
Incidence of Fat Embolism Syndrome in Femur Fractures and Its Associated Risk Factors over Time—A Systematic Review

 , ,
, , 
 and
and
Abstract
:1. Introduction
- Are the diagnostic standards applicable to all trauma patients?
- Has the incidence of FES changed over time since its clinical description?
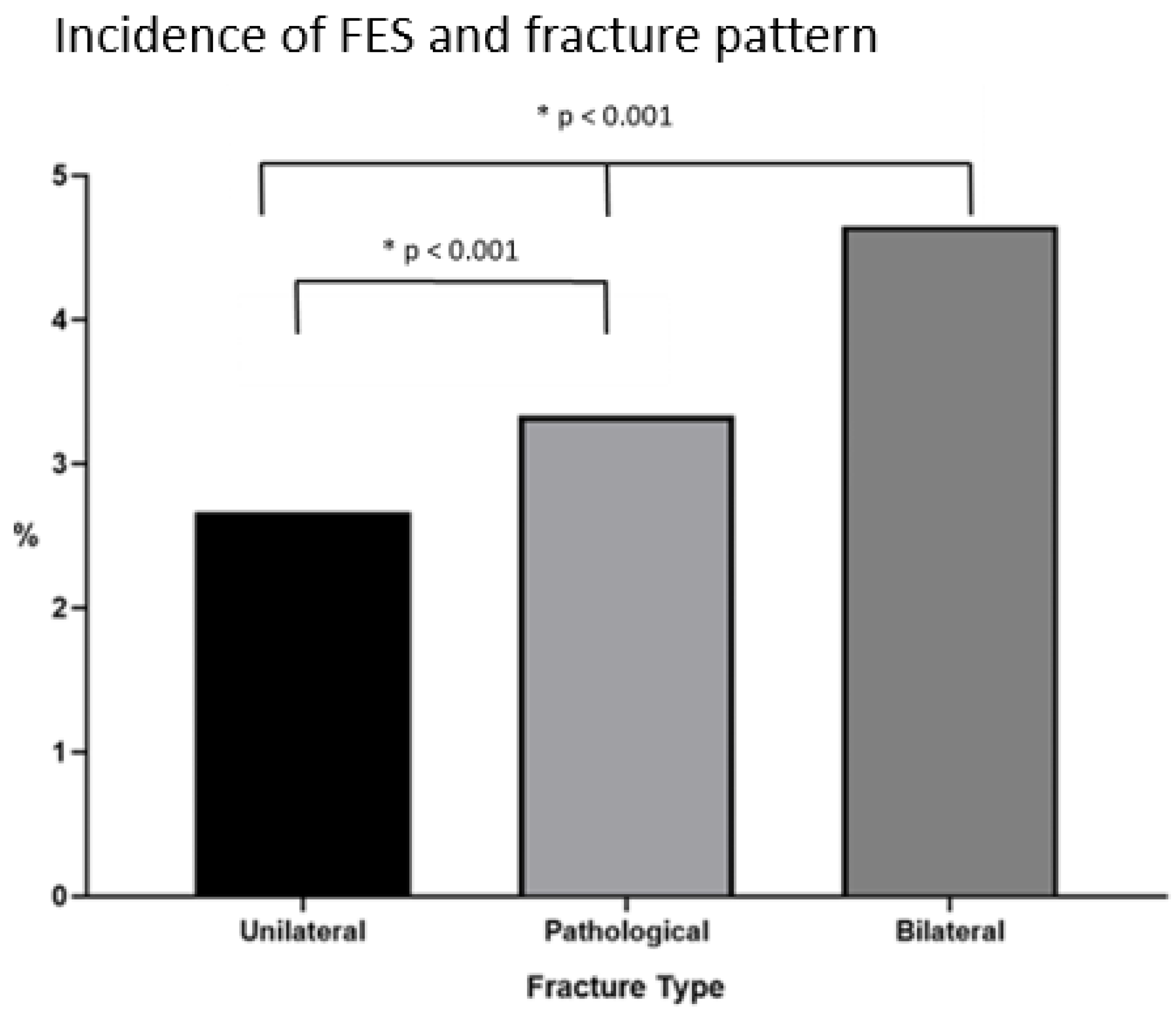
- Does the injury pattern (unilateral versus bilateral acute high-energy fractures versus pathological fractures) have an impact on the incidence of FES?
- Are specific evidence-based therapeutic recommendations available in the recent literature?
