
Development of a Novel Dorsal Incision Only Invagination Type Pancreatogastrostomy (Charité-PG) Following Open Pancreaticoduodenectomy—A Single Centre Experience


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Collection and Exclusion Criteria
2.2. Preoperative Assessment and Preparation
2.3. Surgical Approach
2.4. Reconstruction Following PD via vgPG
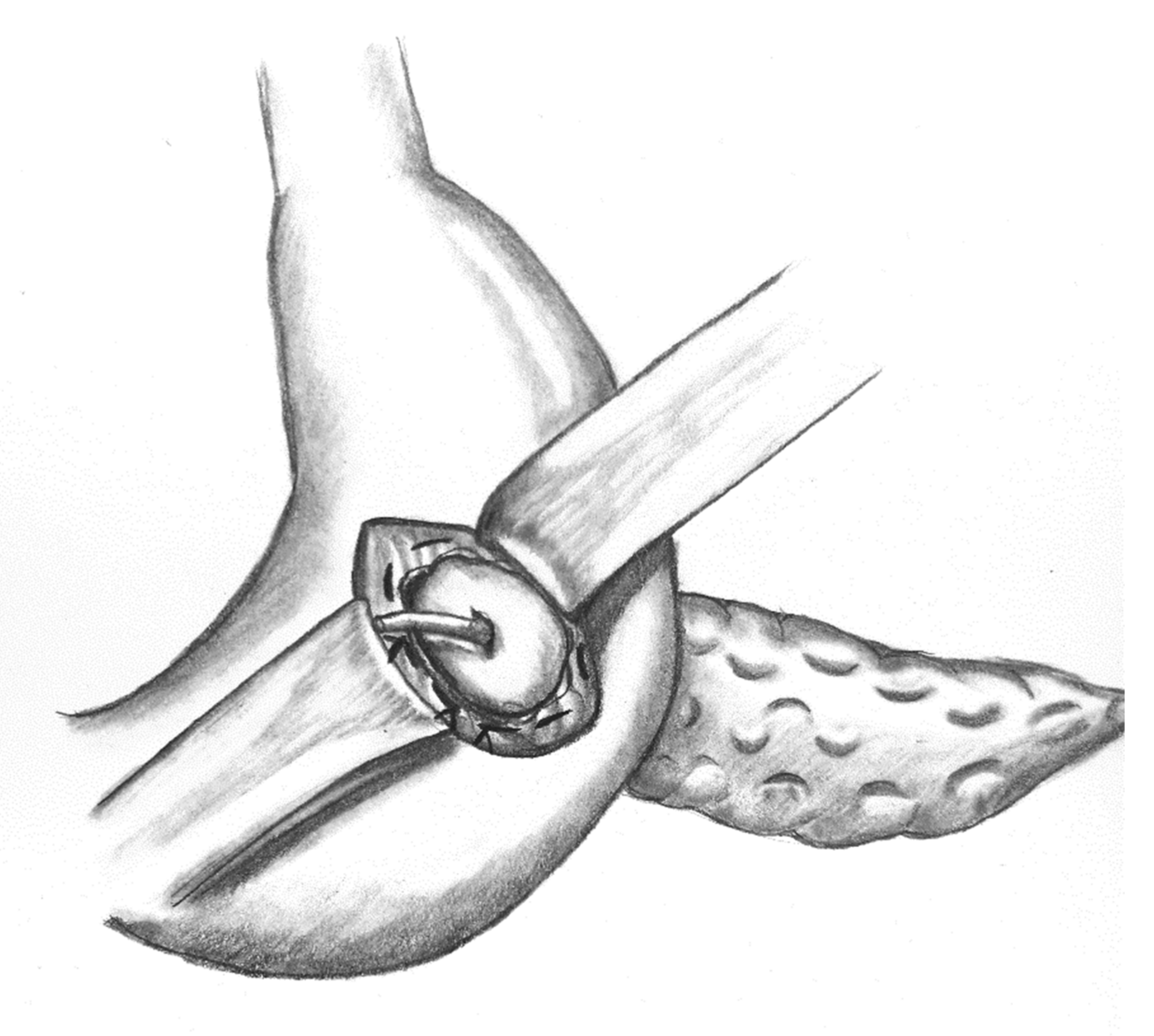
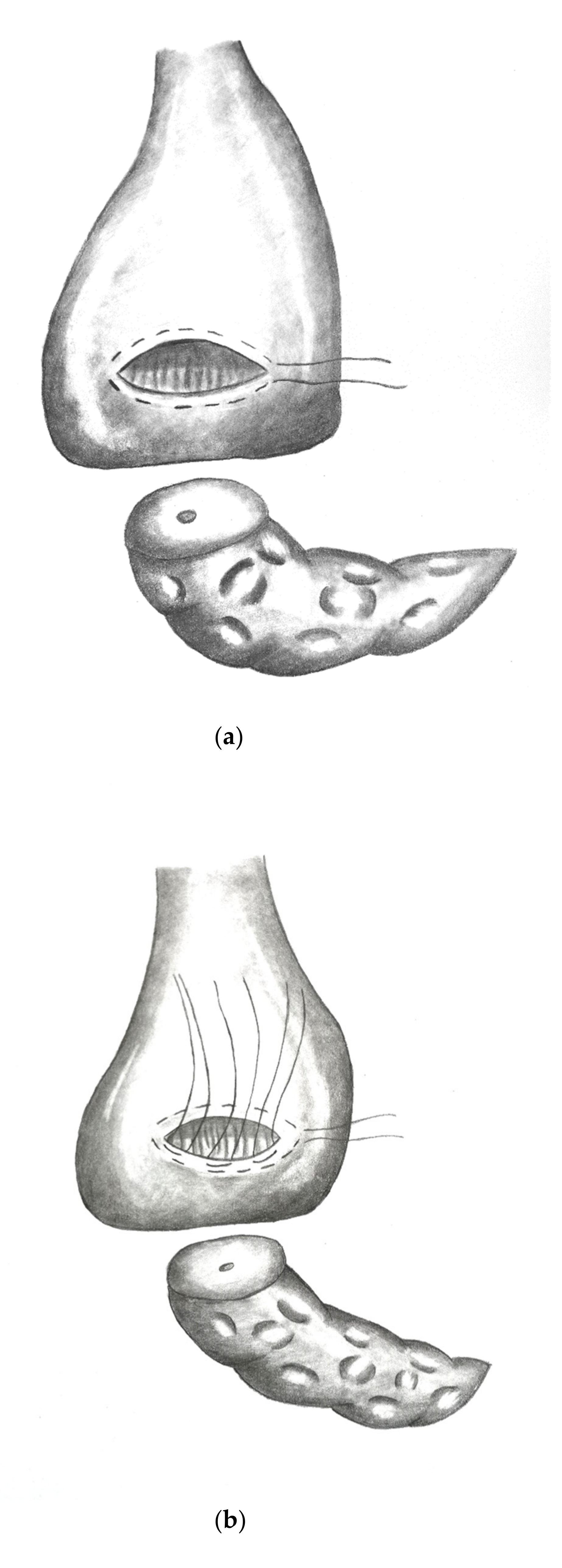
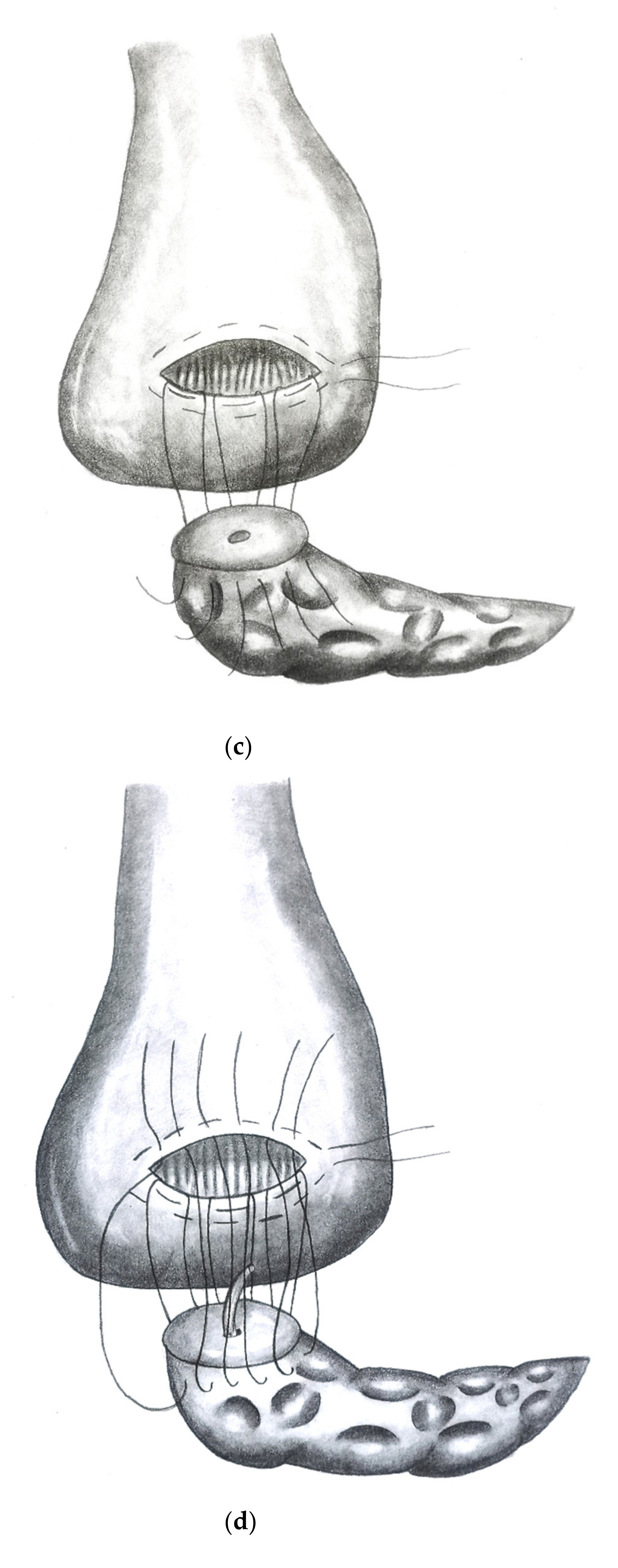
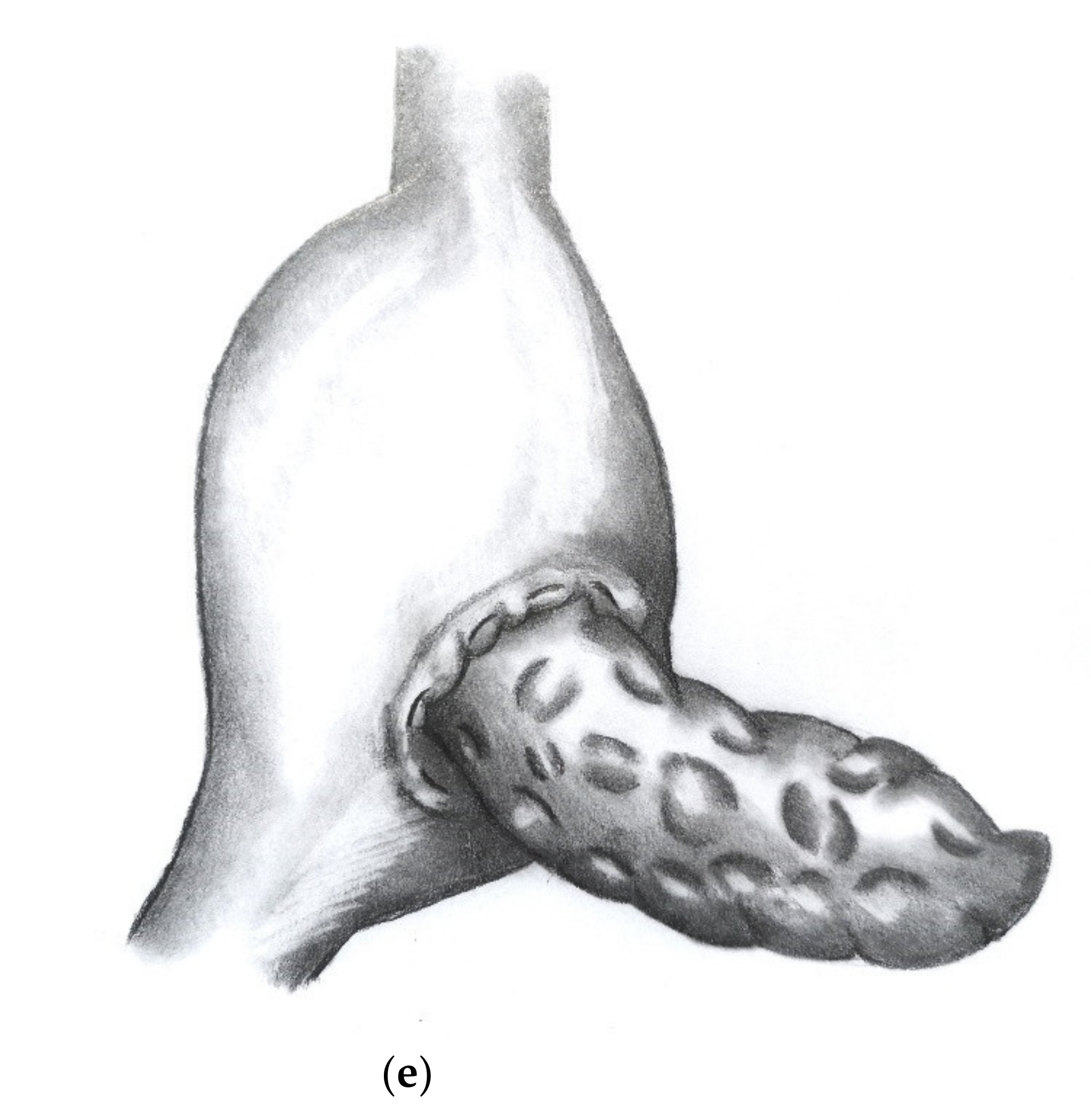
2.5. Reconstruction Following PD via dioPG (“Charité-PG”)
2.6. Postoperative Course
2.7. Statistics
3. Results
3.1. Patients’ Characteristics
3.2. Perioperative Parameters
3.3. Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Schnelldorfer, T.; Adams, D.B.; Warshaw, A.L.; Lillemoe, K.D.; Sarr, M.G. Forgotten pioneers of pancreatic surgery: Beyond the favorite few. Ann. Surg. 2008, 247, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Kausch, W. Das Carcinom der Papilla duodeni und seine radikale Entfernung. Beiträge Klin. Chir. 1912, 78, 439–486. [Google Scholar]
- Whipple, A.O. Observations on radical surgery for lesions of the pancreas. Surg. Gynecol. Obstet. 1946, 82, 623–631. [Google Scholar]
- Cattell, R.B. Anastomosis of the duct of Wirsung; its use in palliative operations for cancer of the head of the pancreas. Surg. Clin. N. Am. 1947, 27, 636–643. [Google Scholar] [CrossRef]
