
Perihematomal Edema and Clinical Outcome in Intracerebral Hemorrhage Related to Different Oral Anticoagulants

 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Material and Methods
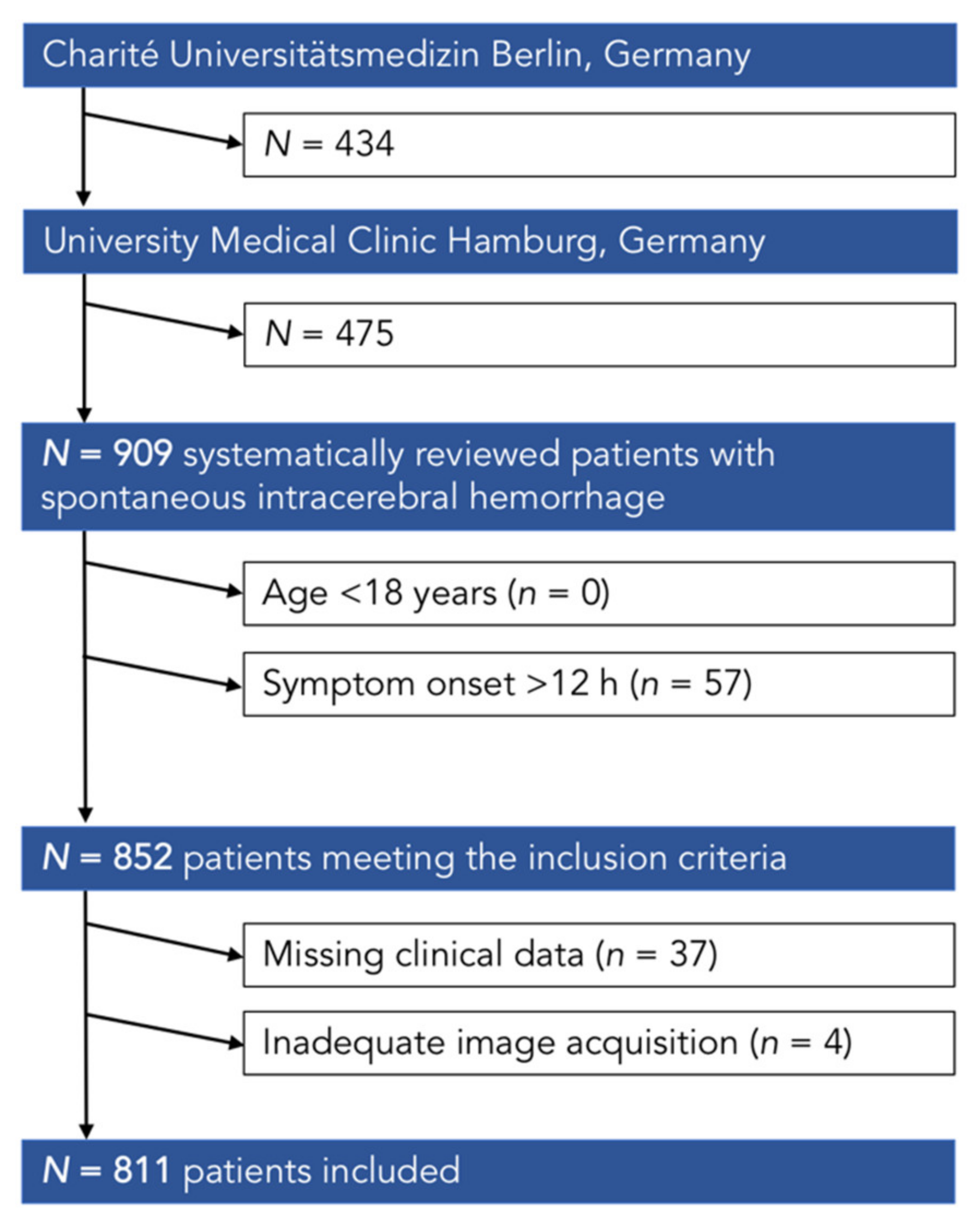
2.1. Study Population
2.2. Imaging
2.2.1. Image Acquisitions
2.2.2. Image Analysis
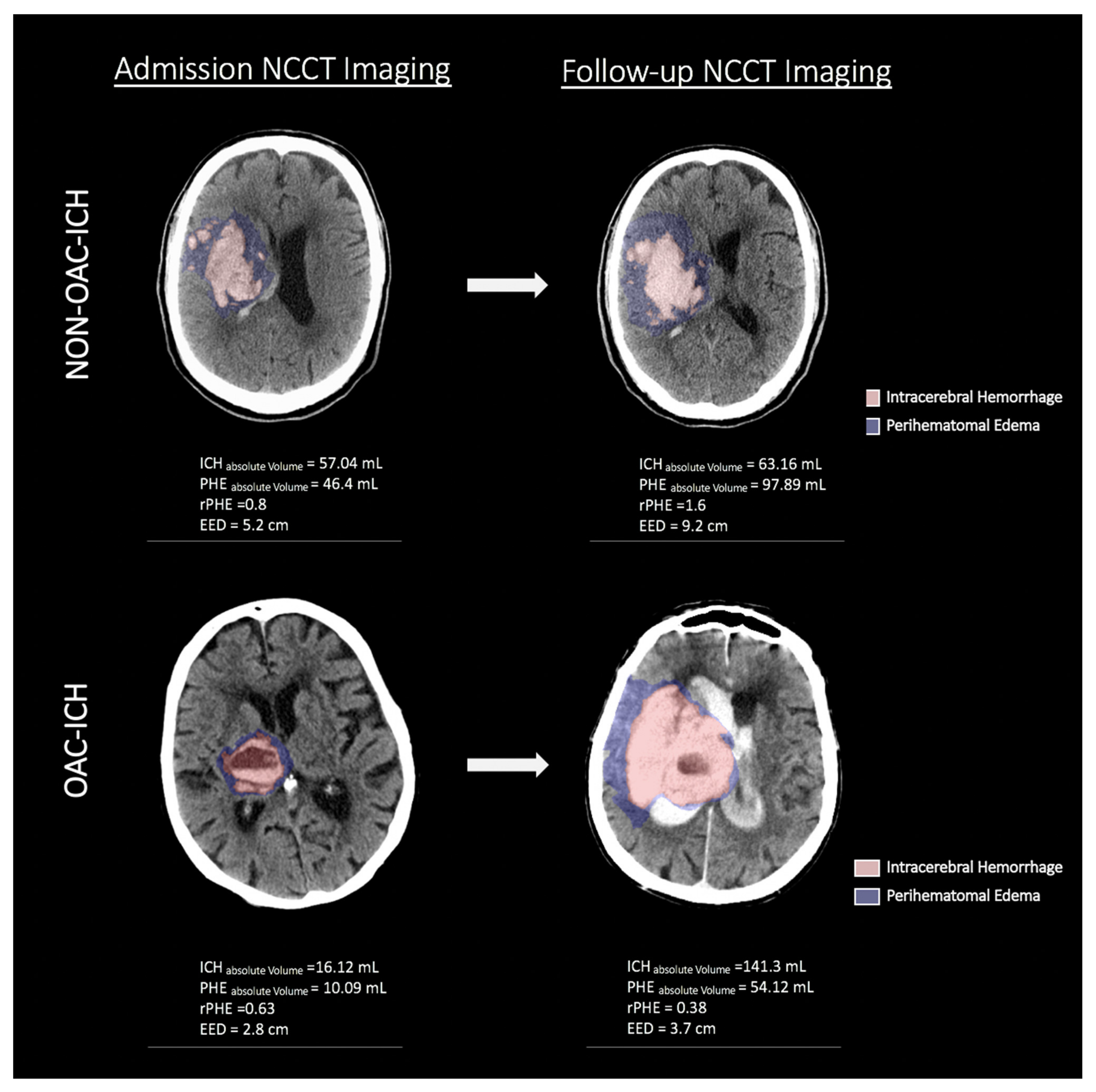
2.2.3. Perihematomal Edema Measurements
- Edema Extension Distance: Edema extension distance (EED) refers to the difference between the radius of a sphere equal to the absolute PHE volume and the radius of a sphere equal to the ICH volume alone. In brief, PHE volume corresponds to the absolute edema volume and π corresponds to the radius of a sphere equal to the combined volume of PHE and ICH and π the radius of a sphere equal to the volume of the ICH alone [18,22]. This can be calculated using the following formula:
2.3. Clinical Outcomes
2.4. Statistical Methods
2.4.1. Exploratory Analyses