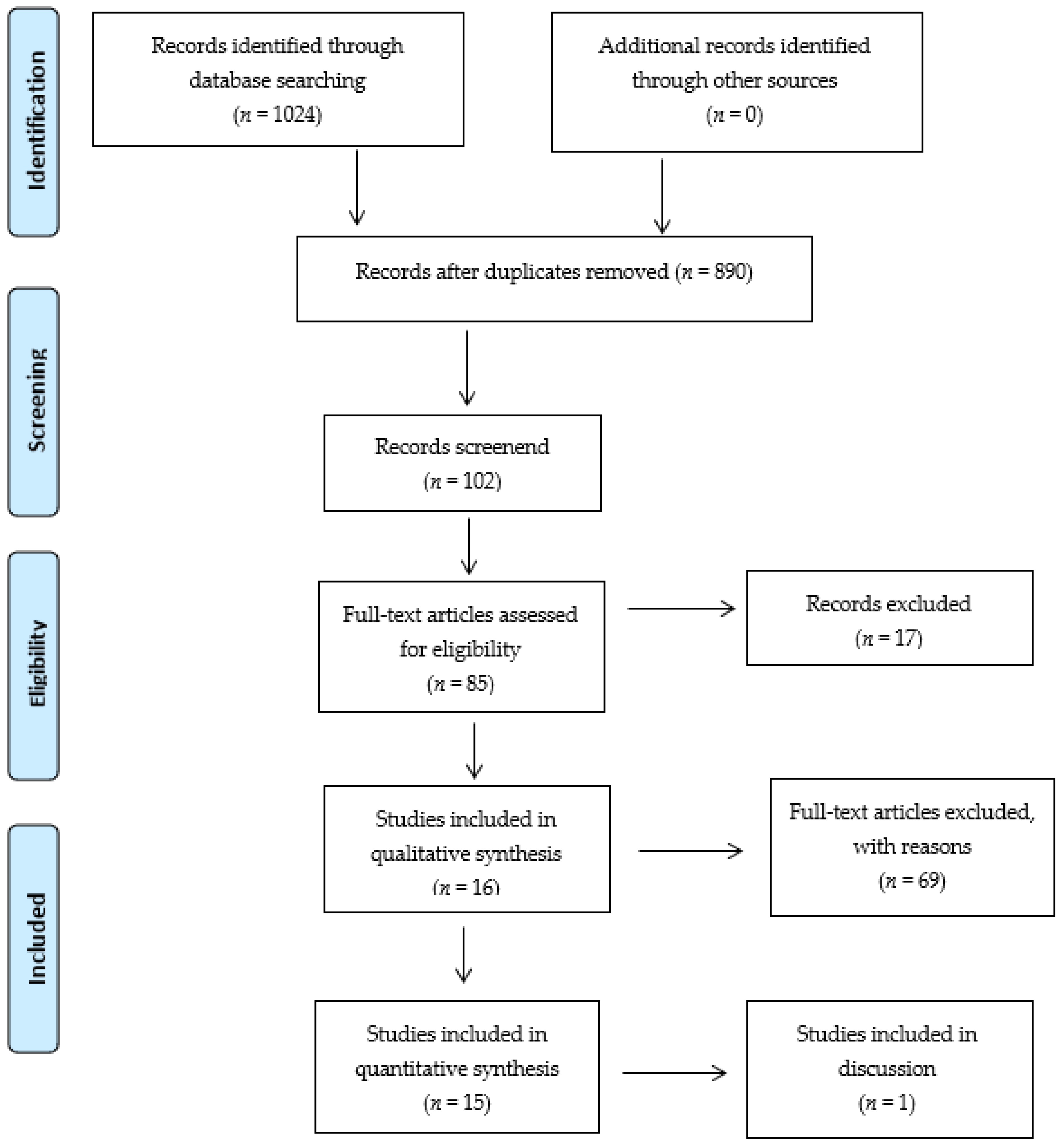
2. Methods
2.1. Search Strategy
2.2. Study Selection
2.3. Inclusion and Exclusion Criteria
- isolated and multiple femur fractures caused by high- or low-energy injuries and pathological fractures;
- description of primary and secondary outcomes (mortality, complications, length of intensive care unit stay, or length of hospital stay);
- original patient data from a single- or multicenter approach.
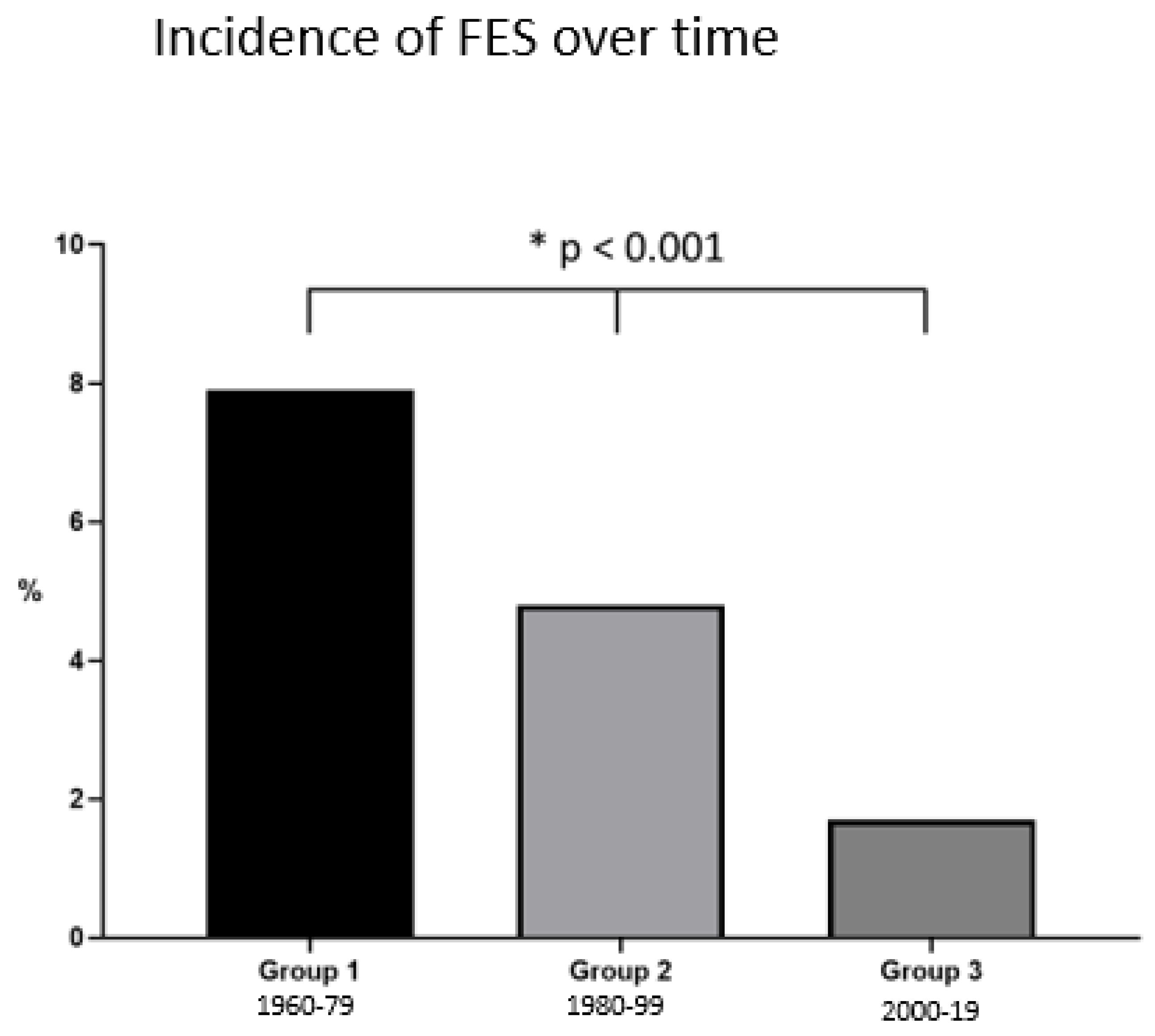
2.4. Group Distribution
- Group 1 (1 January 1960–31 December 1979),
- Group 2 (1 January 1980–31 December 1999),
- Group 3 (1 January 2000–31 December 2019).
