
Usefulness of the Novel Snare-over-the-Guidewire Method for Transpapillary Plastic Stent Replacement (with Video)


 , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Ethical Considerations
2.2. Patients
2.3. ERCP
2.4. Endoscopic Replacement of Transpapillary Biliary PS
2.5. Outcome Definitions
2.6. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Comparison of Procedural Success Rates between the SOG and SOS Groups
3.3. Comparison of the Time Required for PS Removal and Adverse Event Incidence Rate between the SOG and SOS Groups
3.4. Univariate and Multivariate Analyses of Predictors for Unsuccessful PS Replacement
4. Discussion
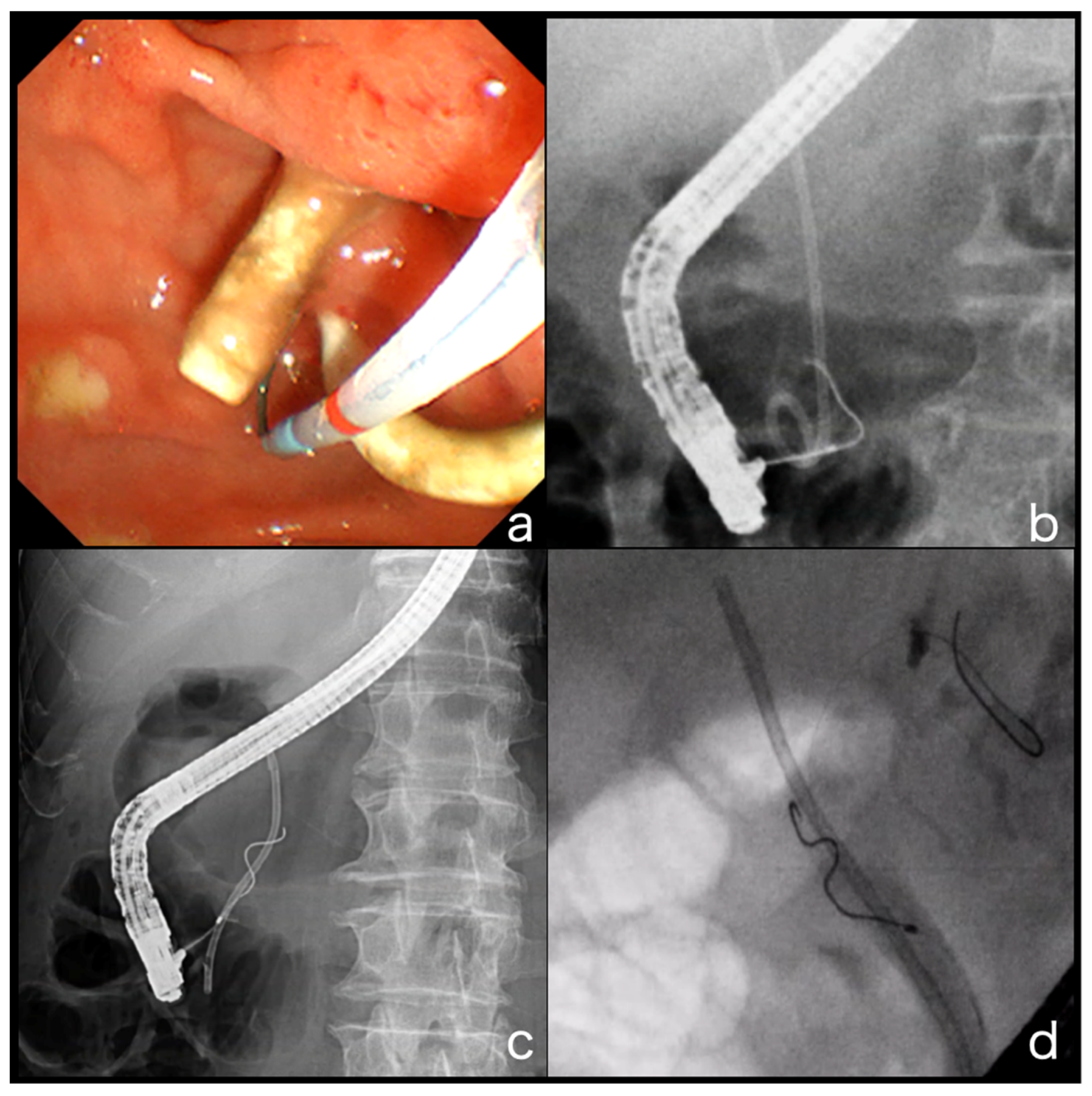
4.1. GW Insertion into the Bile Duct Where the PS Is Inserted
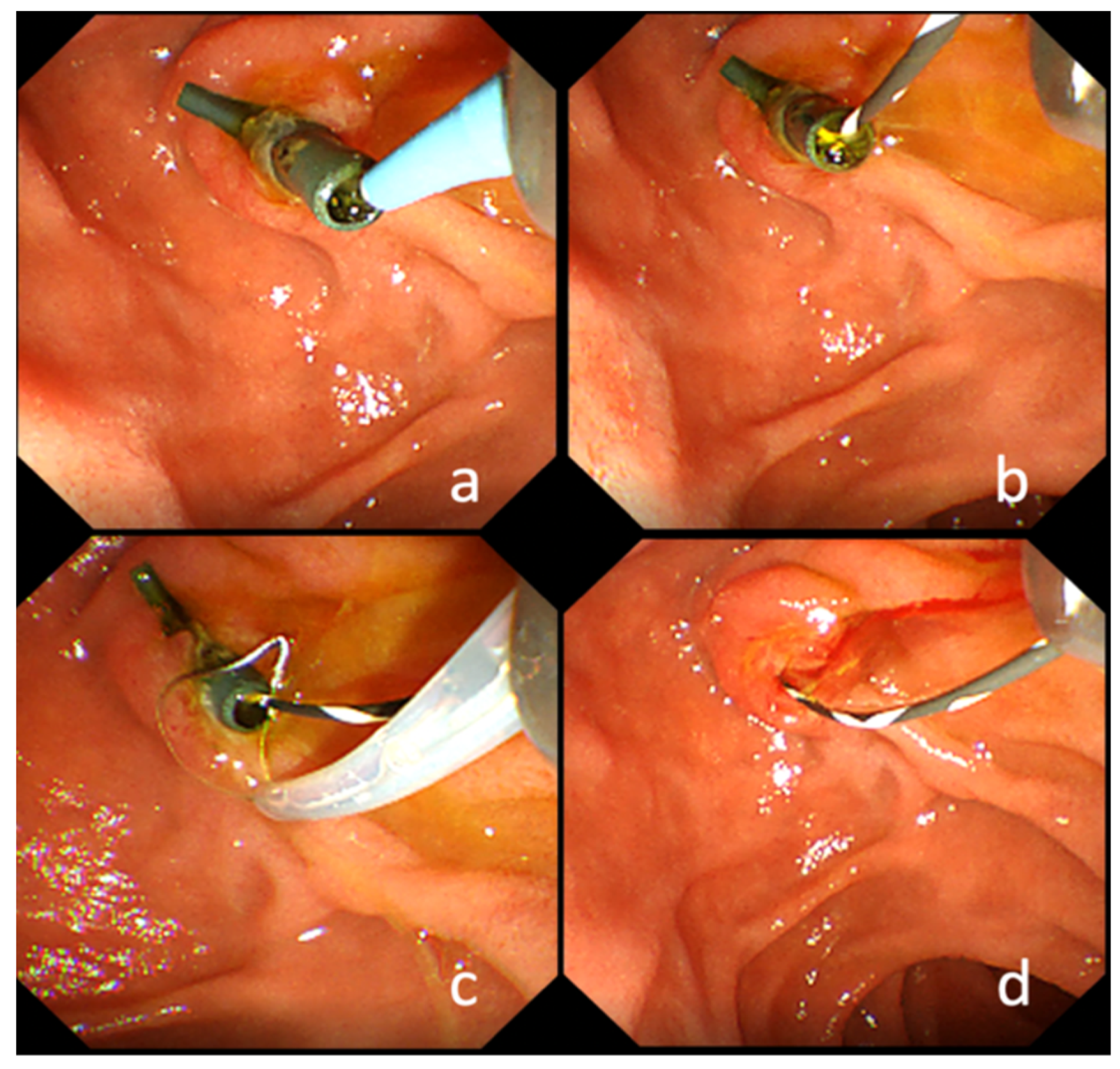
4.2. PS Removal While Leaving the GW
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Artifon, E.L.; Sakai, P.; Cunha, J.E.M.; Dupont, A.; Maluf-Filho, F.; Hondo, F.Y.; Ishioka, S.; Raju, G.S. Surgery or Endoscopy for Palliation of Biliary Obstruction Due to Metastatic Pancreatic Cancer. Am. J. Gastroenterol. 2006, 101, 2031–2037. [Google Scholar] [CrossRef]
- Bergman, J.J.; Rauws, E.A.; Tijssen, J.G.; Tytgat, G.N.; Huibregtse, K. Biliary endoprostheses in elderly patients with endoscopically irretrievable common bile duct stones: Report on 117 patients. Gastrointest. Endosc. 1995, 42, 195–201. [Google Scholar] [CrossRef]
- Misra, S.P.; Dwivedi, M. Biliary Endoprosthesis as an Alternative to Endoscopic Nasobiliary Drainage in Patients with Acute Cholangitis. Endoscopy 1996, 28, 746–749. [Google Scholar] [CrossRef] [PubMed]
- Navicharern, P.; Rhodes, M.; Floor, D.; Lawrie, B. Endoscopic Retrograde Cholangiopancreatography (Ercp) and Stent Placement in the Management of Large Common Bile Duct Stones. ANZ J. Surg. 1994, 64, 840–842. [Google Scholar] [CrossRef]
- Shepherd, H.A.; Royle, G.; Ross, A.P.R.; Diba, A.; Arthur, M.; Colin-Jones, D. Endoscopic biliary endoprosthesis in the palliation of malignant obstruction of the distal common bile duct: A randomized trial. BJS 2005, 75, 1166–1168. [Google Scholar] [CrossRef]