- Grobmyer, S.R.; Kooby, D.; Blumgart, L.H.; Hochwald, S.N. Novel pancreaticojejunostomy with a low rate of anastomotic failure-related complications. J. Am. Coll. Surg. 2010, 210, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Cao, F.; Tong, X.; Li, A.; Li, J.; Li, F. Meta-analysis of modified Blumgart anastomosis and interrupted transpancreatic suture in pancreaticojejunostomy after pancreaticoduodenectomy. Asian J. Surg. 2020. [Google Scholar] [CrossRef]
- Waugh, J.M.; Clagett, O.T. Resection of the duodenum and head of the pancreas for carcinoma; an analysis of thirty cases. Surgery 1946, 20, 224–232. [Google Scholar]
- Barreto, S.G.; Shukla, P.J. Different types of pancreatico-enteric anastomosis. Transl. Gastroenterol. Hepatol. 2017, 2, 89. [Google Scholar] [CrossRef] [PubMed]
- Wente, M.N.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.; Padbury, R.T.; Sarr, M.G.; Traverso, L.W.; et al. Delayed gastric emptying (DGE) after pancreatic surgery: A suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007, 142, 761–768. [Google Scholar] [CrossRef]
- Wente, M.N.; Veit, J.A.; Bassi, C.; Dervenis, C.; Fingerhut, A.; Gouma, D.J.; Izbicki, J.R.; Neoptolemos, J.; Padbury, R.T.; Sarr, M.G.; et al. Postpancreatectomy hemorrhage (PPH): An International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007, 142, 20–25. [Google Scholar] [CrossRef]
