
Utility of Acute Physiology and Chronic Health Evaluation (APACHE II) in Predicting Mortality in Patients with Pyogenic Liver Abscess: A Retrospective Study

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
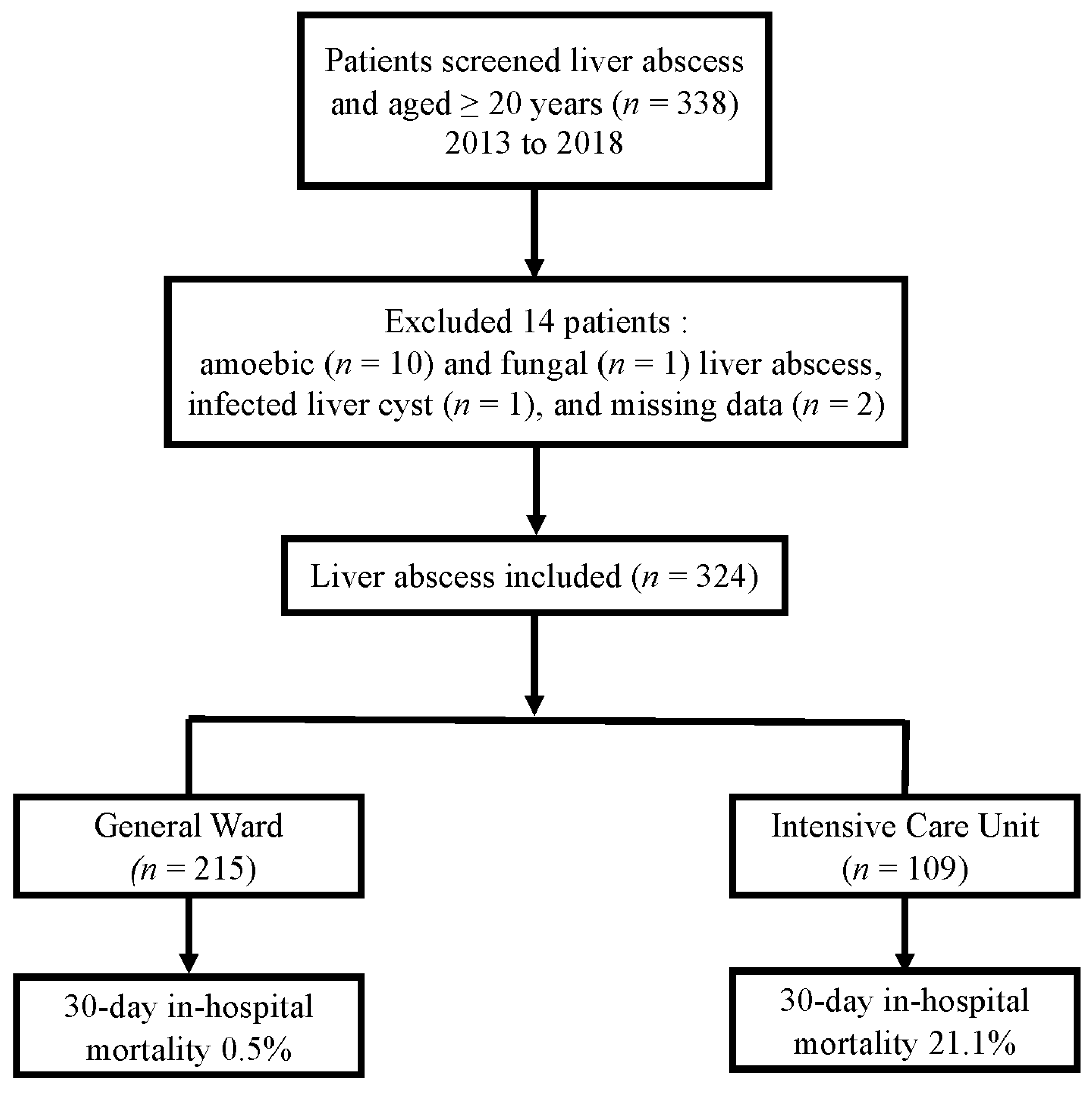
2.1. Study Design and Patient Selection
2.2. Data Collection and Definition of the Variables
2.3. Treatment and Outcomes
2.4. Statistical Analyses
3. Results
3.1. Clinical Manifestations and Laboratory, Microbiologic, and Imaging Findings
3.2. Treatment, Complications, and Outcomes
3.3. Multivariate Analyses of Clinical Factors in Relation to 30-Day Mortality
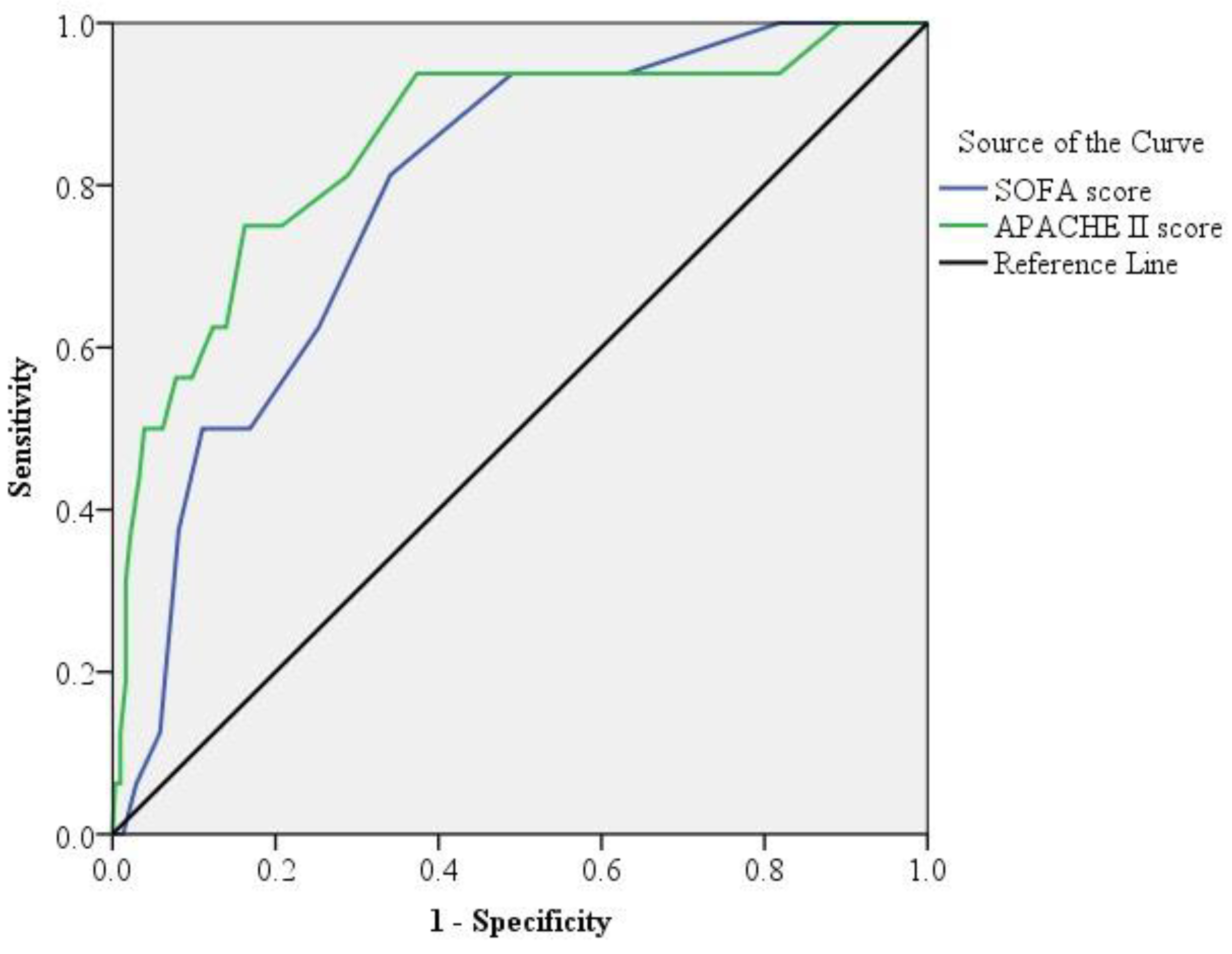
3.4. ROC and Kaplan–Meier Curve Analyses of APACHE II and SOFA Scores and Cutoff Points Predicting 30-Day Mortality
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, S.C.; Lee, Y.T.; Lai, K.C.; Cheng, K.S.; Jeng, L.B.; Wu, W.Y.; Chen, C.C.; Lee, M.C. Risk factors for developing metastatic infection from pyogenic liver abscesses. Swiss. Med. Wkly. 2006, 136, 119–126. [Google Scholar]
- Chen, S.C.; Lee, Y.T.; Yen, C.-H.; Lai, K.C.; Jeng, L.B.; Lin, D.B.; Wang, P.H.; Chen, C.C.; Lee, M.C.; Bell, W.R. Pyogenic liver abscess in the elderly: Clinical features, outcomes and prognostic factors. Age Ageing 2009, 38, 271–276. [Google Scholar] [CrossRef][Green Version]
- Chen, Y.C.; Lin, C.H.; Chang, S.N.; Shi, Z.Y. Epidemiology and clinical outcome of pyogenic liver abscess: An analysis from the National Health Insurance Research Database of Taiwan, 2000–2011. J. Microbiol. Immunol. Infect. 2016, 49, 646–653. [Google Scholar] [CrossRef]
- Li, W.; Chen, H.; Wu, S.; Peng, J. A comparison of pyogenic liver abscess in patients with or without diabetes: A retrospective study of 246 cases. BMC Gastroenterol. 2018, 18, 144. [Google Scholar] [CrossRef]
- Serraino, C.; Elia, C.; Bracco, C.; Rinaldi, G.; Pomero, F.; Silvestri, A.; Melchio, R.; Fenoglio, L.M. Characteristics and management of pyogenic liver abscess: A European experience. Medicine 2018, 97, e0628. [Google Scholar] [CrossRef]
