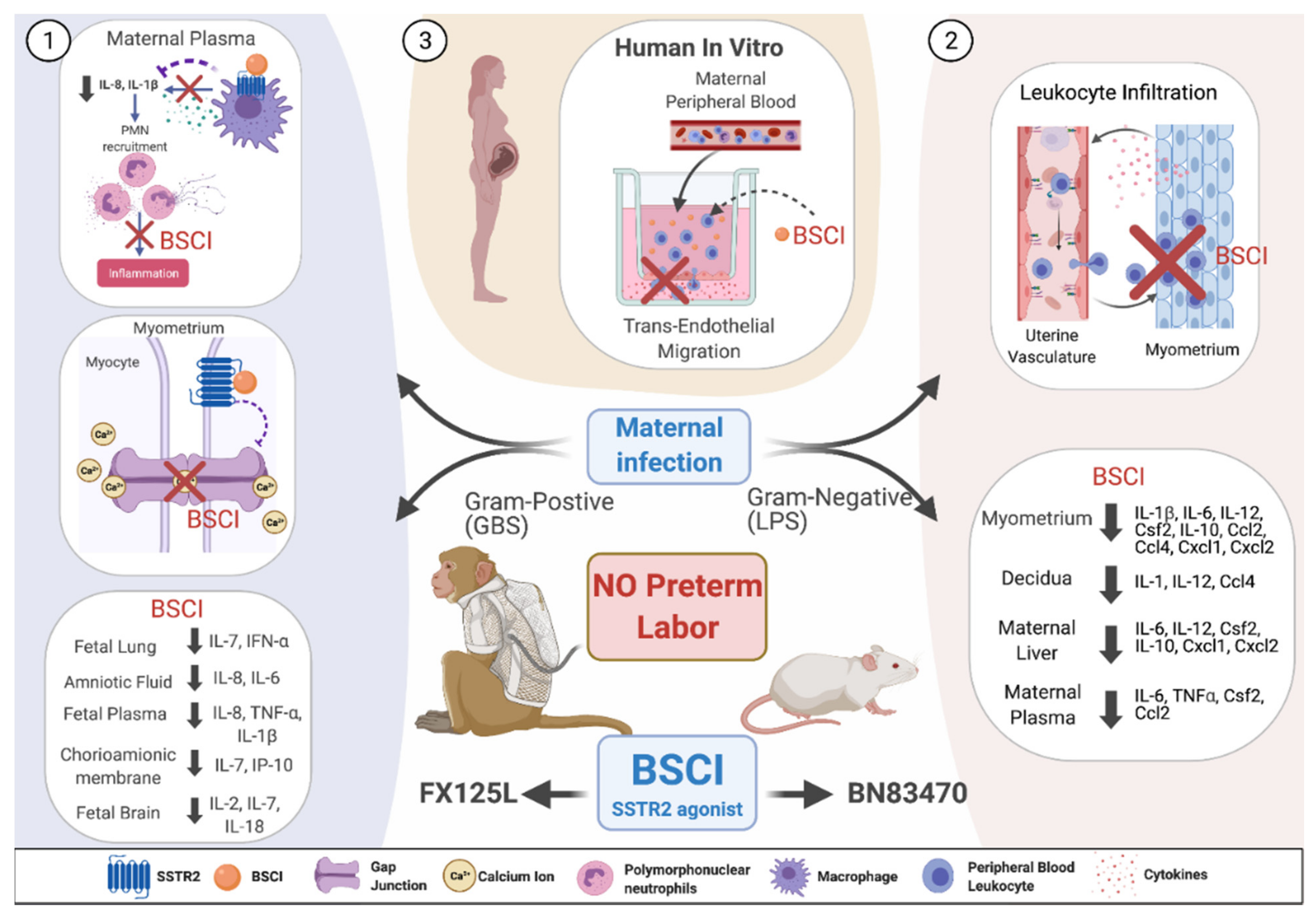
- Coleman, M.; Orvis, A.; Wu, T.Y.; Dacanay, M.; Merillat, S.; Ogle, J.; Baldessari, A.; Kretzer, N.M.; Munson, J.; Boros-Rausch, A.J.; et al. A Broad Spectrum Chemokine Inhibitor Prevents Preterm Labor but Not Microbial Invasion of the Amniotic Cavity or Neonatal Morbidity in a Non-human Primate Model. Front. Immunol. 2020, 11, 770. [Google Scholar] [CrossRef]
- Shynlova, O.; Dorogin, A.; Li, Y.; Lye, S. Inhibition of infection-mediated preterm birth by administration of broad spectrum chemokine inhibitor in mice. J. Cell Mol. Med. 2014, 18, 1816–1829. [Google Scholar] [CrossRef]
- Yuan, M.; Jordan, F.; McInnes, I.B.; Harnett, M.M.; Norman, J.E. Leukocytes are primed in peripheral blood for activation during term and preterm labour. Mol. Hum. Reprod 2009, 15, 713–724. [Google Scholar] [CrossRef]
- Thomson, A.J.; Telfer, J.F.; Young, A.; Campbell, S.; Stewart, C.J.; Cameron, I.T.; Greer, I.A.; Norman, J.E. Leukocytes infiltrate the myometrium during human parturition: Further evidence that labour is an inflammatory process. Hum. Reprod. 1999, 14, 229–236. [Google Scholar] [CrossRef]
- Shynlova, O.; Tsui, P.; Dorogin, A.; Lye, S.J. Monocyte chemoattractant protein-1 (CCL-2) integrates mechanical and endocrine signals that mediate term and preterm labor. J. Immunol. 2008, 181, 1470–1479. [Google Scholar] [CrossRef]
- Keski-Nisula, L.T.; Aalto, M.L.; Kirkinen, P.P.; Kosma, V.M.; Heinonen, S.T. Myometrial inflammation in human delivery and its association with labor and infection. Am. J. Clin. Pathol. 2003, 120, 217–224. [Google Scholar] [CrossRef]
- Singh, N.; Herbert, B.; Sooranna, G.R.; Orsi, N.M.; Edey, L.; Dasgupta, T.; Sooranna, S.R.; Yellon, S.M.; Johnson, M.R. Is myometrial inflammation a cause or a consequence of term human labour? J. Endocrinol. 2017, 235, 69–83. [Google Scholar] [CrossRef]
- Grainger, D.J.; Reckless, J. Broad-spectrum chemokine inhibitors (BSCIs) and their anti-inflammatory effects in vivo. Biochem. Pharmacol. 2003, 65, 1027–1034. [Google Scholar] [CrossRef]
- Fox, D.J.; Reckless, J.; Lingard, H.; Warren, S.; Grainger, D.J. Highly potent, orally available anti-inflammatory broad-spectrum chemokine inhibitors. J. Med. Chem. 2009, 52, 3591–3595. [Google Scholar] [CrossRef]
- Reckless, J.; Tatalick, L.; Wilbert, S.; McKilligin, E.; Grainger, D.J. Broad-spectrum chemokine inhibition reduces vascular macrophage accumulation and collagenolysis consistent with plaque stabilization in mice. J. Vasc Res. 2005, 42, 492–502. [Google Scholar] [CrossRef]
- Naidu, B.V.; Farivar, A.S.; Krishnadasan, B.; Woolley, S.M.; Grainger, D.J.; Verrier, E.D.; Mulligan, M.S. Broad-spectrum chemokine inhibition ameliorates experimental obliterative bronchiolitis. Ann. Thorac. Surg. 2003, 75, 1118–1122. [Google Scholar] [CrossRef]
- Miklos, S.; Mueller, G.; Chang, Y.; Bouazzaoui, A.; Spacenko, E.; Schubert, T.E.O.; Grainger, D.J.; Holler, E.; Andreesen, R.; Hildebrandt, G.C. Preventive usage of broad spectrum chemokine inhibitor NR58-3.14.3 reduces the severity of pulmonary and hepatic graft-versus-host disease. Int. J. Hematol. 2009, 89, 383–397. [Google Scholar] [CrossRef]