- Somogyi, L.; Chuttani, R.; Croffie, J.; DiSario, J.; Liu, J.; Mishkin, D.S.; Shah, R.; Tierney, W.; Song, L.M.W.K.; Petersen, B.T. Biliary and pancreatic stents. Gastrointest. Endosc. 2006, 63, 910–919. [Google Scholar] [CrossRef] [PubMed]
- Soehendra, N.; Reynders-Frederix, V. Palliative Bile Duct Drainage - A New Endoscopic Method of Introducing a Transpapillary Drain. Endoscopy 1980, 12, 8–11. [Google Scholar] [CrossRef]
- Almadi, M.; Barkun, A.; Martel, M. Plastic vs. Self-Expandable Metal Stents for Palliation in Malignant Biliary Obstruction: A Series of Meta-Analyses. Am. J. Gastroenterol. 2017, 112, 260–273. [Google Scholar] [CrossRef] [PubMed]
- Davids, P.; Groen, A.; Rauws, E.; Tytgat, G.; Huibregtse, K. Randomised trial of self-expanding metal stents versus polyethylene stents for distal malignant biliary obstruction. Lancet 1992, 340, 1488–1492. [Google Scholar] [CrossRef]
- Isayama, H.; Yasuda, I.; Ryozawa, S.; Maguchi, H.; Igarashi, Y.; Matsuyama, Y.; Katanuma, A.; Hasebe, O.; Irisawa, A.; Itoi, T.; et al. Results of a Japanese Multicenter, Randomized Trial of Endoscopic Stenting for Non-Resectable Pancreatic Head Cancer (Jm-Test): Covered Wallstent Versus Doublelayer Stent. Dig. Endosc. 2011, 23, 310–315. [Google Scholar] [CrossRef]
- Lammer, J.; A Hausegger, K.; Fluckiger, F.; Winkelbauer, F.W.; Wildling, R.; Klein, G.E.; Thurnher, S.A.; Havelec, L. Common bile duct obstruction due to malignancy: Treatment with plastic versus metal stents. Radiology 1996, 201, 167–172. [Google Scholar] [CrossRef]
- Moses, P.L.; AlNaamani, K.M.; Barkun, A.N.; Gordon, S.R.; Mitty, R.D.; Branch, M.S.; E Kowalski, T.; Martel, M.; Adam, V. Randomized trial in malignant biliary obstruction: Plastic vs partially covered metal stents. World J. Gastroenterol. 2013, 19, 8638–8646. [Google Scholar] [CrossRef]
- Soderlund, C.; Linder, S. Covered metal versus plastic stents for malignant common bile duct stenosis: A prospective, randomized, controlled trial. Gastrointest. Endosc. 2006, 63, 986–995. [Google Scholar] [CrossRef] [PubMed]
