
Thoracic Surgery in the COVID-19 Pandemic: A Novel Approach to Reach Guideline Consensus

 , , ,
, , ,  ,
,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistics
3. Results
- General Statements
- Staff
- Precautions in the theater
- Diagnostics
- Treatment
- Chest drains
3.1. Statements
3.1.1. General Statements
- The guidelines and recommendations should be adapted according to the local prevalence of COVID-19 and the hospital’s resources (SRC A).
- 2.
- All patients for whom the delay of surgical procedures is necessary should be tracked and their treatment should be prioritized. The usage of alternative treatment options should be considered and documented (SRC A).
- 3.
- If standard care (e.g., resection) is not available, an individual treatment plan should be made for each patient by a multidisciplinary team (SRC A).
- 4.
- The attendance of patients in the hospital should be limited. Family visits should be reduced to one or no visitors (SRC A).
- 5.
- On arrival at the clinic, all patients should wear surgical masks (SRC A).
- 6.
- Staff should wear surgical masks at any patient contact (SRC A).
3.1.2. Staff
- 7.
- Staffing should be kept to a minimum. Virtual appointments/conferences and consultations should be preferred (SRC A).
- 8.
- Staff members should not be screened for SARS-CoV-2 (SRC C).
3.1.3. Screening of Patients
- 9.
- All patients should be evaluated for respiratory symptoms before hospitalization (SRC A).
- 10.
- All patients should be screened for SARS-CoV-2 by nasopharyngeal swabs (SRC C).
- 11.
- Serology tests are generally recommended (SRC C).
- 12.
- Preoperative CT scans should be conducted for all cancer surgery patients that require critical care (IMC/ICU) postoperatively (SRC C).
3.1.4. Precautions in the Theater
- 13.
- A designated theater and scrub room should be used for suspected or proven COVID-19 patients. A preoperative COVID-19 checklist should be used for suspected and confirmed COVID-19 patients (SRC B).
- 14.