- Berkkanoglu, M.; Zhang, L.; Ulukus, M.; Cakmak, H.; Kayisli, U.A.; Kursun, S.; Arici, A. Inhibition of chemokines prevents intraperitoneal adhesions in mice. Hum. Reprod. 2005, 20, 3047–3052. [Google Scholar] [CrossRef]
- Fox, D.J.; Reckless, J.; Wilbert, S.M.; Greig, I.; Warren, S.; Grainger, D.J. Identification of 3-(acylamino)azepan-2-ones as stable broad-spectrum chemokine inhibitors resistant to metabolism in vivo. J. Med. Chem. 2005, 48, 867–874. [Google Scholar] [CrossRef] [PubMed]
- Reckless, J.; Tatalick, L.M.; Grainger, D.J. The pan-chemokine inhibitor NR58-3.14.3 abolishes tumour necrosis factor-alpha accumulation and leucocyte recruitment induced by lipopolysaccharide in vivo. Immunology 2001, 103, 244–254. [Google Scholar] [CrossRef] [PubMed]
- Elliott, D.E.; Li, J.; Blum, A.M.; Metwali, A.; Patel, Y.C.; Weinstock, J.V. SSTR2A is the dominant somatostatin receptor subtype expressed by inflammatory cells, is widely expressed and directly regulates T cell IFN-gamma release. Eur. J. Immunol. 1999, 29, 2454–2463. [Google Scholar] [CrossRef]
- Olias, G.; Viollet, C.; Kusserow, H.; Epelbaum, J.; Meyerhof, W. Regulation and function of somatostatin receptors. J. Neurochem. 2004, 89, 1057–1091. [Google Scholar] [CrossRef] [PubMed]
- Armani, C.; Catalani, E.; Balbarini, A.; Bagnoli, P.; Cervia, D. Expression, pharmacology, and functional role of somatostatin receptor subtypes 1 and 2 in human macrophages. J. Leukoc. Biol. 2007, 81, 845–855. [Google Scholar] [CrossRef] [PubMed]
- Cervia, D.; Nunn, C.; Bagnoli, P. Multiple Signalling Transduction Mechanisms Differentially Coupled to Somatostatin Receptor Subtypes: A Current View. Curr. Enzym. Inhib. 2005, 1. [Google Scholar] [CrossRef]
- Krantic, S. Peptides as regulators of the immune system: Emphasis on somatostatin. Peptides 2000, 21, 1941–1964. [Google Scholar] [CrossRef]
- Lichtenauer-Kaligis, E.G.; van Hagen, P.M.; Lamberts, S.W.; Hofland, L.J. Somatostatin receptor subtypes in human immune cells. Eur. J. Endocrinol. 2000, 143 (Suppl. 1), S21–S25. [Google Scholar] [CrossRef]
- Jana, B.; Calka, J.; Czajkowska, M. The role of somatostatin and its receptors (sstr2, sstr5) in the contractility of gilt inflamed uterus. Res. Vet. Sci. 2020, 133, 163–173. [Google Scholar] [CrossRef]
- Olson, D.M.; Ammann, C. Role of the prostaglandins in labour and prostaglandin receptor inhibitors in the prevention of preterm labour. Front. Biosci. 2007, 12, 1329–1343. [Google Scholar] [CrossRef]
- Senior, J.; Marshall, K.; Sangha, R.; Clayton, J.K. In vitro characterization of prostanoid receptors on human myometrium at term pregnancy. Br. J. Pharmacol. 1993, 108, 501–506. [Google Scholar] [CrossRef]
- Grigsby, P.L.; Sooranna, S.R.; Adu-Amankwa, B.; Pitzer, B.; Brockman, D.E.; Johnson, M.R.; Myatt, L. Regional expression of prostaglandin E2 and F2alpha receptors in human myometrium, amnion, and choriodecidua with advancing gestation and labor. Biol. Reprod. 2006, 75, 297–305. [Google Scholar] [CrossRef][Green Version]
- Ulug, U.; Goldman, S.; Ben-Shlomo, I.; Shalev, E. Matrix metalloproteinase (MMP)-2 and MMP-9 and their inhibitor, TIMP-1, in human term decidua and fetal membranes: The effect of prostaglandin F(2alpha) and indomethacin. Mol. Hum. Reprod. 2001, 7, 1187–1193. [Google Scholar] [CrossRef]