- Mukai, T.; Yasuda, I.; Nakashima, M.; Doi, S.; Iwashita, T.; Iwata, K.; Kato, T.; Tomita, E.; Moriwaki, H. Metallic stents are more efficacious than plastic stents in unresectable malignant hilar biliary strictures: A randomized controlled trial. J. Hepato-Biliary-Pancreat. Sci. 2012, 20, 214–222. [Google Scholar] [CrossRef] [PubMed]
- Goldstein, D.; El-Maraghi, R.H.; Hammel, P.; Heinemann, V.; Kunzmann, V.; Sastre, J.; Scheithauer, W.; Siena, S.; Tabernero, J.; Teixeira, L.; et al. nab-Paclitaxel Plus Gemcitabine for Metastatic Pancreatic Cancer: Long-Term Survival from a Phase III Trial. J. Natl. Cancer Inst. 2015, 107–413. [Google Scholar] [CrossRef] [PubMed]
- Valle, J.; Wasan, H.; Palmer, D.H.; Cunningham, D.; Anthoney, A.; Maraveyas, A.; Madhusudan, S.; Iveson, T.; Hughes, S.; Pereira, S.P.; et al. Cisplatin plus Gemcitabine versus Gemcitabine for Biliary Tract Cancer. N. Engl. J. Med. 2010, 362, 1273–1281. [Google Scholar] [CrossRef] [Green Version]
- Von Hoff, D.D.; Ervin, T.; Arena, F.P.; Chiorean, E.G.; Infante, J.; Moore, M.; Seay, T.; Tjulandin, S.A.; Ma, W.W.; Saleh, M.N.; et al. Increased Survival in Pancreatic Cancer with nab-Paclitaxel plus Gemcitabine. N. Engl. J. Med. 2013, 369, 1691–1703. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.K.W.; Guo, H.; Cheng, S.; Beca, J.M.; Redmond-Misner, R.; Isaranuwatchai, W.; Qiao, L.; Earle, C.; Berry, S.R.; Biagi, J.J.; et al. Real-world outcomes of FOLFIRINOX vs gemcitabine and nab-paclitaxel in advanced pancreatic cancer: A population-based propensity score-weighted analysis. Cancer Med. 2019, 9, 160–169. [Google Scholar] [CrossRef]
- Costamagna, G.; Pandolfi, M. Endoscopic Stenting for Biliary and Pancreatic Malignancies. J. Clin. Gastroenterol. 2004, 38, 59–67. [Google Scholar] [CrossRef]
- Levy, M.J.; Baron, T.H.; Gostout, C.J.; Petersen, B.T.; Farnell, M.B. Palliation of malignant extrahepatic biliary obstruction with plastic versus expandable metal stents: An evidence-based approach. Clin. Gastroenterol. Hepatol. 2004, 2, 273–285. [Google Scholar] [CrossRef]