2.5. Statistics
3. Results
3.1. Study Populations
3.2. Diagnostic Criteria
3.3. Changes in the Incidence of FES over Time
3.4. FES and Injury Patterns
3.5. Treatment Recommendations
4. Discussion
- Regarding diagnostic standards, most authors appeared to mainly rely on the Gurd’s criteria to diagnose the clinical syndrome. Magnetic resonance imaging (T2) has been routinely used as an adjunct tool in the radiologic literature [43], but the studies looked over in our review did not routinely use it.
- The incidence of FES has decreased from almost 8% to close to 2% since its clinical description. Our results indicated that this appears to apply especially for the period after the year 2000 (p < 0.01).
- We found a clear association between the incidence of FES and the injury pattern as follows: unilateral fractures (traumatic and pathological) were associated with a lower incidence of FES than bilateral fractures. Additionally, unilateral pathological fractures were associated with a higher incidence of FES compared to traumatic unilateral fractures.
- No universal recommendations in the literature regarding therapeutic strategies were found. Some authors recommended using steroids in the early years [9], but this treatment was rapidly discontinued due to infectious complications. Some authors even recommended prophylactic positioning of these particular patients at risk in the prone position [44].
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Major Criteria |
| Axillary or subconjunctival petechiae |
| Hypoxemia PaO2 < 60 mm Hg, FIO2 = 0.4 |
| Central nervous system depression disproportionate to hypoxemia |
| Pulmonary edema |
| Minor Criteria |
| Tachycardia more than 110 beats per minute |
| Pyrexia more than 38.5 °C |
| Fat globules present in urine |
| Changes in renal function (reduced urine output) |
| Drop in hemoglobin levels (more than 20% of the value upon admission) |
| Drop in hematocrit values |
| Drop in platelet values (more than 50% of the value upon admission) |
| Increasing erythrocyte sedimentation rate (ESR) (greater than 71 mm per h) |
| Fat globules present in the sputum |
| Emboli present in the retina on fundoscopy |
References
- Blokhuis, T.J.; Pape, H.-C.; Frölke, J.-P. Timing of definitive fixation of major long bone fractures: Can fat embolism syndrome be prevented? Injury 2017, 48, S3–S6. [Google Scholar] [CrossRef]
- Horst, K.; Andruszkow, H.; Weber, C.D.; Pishnamaz, M.; Herren, C.; Zhi, Q.; Knobe, M.; Lefering, R.; Hildebrand, F.; Pape, H.-C. Thoracic trauma now and then: A 10 year experience from 16,773 severely injured patients. PLoS ONE 2017, 12, e0186712. [Google Scholar]
- Tzioupis, C.C.; Giannoudis, P.V. Fat embolism syndrome: What have we learned over the years? Trauma 2011, 13, 259–281. [Google Scholar] [CrossRef]
- Kristiansen, S.; Madsen, M.R.; Steen, R.; Nielsen, E.W. A young trauma patient with five fractures and multi-organ failure. Tidsskr. Den Nor. Laegeforen. 2018, 138. [Google Scholar] [CrossRef]
- Nieman, G.F.; Gatto, L.A.; Habashi, N.M. Impact of mechanical ventilation on the pathophysiology of progressive acute lung injury. J. Appl. Physiol. 2015, 119, 1245–1261. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Capan, L. MSaPK. Fat embolism. Anesthesiol. Clin. N. Am. 1993, 11, 25–54. [Google Scholar] [CrossRef]
- Pandey, S.; Sharma, R.K. Practice of Intramedullary Nailing; Charles, C., Ed.; Thomas: Springfield, IL, USA, 1967. [Google Scholar]
- Hughes, S.P.; Reichert, I.L.; McCarthy, I.D. Biological effects of intramedullary reaming. J. Bone Jt. Surg. Br. 1993, 75, 845–847. [Google Scholar] [CrossRef]
- Schonfeld, S.A.; Ploysongsang, Y.; Dilisio, R.; Crissman, J.D.; Miller, E.; Hammerschmidt, D.E.; Jacob, H.S. Fat embolism prophylaxis with corticosteroids. A prospective study in high-risk patients. Ann. Intern. Med. 1983, 99, 438–443. [Google Scholar] [CrossRef]
- Vedrinne, J.M.; Guillaume, C.; Gagnieu, M.C.; Gratadour, P.; Fleuret, C.; Motin, J. Bronchoalveolar Lavage in Trauma Patients for Diagnosis of Fat Embolism Syndrome. Chest 1992, 102, 1323–1327. [Google Scholar] [CrossRef]
- Lindeque, B.G.; Schoeman, H.S.; Dommisse, G.F.; Boeyens, M.C.; Vlok, A.L. Fat embolism and the fat embolism syndrome. A double-blind therapeutic study. J. Bone Jt. Surg. Br. 1987, 69, 128–131. [Google Scholar] [CrossRef] [Green Version]
- Gurd, A.R.; Wilson, R.I. The fat embolism syndrome. J. Bone Jt. Surg. Br. 1974, 56b, 408–416. [Google Scholar] [CrossRef] [Green Version]
