
Urine and Serum Electrolytes and Biochemical Values Associated with Osteoporosis in Premenopausal and Postmenopausal Women: A Longitudinal and Cross-Sectional Study Using Korean Genome and Epidemiology Study (KoGES) Cohort

Abstract
:1. Introduction
2. Materials and Methods
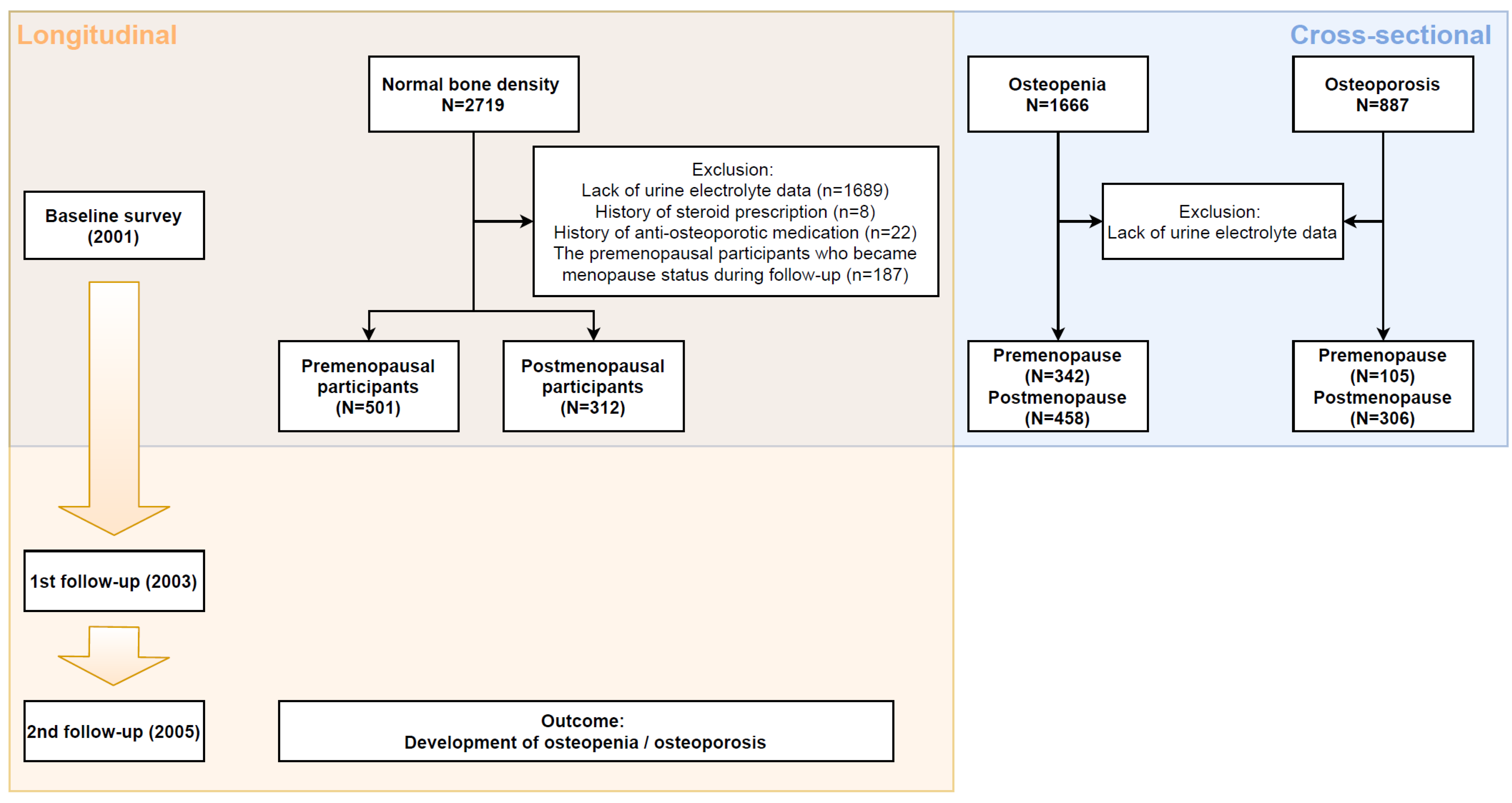
2.1. Study Setting and Study Cohort
2.2. Study Groups
2.2.1. Longitudinal Observational Study
2.2.2. Cross-Sectional Study
2.3. Study Outcome
2.4. Data Collection
2.5. Statistical Analyses
3. Results
3.1. Baseline Characteristics of Longitudinal Cohort
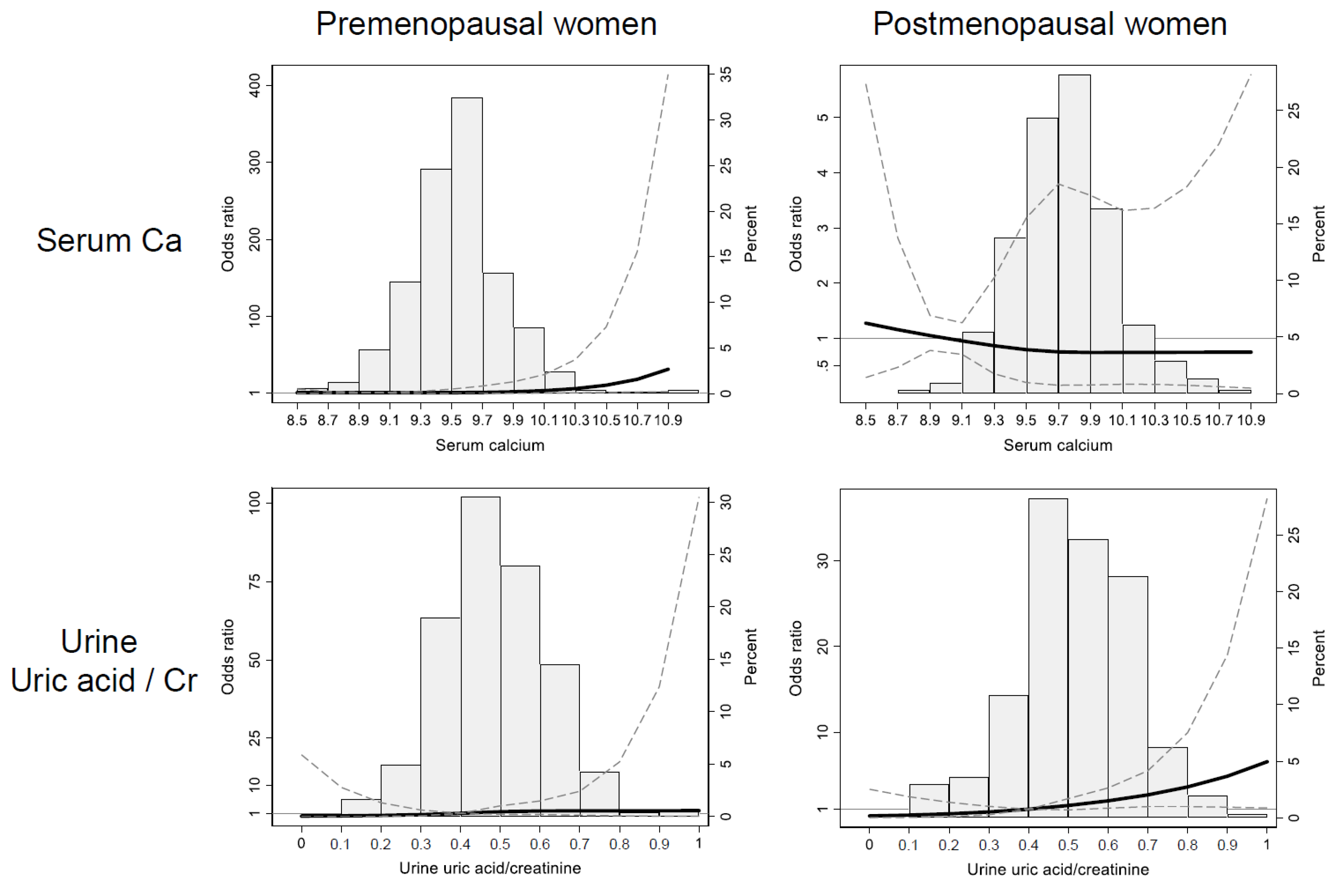
3.2. Risk Factors for Osteopenia and Osteoporosis in Pre- and Postmenopausal Participants in the Longitudinal Analysis
3.3. Difference of Serum Calcium, and Urine Uric Acid Levels between Bone Density Groups in Cross-Sectional Cohort
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Sozen, T.; Ozisik, L.; Basaran, N.C. An overview and management of osteoporosis. Eur. J. Rheumatol. 2017, 4, 46–56. [Google Scholar] [CrossRef] [PubMed]
- Ensrud, K.E.; Ewing, S.K.; Taylor, B.C.; Fink, H.A.; Stone, K.L.; Cauley, J.A.; Tracy, J.K.; Hochberg, M.C.; Rodondi, N.; Cawthon, P.M.; et al. Frailty and risk of falls, fracture, and mortality in older women: The study of osteoporotic fractures. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 744–751. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kanis, J.A.; on behalf of the World Health Organization Scientific Group. WHO Scientific Group on the Assessment of Osteoporosis at the Primary Health Care Level: Summary Meeting Report; World Health Organization Collaborating Centre for Metabolic Bone Diseases, University of Sheffield: Sheffield, UK, 2007. [Google Scholar]
- Force, U.S.P.S.T. Screening for osteoporosis: U.S. preventive services task force recommendation statement. Ann. Intern. Med. 2011, 154, 356–364. [Google Scholar]
- Ji, M.X.; Yu, Q. Primary osteoporosis in postmenopausal women. Chronic Dis. Transl. Med. 2015, 1, 9–13. [Google Scholar]
- Lerner, U.H. Bone remodeling in post-menopausal osteoporosis. J. Dent. Res. 2006, 85, 584–595. [Google Scholar] [CrossRef]
- Cawthon, P.M. Gender differences in osteoporosis and fractures. Clin. Orthop. Relat. Res. 2011, 469, 1900–1905. [Google Scholar] [CrossRef] [Green Version]
