
Evaluation of Intracranial Hypertension in Traumatic Brain Injury Patient: A Noninvasive Approach Based on Cranial Computed Tomography Features


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Setting
2.2. Data Sources and Measurements
2.3. Statistical Analysis
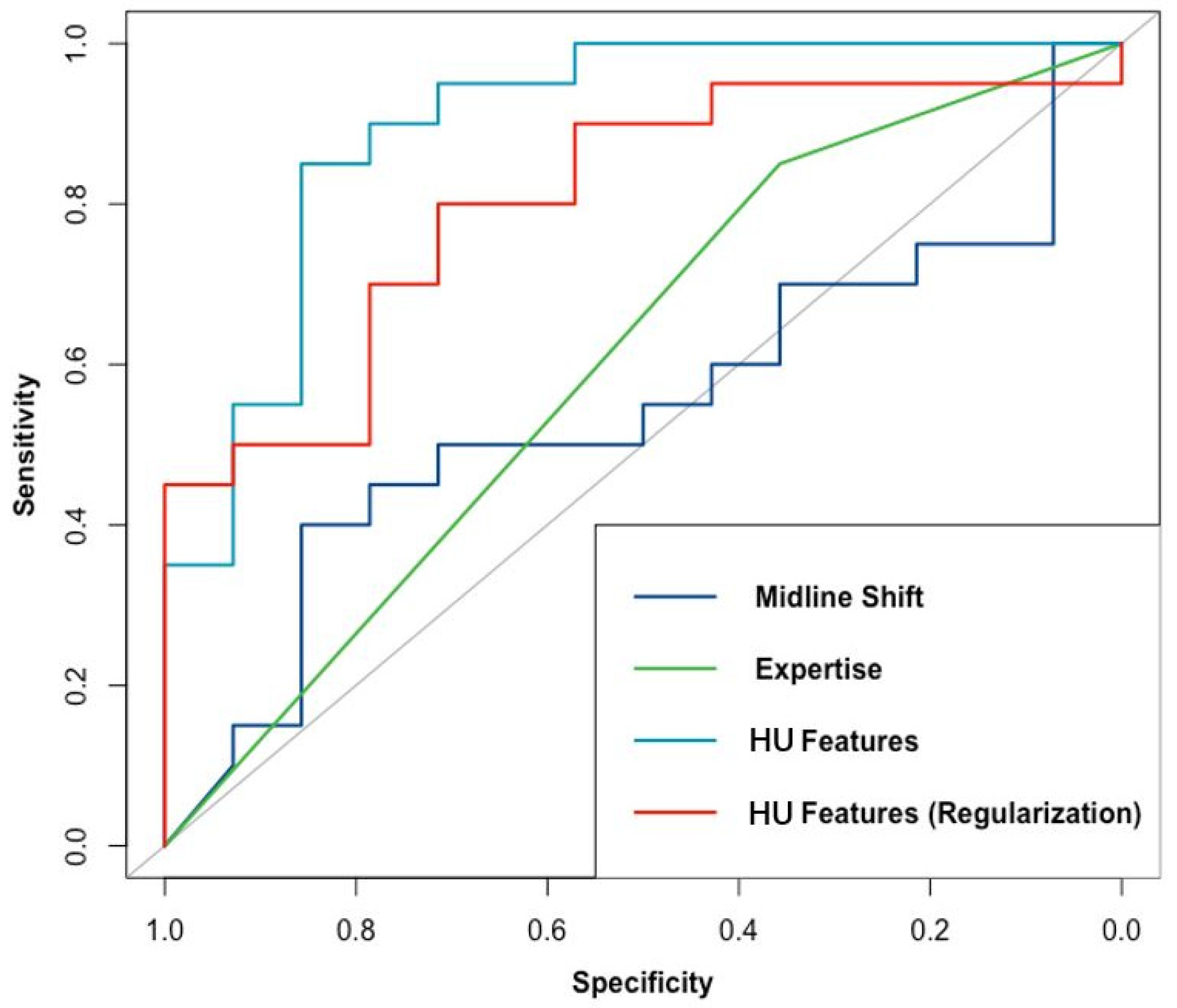
3. Results
Comparative Results of the Three Models
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roozenbeek, B.; Maas, A.I.; Menon, D.K. Changing patterns in the epidemiology of traumatic brain injury. Nat. Rev. Neurol. 2013, 9, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Galgano, M.; Toshkezi, G.; Qiu, X.; Russell, T.; Chin, L.; Zhao, L.R. Traumatic Brain Injury: Current Treatment Strategies and Future Endeavors. Cell Transplant. 2017, 26, 1118–1130. [Google Scholar] [CrossRef]
- Harary, M.; Dolmans, R.G.F.; Gormley, W.B. Intracranial Pressure Monitoring-Review and Avenues for Development. Sensors (Basel) 2018, 18, 465. [Google Scholar] [CrossRef]
- Nag, D.S.; Sahu, S.; Swain, A.; Kant, S. Intracranial pressure monitoring: Gold standard and recent innovations. World J. Clin. Cases 2019, 7, 1535–1553. [Google Scholar] [CrossRef] [PubMed]
- Narayan, V.; Mohammed, N.; Savardekar, A.R.; Patra, D.P.; Notarianni, C.; Nanda, A. Noninvasive Intracranial Pressure Monitoring for Severe Traumatic Brain Injury in Children: A Concise Update on Current Methods. World Neurosurg. 2018, 114, 293–300. [Google Scholar] [CrossRef]
- Nagesh, M.; Patel, K.R.; Mishra, A.; Yeole, U.; Prabhuraj, A.R.; Shukla, D. Role of repeat CT in mild to moderate head injury: An institutional study. Neurosurg. Focus 2019, 47, E2. [Google Scholar] [CrossRef] [PubMed]
- Nelson, D.W.; Nystrom, H.; MacCallum, R.M.; Thornquist, B.; Lilja, A.; Bellander, B.M.; Rudehill, A.; Wanecek, M.; Weitzberg, E. Extended analysis of early computed tomography scans of traumatic brain injured patients and relations to outcome. J. Neurotrauma 2010, 27, 51–64. [Google Scholar] [CrossRef] [PubMed]
- Alali, A.S.; Temkin, N.; Barber, J.; Pridgeon, J.; Chaddock, K.; Dikmen, S.; Hendrickson, P.; Videtta, W.; Lujan, S.; Petroni, G.; et al. A clinical decision rule to predict intracranial hypertension in severe traumatic brain injury. J. Neurosurg. 2018, 131, 612–619. [Google Scholar] [CrossRef]
- Yuh, E.L.; Cooper, S.R.; Ferguson, A.R.; Manley, G.T. Quantitative CT improves outcome prediction in acute traumatic brain injury. J. Neurotrauma 2012, 29, 735–746. [Google Scholar] [CrossRef]
- Friedman, J.; Hastie, T.; Tibshirani, R. Regularization Paths for Generalized Linear Models via Coordinate Descent. J. Stat. Softw. 2010, 33, 1–22. [Google Scholar] [CrossRef] [PubMed]