- Newbigin, K.; Souza, C.A.; Torres, C.; Marchiori, E.; Gupta, A.; Inacio, J.; Armstrong, M.; Peña, E. Fat embolism syndrome: State-of-the-art review focused on pulmonary imaging findings. Respir. Med. 2016, 113, 93–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Buskens, C.J.; Gratama, J.W.C.; Hogervorst, M.; Van Leeuwen, R.B.; Rommes, J.H.; Spronk, P.E. Encephalopathy and MRI abnormalities in fat embolism syndrome: A case report. Med. Sci. Monit. 2008, 14, Cs125–Cs129. [Google Scholar] [PubMed]
- Scarpino, M.; Lanzo, G.; Lolli, F.; Grippo, A. From the diagnosis to the therapeutic management: Cerebral fat embolism, a clinical challenge. Int. J. Gen. Med. 2019, 12, 39–48. [Google Scholar] [CrossRef] [Green Version]
- Denman, F.R.; Gragg, L. Fat embolism; a diagnostic enigma. Arch. Surg. 1948, 57, 325–332. [Google Scholar] [CrossRef] [PubMed]
- Hiss, J.; Kahana, T.; Kugel, C. Beaten to death: Why do they die? J. Trauma 1996, 40, 27–30. [Google Scholar] [CrossRef] [PubMed]
- Wyatt, J.P.; Khoo, P. Fat Embolism in Trauma. Am. J. Clin. Pathol. 1950, 20, 637–640. [Google Scholar] [CrossRef]
- Eriksson, E.A.; Pellegrini, D.C.; Vanderkolk, W.E.; Minshall, C.T.; Fakhry, S.M.; Cohle, S.D. Incidence of Pulmonary Fat Embolism at Autopsy: An Undiagnosed Epidemic. J. Trauma 2011, 71, 312–315. [Google Scholar] [CrossRef]
- Mudd, K.L.; Hunt, A.; Matherly, R.C.; Goldsmith, L.J.; Campbell, F.R.; Nichols, G.R. Analysis of pulmonary fat embolism in blunt force fatalities. J. Trauma 2000, 48, 711–715. [Google Scholar] [CrossRef]
- Christie, J.; Robinson, C.M.; Pell, A.C.; McBirnie, J.; Burnett, R. Transcardiac echocardiography during invasive intramedullary procedures. J. Bone Jt. Surg. Br. 1995, 77, 450–455. [Google Scholar] [CrossRef]
- Tsai, I.-T.; Hsu, C.-J.; Chen, Y.-H.; Fong, Y.-C.; Hsu, H.-C.; Tsai, C.-H. Fat Embolism Syndrome in Long Bone Fracture—Clinical Experience in a Tertiary Referral Center in Taiwan. J. Chin. Med. Assoc. 2010, 73, 407–410. [Google Scholar] [CrossRef] [Green Version]
- Prakash, S.; Sen, R.K.; Tripathy, S.K.; Sen, I.M.; Sharma, R.R.; Sharma, S. Role of Interleukin-6 as an Early Marker of Fat Embolism Syndrome: A Clinical Study. Clin. Orthop. Relat. Res. 2013, 471, 2340–2346. [Google Scholar] [CrossRef] [Green Version]
- Bulger, E.M.; Smith, D.G.; Maier, R.V.; Jurkovich, G.J. Fat embolism syndrome. A 10-year review. Arch. Surg. 1997, 132, 435–439. [Google Scholar] [CrossRef]
- Fabian, T.C.; Hoots, A.V.; Stanford, D.S.; Patterson, C.R.; Mangiante, E.C. Fat embolism syndrome: Prospective evaluation in 92 fracture patients. Crit. Care Med. 1990, 18, 42–46. [Google Scholar] [CrossRef]
- Assal, M.; Zanone, X.; Peter, R.E. Osteosynthesis of Metastatic Lesions of the Proximal Femur With a Solid Femoral Nail and Interlocking Spiral Blade Inserted Without Reaming. J. Orthop. Trauma 2000, 14, 394–397. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savović, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A.C.; et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 343, d5928. [Google Scholar] [CrossRef] [Green Version]
- Cole, A.S.; Hill, G.A.; Theologis, T.N.; Gibbons, C.; Willett, K. Femoral nailing for metastatic disease of the femur: A comparison of reamed and unreamed femoral nailing. Injury 2000, 31, 25–31. [Google Scholar] [CrossRef]
- Talucci, R.C.; Manning, J.; Lampard, S.; Bach, A.; Carrico, C.J. Early intramedullary nailing of femoral shaft fractures: A cause of fat embolism syndrome. Am. J. Surg. 1983, 146, 107–111. [Google Scholar] [CrossRef]
- ten Duis, H.J.; Nijsten, M.W.; Klasen, H.J.; Binnendijk, B. Fat embolism in patients with an isolated fracture of the femoral shaft. J. Trauma 1988, 28, 383–390. [Google Scholar] [CrossRef] [PubMed]
- Veith, R.G.; Winquist, R.A.; Hansen, S.T., Jr. Ipsilateral fractures of the femur and tibia. A report of fifty-seven consecutive cases. J. Bone Jt. Surg. Am. 1984, 66, 991–1002. [Google Scholar] [CrossRef]
- King, K.F.; Rush, J. Closed intramedullary nailing of femoral shaft fractures. A review of one hundred and twelve cases treated by the Kuntscher technique. J. Bone Jt. Surg. Am. 1981, 63, 1319–1323. [Google Scholar] [CrossRef]
- Bonnevialle, P.; Cauhepe, C.; Alqoh, F.; Bellumore, Y.; Rongieres, M.; Mansat, M. Risks and results after simultaneous intramedullary nailing in bilateral femoral fractures: A retrospective study of 40 cases. Rev. Chir. Orthop. Reparatrice Appar. Mot. 2000, 86, 598–607. [Google Scholar]