- Dornemann, T.M.; McMurray, R.G.; Renner, J.B.; Anderson, J.J. Effects of high-intensity resistance exercise on bone mineral density and muscle strength of 40-50-year-old women. J. Sports Med. Phys. Fit. 1997, 37, 246–251. [Google Scholar]
- Shapses, S.A.; Von Thun, N.L.; Heymsfield, S.B.; Ricci, T.A.; Ospina, M.; Pierson, R.N., Jr.; Stahl, T. Bone turnover and density in obese premenopausal women during moderate weight loss and calcium supplementation. J. Bone Miner. Res. 2001, 16, 1329–1336. [Google Scholar] [CrossRef]
- Teegarden, D.; Lyle, R.M.; McCabe, G.P.; McCabe, L.D.; Proulx, W.R.; Michon, K.; Knight, A.P.; Johnston, C.C.; Weaver, C.M. Dietary calcium, protein, and phosphorus are related to bone mineral density and content in young women. Am. J. Clin. Nutr. 1998, 68, 749–754. [Google Scholar] [CrossRef] [Green Version]
- Holm, J.P.; Amar, A.O.S.; Hyldstrup, L.; Jensen, J.E.B. Hyponatremia, a risk factor for osteoporosis and fractures in women. Osteoporos. Int. 2016, 27, 989–1001. [Google Scholar] [CrossRef] [PubMed]
- Yakout, S.M.; Alharbi, F.; Abdi, S.; Al-Daghri, N.M.; Al-Amro, A.; Khattak, M.N.K. Serum minerals (Ca, P, Co, Mn, Ni, Cd) and growth hormone (IGF-1 and IGF-2) levels in postmenopausal Saudi women with osteoporosis. Medicine 2020, 99, e20840. [Google Scholar] [CrossRef]
- Guiducci, L.; Maffei, S.; Sabatino, L.; Zyw, L.; Battaglia, D.; Vannucci, A.; Di Cecco, P.; Vassalle, C. Significance of the ionized calcium measurement to assess calcium status in osteopenic/osteoporosis postmenopausal outpatients. Gynecol. Endocrinol. 2017, 33, 383–388. [Google Scholar] [CrossRef]
- Kim, Y.; Han, B.G.; Ko, G.E.S.g. Cohort Profile: The Korean Genome and Epidemiology Study (KoGES) Consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef]
- Lewiecki, E.M.; Gordon, C.M.; Baim, S.; Leonard, M.B.; Bishop, N.J.; Bianchi, M.L.; Kalkwarf, H.J.; Langman, C.B.; Plotkin, H.; Rauch, F.; et al. International Society for Clinical Densitometry 2007 Adult and Pediatric Official Positions. Bone 2008, 43, 1115–1121. [Google Scholar] [CrossRef]