2.4.2. Regression Analyses
3. Results
3.1. Clinical Parameters
3.2. Surgical Procedures and Clinical Outcome
3.3. Radiological Parameters
3.4. Exploratory Analyses
3.5. Perihematomal Edema Based Clinical Outcome Prediction
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Morotti, A.; Goldstein, J.N. Anticoagulant-associated intracerebral hemorrhage. Brain Hemorrhages 2020, 1, 89–94. [Google Scholar] [CrossRef]
- Kuramatsu, J.B.; Sembill, J.A.; Huttner, H.B. Reversal of oral anticoagulation in patients with acute intracerebral hemorrhage. Crit. Care 2019, 23, 206. [Google Scholar] [CrossRef]
- Cervera, A.; Amaro, S.; Chamorro, A. Oral anticoagulant-associated intracerebral hemorrhage. J. Neurol. 2012, 259, 212–224. [Google Scholar] [CrossRef]
- Feigin, V.L.; Lawes, C.M.; Bennett, D.A.; Anderson, C.S. Stroke epidemiology: A review of population-based studies of incidence, prevalence, and case-fatality in the late 20th century. Lancet Neurol. 2003, 2, 43–53. [Google Scholar] [CrossRef]
- Venkatasubramanian, C.; Mlynash, M.; Finley-Caulfield, A.; Eyngorn, I.; Kalimuthu, R.; Snider, R.W.; Wijman, C.A. Natural History of Perihematomal Edema After Intracerebral Hemorrhage Measured by Serial Magnetic Resonance Imaging. Stroke 2011, 42, 73–80. [Google Scholar] [CrossRef]
- Gebel, J.M.; Brott, T.G.; Sila, C.A.; Tomsick, T.A.; Jauch, E.; Salisbury, S.; Khoury, J.; Miller, R.; Pancioli, A.; Duldner, J.E.; et al. Decreased perihematomal edema in thrombolysis-related intracerebral hemorrhage compared with spontaneous intracerebral hemorrhage. Stroke 2000, 31, 596–600. [Google Scholar] [CrossRef] [PubMed]
- Analysis of Acute Perihematomal Edema in Warfarin-Related Intracerebral Hemorrhage. Available online: https://www.researchgate.net/publication/283075853_Analysis_of_Acute_Perihematomal_Edema_in_Warfarin-Related_Intracerebral_Hemorrhage (accessed on 2 October 2020).