- Pinney, S.J.; Keating, J.F.; Meek, R.N. Fat embolism syndrome in isolated femoral fractures: Does timing of nailing influence incidence? Injury 1998, 29, 131–133. [Google Scholar] [CrossRef]
- Barwood, S.A.; Wilson, J.L.; Molnar, R.R.; Choong, P.F. The incidence of acute cardiorespiratory and vascular dysfunction following intramedullary nail fixation of femoral metastasis. Acta Orthop. Scand. 2000, 71, 147–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cannada, L.K.; Taghizadeh, S.; Murali, J.; Obremskey, W.T.; DeCook, C.; Bosse, M.J. Retrograde Intramedullary Nailing in Treatment of Bilateral Femur Fractures. J. Orthop. Trauma 2008, 22, 530–534. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Silva, J.J.A.B.; Diana, D.D.A.; Salas, V.E.R.; Zamboni, C.; Neto, J.S.H.; Christian, R.W. Fat embolism syndrome in femoral shaft fractures: Does the initial treatment make a difference? Rev. Bras. Ortop. 2017, 52, 535–537. [Google Scholar] [CrossRef] [PubMed]
- Bone, L.B.; Johnson, K.D.; Weigelt, J.; Scheinberg, R. Early versus delayed stabilization of femoral fractures. A prospective randomized study. J. Bone Jt. Surg. Am. 1989, 71, 336–340. [Google Scholar] [CrossRef]
- Adi, O.; Fong, C.P.; Azil, A.; Wahab, S.F.A. Fat embolism in right internal jugular vein: Incidental ultrasound finding during internal jugular vein cannulation. Ultrasound J. 2019, 11, 1. [Google Scholar] [CrossRef] [PubMed]
- Dalavayi, S.; Prahlow, J.A. Sudden death during hip replacement surgery: A case series. J. Forensic Leg. Med. 2019, 66, 138–143. [Google Scholar] [CrossRef]
- Lari, A.; Abdulshakoor, A.; Zogheib, E.; Assaf, N.; Mojallal, A.; Lari, A.-R.; Bauer, C.; Sinna, R. How to Save a Life From Macroscopic Fat Embolism: A Narrative Review of Treatment Options. Aesthetic Surg. J. 2020, 40, 1098–1107. [Google Scholar] [CrossRef]
- Dunkel, J.; Roth, C.; Erbguth, F.; Dietrich, W.; Hügens-Penzel, M.; Ferbert, A. Cerebral Fat Embolism: Clinical Presentation, Diagnostic Steps and Long-Term Follow-Up. Eur. Neurol. 2017, 78, 181–187. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, A.; Aggarwal, R.; Soni, K.D.; Trikha, A. Prone Positioning for Management of Fat Embolism Syndrome in a Patient with Spine Fracture; An Unusual Scenario and Review of Literature. Bull. Emerg. Trauma 2019, 7, 192–195. [Google Scholar] [CrossRef]
- Popovich, I.; Singh, V.; Vickery, B. Perioperative support of a patient with fat embolism syndrome with extracorporeal membraneoxygenation. BMJ Case Rep. 2019, 12, e227747. [Google Scholar] [CrossRef] [PubMed]
- Stein, P.D.; Yaekoub, A.Y.; Matta, F.; Kleerekoper, M. Fat Embolism Syndrome. Am. J. Med. Sci. 2008, 336, 472–477. [Google Scholar] [CrossRef] [PubMed]
- Gurd, A.R. Fat embolism: An aid to diagnosis. J. Bone Jt. Surg. Br. 1970, 52, 732–737. [Google Scholar] [CrossRef]
- Rothberg, D.L.; Makarewich, C.A. Fat Embolism and Fat Embolism Syndrome. J. Am. Acad. Orthop. Surg. 2019, 27, e346–e355. [Google Scholar] [CrossRef]
- Parizel, P.; Demey, H.; Veeckmans, G.; Verstreken, F.; Cras, P.; Jorens, P.; De Schepper, A. Early diagnosis of cerebral fat embolism syndrome by diffusion-weighted MRI (starfield pattern). Stroke 2001, 32, 2942–2944. [Google Scholar] [CrossRef] [PubMed]
- Gupta, A.; Reilly, C.S. Fat embolism. BJA Educ. 2007, 7, 148–151. [Google Scholar] [CrossRef] [Green Version]
- Bradford, D.S.; Foster, R.R.; Nossel, H.L. Coagulation alterations, hypoxemia, and fat embolism in fracture patients. J. Trauma 1970, 10, 307–321. [Google Scholar] [CrossRef]
- Renne, J.; Wuthier, R.; House, E.; Cancro, J.C.; Hoaglund, F.T. Fat macroglobulemia caused by fractures or total hip replacement. J. Bone Jt. Surg. Am. 1978, 60, 613–618. [Google Scholar] [CrossRef]
- Pape, H.C.; Giannoudis, P.; Krettek, C. The timing of fracture treatment in polytrauma patients: Relevance of damage control orthopedic surgery. Am. J. Surg. 2002, 183, 622–629. [Google Scholar] [CrossRef]
- Gossling, H.R.; Donohue, T.A. The Fat Embolism Syndrome. JAMA 1979, 241, 2472–2740. [Google Scholar] [CrossRef] [PubMed]
- Dunn, R.H.; Jackson, T.; Burlew, C.C.; Pieracci, F.M.; Fox, C.; Cohen, M.; Campion, E.M.; Lawless, R.; Mauffrey, C. Fat emboli syndrome and the orthopaedic trauma surgeon: Lessons learned and clinical recommendations. Int. Orthop. 2017, 41, 1729–1734. [Google Scholar] [CrossRef] [PubMed]
- Pape, H.C.; Tornetta, P.; Tarkin, I.; Tzioupis, C.; Sabeson, V.; Olson, S.A. Timing of fracture fixation in multitrauma patients: The role of early total care and damage control surgery. J. Am. Acad. Orthop. Surg. 2009, 17, 541–549. [Google Scholar] [CrossRef] [Green Version]