- Ferrari, S.; Bianchi, M.L.; Eisman, J.A.; Foldes, A.J.; Adami, S.; Wahl, D.A.; Stepan, J.J.; de Vernejoul, M.C.; Kaufman, J.M.; For the IOF Committee of Scientific Advisors Working Group on Osteoporosis Pathophysiology. Osteoporosis in young adults: Pathophysiology, diagnosis, and management. Osteoporos. Int. 2012, 23, 2735–2748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Damilakis, J.; Papadokostakis, G.; Vrahoriti, H.; Tsagaraki, I.; Perisinakis, K.; Hadjipavlou, A.; Gourtsoyiannis, N. Ultrasound velocity through the cortex of phalanges, radius, and tibia in normal and osteoporotic postmenopausal women using a new multisite quantitative ultrasound device. Investig. Radiol. 2003, 38, 207–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chong, K.H.; Poh, B.K.; Jamil, N.A.; Kamaruddin, N.A.; Deurenberg, P. Radial quantitative ultrasound and dual energy x-ray absorptiometry: Intermethod agreement for bone status assessment in children. BioMed Res. Int. 2015, 2015, 232876. [Google Scholar] [PubMed]
- Orsini, N.; Greenland, S. A Procedure to Tabulate and Plot Results after Flexible Modeling of a Quantitative Covariate. Stata J. 2011, 11, 1–29. [Google Scholar] [CrossRef] [Green Version]
- Marrie, R.A.; Dawson, N.V.; Garland, A. Quantile regression and restricted cubic splines are useful for exploring relationships between continuous variables. J. Clin. Epidemiol. 2009, 62, 511–517.e1. [Google Scholar] [CrossRef]
- Reinsch, C.H. Smoothing by spline functions. Numer. Math. 1967, 10, 177–183. [Google Scholar] [CrossRef]
- Tarantino, U.; Iolascon, G.; Cianferotti, L.; Masi, L.; Marcucci, G.; Giusti, F.; Marini, F.; Parri, S.; Feola, M.; Rao, C.; et al. Clinical guidelines for the prevention and treatment of osteoporosis: Summary statements and recommendations from the Italian Society for Orthopaedics and Traumatology. J. Orthop. Traumatol. 2017, 18, 3–36. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cerani, A.; Zhou, S.; Forgetta, V.; Morris, J.A.; Trajanoska, K.; Rivadeneira, F.; Larsson, S.C.; Michaelsson, K.; Richards, J.B. Genetic predisposition to increased serum calcium, bone mineral density, and fracture risk in individuals with normal calcium levels: Mendelian randomisation study. BMJ 2019, 366, l4410. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nordin, B.E.; Horowitz, M.; Need, A.; Morris, H.A. Renal leak of calcium in post-menopausal osteoporosis. Clin. Endocrinol. 1994, 41, 41–45. [Google Scholar] [CrossRef]