- Fujita, N.; Sugawara, T.; Noda, Y.; Kobayashi, G.; Ito, K.; Obana, T.; Horaguchi, J.; Takasawa, O. Snare-Over-The-Wire Technique for Safe Exchange of a Stent Following Endosonography-Guided Biliary Drainage. Dig. Endosc. 2009, 21, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Takenaka, M.; Fujita, T.; Sugiyama, D.; Masuda, A.; Shiomi, H.; Sugimoto, M.; Sanuki, T.; Hayakumo, T.; Azuma, T.; Kutsumi, H. What is the most adapted indication of prophylactic pancreatic duct stent within the high-risk group of post-endoscopic retrograde cholangiopancreatography pancreatitis? Using the propensity score analysis. J. Hepato-Biliary-Pancreat. Sci. 2013, 21, 275–280. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
{kind=link}
{kind=link}
| SOG Group (n = 61) | SOS Group (n = 183) | p-Value | |
|---|---|---|---|
| Age (median, range) | 76 (30–96) | 75 (39–96) | 0.83 |
| Female (n, %) | 21(34.4) | 69 (37.7) | 0.76 |
| Anatomy of the digestive tract (n, %) | 0.43 | ||
| Normal | 54 (88.5) | 169 (92.3) | |
| Postoperative | 7 (11.5) | 14 (7.7) | |
| History of papillary procedures (n, %) | 1.00 | ||
| Existed | 42 (68.9) | 126 (68.9) | |
| None | 19 (31.1) | 57 (31.1) | |
| Degree of oral protrusion (n, %) | 0.62 | ||
| Long | 7 (11.5) | 17 (9.3) | |
| Short | 54 (88.5) | 166 (90.7) | |
| Parapapillary diverticulum (n, %) | 0.68 | ||
| Existed | 8 (13.1) | 30 (16.4) | |
| None | 53 (86.9) | 153 (83.6) | |
| Stent type (n, %) | <0.0001 | ||
| Straight | 61 (100.0) | 55 (30.0) | |
| Not straight | 0 (0.0) | 128 (70.0) | |
| Location of bile duct stricture (n, %) | 0.06 | ||
| Distal | 39 (63.9) | 141 (77.0) | |
| Proximal | 22 (36.1) | 42 (33.0) | |
| Disease (n, %) | |||
| Malignant | 31 (51%) | 82 (45%) | |
| Cholangiocarcinoma | 16 (26%) | 34 (19%) | |
| Pancreatic cancer | 10 (16%) | 37 (20%) | |
| Others | 5 (9%) | 11 (6%) | |
| Benign | 30 (49%) | 101 (55%) | |
| Bile duct stone | 22 (36%) | 71(39%) | |
| Others | 8 (13%) | 30 (16%) | |