- Pape, H.C.; Pfeifer, R. Safe definitive orthopaedic surgery (SDS): Repeated assessment for tapered application of Early Definitive Care and Damage Control?: An inclusive view of recent advances in polytrauma management. Injury 2015, 46, 1–3. [Google Scholar] [CrossRef]
- Stinner, D.J.; Edwards, D. Surgical Management of Musculoskeletal Trauma. Surg. Clin. N. Am. 2017, 97, 1119–1131. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.A.; Swiontkowski, M.; Bhandari, M.; Walter, S.D.; Schemitsch, E.H.; Sanders, D.; Tometta, P. Reaming Does Not Affect Functional Outcomes after Open and Closed Tibial Shaft Fractures: The Results of a Randomized Controlled Trial. J. Orthop. Trauma 2016, 30, 142–148. [Google Scholar] [CrossRef] [Green Version]
- Cox, G.; Jones, E.; McGonagle, D.; Giannoudis, P.V. Reamer-irrigator-aspirator indications and clinical results: A systematic review. Int. Orthop. 2011, 35, 951–956. [Google Scholar] [CrossRef] [Green Version]
- Pape, H.C.; Zelle, B.A.; Hildebrand, F.; Giannoudis, P.V.; Krettek, C.; van Griensven, M. Reamed femoral nailing in sheep: Does irrigation and aspiration of intramedullary contents alter the systemic response? J. Bone Jt. Surg. Am. 2005, 87, 2515–2522. [Google Scholar] [CrossRef]
- Husebye, I.E.E.; Lyberg, T.; Madsen, J.E.; Eriksen, M.; Røise, O. The influence of a one-step reamer-irrigator-aspirator technique on the intramedullary pressure in the pig femur. Injury 2006, 37, 935–940. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hall, J.A.; McKee, M.D.; Vicente, M.R.; Morison, Z.A.; Dehghan, N.; Schemitsch, C.E.; Kreder, H.J.; Petrisor, B.; Schemitsch, E. Prospective Randomized Clinical Trial Investigating the Effect of the Reamer-Irrigator-Aspirator on the Volume of Embolic Load and Respiratory Function During Intramedullary Nailing of Femoral Shaft Fractures. J. Orthop. Trauma 2017, 31, 200–204. [Google Scholar] [CrossRef]
- Pape, H.C. RIA 2 System: New Generation Reamer-Irrigator-Aspirator; AO Technical Commission; AO Foundation: Davos, Switzerland, 2019. [Google Scholar]
- Behrman, S.W.; Fabian, T.C.; Kudsk, K.A.; Taylor, J.C. Improved outcome with femur fractures: Early vs. delayed fixation. J. Trauma 1990, 30, 792–797; discussion 797–798. [Google Scholar] [CrossRef] [PubMed]
- van Os, J.P.; Roumen, R.M.; Schoots, F.J.; Heystraten, F.M.; Goris, R.J. Is early osteosynthesis safe in multiple trauma patients with severe thoracic trauma and pulmonary contusion? J. Trauma 1994, 36, 495–498. [Google Scholar] [CrossRef]
- Lhowe, D.W.; Hansen, S.T. Immediate nailing of open fractures of the femoral shaft. J. Bone Jt. Surg. Am. 1988, 70, 812–820. [Google Scholar] [CrossRef]
- Giannoudis, P.V.; Smith, R.M.; Banks, R.E.; Windsor, A.C.; Dickson, R.A.; Guillou, P.J. Stimulation of inflammatory markers after blunt trauma. Br. J. Surg. 1998, 85, 986–990. [Google Scholar] [CrossRef] [PubMed]
- Morley, J.R.; Smith, R.M.; Pape, H.C.; MacDonald, D.A.; Trejdosiewitz, L.K.; Giannoudis, P.V. Stimulation of the local femoral inflammatory response to fracture and intramedullary reaming: A preliminary study of the source of the second hit phenomenon. J. Bone Jt. Surg. Br. 2008, 90, 393–399. [Google Scholar] [CrossRef] [Green Version]
- Pape, H.-C.; Rixen, D.; Morley, J.; Husebye, E.E.; Mueller, M.; Dumont, C.; Gruner, A.; Oestern, H.J.; Bayeff-Filoff, M.; Garving, C.; et al. Impact of the Method of Initial Stabilization for Femoral Shaft Fractures in Patients With Multiple Injuries at Risk for Complications (Borderline Patients). Ann. Surg. 2007, 246, 491–499; discussion 499–501. [Google Scholar] [CrossRef]
- Weber, C.D.; Lefering, R.; Dienstknecht, T.; Kobbe, P.; Sellei, R.M.; Hildebrand, F.; Pape, H.C.; TraumaRegister DGU. Classification of soft-tissue injuries in open femur fractures: Relevant for systemic complications? J. Trauma Acute Care Surg. 2016, 81, 824–833. [Google Scholar] [CrossRef] [Green Version]
- Kontakis, G.M.; Tossounidis, T.; Weiss, K.; Pape, H.-C.; Giannoudis, P.V. Fat embolism: Special situations Bilateral femoral fractures and pathologic femoral fractures. Injury 2006, 37, S19–S24. [Google Scholar] [CrossRef]
- Gauss, H. The pathology of fat embolisM. JAMA Surg. 1924, 9, 593–605. [Google Scholar] [CrossRef]