- Cheng, L.; Zhang, K.; Zhang, Z. Effectiveness of thiazides on serum and urinary calcium levels and bone mineral density in patients with osteoporosis: A systematic review and meta-analysis. Drug Des. Dev. Ther. 2018, 12, 3929–3935. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalemo, S.; Eggertsen, R.; Hjerpe, P.; Almqvist, E.G.; Bostrom, K.B. Bone mineral density in primary care patients related to serum calcium concentrations: A longitudinal cohort study from Sweden. Scand. J. Prim. Health Care 2018, 36, 198–206. [Google Scholar] [CrossRef] [Green Version]
- Liu, M.; Yao, X.; Zhu, Z. Associations between serum calcium, 25(OH)D level and bone mineral density in older adults. J. Orthop. Surg. Res. 2019, 14, 458. [Google Scholar] [CrossRef]
- Lufkin, E.G.; Wahner, H.W.; O’Fallon, W.M.; Hodgson, S.F.; Kotowicz, M.A.; Lane, A.W.; Judd, H.L.; Caplan, R.H.; Riggs, B.L. Treatment of postmenopausal osteoporosis with transdermal estrogen. Ann. Intern. Med. 1992, 117, 1–9. [Google Scholar] [CrossRef]
- Charatcharoenwitthaya, N.; Khosla, S.; Atkinson, E.J.; McCready, L.K.; Riggs, B.L. Effect of blockade of TNF-alpha and interleukin-1 action on bone resorption in early postmenopausal women. J. Bone Miner. Res. 2007, 22, 724–729. [Google Scholar] [CrossRef]
- Nabipour, I.; Sambrook, P.N.; Blyth, F.M.; Janu, M.R.; Waite, L.M.; Naganathan, V.; Handelsman, D.J.; Le Couteur, D.G.; Cumming, R.G.; Seibel, M.J. Serum uric acid is associated with bone health in older men: A cross-sectional population-based study. J. Bone Miner. Res. 2011, 26, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Sautin, Y.Y.; Johnson, R.J. Uric acid: The oxidant-antioxidant paradox. Nucleosides Nucleotides Nucleic Acids 2008, 27, 608–619. [Google Scholar] [CrossRef] [Green Version]
- Santos, C.X.; Anjos, E.I.; Augusto, O. Uric acid oxidation by peroxynitrite: Multiple reactions, free radical formation, and amplification of lipid oxidation. Arch. Biochem. Biophys. 1999, 372, 285–294. [Google Scholar] [CrossRef]