- Bobinski, L.; Olivecrona, M.; Koskinen, L.O. Dynamics of brain tissue changes induced by traumatic brain injury assessed with the Marshall, Morris-Marshall, and the Rotterdam classifications and its impact on outcome in a prostacyclin placebo-controlled study. Acta Neurochir. (Wien) 2012, 154, 1069–1079. [Google Scholar] [CrossRef] [PubMed]
- Mata-Mbemba, D.; Mugikura, S.; Nakagawa, A.; Murata, T.; Ishii, K.; Li, L.; Takase, K.; Kushimoto, S.; Takahashi, S. Early CT findings to predict early death in patients with traumatic brain injury: Marshall and Rotterdam CT scoring systems compared in the major academic tertiary care hospital in northeastern Japan. Acad. Radiol. 2014, 21, 605–611. [Google Scholar] [CrossRef]
- Mahadewa, T.G.B.; Golden, N.; Saputra, A.; Ryalino, C. Modified Revised Trauma-Marshall score as a proposed tool in predicting the outcome of moderate and severe traumatic brain injury. Open Access Emerg. M 2018, 10, 135–139. [Google Scholar] [CrossRef]
- Olivecrona, Z.; Bobinski, L.; Koskinen, L.O. Association of ICP, CPP, CT findings and S-100B and NSE in severe traumatic head injury. Prognostic value of the biomarkers. Brain Inj. 2015, 29, 446–454. [Google Scholar] [CrossRef]
- Eide, P.K. The relationship between intracranial pressure and size of cerebral ventricles assessed by computed tomography. Acta Neurochir. (Wien) 2003, 145, 171–179. [Google Scholar] [CrossRef] [PubMed]
- Pappu, S.; Lerma, J.; Khraishi, T. Brain CT to Assess Intracranial Pressure in Patients with Traumatic Brain Injury. J. Neuroimaging 2016, 26, 37–40. [Google Scholar] [CrossRef]
- Oliveira, R.A.; de Oliveira Lima, M.; Paiva, W.S.; de Sa Malbouisson, L.M.; Teixeira, M.J.; Bor-Seng-Shu, E. Comparison between Brain Computed Tomography Scan and Transcranial Sonography to Evaluate Third Ventricle Width, Peri-Mesencephalic Cistern, and Sylvian Fissure in Traumatic Brain-Injured Patients. Front. Neurol. 2017, 8, 44. [Google Scholar] [CrossRef]
- Kanazawa, T.; Takahashi, S.; Minami, Y.; Jinzaki, M.; Toda, M.; Yoshida, K. Early prediction of clinical outcomes in patients with aneurysmal subarachnoid hemorrhage using computed tomography texture analysis. J. Clin. Neurosci. 2020, 71, 144–149. [Google Scholar] [CrossRef]
- Shen, Q.; Shan, Y.; Hu, Z.; Chen, W.; Yang, B.; Han, J.; Huang, Y.; Xu, W.; Feng, Z. Quantitative parameters of CT texture analysis as potential markersfor early prediction of spontaneous intracranial hemorrhage enlargement. Eur. Radiol. 2018, 28, 4389–4396. [Google Scholar] [CrossRef] [PubMed]
- Inaba, K.; Teixeira, P.G.R.; David, J.S.; Brown, C.; Salim, A.; Rhee, P.; Browder, T.; Dubose, J.; Demetriades, D. Computed tomographic brain density measurement as a predictor of elevated intracranial pressure in blunt head trauma. Am. Surgeon. 2007, 73, 1023–1026. [Google Scholar] [CrossRef] [PubMed]