| Reasons for stent replacement (n, %) | 0.21 | ||
| Stent occlusion | 16 (26.2) | 65 (35.5) | |
| Regular exchange | 45 (73.8) | 118 (64.5) | |
| Operator (n, %) | 0.88 | ||
| Experienced | 19 (31.1) | 60 (32.8) | |
| Trainee | 42 (68.9) | 123 (67.2) |
| SOG Group | SOS Group | p-Value | |
|---|---|---|---|
| Overall | |||
| (n = 61) | (n = 183) | ||
| Success rate of removing the stent after inserting the guidewire into the bile duct where the stent was placed (%) | 90.2 (55/61) | 77.1 (141/183) | 0.026 |
| Distal | |||
| (n = 39) | (n = 141) | ||
| Success rate of removing the stent after inserting the guidewire into the bile duct where the stent was placed (%) | 92.3 (36/39) | 77.1 (117/141) | 0.206 |
| Proximal | |||
| (n = 22) | (n = 42) | ||
| Success rate of removing the stent after inserting the guidewire into the bile duct where the stent was placed (%) | 86.4 (19/22) | 57.1 (24/42) | 0.025 |
| SOG Group | SOS Group | p-Value | |
|---|---|---|---|
| Overall | |||
| (n = 61) | (n = 55) | ||
| Success rate of removing the stent after inserting the guidewire into the bile duct where the stent was placed (%) | 90.2 (55/61) | 76.4 (42/55) | 0.077 |
| Distal | |||
| (n = 39) | (n = 46) | ||
| Success rate of removing the stent after inserting the guidewire into the bile duct where the stent was placed (%) | 92.3 (36/39) | 80.4 (37/46) | 0.210 |
| Proximal | |||
| (n = 22) | (n = 9) | ||
| Success rate of removing the stent after inserting the guidewire into the bile duct where the stent was placed (%) | 86.4 (19/22) | 55.6 (5/9) | 0.150 |
| SOG Group | SOS Group | p-Value | |
|---|---|---|---|
| (n = 61) | (n = 183) | ||
| Time required to insert the guidewire into the bile duct where the stent was placed and remove the stent (Successful cases only) (median; seconds (IQR)) | 306 (230–400) | 375 (268–573.5) | 0.012 |
| Adverse event incidence rate (%) | 0 (0/61) | 0.55 (1/183) | 1.00 |
| post-procedure pancreatitis | 0 | 1 | |
| bleeding | 0 | 0 | |
| perforation | 0 | 0 |
| Univariate Analysis | Multivariate Analysis | |||||
