
Expression Pattern of Leptin and Its Receptors in Endometrioid Endometrial Cancer

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. RNA Isolation
2.3. mRNA Microarrays
2.4. Real-Time Quantitative Reverse Transcription Reaction
2.5. ELISA
2.6. Statistical Analysis
3. Results
3.1. Characteristics of Patients Included in the Study and Control Group with the Analysis of the Differences between Groups
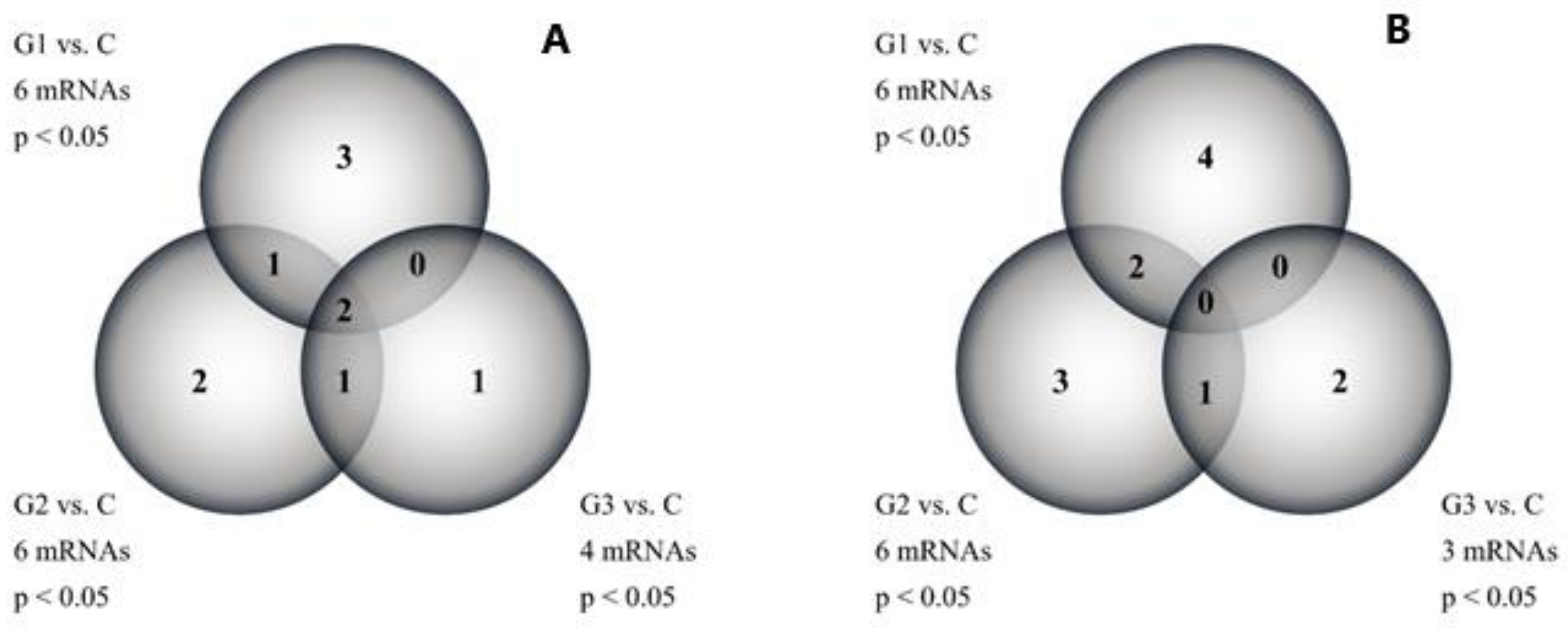
3.2. Leptin-Related Gene Expression Profile in Endometrial Tissues and Whole Blood of Patients Determined by Microarrays and RT-qPCR
3.3. The Level of Leptin Protein in the Serum of Patients Determined by ELISA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lin, T.C.; Lee, T.C.; Hsu, S.L.; Yang, C.S. The molecular mechanism of leptin secretion and expression induced by aristolochic acid in kidney fibroblast. PLoS ONE 2011, 66, e16654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Candelaria, P.V.; Rampoldi, A.; Harbuzariu, A.; Gonzalez-Perez, R.R. Leptin signaling and cancer chemoresistance: Perspectives. World J. Clin. Oncol. 2017, 8, 106–119. [Google Scholar] [CrossRef]
- Poetsch, M.S.; Strano, A.; Guan, K. Role of Leptin in Cardiovascular Diseases. Front. Endocrinol. 2020, 11, 354. [Google Scholar] [CrossRef]
- Ekmen, N.; Helvaci, A.; Gunaldi, M.; Sasani, H.; Yildirmak, S.T. Leptin as an important link between obesity and cardiovascular risk factors in men with acute myocardial infarction. Indian Heart J. 2016, 68, 132–137. [Google Scholar] [CrossRef] [Green Version]
- Yoon, Y.S.; Kwon, A.R.; Lee, Y.K.; Oh, S.W. Circulating adipokines and risk of obesity related cancers: A systematic review and meta-analysis. Obes. Res. Clin. Pract. 2019, 13, 329–339. [Google Scholar] [CrossRef] [PubMed]
- Ray, A. Cancer and comorbidity: The role of leptin in breast cancer and associated pathologies. World J. Clin. Cases 2018, 6, 483–492. [Google Scholar] [CrossRef]
- Modzelewska, P.; Chludzińska, S.; Lewko, J.; Reszeć, J. The influence of leptin on the process of carcinogenesis. Contemp. Oncol. 2019, 23, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Lipsey, C.C.; Harbuzariu, A.; Daley-Brown, D.; Gonzalez-Perez, R.R. Oncogenic role of leptin and Notch interleukin-1 leptin crosstalk outcome in cancer. World J. Methodol. 2016, 6, 43–55. [Google Scholar] [CrossRef]
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021. [Google Scholar] [CrossRef]
- Rizzo, S.; Femia, M.; Buscarino, V.; Franchi, D.; Garbi, A.; Zanagnolo, V.; Del Grande, M.; Manganaro, L.; Alessi, S.; Giannitto, C.; et al. Endometrial cancer: An overview of novelties in treatment and related imaging keypoints for local staging. Cancer Imaging 2018, 18, 45. [Google Scholar] [CrossRef]