- Lazaridis, C.; Rusin, C.G.; Robertson, C.S. Secondary brain injury: Predicting and preventing insults. Neuropharmacology 2019, 145, 145–152. [Google Scholar] [CrossRef]
- Sorrentino, E.; Diedler, J.; Kasprowicz, M.; Budohoski, K.P.; Haubrich, C.; Smielewski, P.; Outtrim, J.G.; Manktelow, A.; Hutchinson, P.J.; Pickard, J.D.; et al. Critical thresholds for cerebrovascular reactivity after traumatic brain injury. Neurocrit Care 2012, 16, 258–266. [Google Scholar] [CrossRef]
- Jiang, J.Y.; Xu, W.; Li, W.P.; Xu, W.H.; Zhang, J.; Bao, Y.H.; Ying, Y.H.; Luo, Q.Z. Efficacy of standard trauma craniectomy for refractory intracranial hypertension with severe traumatic brain injury: A multicenter, prospective, randomized controlled study. J. Neurotrauma 2005, 22, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Moore, N.A.; Brennan, P.M.; Baillie, J.K. Wide variation and systematic bias in expert clinicians’ perceptions of prognosis following brain injury. Br. J. Neurosurg. 2013, 27, 340–343. [Google Scholar] [CrossRef] [PubMed]
- Kahraman, S.; Dutton, R.P.; Hu, P.; Stansbury, L.; Xiao, Y.; Stein, D.M.; Scalea, T.M. Heart rate and pulse pressure variability are associated with intractable intracranial hypertension after severe traumatic brain injury. J. Neurosurg. Anesthesiol. 2010, 22, 296–302. [Google Scholar] [CrossRef] [PubMed]
- Delic, J.; Alhilali, L.; Hughes, M.; Gumus, S.; Fakhran, S. White Matter Injuries in Mild Traumatic Brain Injury and Posttraumatic Migraines: Diffusion Entropy Analysis. Radiology. Radiology 2016, 279, 859–866. [Google Scholar] [CrossRef]
- Cao, C.; Slobounov, S. Application of a novel measure of EEG non-stationarity as ‘Shannon- entropy of the peak frequency shifting’ for detecting residual abnormalities in concussed individuals. Clin. Neurophysiol. 2011, 122, 1314–1321. [Google Scholar] [CrossRef]
- Cardim, D.; Robba, C.; Schmidt, B. Midline shift in patients with closed traumatic brain injury may be driven by cerebral perfusion pressure not intracranial pressure. J. Neurosurg. Sci. 2019. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients with TBI (n = 47) | Patients with Unilateral TBI (n = 34) | |
|---|---|---|
| Initial ICP (mmHg) a | 25 (20–30) | 25 (19–30) |
| >22 mmHg | 29 (62.07%) | 20 (58.73%) |
| Midline shift (mm) a | 4.17 (1.17–6.02) | 3.75 (1.15–6.06) |
| Mean HU | ||
| Higher-value side b | 37.25 (4.87) | 37.72 (5.20) |
| Lower-value side b | 32.31 (3.11) | 32.77 (3.18) |
| Ratio a | 1.10 (1.04–1.24) | 1.10 (1.03–1.25) |
| Standard deviation of HU | ||
| Higher-value side b | 12.09 (3.06) | 12.33 (3.43) |