- Rafat, C.; Messika, J.; Barnaud, G.; Dufour, N.; Magdoud, F.; Billard-Pomarès, T.; Gaudry, S.; Dreyfuss, D.; Branger, C.; Decré, D.; et al. Hypervirulent Klebsiella pneumoniae, a 5-year study in a French ICU. J. Med. Microbiol. 2018, 67, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Rossi, B.; Gasperini, M.L.; Leflon-Guibout, V.; Gioanni, A.; de Lastours, V.; Rossi, G.; Dokmak, S.; Ronot, M.; Roux, O.; Nicolas-Chanoine, M.H.; et al. Hypervirulent klebsiella pneumoniae in cryptogenic liver abscesses, Paris, France. Emerg. Infect. Dis. 2018, 24, 221–229. [Google Scholar] [CrossRef]
- He, S.; Yu, J.; Wang, H.; Chen, X.; He, Z.; Chen, Y. Percutaneous fine-needle aspiration for pyogenic liver abscess (3–6 cm): A two-center retrospective study. BMC Infect. Dis. 2020, 20, 516. [Google Scholar] [CrossRef] [PubMed]
- Qian, Y.; Wong, C.C.; Lai, S.; Chen, H.; He, X.; Sun, L.; Wu, J.; Zhou, J.; Yu, J.; Liu, W.; et al. A retrospective study of pyogenic liver abscess focusing on Klebsiella pneumoniae as a primary pathogen in China from 1994 to 2015. Sci. Rep. 2016, 6, 38587. [Google Scholar] [CrossRef] [PubMed]
- Ko, M.C.; Lin, W.H.; Martini, S.; Chang, Y.H.; Chiu, C.T.; Li, C.Y. A cohort study of age and sex specific risk of pyogenic liver abscess incidence in patients with type 2 diabetes mellitus. Medicine 2019, 98, e15366. [Google Scholar] [CrossRef] [PubMed]
- Molton, J.S.; Chan, M.; Kalimuddin, S.; Oon, J.; Young, B.E.; Low, J.G.; Salada, B.M.A.; Lee, T.H.; Wijaya, L.; Fisher, D.A.; et al. Oral vs intravenous antibiotics for patients with Klebsiella pneumoniae liver abscess: A randomized, controlled noninferiority study. Clin. Infect. Dis. 2019, 71, 952–959. [Google Scholar] [CrossRef] [PubMed]
- Marinova, P.; Stoykov, D.; Tonchev, P.; Dekova, I.; Sabotinov, T. Prognostic score in patients with pyogenic liver abscess-our results in surgical outcome and lethality predicting. HPB 2018, 20, S449–S450. [Google Scholar] [CrossRef][Green Version]
- Chen, S.C.; Lee, Y.T.; Tsai, S.J.; Lai, K.C.; Huang, C.C.; Wang, P.H.; Chen, C.C.; Lee, M.C. Clinical outcomes and prognostic factors of cancer patients with pyogenic liver abscess. J. Gastrointest. Surg. 2011, 15, 2036–2043. [Google Scholar] [CrossRef] [PubMed]