- MacKintosh, M.L.; Crosbie, E.J. Prevention Strategies in Endometrial Carcinoma. Curr. Oncol. Rep. 2018, 20, 101. [Google Scholar] [CrossRef] [Green Version]
- Remmerie, M.; Janssens, V. Targeted Therapies in Type II Endometrial Cancers: Too Little, but Not Too Late. Int. J. Mol. Sci. 2018, 19, 2380. [Google Scholar] [CrossRef] [Green Version]
- Santaballa, A.; Matías-Guiu, X.; Redondo, A.; Carballo, N.; Gil, M.; Gómez, C.; Gorostidi, M.; Gutierrez, M.; Gónzalez-Martín, A. SEOM clinical guidelines for endometrial cancer (2017). Clin. Transl. Oncol. 2018, 20, 29–37. [Google Scholar] [CrossRef] [Green Version]
- Helpman, L.; Kupets, R.; Covens, A.; Saad, R.S.; Khalifa, M.A.; Ismiil, N.; Ghorab, Z.; Dubé, V.; Nofech-Mozes, S. Assessment of endometrial sampling as a predictor of final surgical pathology in endometrial cancer. Br. J. Cancer 2014, 110, 609–615. [Google Scholar] [CrossRef] [Green Version]
- Yu, S.; Shao, H.; Ban, X.; Zhang, H.; You, Y.; Zhou, N.; Mao, X.; Zhao, H.; Chen, J.; Lu, Z. Detection of POLE Subtypes in High-Grade Endometrioid Carcinoma by BaseScope-ISH Assay. Front. Oncol. 2019, 9, 831. [Google Scholar] [CrossRef] [PubMed]
- Raffone, A.; Travaglino, A.; Raimondo, D.; Neola, D.; Renzulli, F.; Santoro, A.; Insabato, L.; Casadio, P.; Zannoni, G.F.; Zullo, F.; et al. Prognostic value of myometrial invasion and TCGA groups of endometrial carcinoma. Gynecol. Oncol. 2021. [Google Scholar] [CrossRef]
- Dziobek, K.; Opławski, M.; Grabarek, B.; Zmarzły, N.; Januszyk, P.; Adwent, I.; Dąbruś, D.; Leśniak, E.; Kiełbasiński, R.; Kieszkowski, P.; et al. Expression of Semaphorin 3B (SEMA3B) in Various Grades of Endometrial Cancer. Med. Sci. Monit. 2019, 25, 4569–4574. [Google Scholar] [CrossRef] [PubMed]
- Koutsi, A.; Vervesou, E.C. Diagnostic molecular techniques in haematology: Recent advances. Ann. Transl. Med. 2018, 6, 242. [Google Scholar] [CrossRef]
- Tobin, N.P.; Foukakis, T.; De Petris, L.; Bergh, J. The importance of molecular markers for diagnosis and selection of targeted treatments in patients with cancer. J. Intern. Med. 2015, 278, 545–570. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Adipose tissue dysfunction contributes to obesity related metabolic diseases. Best Pract. Res. Clin. Endocrinol. Metab. 2013, 27, 163–177. [Google Scholar] [CrossRef]
- Lengyel, E.; Makowski, L.; DiGiovanni, J.; Kolonin, M.G. Cancer as a Matter of Fat: The Crosstalk between Adipose Tissue and Tumors. Trends Cancer 2018, 4, 374–384. [Google Scholar] [CrossRef] [PubMed]
- Kitson, S.; Ryan, N.; MacKintosh, M.L.; Edmondson, R.; Duffy, J.M.; Crosbie, E.J. Interventions for weight reduction in obesity to improve survival in women with endometrial cancer. Cochrane Database Syst. Rev. 2018, 2, CD012513. [Google Scholar] [CrossRef] [PubMed]