- Molina, C.A.; Alvarez-Sabín, J.; Montaner, J.; Abilleira, S.; Arenillas, J.F.; Coscojuela, P.; Romero, F.; Codina, A. Thrombolysis-related hemorrhagic infarction: A marker of early reperfusion, reduced infarct size, and improved outcome in patients with proximal middle cerebral artery occlusion. Stroke 2002, 33, 1551–1556. [Google Scholar] [CrossRef]
- Ruff, C.T.; Giugliano, R.P.; Braunwald, E.; Hoffman, E.B.; Deenadayalu, N.; Ezekowitz, M.D.; Camm, A.J.; Weitz, J.I.; Lewis, B.S.; Parkhomenko, A.; et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: A meta-analysis of randomised trials. Lancet 2014, 383, 955–962. [Google Scholar] [CrossRef]
- Ironside, N.; Chen, C.-J.; Ding, D.; Mayer, S.A.; Connolly, E.S. Perihematomal Edema After Spontaneous Intracerebral Hemorrhage. Stroke 2019, 50, 1626–1633. [Google Scholar] [CrossRef]
- Murthy, S.B.; Moradiya, Y.; Dawson, J.; Lees, K.R.; Hanley, D.F.; Ziai, W.C.; VISTA-ICH Collaborators; Butcher, K.; Davis, S.; Gregson, B.; et al. Perihematomal Edema and Functional Outcomes in Intracerebral Hemorrhage. Stroke 2015, 46, 3088–3092. [Google Scholar] [CrossRef]
- Grunwald, Z.; Beslow, L.A.; Urday, S.; Vashkevich, A.; Ayres, A.; Greenberg, S.M.; Goldstein, J.N.; Leasure, A.; Shi, F.-D.; Kahle, K.T.; et al. Perihematomal Edema Expansion Rates and Patient Outcomes in Deep and Lobar Intracerebral Hemorrhage. Neurocritical. Care 2016, 26, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Arima, H.; Wang, J.G.; Huang, Y.; Heeley, E.; Skulina, C.; Parsons, M.W.; Peng, B.; Li, Q.; Su, S.; Tao, Q.L.; et al. Significance of perihematomal edema in acute intracerebral hemorrhage: The INTERACT trial. Neurology 2009, 73, 1963–1968. [Google Scholar] [CrossRef] [PubMed]
- Volbers, B.; Staykov, D.; Wagner, I.; Dörfler, A.; Saake, M.; Schwab, S.; Bardutzky, J. Semi-automatic volumetric assessment of perihemorrhagic edema with computed tomography. Eur. J. Neurol. 2011, 18, 1323–1328. [Google Scholar] [CrossRef]
- Urday, S.; Beslow, L.A.; Goldstein, D.W.; Vashkevich, A.; Ayres, A.M.; Battey, T.W.; Selim, M.H.; Kimberly, W.T.; Rosand, J.; Sheth, K.N. Measurement of Perihematomal Edema in Intracerebral Hemorrhage. Stroke 2015, 46, 1116–1119. [Google Scholar] [CrossRef] [PubMed]
- Yushkevich, P.A.; Piven, J.; Hazlett, H.C.; Smith, R.G.; Ho, S.; Gee, J.C.; Gerig, G. User-guided 3D active contour segmentation of anatomical structures: Significantly improved efficiency and reliability. Neuroimage 2006, 31, 1116–1128. [Google Scholar] [CrossRef]
- Mishra, M.; Shukla, P.; Bodhit, A.; Asaithambi, G.; Velez, A.; Rosado, C.; Mishra, M.; Saravanapavan, P.; Khan, S.; Reddy, V.; et al. Intracerebral Hematoma Volume Measurement Using ITK-SNAP Software: Initial Experience. Neurology 2014, 82, P7. 145. [Google Scholar]
- Selim, M.; Norton, C. Perihematomal edema: Implications for intracerebral hemorrhage research and therapeutic advances. J. Neurosci. Res. 2020, 98, 212–218. [Google Scholar] [CrossRef]