- Kuo, S.H.; Lee, Y.T.; Li, C.R.; Tseng, C.J.; Chao, W.N.; Wang, P.H.; Wong, R.H.; Chen, C.C.; Chen, S.C.; Lee, M.C. Mortality in emergency department sepsis score as a prognostic indicator in patients with pyogenic liver abscess. Am. J. Emerg. Med. 2013, 31, 916–921. [Google Scholar] [CrossRef]
- Lai, K.C.; Cheng, K.S.; Jeng, L.B.; Huang, C.C.; Lee, Y.T.; Chang, H.R.; Chen, C.C.; Chen, S.C.; Lee, M.C. Factors associated with treatment failure of percutaneous catheter drainage for pyogenic liver abscess in patients with hepatobiliary-pancreatic cancer. Am. J. Surg. 2013, 205, 52–57. [Google Scholar] [CrossRef]
- Chen, W.; Chen, C.H.; Chiu, K.L.; Lai, H.C.; Liao, K.F.; Ho, Y.J.; Hsu, W.H. Clinical outcome and prognostic factors of patients with pyogenic liver abscess requiring intensive care. Crit. Care Med. 2008, 36, 1184–1188. [Google Scholar] [CrossRef]
- Chen, S.C.; Tsai, S.J.; Chen, C.H.; Huang, C.C.; Lin, D.B.; Wang, P.H.; Chen, C.C.; Lee, M.C. Predictors of mortality in patients with pyogenic liver abscess. Neth. J. Med. 2008, 66, 196–203. [Google Scholar]
- Thng, C.B.; Tan, Y.P.; Shelat, V.G. Gas-forming pyogenic liver abscess: A world review. Ann. Hepatobiliary Pancreat. Surg. 2018, 22, 11–18. [Google Scholar] [CrossRef]
- Chen, Y.H.; Li, Y.H.; Lin, Y., Jr.; Chen, Y.P.; Wang, N.K.; Chao, A.N.; Liu, L.; Wu, W.C.; Lai, C.C.; Chen, T.L.; et al. Prognostic factors and visual outcomes of pyogenic liver abscess-related endogenous Klebsiella pneumoniae endophthalmitis: A 20-year retrospective review. Sci. Rep. 2019, 9, 1071. [Google Scholar] [CrossRef]
- de Grooth, H.J.; Geenen, I.L.; Girbes, A.R.; Vincent, J.L.; Parienti, J.J.; Oudemans-van Straaten, H.M. SOFA and mortality endpoints in randomized controlled trials: A systematic review and meta-regression analysis. Crit. Care 2017, 21, 38. [Google Scholar] [CrossRef] [PubMed]
- Raith, E.P.; Udy, A.A.; Bailey, M.; McGloughlin, S.; MacIsaac, C.; Bellomo, R.; Pilcher, D.V.; Australian and New Zealand Intensive Care Society (ANZICS) Centre for Outcomes and Resource Evaluation (CORE). Prognostic accuracy of the SOFA Score, SIRS Criteria, and qSOFA Score for in-hospital mortality among adults with suspected infection admitted to the intensive care unit. JAMA 2017, 317, 290–300. [Google Scholar] [CrossRef]