- Casadio, P.; Guasina, F.; Talamo, M.R.; Paradisi, R.; Morra, C.; Magnarelli, G.; Seracchioli, R. Conservative hysteroscopic treatment of stage I well differentiated endometrial cancer in patients with high surgical risk: A pilot study. J. Gynecol. Oncol. 2019, 30, e62. [Google Scholar] [CrossRef]
- Stone, T.W.; McPherson, M.; Gail Darlington, L. Obesity and Cancer: Existing and New Hypotheses for a Causal Connection. EBioMedicine 2018, 30, 14–28. [Google Scholar] [CrossRef] [Green Version]
- Ding, S.; Madu, C.O.; Lu, Y. The Impact of Hormonal Imbalances Associated with Obesity on the Incidence of Endometrial Cancer in Postmenopausal Women. J. Cancer 2020, 11, 5456–5465. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.E.; Kim, J.M.; Joung, K.H.; Lee, J.H.; You, B.R.; Choi, M.J.; Ryu, M.J.; Ko, Y.B.; Lee, M.A.; Lee, J.; et al. The Roles of Adipokines, Proinflammatory Cytokines, and Adipose Tissue Macrophages in Obesity-Associated Insulin Resistance in Modest Obesity and Early Metabolic Dysfunction. PLoS ONE 2016, 11, e0154003. [Google Scholar] [CrossRef] [Green Version]
- Sahai, E.; Astsaturov, I.; Cukierman, E.; DeNardo, D.G.; Egeblad, M.; Evans, R.M.; Fearon, D.; Greten, F.R.; Hingorani, S.R.; Hunter, T. A framework for advancing our understanding of cancer-associated fibroblasts. Nat. Rev. Cancer 2020, 20, 174–186. [Google Scholar] [CrossRef] [Green Version]
- Giordano, C.; Barone, I.; Vircillo, V.; Panza, S.; Malivindi, R.; Gelsomino, L.; Pellegrino, M.; Rago, V.; Mauro, L.; Lanzino, M.; et al. Activated FXR Inhibits Leptin Signaling and Counteracts Tumor-promoting Activities of Cancer-Associated Fibroblasts in Breast Malignancy. Sci. Rep. 2016, 6, 21782. [Google Scholar] [CrossRef] [PubMed]
- Ray, A.; Cleary, M.P. The potential role of leptin in tumor invasion and metastasis. Cytokine Growth Factor Rev. 2017, 38, 80–97. [Google Scholar] [CrossRef]
- Wcisło-Dziadecka, D.; Grabarek, B.; Kaźmierczak, A.; Gola, J.; & Kruszniewska–Rajs, C. The influence of adalimumab on the expression profile of mRNAs and miRNAs related to the IL-12 and IL-23 signal paths. JEADV 2020, 33, e198–e199. [Google Scholar]
- Qureshy, Z.; Johnson, D.E.; Grandis, J.R. Targeting the JAK/STAT pathway in solid tumors. J. Cancer Metastasis Treat. 2020, 6, 27. [Google Scholar] [PubMed]
- Khanna, P.; Lee, J.S.; Sereemaspun, A.; Lee, H.; Baeg, G.H. GRAMD1B regulates cell migration in breast cancer cells through JAK/STAT and Akt signaling. Sci. Rep. 2018, 8, 9511. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Wu, G.; Zhu, Y.; Zhang, W.; Zhang, H.; Zhou, Y.; Sun, P. HOXA10 deteriorates gastric cancer through activating JAK1/STAT3 signaling pathway. Cancer Manag. Res. 2019, 11, 6625–6635. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shang, A.Q.; Wu, J.; Bi, F.; Zhang, Y.J.; Xu, L.R.; Li, L.L.; Chen, F.F.; Wang, W.W.; Zhu, J.J.; Liu, Y.Y. Relationship between HER2 and JAK/STAT-SOCS3 signaling pathway and clinicopathological features and prognosis of ovarian cancer. Cancer Biol. Ther. 2017, 18, 314–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favoino, E.; Prete, M.; Catacchio, G.; Ruscitti, P.; Navarini, L.; Giacomelli, R.; Perosa, F. Working and safety profiles of JAK/STAT signaling inhibitors. Are these small molecules also smart? Autoimmun. Rev. 2021, 20, 102750. [Google Scholar] [CrossRef]
- Achkar, I.W.; Bhat, A.A.; Zafar, M.; Abbas, M.; Khan, O.S.; Kuttikrishnan, S.; Prabhu, K.S.; Uddin, S. Oncogenic role of dysregulated leptin signaling in the pathogenesis of ovarian cancer. Transl. Med. Commun. 2019, 4. [Google Scholar] [CrossRef] [Green Version]
- Li, F.; Zhao, S.; Guo, T.; Li, J.; Gu, C. The Nutritional Cytokine Leptin Promotes NSCLC by Activating the PI3K/AKT and MAPK/ERK Pathways in NSCLC Cells in a Paracrine Manner. BioMed Res. Int. 2019, 2019, 2585743. [Google Scholar] [CrossRef] [Green Version]
- Cheng, S.P.; Yin, P.H.; Hsu, Y.C.; Chang, Y.C.; Huang, S.Y.; Lee, J.J.; Chi, C.W. Leptin enhances migration of human papillary thyroid cancer cells through the PI3K/AKT and MEK/ERK signaling pathways. Oncol. Rep. 2011, 26, 1265–1271. [Google Scholar] [CrossRef]
- Mishra, A.K.; Parish, C.R.; Wong, M.L.; Licinio, J.; Blackburn, A.C. Leptin signals via TGFB1 to promote metastatic potential and stemness in breast cancer. PLoS ONE 2017, 12, e0178454. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, M.; Cao, F.L.; Li, N.; Gao, X.; Su, X.; Jiang, X. Leptin induces epithelial-to-mesenchymal transition via activation of the ERK signaling pathway in lung cancer cells. Oncol. Lett. 2018, 16, 4782–4788. [Google Scholar] [CrossRef] [Green Version]
- Vuletic, M.S.; Milosevic, V.S.; Jancic, S.A.; Zujovic, J.T.; Krstic, M.S.; Vukmirovic, F.C. Clinical significance of Leptin receptor (LEPR) and Endoglin (CD105) expressions in colorectal adenocarcinoma. J. BUON 2019, 24, 2448–2457. [Google Scholar]
- Zheng, X.J.; Yang, Z.X.; Dong, Y.J.; Zhang, G.Y.; Sun, M.F.; An, X.K.; Pan, L.H.; Zhang, S.L. Downregulation of leptin inhibits growth and induces apoptosis of lung cancer cells via the Notch and JAK/STAT3 signaling pathways. Biol. Open 2016, 15, 794–800. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ma, Y.; Liu, Z.; Zhang, Y.; Lu, B. Serum leptin, adiponectin and endometrial cancer risk in Chinese women. J. Gynecol. Oncol. 2013, 24, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Petridou, E.; Belechri, M.; Dessypris, N.; Koukoulomatis, P.; Diakomanolis, E.; Spanos, E.; Trichopoulos, D. Leptin and body mass index in relation to endometrial cancer risk. Ann. Nutr. Metab. 2002, 46, 147–151. [Google Scholar] [CrossRef] [PubMed]