- Yoshida, M.; Sagawa, N.; Itoh, H.; Yura, S.; Takemura, M.; Wada, Y.; Sato, T.; Ito, A.; Fujii, S. Prostaglandin F(2alpha), cytokines and cyclic mechanical stretch augment matrix metalloproteinase-1 secretion from cultured human uterine cervical fibroblast cells. Mol. Hum. Reprod. 2002, 8, 681–687. [Google Scholar] [CrossRef]
- Slater, D.M.; Zervou, S.; Thornton, S. Prostaglandins and prostanoid receptors in human pregnancy and parturition. J. Soc. Gynecol. Investig. 2002, 9, 118–124. [Google Scholar] [CrossRef]
- Pohl, O.; Chollet, A.; Kim, S.H.; Riaposova, L.; Spezia, F.; Gervais, F.; Guillaume, P.; Lluel, P.; Meen, M.; Lemaux, F.; et al. OBE022, an Oral and Selective Prostaglandin F2alpha Receptor Antagonist as an Effective and Safe Modality for the Treatment of Preterm Labor. J. Pharmacol. Exp. Ther. 2018, 366, 349–364. [Google Scholar] [CrossRef]
- Pohl, O.; Marchand, L.; Gotteland, J.P.; Coates, S.; Taubel, J.; Lorch, U. Pharmacokinetics, safety and tolerability of OBE022, a selective prostaglandin F2alpha receptor antagonist tocolytic: A first-in-human trial in healthy postmenopausal women. Br. J. Clin. Pharmacol. 2018, 84, 1839–1855. [Google Scholar] [CrossRef]
- Taubel, J.; Lorch, U.; Coates, S.; Fernandes, S.; Foley, P.; Ferber, G.; Gotteland, J.P.; Pohl, O. Confirmation of the Cardiac Safety of PGF2alpha Receptor Antagonist OBE022 in a First-in-Human Study in Healthy Subjects, Using Intensive ECG Assessments. Clin. Pharmacol. Drug Dev. 2018, 7, 889–900. [Google Scholar] [CrossRef]
- Pohl, O.; Marchand, L.; Gotteland, J.P.; Coates, S.; Taubel, J.; Lorch, U. Coadministration of the prostaglandin F2alpha receptor antagonist preterm labour drug candidate OBE022 with magnesium sulfate, atosiban, nifedipine and betamethasone. Br. J. Clin. Pharmacol. 2019, 85, 1516–1527. [Google Scholar] [CrossRef]
- Romero, R.; Miranda, J.; Chaiworapongsa, T.; Korzeniewski, S.J.; Chaemsaithong, P.; Gotsch, F.; Dong, Z.; Ahmed, A.I.; Yoon, B.H.; Hassan, S.S.; et al. Prevalence and clinical significance of sterile intra-amniotic inflammation in patients with preterm labor and intact membranes. Am. J. Reprod. Immunol. 2014, 72, 458–474. [Google Scholar] [CrossRef]
- Leimert, K.B.; Messer, A.; Gray, T.; Fang, X.; Chemtob, S.; Olson, D.M. Maternal and fetal intrauterine tissue crosstalk promotes proinflammatory amplification and uterine transitiondagger. Biol. Reprod. 2019, 100, 783–797. [Google Scholar] [CrossRef]
- Leimert, K.B.; Verstraeten, B.S.E.; Messer, A.; Nemati, R.; Blackadar, K.; Fang, X.; Robertson, S.A.; Chemtob, S.; Olson, D.M. Cooperative effects of sequential PGF2alpha and IL-1beta on IL-6 and COX-2 expression in human myometrial cellsdagger. Biol. Reprod. 2019, 100, 1370–1385. [Google Scholar] [CrossRef]
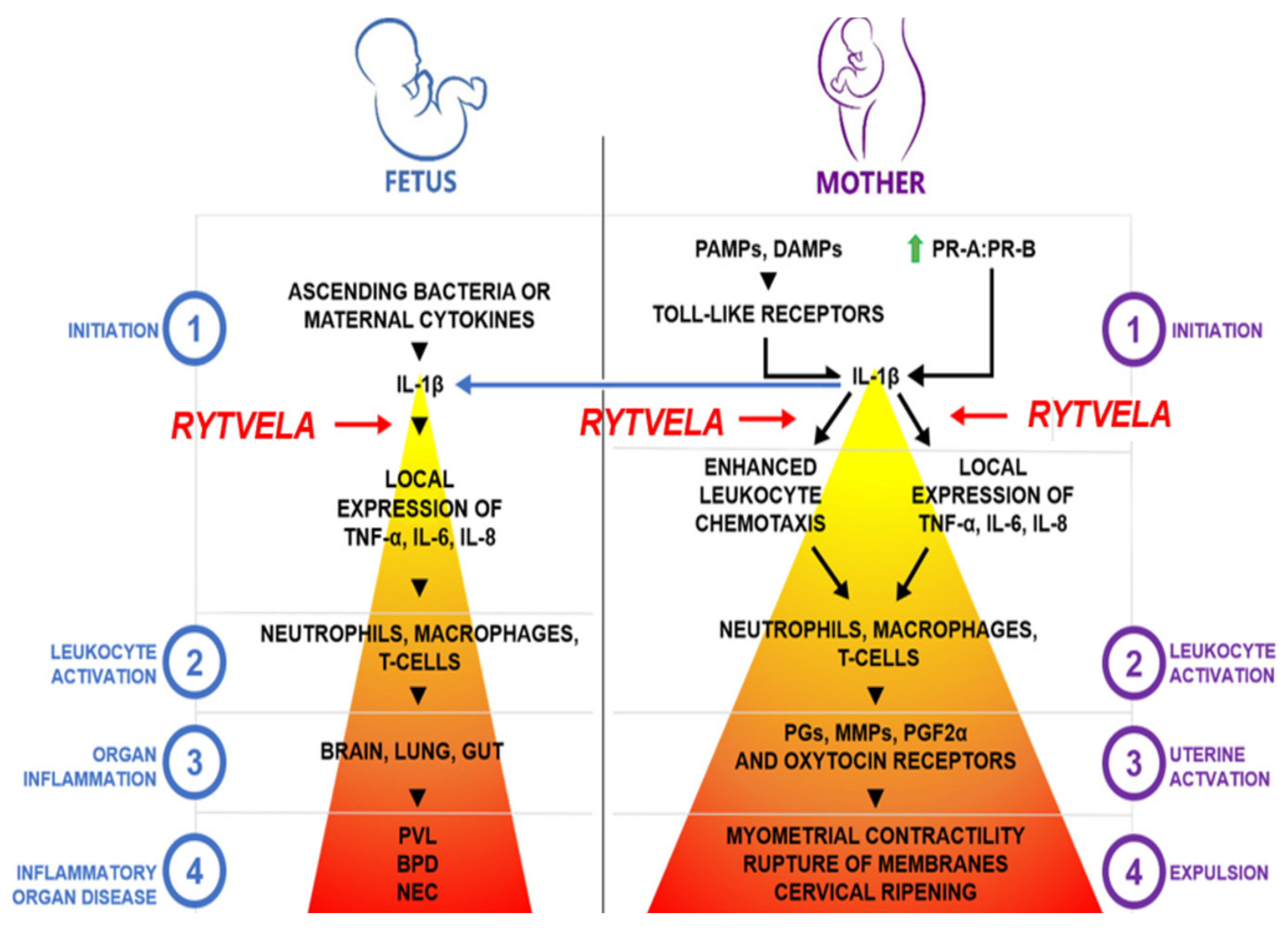
- Nadeau-Vallee, M.; Quiniou, C.; Palacios, J.; Hou, X.; Erfani, A.; Madaan, A.; Sanchez, M.; Leimert, K.; Boudreault, A.; Duhamel, F.; et al. Novel Noncompetitive IL-1 Receptor-Biased Ligand Prevents Infection- and Inflammation-Induced Preterm Birth. J. Immunol. 2015, 195, 3402–3415. [Google Scholar] [CrossRef]