- Lie, K.C.; Lau, C.-Y.; Van Vinh Chau, N.; West, T.E.; Limmathurotsakul, D.; for Southeast Asia Infectious Disease Clinical Research Network. Utility of SOFA score, management and outcomes of sepsis in Southeast Asia: A multinational multicenter prospective observational study. J. Intensive Care 2018, 6, 9. [Google Scholar] [CrossRef]
- Zou, X.; Li, S.; Fang, M.; Hu, M.; Bian, Y.; Ling, J.; Yu, S.; Jing, L.; Li, D.; Huang, J. Acute physiology and chronic health evaluation II Score as a predictor of hospital mortality in patients of coronavirus disease 2019. Crit. Care Med. 2020, 48, e657–e665. [Google Scholar] [CrossRef]
- Siu, L.K.; Yeh, K.M.; Lin, J.C.; Fung, C.P.; Chang, F.Y. Klebsiella pneumoniae liver abscess: A new invasive syndrome. Lancet Infect. Dis. 2012, 12, 881–887. [Google Scholar] [CrossRef]
- Nates, J.L.; Nunnally, M.; Kleinpell, R.; Blosser, S.; Goldner, J.; Birriel, B.; Fowler, C.S.; Byrum, D.; Miles, W.S.; Bailey, H.; et al. ICU admission, discharge, and triage guidelines: A framework to enhance clinical operations, development of institutional policies, and further research. Crit. Care Med. 2016, 44, 1553–1602. [Google Scholar] [CrossRef]
- Vincent, J.L.; Moreno, R.; Takala, J.; Willatts, S.; De Mendonça, A.; Bruining, H.; Reinhart, C.K.; Suter, P.M.; Thijs, L.G. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996, 22, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.D.; Coopersmith, C.M.; et al. The third international consensus definitions for sepsis and septic shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [CrossRef] [PubMed]
- Knaus, W.A.; Draper, E.A.; Wagner, D.P.; Zimmerman, J.E. APACHE II: A severity of disease classification system. Crit. Care Med. 1985, 13, 818–829. [Google Scholar] [CrossRef]
- American College of Chest Physicians/Society of Critical Care Medicine Consensus Conference. Definitions for sepsis and organ failure and guidelines for the use of innovative therapies in sepsis. Crit. Care Med. 1992, 20, 864–874. [Google Scholar] [CrossRef]