- During procedures with suspected or proven COVID-19 patients, no changes in staff should be made. Reduce personnel to a minimum. Non-essential personnel should be absent (e.g., medical students and nurses-to-be) (SRC B).
- 15.
- Appropriate PPE (≥PPE2) should be used for all patients and in case of COVID-19-positive patients: PPE2/3 and goggles (SRC A).
- 16.
- The use of laminar airflow is recommended in the theater (SRC C).
3.1.5. Diagnostics
- 17.
- The routine use of low-dose CT scans instead of chest X-ray (CXR) is not recommended (SRC C).
- 18.
- Bronchoscopy should only be performed in patients who have no symptoms, contact or imaging suggestive of COVID-19 infection and postponed in patients with suspected or confirmed COVID-19 infections (SRC A).
- 19.
- Avoid high-flow nasal oxygen or aerosol-generating procedures (SRC A).
3.1.6. Treatment
- 20.
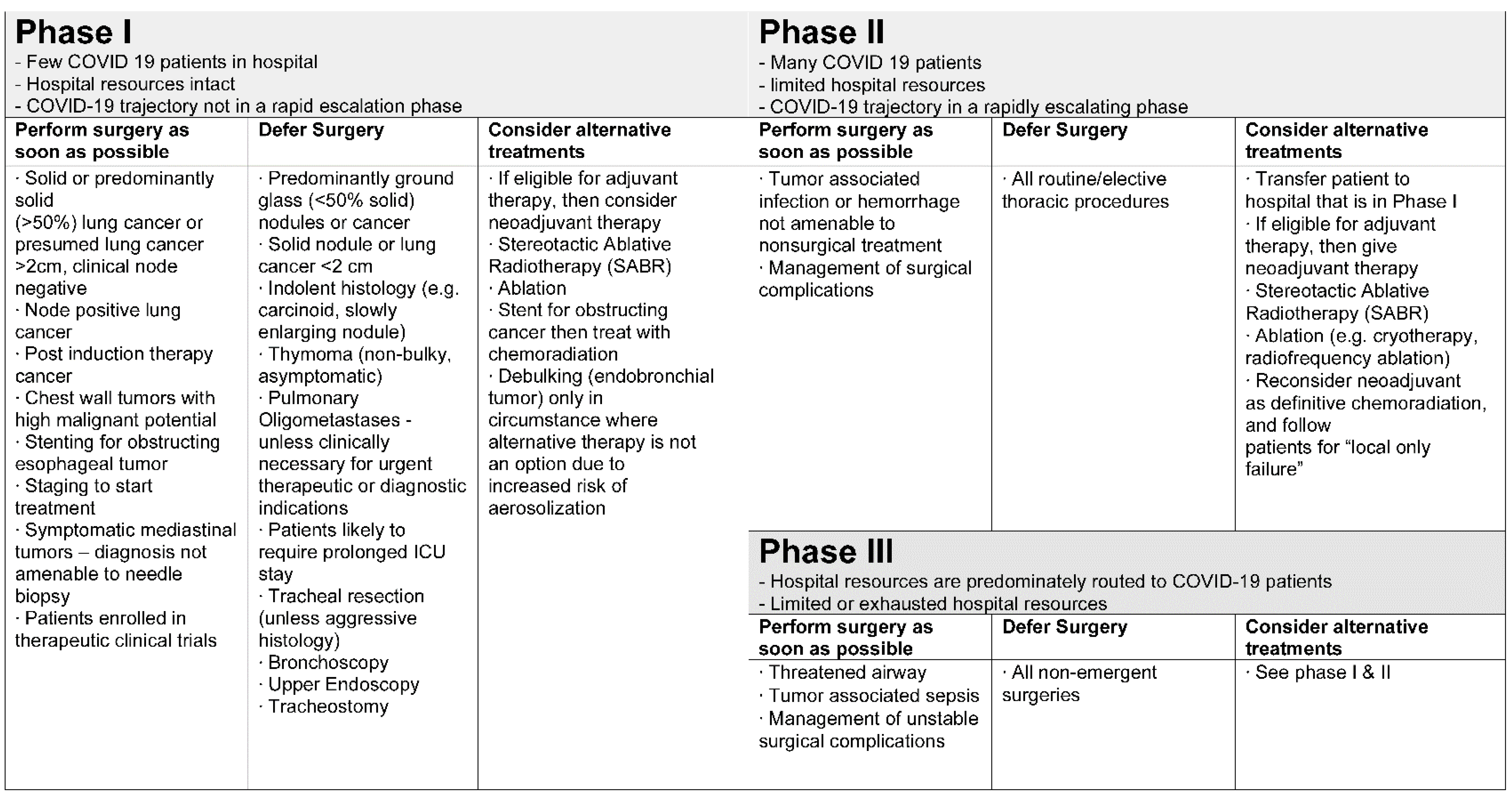
- Triage and surgical indications should be adapted according to the local prevalence of COVID-19 and the hospital’s resources (SRC A).
- 21.
- Patients with symptomatic or more advanced cancers should be prioritized for surgery (SRC A).
- 22.
- Surgery for non-critical elective/benign conditions should be postponed (with constant reevaluation) (SRC A).
- 23.
- In patients with proven COVID-19 infection, only essential and life-saving surgeries should be performed after a multidisciplinary decision (SRC B).
3.1.7. Chest Drains
- 24.
- The use of a closed system connected to a bag instead of a water seal system is recommended in pleural effusions (SRC C).
- 25.
- In pneumothorax with indication of thoracic drainage, it is recommended to connect to a conventional water seal system (SRC B).
- 26.
- There is no benefit of digital drain systems (SRC B).
- 27.
- Avoid early removal of chest drains placed in patients with COVID-19 infection and pneumothorax. Drains should be closed at least 24 hours before radiological confirmation and removal (SRC C).
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization (WHO). Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 1 March 2021).