- Pell, A.C.; Christie, J.; Keating, J.F.; Sutherland, G.R. The detection of fat embolism by transoesophageal echocardiography during reamed intramedullary nailing. A study of 24 patients with femoral and tibial fractures. J. Bone Jt. Surg. Br. 1993, 75, 921–925. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tobin, C.E. Arteriovenous shunts in the peripheral pulmonary circulation in the human lung. Thorax 1966, 21, 197–204. [Google Scholar] [CrossRef] [Green Version]
- Wenda, K.; Runkel, M.; Degreif, J.; Ritter, G. Pathogenesis and clinical relevance of bone marrow embolism in medullary nailing—demonstrated by intraoperative echocardiography. Injury 1993, 24, S73–S81. [Google Scholar] [CrossRef]
- Wozasek, G.E.; Simon, P.; Redl, H.; Schlag, G. Intramedullary pressure changes and fat intravasation during intramedullary nailing: An experimental study in sheep. J. Trauma 1994, 36, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Dahl, O.E.; Aspelin, T.; Lyberg, T. The role of bone traumatization in the initiation of proximal deep vein thrombosis during cemented hip replacement surgery in pigs. Blood Coagul. Fibrinolysis 1995, 6, 709–717. [Google Scholar] [CrossRef]
- Lehman, E.P.; Moore, R.M. Fat embolism: Including experimental production without trauma. JAMA Surg. 1927, 14, 621–662. [Google Scholar] [CrossRef]
- Parker, F.B., Jr.; Wax, S.D.; Kusajima, K.; Webb, W.R. Hemodynamic and pathological findings in experimental fat embolism. Arch. Surg. 1974, 108, 70–74. [Google Scholar] [CrossRef]
- Hulman, G. Fat macroglobule formation from chylomicrons and non-traumatic fat embolism. Clin. Chim. Acta 1988, 177, 173–178. [Google Scholar] [CrossRef]
- Randelli, F.; Capitani, P.; Pace, F.; Favilla, S.; Galante, C.; Randelli, P. Bilateral femoral shaft fractures complicated by fat and pulmonary embolism: A case report. Injury 2015, 46, S28–S30. [Google Scholar] [CrossRef]
- Aggarwal, R.; Pal, S.; Soni, K.D.; Gamangatti, S. Massive cerebral fat embolism leading to brain death: A rare presentation. Indian J. Crit. Care Med. 2015, 19, 687–689. [Google Scholar]
- Guerado, E.; Bertrand, M.L.; Cano, J.R.; Cervan, A.M.; Galan, A. Damage control orthopaedics: State of the art. World J. Orthop. 2019, 10, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Dezman, Z.D.; Comer, A.C.; Smith, G.S.; Narayan, M.; Scalea, T.M.; Hirshon, J.M. Failure to clear elevated lactate predicts 24-hour mortality in trauma patients. J. Trauma Acute Care Surg. 2015, 79, 580–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pape, H.-C.; Halvachizadeh, S.; Leenen, L.; Velmahos, G.; Buckley, R.; Giannoudis, P. Timing of major fracture care in polytrauma patients–An update on principles, parameters and strategies for 2020. Injury 2019, 50, 1656–1670. [Google Scholar] [CrossRef]
- Mellor, A.; Soni, N. Fat embolism. Anaesthesia 2001, 56, 145–154. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.C.; Torrens, L.; Howie, C.R.; Christie, J.; Robinson, C.M. Cognitive function and cerebral emboli after primary hip arthroplasty. Hip Int. 2008, 18, 40–45. [Google Scholar] [CrossRef] [PubMed]
- Gray, A.C.; White, T.O.; Clutton, E.; Christie, J.; Hawes, B.D.; Robinson, C.M. The Stress Response to Bilateral Femoral Fractures: A Comparison of Primary Intramedullary Nailing and External Fixation. J. Orthop. Trauma 2009, 23, 90–97; discussion 8–9. [Google Scholar] [CrossRef] [PubMed]
- Robinson, C.M.; Ludlam, C.A.; Ray, D.C.; Swann, D.G.; Christie, J. The coagulative and cardiorespiratory responses to reamed intramedullary nailing of isolated fractures. J. Bone Jt. Surg. Br. 2001, 83, 963–973. [Google Scholar] [CrossRef]
- Gray, A.C.; Torrens, L.; White, T.O.; Carson, A.; Robinson, C.M. The cognitive effects of fat embolus syndrome following an isolated femoral shaft fracture. A case report. J. Bone Jt. Surg. Am. 2007, 89, 1092–1096. [Google Scholar] [CrossRef]
- Gray, A.C.; Torrens, L.; Christie, J.; Graham, C.; Robinson, C.M. Cerebral emboli and cognitive function after intramedullary fracture fixation. Injury 2009, 40, 742–745. [Google Scholar] [CrossRef]
- Pfeifer, R.; Heussen, N.; Michalewicz, E.; Hilgers, R.D.; Pape, H.C. Incidence of adult respiratory distress syndrome in trauma patients: A systematic review and meta-analysis over a period of three decades. J. Trauma Acute Care Surg. 2017, 83, 496–506. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murphy, P.; Edelist, G.; Byrick, R.J.; Kay, J.C.; Mullen, J.B. Relationship of fat embolism to haemodynamic and echocardiographic changes during cemented arthroplasty. Can. J. Anaesth. 1997, 44, 1293–1300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Byrick, R.J.; Mullen, J.B.; Mazer, C.D.; Guest, C.B. Transpulmonary systemic fat embolism. Studies in mongrel dogs after cemented arthroplasty. Am. J. Respir. Crit. Care Med. 1994, 150, 1416–1422. [Google Scholar] [CrossRef] [PubMed]