- De Waele, J.J.; Boelens, J.; Leroux-Roels, I. Multidrug-resistant bacteria in ICU: Fact or myth. Curr. Opin. Anaesthesiol. 2020, 33, 156–161. [Google Scholar] [CrossRef]
- Spivak, E.S.; Cosgrove, S.E.; Srinivasan, A. Measuring appropriate antimicrobial use: Attempts at opening the black box. Clin. Infect. Dis. 2016, 63, 1639–1644. [Google Scholar] [CrossRef]
- Rismiller, K.; Haaga, J.; Siegel, C.; Ammori, J.B. Pyogenic liver abscesses: A contemporary analysis of management strategies at a tertiary institution. HPB 2017, 19, 889–893. [Google Scholar] [CrossRef] [PubMed]
- Solomkin, J.S.; Mazuski, J.E.; Bradley, J.S.; Rodvold, K.A.; Goldstein, E.J.; Baron, E.J.; O’Neill, P.J.; Chow, A.W.; Dellinger, E.P.; Eachempati, S.R.; et al. Diagnosis and management of complicated intra-abdominal infection in adults and children: Guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin. Infect. Dis. 2010, 50, 133–164. [Google Scholar] [CrossRef] [PubMed]
- Lee, I.R.; Molton, J.S.; Wyres, K.L.; Gorrie, C.; Wong, J.; Hoh, C.H.; Teo, J.; Kalimuddin, S.; Lye, D.C.; Archuleta, S.; et al. Differential host susceptibility and bacterial virulence factors driving Klebsiella liver abscess in an ethnically diverse population. Sci. Rep. 2016, 6, 29316. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | General Ward | Intensive Care Unit | p-Value |
|---|---|---|---|
| Number of patients | 215 | 109 | |
| Age, mean ± SD (years) | 57.8 (15.8) | 62.9 (15.7) | 0.007 |
| Sex, no. (%) | 0.403 | ||
| Male | 148 (68.8) | 70 (64.2) | |
| Female | 67 (31.2) | 39 (35.8) | |
| Comorbidities | |||
| Diabetes mellitus, no. (%) | 84 (39.1) | 61 (56.0) | 0.004 |
| Hemoglobin A1c, no. (%) (n = 137) | 0.244 | ||
| ≥10% (normal range 4.0–5.6%) | 27 (35.5) | 16 (26.2) | |
| Hypertension, no. (%) | 74 (34.4) | 52 (47.7) | 0.020 |
| Biliary disease, no. (%) | 39 (18.1) | 21 (19.3) | 0.805 |
| Chronic liver disease, no. (%) | 43 (20.0) | 20 (18.3) | 0.723 |
| Chronic kidney disease, no. (%) | 6 (2.8) | 7 (6.4) | 0.116 |
| Concomitant neoplasm, no. (%) | 23 (10.7) | 13 (11.9) | 0.739 |