- Staykov, D.; Wagner, I.; Volbers, B.; Hauer, E.-M.; Doerfler, A.; Schwab, S.; Bardutzky, J. Natural Course of Perihemorrhagic Edema After Intracerebral Hemorrhage. Stroke 2011, 42, 2625–2629. [Google Scholar] [CrossRef]
- Gebel, J.M.; Jauch, E.C.; Brott, T.G.; Khoury, J.; Sauerbeck, L.; Salisbury, S.; Spilker, J.; Tomsick, T.A.; Duldner, J.; Broderick, J.P. Relative edema volume is a predictor of outcome in patients with hyperacute spontaneous intracerebral hemorrhage. Stroke 2002, 33, 2636–2641. [Google Scholar] [CrossRef]
- Yu, Z.; Ma, L.; Zheng, J.; You, C. Prognostic role of perihematomal edema in intracerebral hemorrhage: A systematic review. Turk. Neurosurg. 2017. [Google Scholar] [CrossRef]
- Parry-Jones, A.R.; Wang, X.; Sato, S.; Mould, W.A.; Vail, A.; Anderson, C.S.; Hanley, D.F. Edema Extension Distance. Stroke 2015, 46, e137–e140. [Google Scholar] [CrossRef]
- Broderick, J.P.; Adeoye, O.; Elm, J. Evolution of the Modified Rankin Scale and Its Use in Future Stroke Trials. Stroke 2017, 48, 2007–2012. [Google Scholar] [CrossRef]
- Leasure, A.C.; Sheth, K.N.; Comeau, M.; Aldridge, C.; Worrall, B.B.; Vashkevich, A.; Rosand, J.; Langefeld, C.; Moomaw, C.J.; Woo, D.; et al. Identification and Validation of Hematoma Volume Cutoffs in Spontaneous, Supratentorial Deep Intracerebral Hemorrhage. Stroke 2019, 50, 2044–2049. [Google Scholar] [CrossRef] [PubMed]
- Rangaraju, S.; Haussen, D.; Nogueira, R.G.; Nahab, F.; Frankel, M. Comparison of 3-Month Stroke Disability and Quality of Life across Modified Rankin Scale Categories. Interv. Neurol. 2017, 6, 36–41. [Google Scholar] [CrossRef]
- Chen, Q.; Nian, H.; Zhu, Y.; Talbot, H.K.; Griffin, M.R.; Harrell, F.E., Jr. Too many covariates and too few cases?—A comparative study. Stat. Med. 2016, 35, 4546–4558. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.R.; Colon, G.P.; Betz, A.L.; Keep, R.F.; Kim, S.; Hoff, J.T. Edema from intracerebral hemorrhage: The role of thrombin. J. Neurosurg. 1996, 84, 91–96. [Google Scholar] [CrossRef]
- Xi, G.; Wagner, K.R.; Keep, R.F.; Hua, Y.; De Courten-Myers, G.M.; Broderick, J.P.; Brott, T.G.; Hoff, J.T. Role of Blood Clot Formation on Early Edema Development After Experimental Intracerebral Hemorrhage. Stroke 1998, 29, 2580–2586. [Google Scholar] [CrossRef]
- Lee, K.R.; Betz, A.L.; Kim, S.; Keep, R.F.; Hoff, J.T. The role of the coagulation cascade in brain edema formation after intracerebral hemorrhage. Acta Neurochir. 1996, 138, 396–401. [Google Scholar] [CrossRef]
- Urday, S.; Beslow, L.A.; Dai, F.; Zhang, F.; Battey, T.W.K.; Vashkevich, A.; Ayres, A.M.; Leasure, A.C.; Selim, M.H.; Simard, J.M.; et al. Rate of Perihematomal Edema Expansion Predicts Outcome After Intracerebral Hemorrhage. Crit. Care Med. 2016, 44, 790–797. [Google Scholar] [CrossRef]