- Ritschl, P.V.; Nevermann, N.; Wiering, L.; Wu, H.H.; Moroder, P.; Brandl, A.; Hillebrandt, K.; Tacke, F.; Friedersdorff, F.; Schlomm, T.; et al. Solid organ transplantation programs facing lack of empiric evidence in the COVID-19 pandemic: A By-proxy Society Recommendation Consensus approach. Arab. Archaeol. Epigr. 2020, 20, 1826–1836. [Google Scholar] [CrossRef]
- COVIDSurg Collaborative; Bhangu, A.; Lawani, I.; Ng-Kamstra, J.S.; Wang, Y.; Chan, A.; Futaba, K.; Ng, S.; Ebele, E.; Lederhuber, H.; et al. Global guidance for surgical care during the COVID-19 pandemic. BJS 2020, 107, 1097–1103. [Google Scholar] [CrossRef] [Green Version]
- Leow, L.; Ramanathan, K.; Kofidis, T.; Tam, J.K.C.; Mithiran, H. Organization of thoracic surgical services during the COVID pandemic. Surgeon 2021, 19, e1–e8. [Google Scholar] [CrossRef]
- Passaro, A.; Addeo, A.; Von Garnier, C.; Blackhall, F.; Planchard, D.; Felip, E.; Dziadziuszko, R.; de Marinis, F.; Reck, M.; Bouchaab, H.; et al. ESMO Management and treatment adapted recommendations in the COVID-19 era: Lung cancer. ESMO Open 2020, 5, e000820. [Google Scholar] [CrossRef] [PubMed]
- Turaga, K.; Girotra, S. Are we harming cancer patients by delaying their cancer surgery during the COVID-19 pandemic? Ann. Surg. 2020. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, H.; Ma, W.; Liu, F.; Yue, Z.; Fang, M.; Quan, M.; Pan, Z. Factors influencing survival of patients with pancreatic adenocarcinoma and synchronous liver metastases receiving palliative care. Pancreatology 2017, 17, 773–781. [Google Scholar] [CrossRef] [PubMed]
- Chu, D.K.; Akl, E.A.; Duda, S.; Solo, K.; Yaacoub, S.; Schünemann, H.J.; El-Harakeh, A.; Bognanni, A.; Lotfi, T.; Loeb, M.; et al. Physical distancing, face masks, and eye protection to prevent person-to-person transmission of SARS-CoV-2 and COVID-19: A systematic review and meta-analysis. Lancet 2020, 395, 1973–1987. [Google Scholar] [CrossRef]
- Bae, S.; Kim, M.-C.; Kim, J.Y.; Cha, H.-H.; Lim, J.S.; Jung, J.; Oh, D.K.; Lee, M.-K.; Choi, S.-H.; Sung, M.; et al. Effectiveness of Surgical and Cotton Masks in Blocking SARS–CoV-2: A Controlled Comparison in 4 Patients. Ann. Intern. Med. 2020, 173, W22–W23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Leung, N.H.L.; Chu, D.K.W.; Shiu, E.Y.C.; Chan, K.-H.; McDevitt, J.J.; Hau, B.J.P.; Yen, H.-L.; Li, Y.; Ip, D.K.M.; Peiris, J.S.M.; et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat. Med. 2020, 26, 676–680. [Google Scholar] [CrossRef] [Green Version]
- Peeples, L. Face masks: What the data say. Nat. Cell Biol. 2020, 586, 186–189. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, M.; Beyrer, C.; Goosby, E. Masks Do More Than Protect Others During COVID-19: Reducing the Inoculum of SARS-CoV-2 to Protect the Wearer. J. Gen. Intern. Med. 2020, 35, 3063–3066. [Google Scholar] [CrossRef] [PubMed]
- Yeo, D.; Yeo, C.; Kaushal, S.; Tan, G. COVID-19 and the General Surgical Department—Measures to Reduce Spread of SARS-COV-2 Among Surgeons. Ann. Surg. 2020, 272, e3–e4. [Google Scholar] [CrossRef] [PubMed]
- Hunter, E.; Price, D.A.; Murphy, E.; van der Loeff, I.S.; Baker, K.F.; Lendrem, D.; Lendrem, C.; Schmid, M.L.; Pareja-Cebrian, L.; Welch, A.; et al. First experience of COVID-19 screening of health-care workers in England. Lancet 2020, 395, e77–e78. [Google Scholar] [CrossRef]