- Bassi, C.; Marchegiani, G.; Dervenis, C.; Sarr, M.; Abu Hilal, M.; Adham, M.; Allen, P.; Andersson, R.; Asbun, H.J.; Besselink, M.G.; et al. The 2016 update of the International Study Group (ISGPS) definition and grading of postoperative pancreatic fistula: 11 Years After. Surgery 2017, 161, 584–591. [Google Scholar] [CrossRef] [PubMed]
- Dindo, D.; Demartines, N.; Clavien, P.A. Classification of surgical complications: A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann. Surg. 2004, 240, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Pedrazzoli, S. Pancreatoduodenectomy (PD) and postoperative pancreatic fistula (POPF): A systematic review and analysis of the POPF-related mortality rate in 60,739 patients retrieved from the English literature published between 1990 and 2015. Med. Baltim. 2017, 96, e6858. [Google Scholar] [CrossRef] [PubMed]
- Kawaida, H.; Kono, H.; Hosomura, N.; Amemiya, H.; Itakura, J.; Fujii, H.; Ichikawa, D. Surgical techniques and postoperative management to prevent postoperative pancreatic fistula after pancreatic surgery. World J. Gastroenterol. 2019, 25, 3722–3737. [Google Scholar] [CrossRef]
- Callery, M.P.; Pratt, W.B.; Kent, T.S.; Chaikof, E.L.; Vollmer, C.M., Jr. A prospectively validated clinical risk score accurately predicts pancreatic fistula after pancreatoduodenectomy. J. Am. Coll. Surg. 2013, 216, 1–14. [Google Scholar] [CrossRef]