- Parry-Jones, A.R.; Wang, X.; Sato, S.; Mould, W.A.; Vail, A.; Anderson, C.S.; Hanley, D.F. Edema Extension Distance: Outcome Measure for Phase II Clinical Trials Targeting Edema After Intracerebral Hemorrhage. Stroke 2015, 46, e137–e140. [Google Scholar] [CrossRef]
- Marshall, A.L.; Connors, J.-M. Anticoagulation for Noncardiac Indications in Neurologic Patients: Comparative Use of Non-Vitamin K Oral Anticoagulants, Low-Molecular-Weight Heparins, and Warfarin. Curr. Treat. Options Neurol. 2014, 16, 1–15. [Google Scholar] [CrossRef]
- Boulouis, G.; Morotti, A.; Pasi, M.; Goldstein, J.N.; Gurol, M.E.; Charidimou, A. Outcome of intracerebral haemorrhage related to non-vitamin K antagonists oral anticoagulants versus vitamin K antagonists: A comprehensive systematic review and meta-analysis. J. Neurol. Neurosurg. Psychiatry 2018, 89, 263–270. [Google Scholar] [CrossRef]
- Steiner, T.; Köhrmann, M.; Schellinger, P.D.; Tsivgoulis, G. Non-vitamin K oral anticoagulants associated bleeding and its antidotes. J. Stroke 2018, 20, 292–301. [Google Scholar] [CrossRef]
- Lu, L.; Barfejani, A.H.; Qin, T.; Dong, Q.; Ayata, C.; Waeber, C. Fingolimod exerts neuroprotective effects in a mouse model of intracerebral hemorrhage. Brain Res. 2014, 1555, 89–96. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Fu, Y.; Hao, J.; Zhang, N.; Ren, L.; Sun, N.; Li, Y.J.; Yan, Y.; Huang, D.; Yu, C.; Shi, F.D. Fingolimod for the treatment of intracerebral hemorrhage: A 2-arm proof-of-concept study. JAMA Neurol. 2014, 71, 1092–1101. [Google Scholar] [CrossRef]
- Lee, I.-N.; Cheng, W.-C.; Chung, C.-Y.; Lee, M.-H.; Lin, M.H.-C.; Kuo, C.-H.; Weng, H.-H.; Yang, J.-T. Dexamethasone reduces brain cell apoptosis and inhibits inflammatory response in rats with intracerebral hemorrhage. J. Neurosci. Res. 2014, 93, 178–188. [Google Scholar] [CrossRef]
- Misra, U.; Kalita, J.; Ranjan, P.; Mandal, S. Mannitol in intracerebral hemorrhage: A randomized controlled study. J. Neurol. Sci. 2005, 234, 41–45. [Google Scholar] [CrossRef]
- Selim, M.; Hanley, D.; Steiner, T.; Christensen, H.K.; Lafuente, J.; Rodriguez, D.; Keep, R.; Anderson, C.; Parry-Jones, A. Recommendations for Clinical Trials in ICH. Recommendations for Clinical Trials in ICH. Stroke 2020, 51, 1333–1338. [Google Scholar] [CrossRef]
- Cox, M.; Bisangwa, S.; Herpich, F.; Crudele, A.; Pineda, C. Fluid levels in the bleeding brain: A marker for coagulopathy and hematoma expansion Intern. Emerg. Med. 2017, 12, 1071–1073. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Siegal, D.M.; Crowther, M.A. Acute management of bleeding in patients on novel oral anticoagulants. Eur. Heart J. 2013, 34, 489–498. [Google Scholar] [CrossRef]