- Treibel, T.; Manisty, C.; Burton, M.; McKnight, Á.; Lambourne, J.; Augusto, J.; Couto-Parada, X.; Cutino-Moguel, T.; Noursadeghi, M.; Moon, J.C. COVID-19: PCR screening of asymptomatic health-care workers at London hospital. Lancet 2020, 395, 1608–1610. [Google Scholar] [CrossRef]
- Khalil, A.; Hill, R.; Ladhani, S.; Pattisson, K.; O’Brien, P. COVID-19 screening of health-care workers in a London maternity hospital. Lancet Infect. Dis. 2021, 21, 23–24. [Google Scholar] [CrossRef]
- Chow, A.; Htun, H.L.; Kyaw, W.M.; Lee, L.T.; Ang, B. Asymptomatic health-care worker screening during the COVID-19 pandemic. Lancet 2020, 396, 1393–1394. [Google Scholar] [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Sohrabi, C.; Alsafi, Z.; O’Neill, N.; Khan, M.; Kerwan, A.; Al-Jabir, A.; Iosifidis, C.; Agha, R. World Health Organization declares global emergency: A review of the 2019 novel coronavirus (COVID-19). Int. J. Surg. 2020, 76, 71–76. [Google Scholar] [CrossRef]
- Li, Y.; Yao, L.; Li, J.; Chen, L.; Song, Y.; Cai, Z.; Yang, C. Stability issues of RT-PCR testing of SARS-CoV-2 for hospitalized patients clinically diagnosed with COVID-19. J. Med. Virol. 2020, 92, 903–908. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kucirka, L.M.; Lauer, S.A.; Laeyendecker, O.; Boon, D.; Lessler, J. Variation in False-Negative Rate of Reverse Transcriptase Polymerase Chain Reaction–Based SARS-CoV-2 Tests by Time Since Exposure. Ann. Intern. Med. 2020, 173, 262–267. [Google Scholar] [CrossRef]
- Xiao, A.T.; Tong, Y.X.; Zhang, S. False negative of RT-PCR and prolonged nucleic acid conversion in COVID-19: Rather than recurrence. J. Med. Virol. 2020, 92, 1755–1756. [Google Scholar] [CrossRef] [Green Version]
- Mercer, T.R.; Salit, M. Testing at scale during the COVID-19 pandemic. Nat. Rev. Genet. 2021, 1–12. [Google Scholar] [CrossRef]
- United States Food and Drug Administration. Emergency Use Authorizations. Available online: https://www.fda.gov/medical-devices/emergency-situations-medical-devices/emergency-use-authorizations (accessed on 1 March 2021).
- Winter, A.K.; Hegde, S. The important role of serology for COVID-19 control. Lancet Infect. Dis. 2020, 20, 758–759. [Google Scholar] [CrossRef]
- Krammer, F.; Simon, V. Serology assays to manage COVID-19. Science 2020, 368, 1060–1061. [Google Scholar] [CrossRef] [PubMed]
- Lisboa Bastos, M.; Tavaziva, G.; Abidi, S.K.; Campbell, J.R.; Haraoui, L.-P.; Johnston, J.C.; Lan, Z.; Law, S.; MacLean, E.; Trajman, A.; et al. Diagnostic accuracy of serological tests for covid-19: Systematic review and meta-analysis. BMJ 2020, 370, m2516. [Google Scholar] [CrossRef] [PubMed]
- Whitman, J.D.; Hiatt, J.; Mowery, C.T.; Shy, B.R.; Yu, R.; Yamamoto, T.N.; Rathore, U.; Goldgof, G.M.; Whitty, C.; Woo, J.M.; et al. Evaluation of SARS-CoV-2 serology assays reveals a range of test performance. Nat. Biotechnol. 2020, 38, 1174–1183. [Google Scholar] [CrossRef]
- Deeks, J.J.; Dinnes, J.; Takwoingi, Y.; Davenport, C.; Spijker, R.; Taylor-Phillips, S.; Adriano, A.; Beese, S.; Dretzke, J.; Fer-rante Di Ruffano, L.; et al. Antibody tests for identification of current and past infection with SARS-CoV-2. Cochrane Database Syst. Rev. 2020, 6, CD013652. [Google Scholar] [CrossRef] [PubMed]
- The Royal College of Radiologists. Statement on Use of CT Chest to Screen for COVID-19 in Pre-Operative Patients. Available online: https://www.rcr.ac.uk/college/coronavirus-covid-19-what-rcr-doing/clinical-information/role-ct-chest/role-ct-screening-0 (accessed on 1 March 2021).