- Nadeau-Vallee, M.; Chin, P.Y.; Belarbi, L.; Brien, M.E.; Pundir, S.; Berryer, M.H.; Beaudry-Richard, A.; Madaan, A.; Sharkey, D.J.; Lupien-Meilleur, A.; et al. Antenatal Suppression of IL-1 Protects against Inflammation-Induced Fetal Injury and Improves Neonatal and Developmental Outcomes in Mice. J. Immunol. 2017, 198, 2047–2062. [Google Scholar] [CrossRef]
- Sadowsky, D.W.; Adams, K.M.; Gravett, M.G.; Witkin, S.S.; Novy, M.J. Preterm labor is induced by intraamniotic infusions of interleukin-1beta and tumor necrosis factor-alpha but not by interleukin-6 or interleukin-8 in a nonhuman primate model. Am. J. Obstet. Gynecol. 2006, 195, 1578–1589. [Google Scholar] [CrossRef]
- Leitner, K.; Al Shammary, M.; McLane, M.; Johnston, M.V.; Elovitz, M.A.; Burd, I. IL-1 receptor blockade prevents fetal cortical brain injury but not preterm birth in a mouse model of inflammation-induced preterm birth and perinatal brain injury. Am. J. Reprod. Immunol. 2014, 71, 418–426. [Google Scholar] [CrossRef]
- Fidel, P.L., Jr.; Romero, R.; Cutright, J.; Wolf, N.; Gomez, R.; Araneda, H.; Ramirez, M.; Yoon, B.H. Treatment with the interleukin-I receptor antagonist and soluble tumor necrosis factor receptor Fc fusion protein does not prevent endotoxin-induced preterm parturition in mice. J. Soc. Gynecol. Investig. 1997, 4, 22–26. [Google Scholar] [CrossRef]
- Kallapur, S.G.; Nitsos, I.; Moss, T.J.; Polglase, G.R.; Pillow, J.J.; Cheah, F.C.; Kramer, B.W.; Newnham, J.P.; Ikegami, M.; Jobe, A.H. IL-1 mediates pulmonary and systemic inflammatory responses to chorioamnionitis induced by lipopolysaccharide. Am. J. Respir. Crit. Care Med. 2009, 179, 955–961. [Google Scholar] [CrossRef]
- Boonkasidecha, S.; Kannan, P.S.; Kallapur, S.G.; Jobe, A.H.; Kemp, M.W. Fetal skin as a pro-inflammatory organ: Evidence from a primate model of chorioamnionitis. PLoS ONE 2017, 12, e0184938. [Google Scholar] [CrossRef]
- Presicce, P.; Park, C.W.; Senthamaraikannan, P.; Bhattacharyya, S.; Jackson, C.; Kong, F.; Rueda, C.M.; DeFranco, E.; Miller, L.A.; Hildeman, D.A.; et al. IL-1 signaling mediates intrauterine inflammation and chorio-decidua neutrophil recruitment and activation. JCI Insight 2018, 3. [Google Scholar] [CrossRef]
- Romero, R.; Sepulveda, W.; Mazor, M.; Brandt, F.; Cotton, D.B.; Dinarello, C.A.; Mitchell, M.D. The natural interleukin-1 receptor antagonist in term and preterm parturition. Am. J. Obstet. Gynecol. 1992, 167, 863–872. [Google Scholar] [CrossRef]
- Girard, S.; Sebire, G. Transplacental Transfer of Interleukin-1 Receptor Agonist and Antagonist Following Maternal Immune Activation. Am. J. Reprod. Immunol. 2016, 75, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, C.; Knight, A.; Nordstrom, D.; Pettersson, T.; Fransson, J.; Florin-Robertsson, E.; Pilstrom, B. Injection-site reactions upon Kineret (anakinra) administration: Experiences and explanations. Rheumatol. Int. 2012, 32, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Dhimolea, E. Canakinumab. MAbs 2010, 2, 3–13. [Google Scholar] [CrossRef]
- Christopoulos, A.; May, L.T.; Avlani, V.A.; Sexton, P.M. G-protein-coupled receptor allosterism: The promise and the problem(s). Biochem. Soc. Trans. 2004, 32, 873–877. [Google Scholar] [CrossRef]
- Terrillon, S.; Bouvier, M. Roles of G-protein-coupled receptor dimerization. EMBO Rep. 2004, 5, 30–34. [Google Scholar] [CrossRef]