- Adam, S.S.; McDuffie, J.R.; Ortel, T.L.; Williams, J.W. Comparative effectiveness of warfarin and new oral anticoagulants for the management of atrial fibrillation and venous thromboembolism: A systematic review. Ann. Intern. Med. 2012, 157, 796–807. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.S.; Grandi, S.M.; Shimony, A.; Filion, K.B.; Eisenberg, M.J. Meta-Analysis of Efficacy and Safety of New Oral Anticoagulants (Dabigatran, Rivaroxaban, Apixaban) Versus Warfarin in Patients with Atrial Fibrillation. Am. J. Cardiol. 2012, 110, 453–460. [Google Scholar] [CrossRef] [PubMed]
- Morotti, A.; Goldstein, J.N. New Oral Anticoagulants and Their Reversal Agents. Curr. Treat. Options Neurol. 2016, 18, 47. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Baseline Characteristics | All (n = 811) | NON-OAC-ICH (n = 599) | OAC-ICH (n = 212) | p-value |
|---|---|---|---|---|
| Clinical parameters | ||||
| Age (years), median (IQR) | 73 (60-79) | 70 (58-77) | 77 (70-82) | <0.001 |
| Female, n (%) | 348 (42.91) | 254 (42.24) | 94 (44.34) | 0.61 |
| Comorbidities | ||||
| • Hypertension, n (%) | 624 (76.94) | 447 (74.62) | 177 (83.49) | 0.008 |
| • Diabetes mellitus, n (%) | 120 (14.8) | 80 (13.36) | 40 (18.87) | 0.048 |
| Anticoagulation Treatment, n (%) | 212 (26.14) | - | 212 (100) | - |
| Antiplatelet Treatment, n (%) | 190 (23.43) | 160 (26.7) | 30 (14.15) | <0.001 |
| Time difference between symptom onset to imaging (hours), median (IQR) | 2.81 (1.39–11.96) | 2.81(1.28–12.57) | 2.74 (1.56–11.65) | 0.592 |
| GCS admission, median (IQR) | 12 (6–15) | 12 (5–14) | 11 (4–14) | 0.315 |
| NIHSS admission, median (IQR) | 1 (8–14) | 8 (1–15) | 6 (1–14) | 0.44 |
| Radiological parameters | ||||
| ICH Volume (mL), mean (SD) | 47 (54.11) | 46.39 (53.85) | 48.41 (54.84) | 0.767 |
| PHE Volume (mL), mean (SD) | 36.42 (37.89) | 37.61 (38.27) | 33.06 (36.69) | 0.091 |
| rPHE, mean (SD) | 1.2 (2.4) | 1.25 (2.5) | 1.08 (2.09) | 0.001 |
| EED, (cm), mean (SD) | 4.57 (2.5) | 4.72 (2.58) | 4.14 (2.22) | 0.007 |
| Intraventricular hemorrhage, n (%) | 374 (46.12) | 279 (46.58) | 95 (44.81) | 0.799 |
| ICH location, n (%) | ||||
| • lobar | 362 (44.63) | 261 (43.6) | 101 (47.6) | 0.317 |
| • basal ganglia | 306 (37.73) | 238 (39.7) | 68 (32.1) | 0.05 |
| • thalamic | 16 (19.73) | 11 (1.8) | 5 (2.4) | 0.636 |
| • brainstem | 37 (45.62) | 27 (4.5) | 10 (4.7) | 0.896 |
| • cerebellar | 88 (10.85) | 61 (10.2) | 27 (12.7) | 0.301 |
| Procedure process | ||||
| Supratentorial craniectomy, n (%) | 116 (14.3) | 91 (15.19) | 25 (11.79) | 0.358 |
| Suboccipital craniectomy, n (%) | 33 (4.07) | 20 (3.33) | 13 (6.13) | 0.85 |
| EVD, n (%) | 65 (8.01) | 49 (8.2) | 16 (7.55) | 0.785 |
| Clinical outcome | ||||
| mRS 90, n (%) | ||||
| • 0–3 | 225 (27.74) | 164 (27.38) | 61 (28.77) | 0.24 |
| • 4–6 | 586 (72.26) | 435 (72.62) | 151 (71.23) | 0.7 |
| • 6 (death) | 205 (25.27) | 147 (24.54) | 58 (27.35) | 0.068 |
| Radiological Parameters | NON-OAC-ICH (n = 599) | NOAC-ICH (n = 93) | VKA-ICH (n = 81) | p-value |
|---|---|---|---|---|