- Mungroop, T.H.; van Rijssen, L.B.; van Klaveren, D.; Smits, F.J.; van Woerden, V.; Linnemann, R.J.; de Pastena, M.; Klompmaker, S.; Marchegiani, G.; Ecker, B.L.; et al. Alternative Fistula Risk Score for Pancreatoduodenectomy (a-FRS): Design and International External Validation. Ann. Surg. 2019, 269, 937–943. [Google Scholar] [CrossRef]
- Ecker, B.L.; McMillan, M.T.; Maggino, L.; Allegrini, V.; Asbun, H.J.; Ball, C.G.; Bassi, C.; Beane, J.; Behrman, S.W.; Berger, A.C.; et al. Pancreatogastrostomy Vs. Pancreatojejunostomy: A Risk-Stratified Analysis of 5316 Pancreatoduodenectomies. J. Gastrointest. Surg. 2018, 22, 68–76. [Google Scholar] [CrossRef]
- Keck, T.; Wellner, U.F.; Bahra, M.; Klein, F.; Sick, O.; Niedergethmann, M.; Wilhelm, T.J.; Farkas, S.A.; Börner, T.; Bruns, C.; et al. Pancreatogastrostomy Versus Pancreatojejunostomy for RECOnstruction After PANCreatoduodenectomy (RECOPANC, DRKS 00000767): Perioperative and Long-term Results of a Multicenter Randomized Controlled Trial. Ann. Surg. 2016, 263, 440–449. [Google Scholar] [CrossRef]
- Perivoliotis, K.; Sioka, E.; Tatsioni, A.; Stefanidis, I.; Zintzaras, E.; Zacharoulis, D. Pancreatogastrostomy versus Pancreatojejunostomy: An Up-to-Date Meta-Analysis of RCTs. Int. J. Surg. Oncol. 2017, 2017, 7526494. [Google Scholar] [CrossRef]
- Jin, Y.; Feng, Y.Y.; Qi, X.G.; Hao, G.; Yu, Y.Q.; Li, J.T.; Peng, S.Y. Pancreatogastrostomy vs pancreatojejunostomy after pancreaticoduodenectomy: An updated meta-analysis of RCTs and our experience. World J. Gastrointest. Surg. 2019, 11, 322–332. [Google Scholar] [CrossRef]