- Fang, Y.; Zhang, H.; Xie, J.; Lin, M.; Ying, L.; Pang, P.; Ji, W. Sensitivity of Chest CT for COVID-19: Comparison to RT-PCR. Radiology 2020, 296, E115–E117. [Google Scholar] [CrossRef]
- Ai, T.; Yang, Z.; Hou, H.; Zhan, C.; Chen, C.; Lv, W.; Tao, Q.; Sun, Z.; Xia, L. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020, 296, E32–E40. [Google Scholar] [CrossRef] [Green Version]
- Isikbay, M.; Hope, M.D.; Raptis, C.A.; Shah, A.; Bierhals, A.J.; Bhalla, S.; Hammer, M.M.; Kligerman, S.J.; Jeudy, J.; Filev, P.D.; et al. CT on the Diamond Princess: What Might This Tell Us About Sensitivity for COVID-19? Radiol. Cardiothorac. Imaging 2020, 2, e200155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hope, M.D.; Raptis, C.A.; Henry, T.S. Chest Computed Tomography for Detection of Coronavirus Disease 2019 (COVID-19): Don’t Rush the Science. Ann. Intern. Med. 2020, 173, 147–148. [Google Scholar] [CrossRef] [Green Version]
- Bernheim, A.; Mei, X.; Huang, M.; Yang, Y.; Fayad, Z.A.; Zhang, N.; Diao, K.; Lin, B.; Zhu, X.; Li, K.; et al. Chest CT Findings in Coronavirus Disease-19 (COVID-19): Relationship to Duration of Infection. Radiology 2020, 295, 200463. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Islam, N.; Salameh, J.-P.; Leeflang, M.M.; Hooft, L.; McGrath, T.A.; Van Der Pol, C.B.; Frank, R.A.; Kazi, S.; Prager, R.; Hare, S.S.; et al. Thoracic imaging tests for the diagnosis of COVID-19. Cochrane Database Syst. Rev. 2020, 11, CD013639. [Google Scholar] [CrossRef] [PubMed]
- Surgery, S.f.C. Theatre COVID Pathway. Available online: https://scts.org/wp-content/uploads/2020/03/SCTS-ACTACC-SCPS-Theatre-COVID-pathway-Final.pdf (accessed on 1 March 2021).
- Ong, S.; Tan, Y.K.; Chia, P.Y.; Lee, T.H.; Ng, O.T.; Wong, M.S.Y.; Marimuthu, K. Air, Surface Environmental, and Personal Protective Equipment Contamination by Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) From a Symptomatic Patient. JAMA 2020, 323, 1610. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Theodorou, C.; Simpson, G.; Walsh, C. Theatre ventilation. Ann. R. Coll. Surg. Engl. 2021, 103, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Flemming, S.; Hankir, M.; Ernestus, R.-I.; Seyfried, F.; Germer, C.-T.; Meybohm, P.; Wurmb, T.; Vogel, U.; Wiegering, A. Surgery in times of COVID-19—Recommendations for hospital and patient management. Langenbecks Arch. Surg. 2020, 405, 359–364. [Google Scholar] [CrossRef]
- Sadrizadeh, S.; Holmberg, S. Surgical clothing systems in laminar airflow operating room: A numerical assessment. J. Infect. Public Health 2014, 7, 508–516. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Al-Benna, S. Negative pressure rooms and COVID-19. J. Perioper. Pr. 2021, 31, 18–23. [Google Scholar] [CrossRef]
- Gonzalez-Ciccarelli, L.F.; Nilson, J.; Oreadi, D.; Fakitsas, D.; Sekhar, P.; Quraishi, S.A. Reducing transmission of COVID-19 using a continuous negative pressure operative field barrier during oral maxillofacial surgery. Oral Maxillofac. Surg. Cases 2020, 6, 100160. [Google Scholar] [CrossRef] [PubMed]
- Nair, A.; Rodrigues, J.; Hare, S.; Edey, A.; Devaraj, A.; Jacob, J.; Johnstone, A.; McStay, R.; Denton, E.; Robinson, G. A British Society of Thoracic Imaging statement: Considerations in designing local imaging diagnostic algorithms for the COVID-19 pandemic. Clin. Radiol. 2020, 75, 329–334. [Google Scholar] [CrossRef] [PubMed]