| ICH Volume (mL), mean (SD) | 46.39 (53.84) | 51.85 (66.43) | 47.41 (43.7) | 0.667 |
| PHE Volume (mL), mean (SD) | 37.61 (38.27) | 32.94 (37.0) | 36.21 (40.79) | 0.544 |
| rPHE, mean (SD) | 1.2 (2.25) | 1.11 (2.09) | 0.88 (0.59) | 0.399 |
| EED, (cm), mean (SD) | 4.72 (2.58) | 4.07 (2.17) | 4.34 (2.35) | 0.042 |
| Predictor | Poor Outcome (mRS 4–6) in OAC-ICH | |||
|---|---|---|---|---|
| OR | 95% CI | Regression- Coefficient | p-value | |
| Age (years) | - | - | - | 0.953 |
| Gender (ref: female) | - | - | - | 0.568 |
| GCS on admission | 0.758 | 0.629–0.912 | −0.277 | 0.003 |
| NIHSS on admission | 1.123 | 1.028–1.227 | 0.116 | 0.10 |
| PHE Volume (mL) | - | - | - | 0.451 |
| IVH (ref: yes) | - | - | - | 0.213 |
| Craniectomy (ref: supratentorial) | - | - | - | 0.998 |
| Predictor | Poor Outcome (mRS 4–6) in NON-OAC-ICH | |||
|---|---|---|---|---|
| OR | 95% CI | Regression- Coefficient | p-value | |
| Age (years) | - | - | - | 0.248 |
| Gender (ref: female) | 0.520 | 0.283–0.955 | −0.654 | 0.035 |
| GCS on admission | 0.758 | 0.676–0.849 | −0.277 | <0.0001 |
| NIHSS on admission | 1.142 | 1.083–1.204 | 0.132 | <0.0001 |
| PHE Volume (mL) | 1.015 | 1.002–1.028 | 0.014 | 0.027 |
| EED (cm) | - | - | - | 0.843 |
| IVH (ref: yes) | 2.803 | 1.441–5.451 | 1.031 | 0.002 |
| Location (ref: supratentorial) | 0.381 | 0.201–0.723 | −0.966 | 0.003 |
| Craniectomy (ref: supratentorial) | - | - | - | 0.113 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nawabi, J.; Elsayed, S.; Morotti, A.; Speth, A.; Liu, M.; Kniep, H.; McDonough, R.; Broocks, G.; Faizy, T.; Can, E.; et al. Perihematomal Edema and Clinical Outcome in Intracerebral Hemorrhage Related to Different Oral Anticoagulants. J. Clin. Med. 2021, 10, 2234. https://doi.org/10.3390/jcm10112234
Nawabi J, Elsayed S, Morotti A, Speth A, Liu M, Kniep H, McDonough R, Broocks G, Faizy T, Can E, et al. Perihematomal Edema and Clinical Outcome in Intracerebral Hemorrhage Related to Different Oral Anticoagulants. Journal of Clinical Medicine. 2021; 10(11):2234. https://doi.org/10.3390/jcm10112234
Chicago/Turabian StyleNawabi, Jawed, Sarah Elsayed, Andrea Morotti, Anna Speth, Melanie Liu, Helge Kniep, Rosalie McDonough, Gabriel Broocks, Tobias Faizy, Elif Can, and et al. 2021. "Perihematomal Edema and Clinical Outcome in Intracerebral Hemorrhage Related to Different Oral Anticoagulants" Journal of Clinical Medicine 10, no. 11: 2234. https://doi.org/10.3390/jcm10112234
APA StyleNawabi, J., Elsayed, S., Morotti, A., Speth, A., Liu, M., Kniep, H., McDonough, R., Broocks, G., Faizy, T., Can, E., Sporns, P. B., Fiehler, J., Hamm, B., Penzkofer, T., Bohner, G., Schlunk, F., & Hanning, U. (2021). Perihematomal Edema and Clinical Outcome in Intracerebral Hemorrhage Related to Different Oral Anticoagulants. Journal of Clinical Medicine, 10(11), 2234. https://doi.org/10.3390/jcm10112234