- Kenakin, T. Allosteric modulators: The new generation of receptor antagonist. Mol. Interv. 2004, 4, 222–229. [Google Scholar] [CrossRef]
- Kubatzky, K.F.; Liu, W.; Goldgraben, K.; Simmerling, C.; Smith, S.O.; Constantinescu, S.N. Structural requirements of the extracellular to transmembrane domain junction for erythropoietin receptor function. J. Biol. Chem. 2005, 280, 14844–14854. [Google Scholar] [CrossRef]
- Remy, I.; Wilson, I.A.; Michnick, S.W. Erythropoietin receptor activation by a ligand-induced conformation change. Science 1999, 283, 990–993. [Google Scholar] [CrossRef]
- Quiniou, C.; Sapieha, P.; Lahaie, I.; Hou, X.; Brault, S.; Beauchamp, M.; Leduc, M.; Rihakova, L.; Joyal, J.S.; Nadeau, S.; et al. Development of a novel noncompetitive antagonist of IL-1 receptor. J. Immunol. 2008, 180, 6977–6987. [Google Scholar] [CrossRef]
- Gillingham, A.K.; Munro, S. The small G proteins of the Arf family and their regulators. Annu. Rev. Cell Dev. Biol. 2007, 23, 579–611. [Google Scholar] [CrossRef]
- Singh, R.; Wang, B.; Shirvaikar, A.; Khan, S.; Kamat, S.; Schelling, J.R.; Konieczkowski, M.; Sedor, J.R. The IL-1 receptor and Rho directly associate to drive cell activation in inflammation. J. Clin. Investig. 1999, 103, 1561–1570. [Google Scholar] [CrossRef]
- Thumkeo, D.; Watanabe, S.; Narumiya, S. Physiological roles of Rho and Rho effectors in mammals. Eur. J. Cell Biol. 2013, 92, 303–315. [Google Scholar] [CrossRef]
- Quiniou, C.; Kooli, E.; Joyal, J.S.; Sapieha, P.; Sennlaub, F.; Lahaie, I.; Shao, Z.; Hou, X.; Hardy, P.; Lubell, W.; et al. Interleukin-1 and ischemic brain injury in the newborn: Development of a small molecule inhibitor of IL-1 receptor. Semin. Perinatol. 2008, 32, 325–333. [Google Scholar] [CrossRef]
- Rivera, J.C.; Sitaras, N.; Noueihed, B.; Hamel, D.; Madaan, A.; Zhou, T.; Honore, J.C.; Quiniou, C.; Joyal, J.S.; Hardy, P.; et al. Microglia and interleukin-1beta in ischemic retinopathy elicit microvascular degeneration through neuronal semaphorin-3A. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1881–1891. [Google Scholar] [CrossRef]
- Dabouz, R.; Cheng, C.W.H.; Abram, P.; Omri, S.; Cagnone, G.; Sawmy, K.V.; Joyal, J.S.; Desjarlais, M.; Olson, D.; Weil, A.G.; et al. An allosteric interleukin-1 receptor modulator mitigates inflammation and photoreceptor toxicity in a model of retinal degeneration. J. Neuroinflamm. 2020, 17, 359. [Google Scholar] [CrossRef]
- Hamel, D.; Sanchez, M.; Duhamel, F.; Roy, O.; Honore, J.C.; Noueihed, B.; Zhou, T.; Nadeau-Vallee, M.; Hou, X.; Lavoie, J.C.; et al. G-Protein-Coupled Receptor 91 and Succinate Are Key Contributors in Neonatal Postcerebral Hypoxia-Ischemia Recovery. Arterioscler. Thromb. Vasc. Biol. 2013. [Google Scholar] [CrossRef]
- Honore, J.C.; Kooli, A.; Hamel, D.; Alquier, T.; Rivera, J.C.; Quiniou, C.; Hou, X.; Kermorvant-Duchemin, E.; Hardy, P.; Poitout, V.; et al. Fatty acid receptor Gpr40 mediates neuromicrovascular degeneration induced by transarachidonic acids in rodents. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 954–961. [Google Scholar] [CrossRef]
- Sirinyan, M.; Sennlaub, F.; Dorfman, A.; Sapieha, P.; Gobeil, F., Jr.; Hardy, P.; Lachapelle, P.; Chemtob, S. Hyperoxic exposure leads to nitrative stress and ensuing microvascular degeneration and diminished brain mass and function in the immature subject. Stroke 2006, 37, 2807–2815. [Google Scholar] [CrossRef]