- Wahidi, M.M.; Shojaee, S.; Lamb, C.R.; Ost, D.; Maldonado, F.; Eapen, G.; Caroff, D.A.; Stevens, M.P.; Ouellette, D.R.; Lilly, C.; et al. The Use of Bronchoscopy During the Coronavirus Disease 2019 Pandemic. Chest 2020, 158, 1268–1281. [Google Scholar] [CrossRef] [PubMed]
- Agarwal, A.; Basmaji, J.; Muttalib, F.; Granton, D.; Chaudhuri, D.; Chetan, D.; Hu, M.; Fernando, S.M.; Honarmand, K.; Bakaa, L.; et al. High-flow nasal cannula for acute hypoxemic respiratory failure in patients with COVID-19: Systematic reviews of effectiveness and its risks of aerosolization, dispersion, and infection transmission. Can. J. Anesth. 2020, 67, 1217–1248. [Google Scholar] [CrossRef]
- Li, J.; Fink, J.B.; Ehrmann, S. High-flow nasal cannula for COVID-19 patients: Low risk of bio-aerosol dispersion. Eur. Respir. J. 2020, 55, 2000892. [Google Scholar] [CrossRef] [PubMed]
- Demoule, A.; Baron, A.V.; Darmon, M.; Beurton, A.; Géri, G.; Voiriot, G.; Dupont, T.; Zafrani, L.; Girodias, L.; Labbé, V.; et al. High-Flow Nasal Cannula in Critically III Patients with Severe COVID-19. Am. J. Respir. Crit. Care Med. 2020, 202, 1039–1042. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.; Gangemi, A.; Marron, R.; Chowdhury, J.; Yousef, I.; Zheng, M.; Mills, N.; Tragesser, L.; Giurintano, J.; Gupta, R.; et al. Retrospective analysis of high flow nasal therapy in COVID-19-related moderate-to-severe hypoxaemic respiratory failure. BMJ Open Respir. Res. 2020, 7, e000650. [Google Scholar] [CrossRef] [PubMed]
- Leonard, S.; Atwood, C.W.; Walsh, B.K.; DeBellis, R.J.; Dungan, G.C.; Strasser, W.; Whittle, J.S. Preliminary Findings on Control of Dispersion of Aerosols and Droplets During High-Velocity Nasal Insufflation Therapy Using a Simple Surgical Mask. Chest 2020, 158, 1046–1049. [Google Scholar] [CrossRef]
- Antonoff, M.; Backhus, L.; Boffa, D.J.; Broderick, S.R.; Brown, L.M.; Carrott, P.; Clark, J.M.; Cooke, D.; David, E.; Facktor, M.; et al. COVID-19 Guidance for Triage of Operations for Thoracic Malignancies: A Consensus Statement from Thoracic Surgery Outcomes Research Network. Ann. Thorac. Surg. 2020, 110, 692–696. [Google Scholar] [CrossRef] [PubMed]
- Fiorelli, S.; Massullo, D.; Ibrahim, M.; Piccioni, F.; Andreetti, C.; Vanni, C.; Rocco, M.; Rendina, E.A.; Menna, C. Perspectives in surgical and anaesthetic management of lung cancer in the era of coronavirus disease 2019 (COVID-19). Eur. J. Cardio Thorac. Surg. 2020, 58, 676–681. [Google Scholar] [CrossRef] [PubMed]
- Samson, P.; Patel, A.; Garrett, T.; Crabtree, T.; Kreisel, D.; Krupnick, A.S.; Patterson, G.A.; Broderick, S.; Meyers, B.F.; Puri, V. Effects of Delayed Surgical Resection on Short-Term and Long-Term Outcomes in Clinical Stage I Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2015, 99, 1906–1913. [Google Scholar] [CrossRef] [Green Version]
- Samson, P.; Crabtree, T.D.; Robinson, C.G.; Morgensztern, D.; Broderick, S.; Krupnick, A.S.; Kreisel, D.; Patterson, G.A.; Meyers, B.; Puri, V. Defining the Ideal Time Interval Between Planned Induction Therapy and Surgery for Stage IIIA Non-Small Cell Lung Cancer. Ann. Thorac. Surg. 2017, 103, 1070–1075. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, S.H.; Zervos, M.; Kent, A.; Chachoua, A.; Bizekis, C.; Pass, H.; Cerfolio, R.J. Safety of patients and providers in lung cancer surgery during the COVID-19 pandemic. Eur. J. Cardio Thorac. Surg. 2020, 58, 1222–1227. [Google Scholar] [CrossRef] [PubMed]