- Ke, Z.; Cui, J.; Hu, N.; Yang, Z.; Chen, H.; Hu, J.; Wang, C.; Wu, H.; Nie, X.; Xiong, J. Risk factors for postoperative pancreatic fistula: Analysis of 170 consecutive cases of pancreaticoduodenectomy based on the updated ISGPS classification and grading system. Med. Baltim. 2018, 97, e12151. [Google Scholar] [CrossRef] [PubMed]
- Hayama, S.; Senmaru, N.; Hirano, S. Delayed gastric emptying after pancreatoduodenectomy: Comparison between invaginated pancreatogastrostomy and pancreatojejunostomy. BMC Surg. 2020, 20, 60. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics N (%) | All Patients (N = 141) | dioPG (N = 49) | vgPG (N = 92) | p-Value |
|---|---|---|---|---|
| Sex N (%) | 0.896 | |||
| Male | 68 (48.2) | 24 (49) | 44 (47.8) | |
| Female | 73 (51.8) | 25 (51) | 48 (52.2) | |
| Age (years) | ||||
| Mean | 64 | 66.43 | 62.71 | 0.092 |
| Minimum | 23 | 46 | 23 | |
| Maximum | 88 | 88 | 85 | |
| ASA Score N (%) | 0.608 | |||
| 1 | 2 (1.4) | 0 (0) | 2 (2.2) | |
| 2 | 74 (52.2) | 24 (49) | 50 (54.3) | |
| 3 | 57 (40.4) | 21 (42.9) | 36 (39.1) | |
| 4 | 1 (0.7) | 0 (0) | 1 (1.1) | |
| BMI N (%) | 0.666 | |||
| Mean | 24.8 | 25.2 | 24.6 | |
| Minimum | 15.2 | 17.4 | 15.2 | |
| Maximum | 41.8 | 41.8 | 39.5 | |
| Indication | ||||
| Malignoma | 104 (73.8) | 36 (73.5) | 68 (73.9) | |
| Benign Lesion | 37 (26.2) | 13 (26.5) | 24 (26.1) |
| Characteristics N (%) | All Patients (N = 141) | dioPG (N = 49) | vgPG (N = 92) | p-Value |
|---|---|---|---|---|