- Beaudry-Richard, A.; Nadeau-Vallee, M.; Prairie, E.; Maurice, N.; Heckel, E.; Nezhady, M.; Pundir, S.; Madaan, A.; Boudreault, A.; Hou, X.; et al. Author Correction: Antenatal IL-1-dependent inflammation persists postnatally and causes retinal and sub-retinal vasculopathy in progeny. Sci. Rep. 2020, 10, 6634. [Google Scholar] [CrossRef]
- Saltzman, W.M.; Torchilin, V.P. Drug delivery systems. AccessScience 2018. [Google Scholar] [CrossRef]
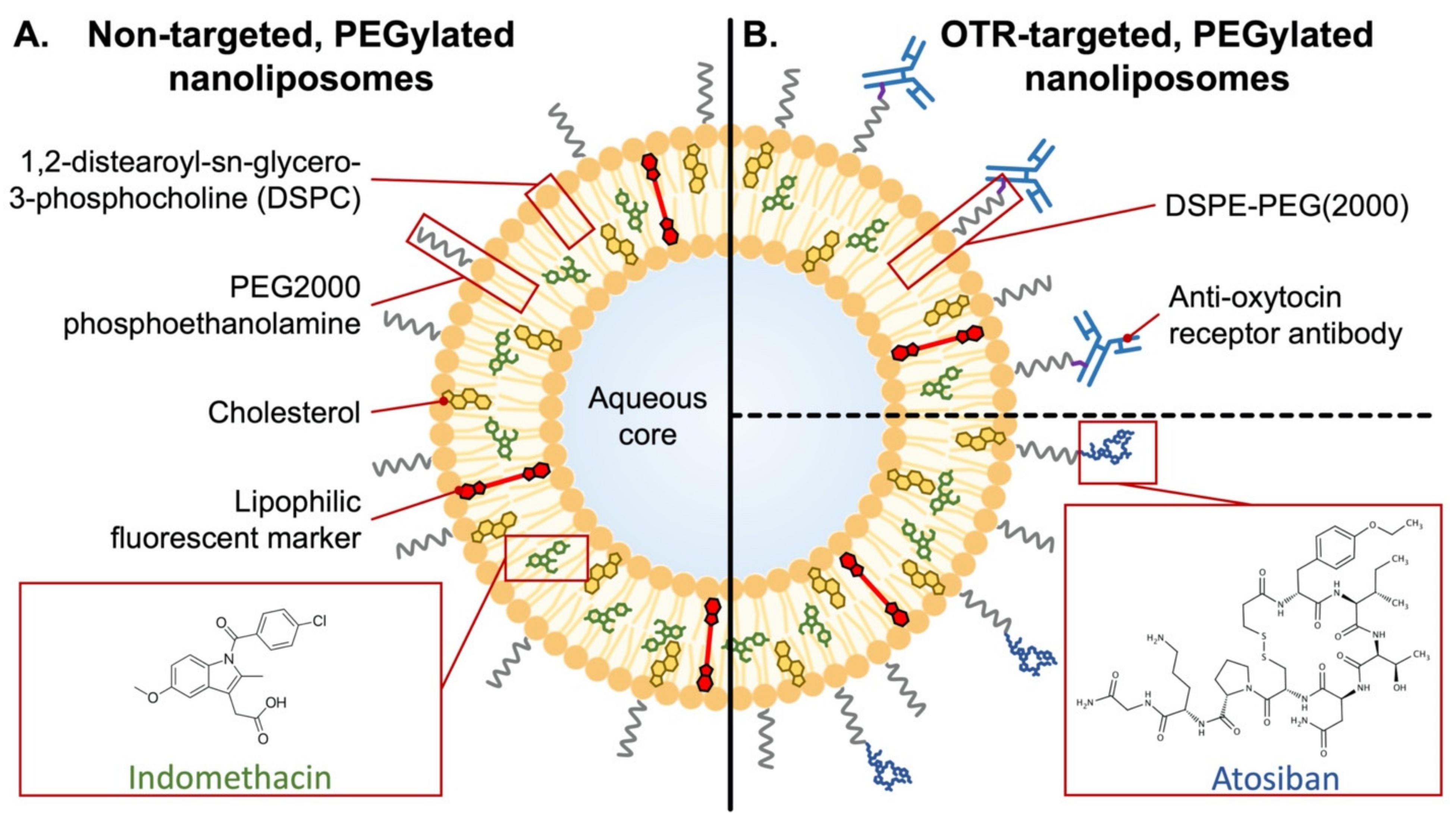
- Refuerzo, J.S.; Alexander, J.F.; Leonard, F.; Leon, M.; Longo, M.; Godin, B. Liposomes: A nanoscale drug carrying system to prevent indomethacin passage to the fetus in a pregnant mouse model. Am. J. Obstet. Gynecol. 2015, 212, 508.e1–508.e7. [Google Scholar] [CrossRef]
- Dutta, E.H.; Behnia, F.; Harirah, H.; Costantine, M.; Saade, G. Perinatal Outcomes after Short versus Prolonged Indomethacin for Tocolysis in Women with Preterm Labor. Am. J. Perinatol. 2016, 33, 844–848. [Google Scholar] [CrossRef]
- Moise, K.J., Jr.; Ou, C.N.; Kirshon, B.; Cano, L.E.; Rognerud, C.; Carpenter, R.J., Jr. Placental transfer of indomethacin in the human pregnancy. Am. J. Obstet. Gynecol. 1990, 162, 549–554. [Google Scholar] [CrossRef]
- Paul, J.; Hua, S.; Smith, R. A Targeted Drug Delivery System for the Uterus. Reprod. Sci. 2015, 22, 57A. [Google Scholar]
- Fuchs, A.R.; Fuchs, F.; Husslein, P.; Soloff, M.S. Oxytocin receptors in the human uterus during pregnancy and parturition. Am. J. Obstet. Gynecol. 1984, 150, 734–741. [Google Scholar] [CrossRef]
- Wathes, D.C.; Borwick, S.C.; Timmons, P.M.; Leung, S.T.; Thornton, S. Oxytocin receptor expression in human term and preterm gestational tissues prior to and following the onset of labour. J. Endocrinol. 1999, 161, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Parkington, H.C.; Stevenson, J.; Tonta, M.A.; Paul, J.; Butler, T.; Maiti, K.; Chan, E.C.; Sheehan, P.M.; Brennecke, S.P.; Coleman, H.A.; et al. Diminished hERG K+ channel activity facilitates strong human labour contractions but is dysregulated in obese women. Nat. Commun. 2014, 5, 4108. [Google Scholar] [CrossRef]
- Paul, J.W.; Hua, S.; Ilicic, M.; Tolosa, J.M.; Butler, T.; Robertson, S.; Smith, R. Drug delivery to the human and mouse uterus using immunoliposomes targeted to the oxytocin receptor. Am. J. Obstet. Gynecol. 2017, 216, 283.e1–283.e14. [Google Scholar] [CrossRef]
- Refuerzo, J.S.; Leonard, F.; Bulayeva, N.; Gorenstein, D.; Chiossi, G.; Ontiveros, A.; Longo, M.; Godin, B. Uterus-targeted liposomes for preterm labor management: Studies in pregnant mice. Sci. Rep. 2016, 6, 34710. [Google Scholar] [CrossRef]
- Hua, S.; Vaughan, B. In vitro comparison of liposomal drug delivery systems targeting the oxytocin receptor: A potential novel treatment for obstetric complications. Int. J. Nanomed. 2019, 14, 2191–2206. [Google Scholar] [CrossRef]
- De Ziegler, D.; Bulletti, C.; De Monstier, B.; Jääskeläinen, A.S. The first uterine pass effect. Ann. N. Y. Acad. Sci. 1997, 828, 291–299. [Google Scholar] [CrossRef]