- Lin, K.M.; Lu, C.L.; Hung, K.C.; Wu, P.C.; Pan, C.F.; Wu, C.J.; Syu, R.S.; Chen, J.S.; Hsiao, P.J.; Lu, K.C. The Paradoxical Role of Uric Acid in Osteoporosis. Nutrients 2019, 11, 2111. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Makovey, J.; Macara, M.; Chen, J.S.; Hayward, C.S.; March, L.; Seibel, M.J.; Sambrook, P.N. Serum uric acid plays a protective role for bone loss in peri- and postmenopausal women: A longitudinal study. Bone 2013, 52, 400–406. [Google Scholar] [CrossRef]
- Ahn, S.H.; Lee, S.H.; Kim, B.J.; Lim, K.H.; Bae, S.J.; Kim, E.H.; Kim, H.K.; Choe, J.W.; Koh, J.M.; Kim, G.S. Higher serum uric acid is associated with higher bone mass, lower bone turnover, and lower prevalence of vertebral fracture in healthy postmenopausal women. Osteoporos. Int. 2013, 24, 2961–2970. [Google Scholar] [CrossRef]
- Rull, M.A.; Cano-Garcia Mdel, C.; Arrabal-Martin, M.; Arrabal-Polo, M.A. The importance of urinary calcium in postmenopausal women with osteoporotic fracture. Can. Urol. Assoc. J. 2015, 9, E183–E186. [Google Scholar] [CrossRef] [PubMed]
- Orriss, I.R.; Arnett, T.R.; George, J.; Witham, M.D. Allopurinol and oxypurinol promote osteoblast differentiation and increase bone formation. Exp. Cell Res. 2016, 342, 166–174. [Google Scholar] [CrossRef] [Green Version]
- Lu, C.L.; Shyu, J.F.; Wu, C.C.; Hung, C.F.; Liao, M.T.; Liu, W.C.; Zheng, C.M.; Hou, Y.C.; Lin, Y.F.; Lu, K.C. Association of Anabolic Effect of Calcitriol with Osteoclast-Derived Wnt 10b Secretion. Nutrients 2018, 10, 1164. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laspa, E.; Bastepe, M.; Juppner, H.; Tsatsoulis, A. Phenotypic and molecular genetic aspects of pseudohypoparathyroidism type Ib in a Greek kindred: Evidence for enhanced uric acid excretion due to parathyroid hormone resistance. J. Clin. Endocrinol. Metab. 2004, 89, 5942–5947. [Google Scholar] [CrossRef]
- Thakkinstian, A.; Anothaisintawee, T.; Chailurkit, L.; Ratanachaiwong, W.; Yamwong, S.; Sritara, P.; Ongphiphadhanakul, B. Potential causal associations between vitamin D and uric acid: Bidirectional mediation analysis. Sci. Rep. 2015, 5, 14528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Isnuwardana, R.; Bijukchhe, S.; Thadanipon, K.; Ingsathit, A.; Thakkinstian, A. Association Between Vitamin D and Uric Acid in Adults: A Systematic Review and Meta-Analysis. Horm. Metab. Res. 2020, 52, 732–741. [Google Scholar] [CrossRef]