- Passaro, A.; Peters, S.; Mok, T.; Attili, I.; Mitsudomi, T.; de Marinis, F. Testing for COVID-19 in lung cancer patients. Ann. Oncol. 2020, 31, 832–834. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.-K.; Peng, S.; Li, L.-Q.; Wang, Q.; Ping, W.; Zhang, N.; Fu, X.-N. Clinical and Transmission Characteristics of Covid-19—A Retrospective Study of 25 Cases from a Single Thoracic Surgery Department. Curr. Med. Sci. 2020, 40, 295–300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tuech, J.-J.; Gangloff, A.; Di Fiore, F.; Michel, P.; Brigand, C.; Slim, K.; Pocard, M.; Schwarz, L. Strategy for the practice of digestive and oncological surgery during the Covid-19 epidemic. J. Visc. Surg. 2020, 157, S7–S12. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Ceylan, K.C.; Batihan, G.; Yazgan, S.; Gürsoy, S.; Kıraklı, S.C.; Ataman, S. Pleural complications in patients with coronavirus disease 2019 (COVID-19): How to safely apply and follow-up with a chest tube during the pandemic? Eur. J. Cardio Thorac. Surg. 2020, 58, 1216–1221. [Google Scholar] [CrossRef]
- Dhanasopon, A.P.; Zurich, H.; Preda, A. Chest Tube Drainage in the Age of COVID-19. Physician Assist. Clin. 2021, 6, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Pieracci, F.M.; Burlew, C.C.; Spain, D.; Livingston, D.H.; Bulger, E.M.; Davis, K.A.; Michetti, C. Tube thoracostomy during the COVID-19 pandemic: Guidance and recommendations from the AAST Acute Care Surgery and Critical Care Committees. Trauma Surg. Acute Care Open 2020, 5, e000498. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, E.D.A.; De Oliveira, M.V.B. Safety model for chest drainage in pandemic by COVID-19. Rev. Colégio Bras. Cir. 2020, 47, e20202568. [Google Scholar] [CrossRef] [PubMed]
- Batchelor, T.J.P.; Rasburn, N.J.; Abdelnour-Berchtold, E.; Brunelli, A.; Cerfolio, R.J.; Gonzalez, M.; Ljungqvist, O.; Petersen, R.H.; Popescu, W.M.; Slinger, P.D.; et al. Guidelines for enhanced recovery after lung surgery: Recommendations of the Enhanced Recovery After Surgery (ERAS®) Society and the European Society of Thoracic Surgeons (ESTS). Eur. J. Cardio Thorac. Surg. 2018, 55, 91–115. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dziodzio, T.; Knitter, S.; Wu, H.H.; Ritschl, P.V.; Hillebrandt, K.-H.; Jara, M.; Juraszek, A.; Öllinger, R.; Pratschke, J.; Rückert, J.; et al. Thoracic Surgery in the COVID-19 Pandemic: A Novel Approach to Reach Guideline Consensus. J. Clin. Med. 2021, 10, 2769. https://doi.org/10.3390/jcm10132769
Dziodzio T, Knitter S, Wu HH, Ritschl PV, Hillebrandt K-H, Jara M, Juraszek A, Öllinger R, Pratschke J, Rückert J, et al. Thoracic Surgery in the COVID-19 Pandemic: A Novel Approach to Reach Guideline Consensus. Journal of Clinical Medicine. 2021; 10(13):2769. https://doi.org/10.3390/jcm10132769
Chicago/Turabian StyleDziodzio, Tomasz, Sebastian Knitter, Helen Hairun Wu, Paul Viktor Ritschl, Karl-Herbert Hillebrandt, Maximilian Jara, Andrzej Juraszek, Robert Öllinger, Johann Pratschke, Jens Rückert, and et al. 2021. "Thoracic Surgery in the COVID-19 Pandemic: A Novel Approach to Reach Guideline Consensus" Journal of Clinical Medicine 10, no. 13: 2769. https://doi.org/10.3390/jcm10132769
APA StyleDziodzio, T., Knitter, S., Wu, H. H., Ritschl, P. V., Hillebrandt, K.-H., Jara, M., Juraszek, A., Öllinger, R., Pratschke, J., Rückert, J., & Neudecker, J. (2021). Thoracic Surgery in the COVID-19 Pandemic: A Novel Approach to Reach Guideline Consensus. Journal of Clinical Medicine, 10(13), 2769. https://doi.org/10.3390/jcm10132769