| Lower-value side b | 8.93 (1.82) | 8.77 (1.80) |
| Ratio a | 1.25 (1.09–1.55) | 1.31 (1.12–1.65) |
| Shannon entropy of HU | ||
| Total on both sides a | 1.94 (1.76–2.07) | 1.94 (1.73–2.04) |
| Higher-value side a | 1.93 (1.78–2.05) | 1.92 (1.75–2.04) |
| Lower-value side a | 1.69 (1.57–1.80) | 1.66 (1.57–1.78) |
| Ratio a | 1.11 (1.05–1.21) | 1.13 (1.05–1.19) |
| HU Features | HU Features (Regularized) | Midline Shift | Expertise | |
|---|---|---|---|---|
| Accuracy | 80.85% | 65.96% | 61.70% | 63.83% |
| Precision | 83.33% | 84.21% | 61.70% | 67.65% |
| Recall | 86.21% | 55.17% | 100.00% | 79.31% |
| F1 Score | 0.85 | 0.79 | 0.76 | 0.78 |
| AUC (95% CI) | 0.81 (0.68–0.94) | 0.73 (0.58–0.88) | 0.49 (0.32–0.66) | 0.59 (0.45–0.73) |
| HU Features | HU Features (Regularized) | Midline Shift | Expertise | |
|---|---|---|---|---|
| Accuracy | 85.29% | 70.59% | 58.82% | 64.71% |
| Precision | 85.71% | 67.86% | 58.82% | 65.38% |
| Recall | 90.00% | 95.00% | 100.00% | 85.00% |
| F1 Score | 0.88 | 0.79 | 0.74 | 0.74 |
| AUC (95% CI) | 0.90 (0.78–1.00) | 0.80 (0.65–0.95) | 0.54 (0.34–0.74) | 0.60 (0.45–0.76) |
| HU Model | Midline Shift Model | |
|---|---|---|
| All TBI patients (n = 47) | ||
| Accuracy | 61.70% | 40.43% |
| Precision * | 61.06% | 32.90% |
| Recall * | 61.70% | 40.43% |
| F1 Score * | 0.61 | 0.29 |
| Unilateral TBI patients (n = 34) | ||
| Accuracy | 64.71% | 41.18% |
| Precision * | 64.02% | 16.96% |
| Recall * | 64.71% | 41.18% |
| F1 Score * | 0.64 | 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shan, Y.; Li, Y.; Xu, X.; Feng, J.; Wu, X.; Gao, G. Evaluation of Intracranial Hypertension in Traumatic Brain Injury Patient: A Noninvasive Approach Based on Cranial Computed Tomography Features. J. Clin. Med. 2021, 10, 2524. https://doi.org/10.3390/jcm10112524
Shan Y, Li Y, Xu X, Feng J, Wu X, Gao G. Evaluation of Intracranial Hypertension in Traumatic Brain Injury Patient: A Noninvasive Approach Based on Cranial Computed Tomography Features. Journal of Clinical Medicine. 2021; 10(11):2524. https://doi.org/10.3390/jcm10112524
Chicago/Turabian StyleShan, Yingchi, Yihua Li, Xuxu Xu, Junfeng Feng, Xiang Wu, and Guoyi Gao. 2021. "Evaluation of Intracranial Hypertension in Traumatic Brain Injury Patient: A Noninvasive Approach Based on Cranial Computed Tomography Features" Journal of Clinical Medicine 10, no. 11: 2524. https://doi.org/10.3390/jcm10112524
APA StyleShan, Y., Li, Y., Xu, X., Feng, J., Wu, X., & Gao, G. (2021). Evaluation of Intracranial Hypertension in Traumatic Brain Injury Patient: A Noninvasive Approach Based on Cranial Computed Tomography Features. Journal of Clinical Medicine, 10(11), 2524. https://doi.org/10.3390/jcm10112524