- Manolagas, S.C. Steroids and osteoporosis: The quest for mechanisms. J. Clin. Investig. 2013, 123, 1919–1921. [Google Scholar] [CrossRef] [PubMed] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | Premenopausal Women | Postmenopausal Women | |
|---|---|---|---|
| n = 501 | n = 312 | p-Value | |
| Age, years | 43 (41–45) | 55 (52–61) | <0.001 |
| Body mass index, kg/m2 | 23.9 (22.2–26.0) | 24.4 (22.6–26.7) | 0.034 |
| Waist-hip ratio, cm/cm | 0.83 (0.78–0.89) | 0.89 (0.83–0.94) | <0.001 |
| Hypertension, n (%) | 30 (6.0%) | 59 (18.9%) | <0.001 |
| Diabetes mellitus, n (%) | 17 (3.4%) | 23 (7.4%) | 0.011 |
| Myocardial infarction, n (%) | 3 (0.6%) | 5 (1.6%) | 0.159 |
| Alcohol habit, n (%) | 0.016 | ||
| Never drinker | 331 (66.1%) | 237 (76.0%) | |
| Ex-drinker | 12 (2.4%) | 7 (2.2%) | |
| Current drinker | 148 (29.5%) | 65 (20.8%) | |
| Smoking habit, n (%) | 0.346 | ||
| Never smoker | 468 (93.4%) | 296 (94.9%) | |
| Ex-smoker | 3 (0.6%) | 1 (0.3%) | |
| Current smoker | 12 (2.4%) | 13 (4.2%) | |
| Serum albumin, g/dL | 4.1 (3.9–4.1) | 4.1(3.9–4.1) | 0.506 |
| Serum blood urea nitrogen, mg/dL | 12.3 (10.3–14.6) | 13.7 (11.6–16.1) | <0.001 |
| Estimated GFR, mL/min/1.73m2 | 104.2 (98.5–105.7) | 93.8 (83.3–97.9) | <0.001 |
| Bone density at baseline | |||
| distal radius T-score | 1.2 (0.4–2.1) | 0.5 (−0.1 to 1.25) | <0.001 |
| distal radius Z-score | 1.3 (0.5–2.1) | 1.7 (1.0–2.6) | <0.001 |
| midshaft tibia T-score | 0.1 (−0.3–1.1) | 0 (−0.6–0.6) | <0.001 |
| midshaft tibia Z-score | 0.3 (−0.2–1.2) | 1.0 (0.4–1.7) | <0.001 |
| Serum and Urine electrolytes | |||
| Serum calcium (albumin corrected), mg/dL | 9.5 (9.3–9.7) | 9.7 (9.5–9.9) | <0.001 |
| Serum sodium, mmol/L | 142 (140–143) | 143 (141–144) | <0.001 |
| Urine calcium/creatinine, mg/mg | 0.12 (0.08–0.17) | 0.14 (0.09–0.20) | <0.001 |
| Urine sodium/creatinine, mmol/mg | 1.51 (1.08–2.16) | 1.93 (1.30–2.60) | <0.001 |
| Urine uric acid/creatinine, mg/mg | 0.48 (0.40–0.58) | 0.52 (0.43–0.62) | <0.001 |
| Urine protein/creatinine, mg/mg | 0.06 (0.04–0.11) | 0.08 (0.05–0.14) | <0.001 |
| Variables | Osteopenia (Compared to Normal Bone Density) | Osteoporosis (Compared to Normal Bone Density) | ||
|---|---|---|---|---|
| RRR (95% CI) | p-Value | RRR (95% CI) | p-Value | |
| In premenopausal women * | ||||
| Age, years | 1.13 (1.06–1.21) | <0.001 | 1.15 (1.04–1.28) | 0.001 |