| R0 Resection State N (%) | 66 (63.5) | 25 (67.6) | 41 (61.2) | 0.511 |
| Operation Time (min) | ||||
| Mean | 312.5 | 297.5 | 320.5 | 0.04 |
| Minimum | 162 | 162 | 191 | |
| Maximum | 485 | 437 | 485 | |
| Overall Complications N (%) | 97 (68.8) | 31 (63.3) | 66 (71.7) | 0.301 |
| Clavien/Dindo Classification N(%) | 0.6 | |||
| 0 | 44 (31.2) | 18 (36.7) | 26 (28.3) | |
| 1 | 14 (9.9) | 4 (8.2) | 10 (10.9) | |
| 2 | 12 (8.5) | 6 (12.2) | 6 (6.5) | |
| 3a | 34 (24.1) | 5 (10.2) | 29 (31.5) | |
| 3b | 11 (7.8) | 4 (8.2) | 7 (7.6) | |
| 4a | 15 (10.6) | 9 (18.4) | 6 (6.5) | |
| 4b | 2 (1.4) | 0 (0) | 2 (2.2) | |
| 5 | 9 (6.4) | 3 (6.1) | 6 (6.5) | |
| POPF N(%) | 0.737 | |||
| Biochemical Leak | 5 (3.5) | 2 (4.1) | 3 (3.3) | |
| B | 18 (12.8) | 7 (14.3) | 11 (12) | |
| C | 2 (1.4) | 0 (0) | 2 (2.2) | |
| PPH N (%) | 0.899 | |||
| A | 5 (3.5) | 2 (4.1) | 3 (3.3) | |
| B | 12 (8.5) | 5 (10.2) | 7 (7.6) | |
| C | 2 (1.4) | 1 (2) | 1 (1.1) | |
| SSI N (%) | 22 (15.6) | 7 (14.3) | 15 (16.3) | 0.753 |
| DGE N (%) | 28 (19.9) | 5 (10.2) | 23 (25) | 0.036 |
| PG-Insufficiency N (%) | 7 (5) | 3 (6.1) | 4 (4.3) | 0.644 |
| Insufficiency hepaticojejunostomy N (%) | 11 (7.8) | 4 (8.2) | 7 (7.6) | 0.907 |
| Reoperation Rate N (%) | 16 (11.3) | 3 (6.1) | 13 (14.1) | 0.153 |
| Intervention N (%) | 53 (37.6) | 15 (30.6) | 38 (41.3) | 0.212 |
| 30-day Mortality N (%) | 7 (5) | 2 (4.1) | 5 (5.4) | 0.725 |