- Ensign, L.M.; Tang, B.C.; Wang, Y.Y.; Tse, T.A.; Hoen, T.; Cone, R.; Hanes, J. Mucus-penetrating nanoparticles for vaginal drug delivery protect against herpes simplex virus. Sci. Transl. Med. 2012, 4, 138ra179. [Google Scholar] [CrossRef]
- Hoang, T.; Zierden, H.; Date, A.; Ortiz, J.; Gumber, S.; Anders, N.; He, P.; Segars, J.; Hanes, J.; Mahendroo, M.; et al. Development of a mucoinert progesterone nanosuspension for safer and more effective prevention of preterm birth. J. Control. Release 2019, 295, 74–86. [Google Scholar] [CrossRef]
- Zierden, H.C.; Ortiz, J.I.; DeLong, K.; Yu, J.; Li, G.; Dimitrion, P.; Bensouda, S.; Laney, V.; Bailey, A.; Anders, N.M.; et al. Enhanced drug delivery to the reproductive tract using nanomedicine reveals therapeutic options for prevention of preterm birth. Sci. Transl. Med. 2021, 13. [Google Scholar] [CrossRef]
- Vyas, V.; Ashby, C.R., Jr.; Olgun, N.S.; Sundaram, S.; Salami, O.; Munnangi, S.; Pekson, R.; Mahajan, P.; Reznik, S.E. Inhibition of sphingosine kinase prevents lipopolysaccharide-induced preterm birth and suppresses proinflammatory responses in a murine model. Am. J. Pathol. 2015, 185, 862–869. [Google Scholar] [CrossRef]
- Giusto, K.; Patki, M.; Koya, J.; Ashby, C.R., Jr.; Munnangi, S.; Patel, K.; Reznik, S.E. A vaginal nanoformulation of a SphK inhibitor attenuates lipopolysaccharide-induced preterm birth in mice. Nanomedicine 2019, 14, 2835–2851. [Google Scholar] [CrossRef]
- Rani, S.; Rana, R.; Saraogi, G.K.; Kumar, V.; Gupta, U. Self-Emulsifying Oral Lipid Drug Delivery Systems: Advances and Challenges. AAPS PharmSciTech 2019, 20, 129. [Google Scholar] [CrossRef]
- Washington, H.A. Medical Apartheid: The Dark History of Medical Experimentation on Black Americans from Colonial Times to the Present; First Anchor Books: New York, NY, USA, 2006. [Google Scholar]
- Turner, M.A.; Davis, J.M.; McCune, S.; Bax, R.; Portman, R.J.; Hudson, L.D. The International Neonatal Consortium: Collaborating to advance regulatory science for neonates. Pediatr Res. 2016, 80, 462–464. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Therapeutic | Route | Mechanism of Action | Stage of Development | Side Effects | Other Notes |
|---|---|---|---|---|---|
| Terbutaline (Bricanyl, Marex) | oral, IV | beta-2 adrenergic agonist | clinical use | Tremor, shakiness | |
| Atosiban (Tractocile, Antocin) | IV | oxytocin and vasopressin antagonist | clinical use | Nausea, vomiting, headache | |
| Nifedipine (Procardia, Adalat, Afeditab) | oral | calcium channel blocker | clinical use | Headache, flushing, constipation | |
| Antibiotics | oral, IV | dependent on the bacterial target | clinical use | Depends on antibiotic type | Used after PPROM |
| Aspirin 1 | oral | COX inhibitor | clinical use | Rash, peptic ulcers, abdominal pain, nausea | |
| Makena® (hydroxypro-gesterone caproate) 2 | IM | 17-OH-Progesterone | clinical use | Itching, nausea, diarrhea, injection site reaction | |
| OBE022 (Ebopiprant) | oral | prostaglandin receptor antagonist | Phase II | Headache, constipation | |
| Rytvela | IV, SC | IL-1 receptor allosteric modulator | pre-clinical | None noted in mothers or offspring | None noted in mothers or offspring |