| Baseline T-score | 0.38 (0.27–0.53) | <0.001 | 0.12 (0.03–0.44) | 0.009 |
| Serum calcium, mg/dL | 0.90 (0.46–1.75) | 0.752 | 4.03 (1.09–14.93) | 0.037 |
| In postmenopausal women ** | ||||
| Age, years | 1.03 (0.99–1.08) | 0.169 | 1.07 (1.00–1.14) | 0.043 |
| Baseline T-score | 0.33 (0.21–0.52) | <0.001 | 0.19 (0.09–0.40) | <0.001 |
| Hypertension | 2.30 (1.02–5.19) | 0.044 | 3.83 (1.43–10.25) | 0.008 |
| Urine uric acid/creatinine, mg/mg | 2.47 (0.38–16.20) | 0.345 | 24.08 (1.79–323.69) | 0.016 |
| Serum calcium, mg/dL | 3.33 (1.34–8.32) | 0.01 | 1.77 (0.48–6.59) | 0.395 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, H.-S.; Kim, G.-Y.; Lo, J.-A.; Kim, J.-S.; Ahn, S.-Y.; Ko, G.-J.; Kwon, Y.-J.; Kim, J.-E. Urine and Serum Electrolytes and Biochemical Values Associated with Osteoporosis in Premenopausal and Postmenopausal Women: A Longitudinal and Cross-Sectional Study Using Korean Genome and Epidemiology Study (KoGES) Cohort. J. Clin. Med. 2021, 10, 2155. https://doi.org/10.3390/jcm10102155
Park H-S, Kim G-Y, Lo J-A, Kim J-S, Ahn S-Y, Ko G-J, Kwon Y-J, Kim J-E. Urine and Serum Electrolytes and Biochemical Values Associated with Osteoporosis in Premenopausal and Postmenopausal Women: A Longitudinal and Cross-Sectional Study Using Korean Genome and Epidemiology Study (KoGES) Cohort. Journal of Clinical Medicine. 2021; 10(10):2155. https://doi.org/10.3390/jcm10102155
Chicago/Turabian StylePark, Hae-Sang, Ga-Young Kim, Jong-Ah Lo, Jin-Sun Kim, Shin-Young Ahn, Gang-Jee Ko, Young-Joo Kwon, and Ji-Eun Kim. 2021. "Urine and Serum Electrolytes and Biochemical Values Associated with Osteoporosis in Premenopausal and Postmenopausal Women: A Longitudinal and Cross-Sectional Study Using Korean Genome and Epidemiology Study (KoGES) Cohort" Journal of Clinical Medicine 10, no. 10: 2155. https://doi.org/10.3390/jcm10102155
APA StylePark, H.-S., Kim, G.-Y., Lo, J.-A., Kim, J.-S., Ahn, S.-Y., Ko, G.-J., Kwon, Y.-J., & Kim, J.-E. (2021). Urine and Serum Electrolytes and Biochemical Values Associated with Osteoporosis in Premenopausal and Postmenopausal Women: A Longitudinal and Cross-Sectional Study Using Korean Genome and Epidemiology Study (KoGES) Cohort. Journal of Clinical Medicine, 10(10), 2155. https://doi.org/10.3390/jcm10102155