- Herndon, J.H.; Bechtol, C.O.; Crickenberger, D.P. Fat embolism during total hip replacement. A prospective study. J. Bone Jt. Surg. Am. 1974, 56, 1350–1362. [Google Scholar] [CrossRef]
| Study | Confounding | Subject Selection | Intervention Measurement | Deviation from Intended Intervention | Attrition | Outcomes Measurement | Selective Reporting | Overall |
|---|---|---|---|---|---|---|---|---|
| Cole et al. [23] | Low | Low | Low | Moderate | Low | Moderate | Serious | Serious |
| Prakash et al. [25] | Moderate | Low | Low | Low | Low | Moderate | Moderate | Moderate |
| Fabian et al. [29] | Moderate | Moderate | Low | Moderate | Low | Low | Moderate | Moderate |
| Talucci et al. [30] | Moderate | Critical | Moderate | Moderate | Low | Moderate | Serious | Critical |
| Ten Duis et al. [31] | Moderate | Moderate | Low | Serious | Low | Moderate | Moderate | Serious |
| Author | Study Period | Total Patients (n) | Injury Pattern | Trauma Mechanism | Fracture | Sex (M/F) | Age Range (Years) |
|---|---|---|---|---|---|---|---|
| Ten Duis [22] * | 1967–1985 | 172 | U | blunt | 21 open | 133/29 * | 16–65 |
| 151 closed | |||||||
| Talucci [23] | 1978–1981 | 100 | U | n.a. | n.a. | n.a. | n.a. |
| Veith [25] | 1968–1978 | 54 | U | blunt | open/ | 32/22 | 15–58 |
| closed | |||||||
| King [26] | 1972–1977 | 112 | U | blunt | 19 open | n.a. | n.a. |
| 93 closed | |||||||
| Bone [29] | 1985–1987 | 79 | U | n.a. | n.a. | n.a. | n.a. |
| Bonneviale [30] | 1986–1999 | 40 | Bi | blunt | n.a. | 27/13 | 17–50 |
| Pinney [31] | 1987–1994 | 274 | U | n.a. | n.a. | 189/85 | 13–96 |
| Cole [32] | 1990–1996 | 65 | Pa | n.a. | n.a. | n.a. | 15–92 |
| Fabian [33] | 1990 | 92 | U | n.a. | n.a. | n.a. | n.a. |
| Assal [34] | 1994–1997 | 10 | Pa | n.a. | n.a. | 3/7 | 53–99 |
| Barwood [35] | 1994–1997 | 43 | Pa | n.a. | closed | 17/26 | 39–93 |
| Tsai [36] | 1997–2008 | 1541 | U | n.a. | n.a. | n.a. | n.a. |
| Cannada [37] | 2000–2004 | 89 | Bi | blunt | n.a. | 46/43 | 16–63 |
| Prakash [38] | 2010–2011 | 48 | U | n.a. | closed | 38/10 | 16–40 |
| Silva [39] | 2011–2015 | 272 | U | n.a. | n.a. | 229/43 | >16 |
| Author | Period | Incidence of FES (%) | Diagnostic Criteria for FES |
|---|---|---|---|
| Ten Duis et al. [22] | 1967–1985 | 3.5 | GURD |
| Talucci et al. [23] | 1978–1981 | 5 | GURD |
| Veith et al. [25] | 1968–1978 | 13 | 1 out of GURD |
| King et al. [26] | 1972–1977 | 15.18 | “clinical evidence” |
| Bone et al. [29] | 1985–1987 | 1.12 | n.a. |
| Bonneviale et al. [30] | 1986–1999 | 5 | GURD |
| Pinney et al. [31] | 1987–1994 | 4 | GURD |
| Cole et al. [32] | 1990–1996 | 3.08 | Autopsy |
| Fabian et al. [33] | to1990 start unknown | 10.87 | n.a. |
| Assal et al. [34] | 1994–1997 | 10 | Autopsy |
| Barwood et al. [35] | 1994–1997 | 2.2 | CRVD |
| Tsai et al. [36] | 1997–2008 | 0.78 | GURD |
| Cannada et al. [37] | 2000–2004 | 4 | GURD |
| Prakash et al. [38] | 2010–2011 | 23 | GURD |
| Silva et al. [39] | 2011–2015 | 4 | n.a. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lempert, M.; Halvachizadeh, S.; Ellanti, P.; Pfeifer, R.; Hax, J.; Jensen, K.O.; Pape, H.-C. Incidence of Fat Embolism Syndrome in Femur Fractures and Its Associated Risk Factors over Time—A Systematic Review. J. Clin. Med. 2021, 10, 2733. https://doi.org/10.3390/jcm10122733
Lempert M, Halvachizadeh S, Ellanti P, Pfeifer R, Hax J, Jensen KO, Pape H-C. Incidence of Fat Embolism Syndrome in Femur Fractures and Its Associated Risk Factors over Time—A Systematic Review. Journal of Clinical Medicine. 2021; 10(12):2733. https://doi.org/10.3390/jcm10122733
Chicago/Turabian StyleLempert, Maximilian, Sascha Halvachizadeh, Prasad Ellanti, Roman Pfeifer, Jakob Hax, Kai O. Jensen, and Hans-Christoph Pape. 2021. "Incidence of Fat Embolism Syndrome in Femur Fractures and Its Associated Risk Factors over Time—A Systematic Review" Journal of Clinical Medicine 10, no. 12: 2733. https://doi.org/10.3390/jcm10122733
APA StyleLempert, M., Halvachizadeh, S., Ellanti, P., Pfeifer, R., Hax, J., Jensen, K. O., & Pape, H.-C. (2021). Incidence of Fat Embolism Syndrome in Femur Fractures and Its Associated Risk Factors over Time—A Systematic Review. Journal of Clinical Medicine, 10(12), 2733. https://doi.org/10.3390/jcm10122733