- Zhou, X.; Li, H.; Chai, Y.; Liu, Z. Leptin Inhibits the Apoptosis of Endometrial Carcinoma Cells Through Activation of the Nuclear Factor κB-inducing Kinase/IκB Kinase Pathway. Int. J. Gynecol. Cancer 2015, 25, 770–778. [Google Scholar] [CrossRef]
- Wang, P.P.; He, X.Y.; Wang, R.; Wang, Z.; Wang, Y.G. High leptin level is an independent risk factor of endometrial cancer: A meta-analysis. Cell. Physiol. Biochem. 2014, 34, 1477–1484. [Google Scholar] [CrossRef] [Green Version]
- Gao, Y.; Dai, X.; Lee, A.C.; Wise, M.R.; Shen, F.; Chen, Q. Body Mass Index is Negatively Associated with Endometrial Cancer Stage, Regardless of Subtype and Menopausal Status. J. Cancer 2018, 9, 4756–4761. [Google Scholar] [CrossRef]
- Davis, C.D. The Gut Microbiome and Its Role in Obesity. Nutr. Today 2016, 51, 167–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vamanu, E. Complementary Functional Strategy for Modulation of Human Gut Microbiota. Curr. Pharm. Des. 2018, 24, 4144–4149. [Google Scholar] [CrossRef]
- Lin, C.; Cai, X.; Zhang, J.; Wang, W.; Sheng, Q.; Hua, H.; Zhou, X. Role of Gut Microbiota in the Development and Treatment of Colorectal Cancer. Digestion 2019, 100, 72–78. [Google Scholar] [CrossRef]
- Ma, W.; Mao, Q.; Xia, W.; Dong, G.; Yu, C.; Jiang, F. Gut Microbiota Shapes the Efficiency of Cancer Therapy. Front. Microbiol. 2019, 10, 1050. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, C.; Chang, Y.C.; Lan, M.S.; Breslin, M. Leptin stimulates ovarian cancer cell growth and inhibits apoptosis by increasing cyclin D1 and Mcl-1 expression via the activation of the MEK/ERK1/2 and PI3K/Akt signaling pathways. Int. J. Oncol. 2013, 42, 1113–1119. [Google Scholar] [CrossRef] [Green Version]
- Park, J.W.; Zhao, L.; Willingham, M.C.; Cheng, S.Y. Inhibition of STAT3 signaling blocks obesity-induced mammary hyperplasia in a mouse model. Am. J. Cancer Res. 2017, 7, 727–739. [Google Scholar] [PubMed]
- Carino, C.; Olawaiye, A.B.; Cherfils, S.; Serikawa, T.; Lynch, M.P.; Rueda, B.R.; Gonzalez, R.R. Leptin regulation of proangiogenic molecules in benign and cancerous endometrial cells. Int. J. Cancer 2008, 123, 2782–2790. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| mRNA | Sequence |
|---|---|
| LEP | Forward 5′-GAAGACCACATCCACACACG-3′ Reverse 5′-AGCTCAGCCAGACCCATCTA-3′ |
| LEPROT | Forward 5′-GCTTGGAGAGGCAGATAACG-3′ Reverse ′-AATGTCCTGGGTCCAGAGTG-3′ |
| LEPROTL1 | Forward 5′-TGCAATGTGGGAAGAAATGA-3′ Reverse 5′-AAGGAGGAAGCAGAGGAAGG-3′ |
| LEPR | Forward 5′-ACAGTCCCTTTGTGGGTCAG-3′ Reverse 5′-TATCCGAGCTCCAGCGTACT-3′ |
| ACTB | Forward 5′-TCACCCACACTGTGCCCATCTACGA-3′ Reverse 5′-CAGCGGAACCGCTCATTGCCAATGG-3′ |
| Parameter | C | G1 | G2 | G3 |
|---|---|---|---|---|
| Age (years) | 65.36 ± 10.29 | 67.22 ± 8.04 | 68.4 ± 10.09 | 64.88 ± 12.02 |
| Height (m) | 1.63 ± 0.14 | 1.59 ± 0.08 | 1.62 ± 0.05 | 1.59 ± 0.04 |