| Alcohol consumption, no. (%) | 74 (34.4) | 33 (30.3) | 0.454 |
| Severity of illness on the day of hospitalization | |||
| Duration of hospitalization, mean ± SD (days) | 14.0 (7.9) | 26.1 (24.5) | <0.001 |
| SOFA, mean ± SD | 4.0 (2.0) | 7.3 (2.8) | <0.001 |
| SOFA ≥6, no. (%) | 43 (20.0) | 75 (68.8) | <0.001 |
| APACHE II score, mean ± SD | 12.6 (4.1) | 17.7 (6.6) | <0.001 |
| APACHE II score ≥18, no. (%) | 20 (9.3) | 42 (38.5) | <0.001 |
| Characteristics, no. (%) | General Ward (n = 215) | Intensive Care Unit (n = 109) | p-Value |
|---|---|---|---|
| Time from infection diagnosis to initiation of antibiotic use, mean ± SD (days) | 1.14 (0.9) | 1.27 (1.5) | 0.358 |
| Duration of parenteral antibiotics, mean ± SD (days) | 14.0 (7.9) | 21.7 (16.8) | <0.001 |
| Subsequent antibiotic treatment a, no. (%) | 82 (38.1) | 60 (55.0) | 0.004 |
| Inappropriate antibiotic therapy, no. (%) | 13 (6.0) | 11 (10.1) | 0.189 |
| Antibiotics used, no. (%) | 0.001 | ||
| Monotherapy | 173 (80.5) | 69 (63.3) | |
| Combination therapy | 42 (19.5) | 40 (36.7) | |
| Percutaneous catheter drainage, no. (%) | 116 (54.0) | 66 (60.6) | 0.258 |
| Clinical response, no. (%) | 0.008 | ||
| Response | 184 (85.6) | 80 (73.4) | |
| Non-response | 31 (14.4) | 29 (26.6) | |
| Surgical intervention, no. (%) | 6 (2.8) | 11 (10.1) | 0.005 |
| Complications | |||
| Metastatic infections, no. (%) (n = 324) | 8 (3.7) | 9 (8.3) | 0.032 |
| Abscess rupture, no. (%) (n = 324) | 2 (0.9) | 3 (2.8) | 0.209 |
| Septic shock, no. (%) | 25 (11.6) | 12 (11.0) | 0.501 |
| Concomitant infection b, no. (%) (n = 324) | 25 (11.6) | 66 (60.6) | <0.001 |
| Mortality, no. (%) | 1 (0.5) | 23 (21.1) | <0.001 |
| 30-Day mortality, no. (%) | <0.001 | ||
| Alive | 214 (99.5) | 86 (78.9) | |
| Death directly attributed to PLA | 1 (0.5) | 15 (13.8) | |
| Death due to complication or comorbidity | 0 | 8 (7.3) |
| Variables | Univariate Analysis | Multivariable Analysis | ||
|---|---|---|---|---|
| OR (95% CI) | p-Value | aOR a (95% CI) | p-Value | |
| Baseline Characteristics | ||||
| Age | 1.05 (1.02–1.09) | 0.001 | 1.04 (0.99–1.09) | 0.119 |
| Diabetes mellitus | ||||
| No | 1.00 | 1.00 | ||