|---|---|---|---|---|---|---|
| OR | 95% CI | p-Value | OR | 95% CI | p-Value | |
| SOS method | 2.73 | 1.10–6.79 | 0.026 | 3.64 | 1.48–10.46 | 0.0038 |
| Stent type | 0.2598 | |||||
| Proximal biliary stenosis | 2.77 | 1.43–5.37 | 0.0032 | 5.08 | 2.37–11.21 | <0.0001 |
| Postoperative anatomy | 2.22 | 0.85–5.85 | 0.15 | |||
| Stent occlusion | 1.41 | 0.74–2.72 | 0.31 | |||
| Trainee | 1.65 | 0.76–3.58 | 0.40 | |||
| Naïve papilla | 0.89 | 0.45–1.78 | 0.86 | |||
| Long oral protrusion | 2.25 | 0.90–5.62 | 0.10 | |||
| Parapapillary diverticulum | 2.54 | 1.19–5.45 | 0.0243 | 4.57 | 1.91–10.93 | 0.0007 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshida, A.; Takenaka, M.; Takashima, K.; Tanaka, H.; Okamoto, A.; Yamazaki, T.; Nakai, A.; Omoto, S.; Minaga, K.; Kamata, K.; et al. Usefulness of the Novel Snare-over-the-Guidewire Method for Transpapillary Plastic Stent Replacement (with Video). J. Clin. Med. 2021, 10, 2858. https://doi.org/10.3390/jcm10132858
Yoshida A, Takenaka M, Takashima K, Tanaka H, Okamoto A, Yamazaki T, Nakai A, Omoto S, Minaga K, Kamata K, et al. Usefulness of the Novel Snare-over-the-Guidewire Method for Transpapillary Plastic Stent Replacement (with Video). Journal of Clinical Medicine. 2021; 10(13):2858. https://doi.org/10.3390/jcm10132858
Chicago/Turabian StyleYoshida, Akihiro, Mamoru Takenaka, Kota Takashima, Hidekazu Tanaka, Ayana Okamoto, Tomohiro Yamazaki, Atsushi Nakai, Shunsuke Omoto, Kosuke Minaga, Ken Kamata, and et al. 2021. "Usefulness of the Novel Snare-over-the-Guidewire Method for Transpapillary Plastic Stent Replacement (with Video)" Journal of Clinical Medicine 10, no. 13: 2858. https://doi.org/10.3390/jcm10132858
APA StyleYoshida, A., Takenaka, M., Takashima, K., Tanaka, H., Okamoto, A., Yamazaki, T., Nakai, A., Omoto, S., Minaga, K., Kamata, K., Yamao, K., Komeda, Y., Nishida, N., & Kudo, M. (2021). Usefulness of the Novel Snare-over-the-Guidewire Method for Transpapillary Plastic Stent Replacement (with Video). Journal of Clinical Medicine, 10(13), 2858. https://doi.org/10.3390/jcm10132858