| Weight (kg) | 72.99 ± 13.95 | 74.41 ± 11.79 *# | 85.77 ± 21.99 ** | 85.22 ± 13.11 ***### |
| BMI | 28.77 ± 7.14 (overweight) | 29.01 ± 3.14 # (overweight) | 36.15 ± 10.44 **## (2nd degree of obesity) | 33.18 ± 5.44 ***### (1st degree of obesity) |
| Material | mRNA | ID | Microarray | RT-qPCR | ||||
|---|---|---|---|---|---|---|---|---|
| G1 vs. C | G2 vs. C | G3 vs. C | G1 vs. C | G2 vs. C | G3 vs. C | |||
| Tissue | LEP | 207092_at | 3.74 * | 5.58 * | 11.98 * | 3.22 * | 6.01 * | 12.11 * |
| LEPROT | 202377_at 202378_s_at | 4.12 * 4.01 * | 4.52 * 4.33 * | 4.69 * 5.01 * | 3.99 * | 4.88 * | 4.21 * | |
| LEPROTL1 | 202594_at 202595_s_at | 8.54 * 8.41 * | 7.98 * 8.22 * | 9.36 * 10.02 * | 9.01 * | 8.61 * | 9.00 * | |
| LEPR | 209894_at 209959_at 211167_s_at 211354_s_at 211355_x_at | 7.58 * 8.01 * 6.58 * 8.14 * 7.69 * | 8.99 10.01 * 7.44 * 8.98 * 6.01 * | 12.36 * 11.25 * 12.47 * 12.36 * 13.11 * | 9.54 * | 8.66 * | 11.63 * | |
| Whole blood | LEP | 207092_at | 8.99 * | 14.58 * | 18.51 * | 7.52 * | 12.63 * | 19.63 * |
| LEPROT | 202377_at 202378_s_at | 5.01 * 4.58 * | 4.99 * 5.09 * | 4.77 * 5.01 * | 4.36 * | 4.22 * | 4.59 * | |
| LEPROTL1 | 202594_at 202595_s_at | 7.58 * 7.63 * | 8.01 * 8.98 * | 10.65 * 11.01 * | 8.02 * | 8.96 * | 10.54 * | |
| LEPR | 209894_at 209959_at 211167_s_at 211354_s_at 211355_x_at 211356_x_at | 9.63 * 9.62 * 9.54 * 9.88 * 9.10 * 10.04 * | 11.25 * 11.44 * 11.01 * 11.36 * 10.58 * 11.66 * | 14.21 * 14.26 * 14.20 * 14.01 * 13.57 * 14.74 * | 9.01 * | 10.56 * | 13.25 * | |
| Group | C | G1 | G2 | G3 |
|---|---|---|---|---|
| ELISA (pg/mL) | 58.66 ± 3.63 | 369.68 ± 2.11 * | 499.32 ± 6.18 * | 714.01 ± 4.52 * |
| Pearson correlation (r) BMI | 0.889 * | 0.841 * | 0.914 * | 0.924 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Boroń, D.; Nowakowski, R.; Grabarek, B.O.; Zmarzły, N.; Opławski, M. Expression Pattern of Leptin and Its Receptors in Endometrioid Endometrial Cancer. J. Clin. Med. 2021, 10, 2787. https://doi.org/10.3390/jcm10132787
Boroń D, Nowakowski R, Grabarek BO, Zmarzły N, Opławski M. Expression Pattern of Leptin and Its Receptors in Endometrioid Endometrial Cancer. Journal of Clinical Medicine. 2021; 10(13):2787. https://doi.org/10.3390/jcm10132787
Chicago/Turabian StyleBoroń, Dariusz, Robert Nowakowski, Beniamin Oskar Grabarek, Nikola Zmarzły, and Marcin Opławski. 2021. "Expression Pattern of Leptin and Its Receptors in Endometrioid Endometrial Cancer" Journal of Clinical Medicine 10, no. 13: 2787. https://doi.org/10.3390/jcm10132787
APA StyleBoroń, D., Nowakowski, R., Grabarek, B. O., Zmarzły, N., & Opławski, M. (2021). Expression Pattern of Leptin and Its Receptors in Endometrioid Endometrial Cancer. Journal of Clinical Medicine, 10(13), 2787. https://doi.org/10.3390/jcm10132787