| Yes | 1.50 (0.65–3.47) | 0.338 | 0.92 (0.27–3.19) | 0.893 |
| Hypertension | ||||
| No | 1.00 | 1.00 | ||
| Yes | 2.35 (1.01–5.47) | 0.047 | 2.56 (0.71–9.27) | 0.153 |
| SOFA | ||||
| <6 | 1.00 | 1.00 | ||
| ≥6 | 14.65 (4.27–50.30) | <0.001 | 1.96 (0.38–10.07) | 0.418 |
| APACHE II score | ||||
| <18 | 1.00 | 1.00 | ||
| ≥18 | 30.71 (10.00–94.32) | <0.001 | 19.31 (4.77–78.22) | <0.001 |
| Laboratory data and Complications | ||||
| Blood samples results | ||||
| No growth | 1.00 | 1.00 | ||
| Growth of blood samples | 1.35 (0.57–3.17) | 0.498 | 0.47 (0.07–3.36) | 0.453 |
| Metastatic infections | ||||
| No | 1.00 | 1.00 | ||
| Yes | 2.92 (0.78–10.96) | 0.113 | 9.74 (0.91–104.22) | 0.060 |
| Concomitant infections | ||||
| No | 1.00 | 1.00 | ||
| Yes | 36.83 (8.45–160.53) | <0.001 | 34.33 (5.60–210.55) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, Y.-T.; Wang, C.-C.; Li, C.-F.; Chen, H.-Y.; Liao, H.-H.; Lin, C.-C. Utility of Acute Physiology and Chronic Health Evaluation (APACHE II) in Predicting Mortality in Patients with Pyogenic Liver Abscess: A Retrospective Study. J. Clin. Med. 2021, 10, 2644. https://doi.org/10.3390/jcm10122644
Lee Y-T, Wang C-C, Li C-F, Chen H-Y, Liao H-H, Lin C-C. Utility of Acute Physiology and Chronic Health Evaluation (APACHE II) in Predicting Mortality in Patients with Pyogenic Liver Abscess: A Retrospective Study. Journal of Clinical Medicine. 2021; 10(12):2644. https://doi.org/10.3390/jcm10122644
Chicago/Turabian StyleLee, Yuan-Ti, Chi-Chih Wang, Chien-Feng Li, Hsuan-Yi Chen, Hsien-Hua Liao, and Chia-Chun Lin. 2021. "Utility of Acute Physiology and Chronic Health Evaluation (APACHE II) in Predicting Mortality in Patients with Pyogenic Liver Abscess: A Retrospective Study" Journal of Clinical Medicine 10, no. 12: 2644. https://doi.org/10.3390/jcm10122644
APA StyleLee, Y.-T., Wang, C.-C., Li, C.-F., Chen, H.-Y., Liao, H.-H., & Lin, C.-C. (2021). Utility of Acute Physiology and Chronic Health Evaluation (APACHE II) in Predicting Mortality in Patients with Pyogenic Liver Abscess: A Retrospective Study. Journal of Clinical Medicine, 10(12), 2644. https://doi.org/10.3390/jcm10122644