| Kineret® (Anakinra) | SC | IL-1 receptor antagonist | clinically approved | Injection site reaction, immune suppression (increased infection risk) | Not approved (or used) to prevent preterm birth |
| BSCI | IV | SSTR2 | pre-clinical | ||
| Immunoliposome |
| Company | Study (Type) | Drug | n, Target Population | Design | Primary Endpoint | Findings |
|---|---|---|---|---|---|---|
| AMAG | MEIS P2 | Makena (17-OHP) | n = 463 16–21 week with history of PTB | RCT (US multi-center) | Reduction of PTB (<37 week, <35 week, <32 week) | PTB RR 0.66, 0.67, 0.58; Cl 0.54–0.81, 0.48–0.93, 0.37–0.91 |
| AMAG | PROLONG P3 | Makena (17-OHP) | n = 1708 16–21 week with history of PTB | RCT (international multi-center) | Reduction of PTB (<35 week), neonatal morbidity | No reduction in PTB or neonatal morbidity PTB RR 0.95, Cl 0.71, 1.26 |
| ObsEva | TERM P2 | OBE-001 (oxytocin receptor antagonist) | n = 10 34–36 week with PRETERM LABOR | RCT | Incidence of delivery within 7 days | terminated |
| ObsEva | PROLONG P2 | OBE-022 (PGF2α receptor) | n = 120 28–34 week with PRETERM LABOR | RCT | Delivery < 2 days, Delivery < 7 days, delivery < 37 week, time to delivery | ongoing |
| GSK | P2 | Retosiban (oxytocin receptor antagonist) | n = 64 30–35 week with PRETERM LABOR | RCT | Resolution of contractions | terminated |
| Ferring Pharma | P2 | Barusiban (oxytocin receptor antagonist) | n = 163 34–36 week with PRETERM LABOR | RCT | Delivery within 48 h | No reduction in delivery within 48 h |
| Lipocine | P3 | LPCN1107 (oral 17-OHP) | n = 1100 | RCT 17OHP oral vs. IM | Reduction of PTB < 37 week | ongoing |
| Hadassah Medical Organization | P2 | Indomethacin | n = 300 24–32 week with PRETERM LABOR | RCT Indometh vs. nifedipine | Time to delivery, GA at delivery | proposed |
| University of Hong Kong | P3 | Oral dydrogesterone | n = 1714 <14 week | RCT | Rate of PTB < 37 week | ongoing |
| NICHD | ASPIRIN | Oral Aspirin | n = 11,976 6–14 week | RCT (international multi-center) | Rate of PTB < 37 week | PTB RR 0.89, Cl 0.81–0.98 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Coler, B.S.; Shynlova, O.; Boros-Rausch, A.; Lye, S.; McCartney, S.; Leimert, K.B.; Xu, W.; Chemtob, S.; Olson, D.; Li, M.; et al. Landscape of Preterm Birth Therapeutics and a Path Forward. J. Clin. Med. 2021, 10, 2912. https://doi.org/10.3390/jcm10132912
Coler BS, Shynlova O, Boros-Rausch A, Lye S, McCartney S, Leimert KB, Xu W, Chemtob S, Olson D, Li M, et al. Landscape of Preterm Birth Therapeutics and a Path Forward. Journal of Clinical Medicine. 2021; 10(13):2912. https://doi.org/10.3390/jcm10132912
Chicago/Turabian StyleColer, Brahm Seymour, Oksana Shynlova, Adam Boros-Rausch, Stephen Lye, Stephen McCartney, Kelycia B. Leimert, Wendy Xu, Sylvain Chemtob, David Olson, Miranda Li, and et al. 2021. "Landscape of Preterm Birth Therapeutics and a Path Forward" Journal of Clinical Medicine 10, no. 13: 2912. https://doi.org/10.3390/jcm10132912
APA StyleColer, B. S., Shynlova, O., Boros-Rausch, A., Lye, S., McCartney, S., Leimert, K. B., Xu, W., Chemtob, S., Olson, D., Li, M., Huebner, E., Curtin, A., Kachikis, A., Savitsky, L., Paul, J. W., Smith, R., & Adams Waldorf, K. M. (2021). Landscape of Preterm Birth Therapeutics and a Path Forward. Journal of Clinical Medicine, 10(13), 2912. https://doi.org/10.3390/jcm10132912