| 90-day Readmission Rate N (%) | 12 (8.5) | 4 (8.2) | 8 (8.7) | 0.914 |
| In-hospital stay (days) | ||||
| Mean | 19.79 | 18.37 | 20.54 | 0.261 |
| Minimum | 7 | 9 | 7 | |
| Maximum | 59 | 59 | 56 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Timmermann, L.; Bahra, M.; Pratschke, J.; Malinka, T. Development of a Novel Dorsal Incision Only Invagination Type Pancreatogastrostomy (Charité-PG) Following Open Pancreaticoduodenectomy—A Single Centre Experience. J. Clin. Med. 2021, 10, 2573. https://doi.org/10.3390/jcm10122573
Timmermann L, Bahra M, Pratschke J, Malinka T. Development of a Novel Dorsal Incision Only Invagination Type Pancreatogastrostomy (Charité-PG) Following Open Pancreaticoduodenectomy—A Single Centre Experience. Journal of Clinical Medicine. 2021; 10(12):2573. https://doi.org/10.3390/jcm10122573
Chicago/Turabian StyleTimmermann, Lea, Marcus Bahra, Johann Pratschke, and Thomas Malinka. 2021. "Development of a Novel Dorsal Incision Only Invagination Type Pancreatogastrostomy (Charité-PG) Following Open Pancreaticoduodenectomy—A Single Centre Experience" Journal of Clinical Medicine 10, no. 12: 2573. https://doi.org/10.3390/jcm10122573
APA StyleTimmermann, L., Bahra, M., Pratschke, J., & Malinka, T. (2021). Development of a Novel Dorsal Incision Only Invagination Type Pancreatogastrostomy (Charité-PG) Following Open Pancreaticoduodenectomy—A Single Centre Experience. Journal of Clinical Medicine, 10(12), 2573. https://doi.org/10.3390/jcm10122573