
An Inverse Relation between Hyperglycemia and Skeletal Muscle Mass Predicted by Using a Machine Learning Approach in Middle-Aged and Older Adults in Large Cohorts



Abstract
1. Introduction
2. Methods
2.1. Participants
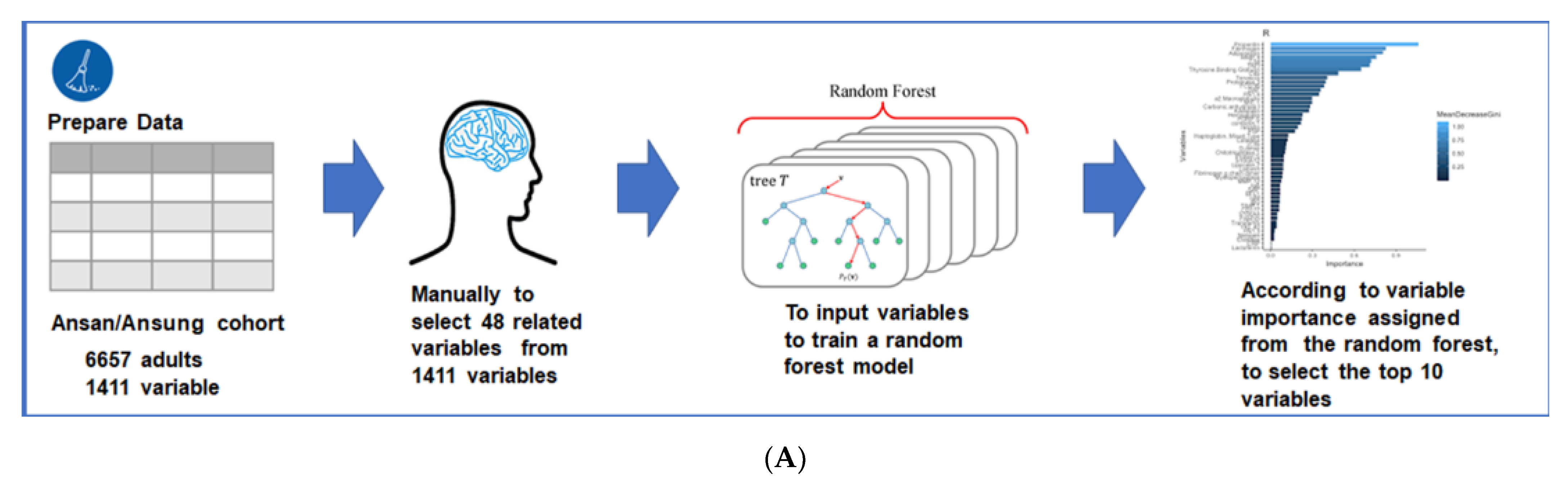
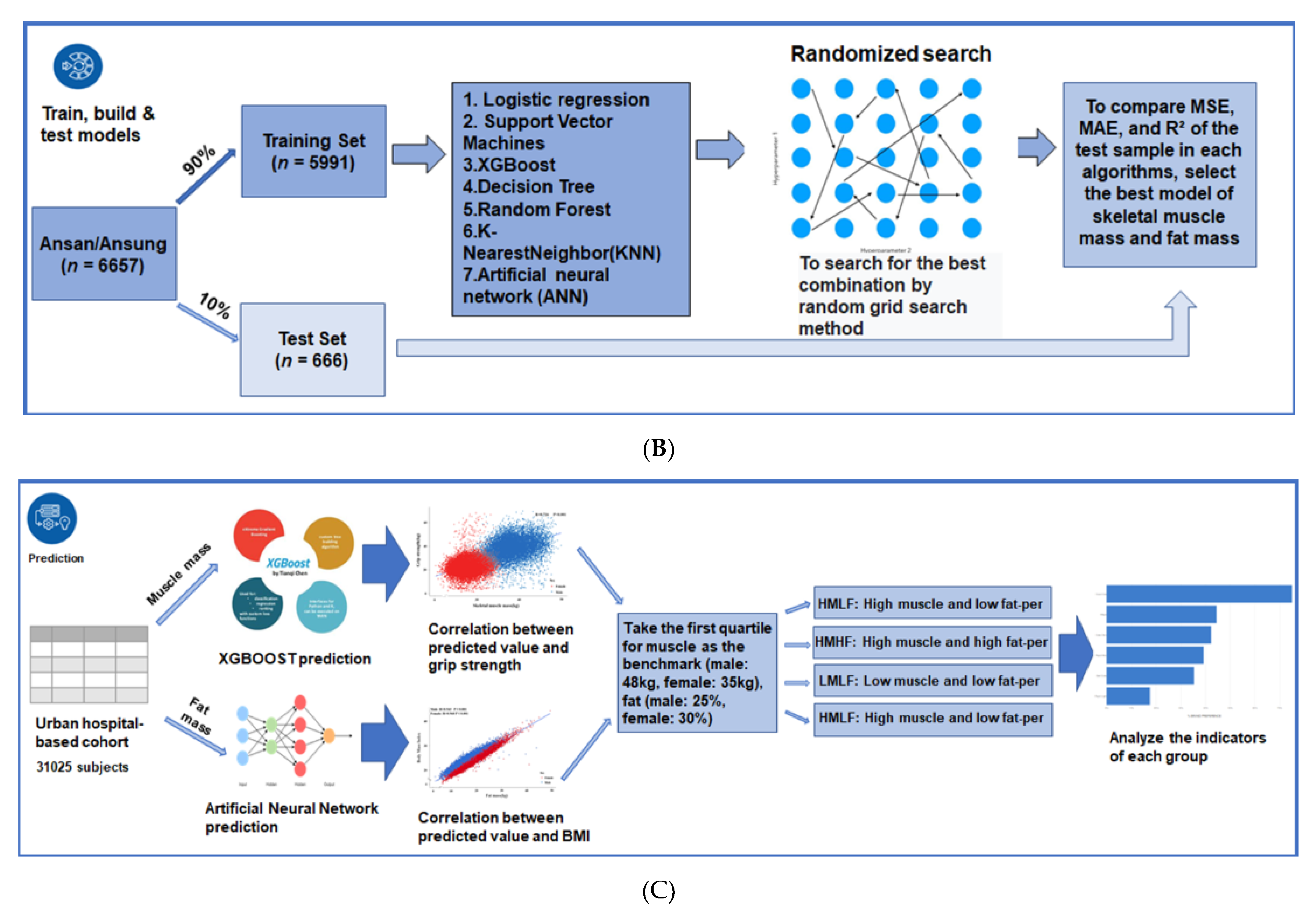
2.2. Experiment Design
2.3. Training for SMM and FM Prediction Model
2.4. Verifying the Predictive Models
2.5. Predictions of SMM and FM in the Urban Hospital-Based Cohort Using the Predictive Algorithm Models
2.6. Statistical Analysis
3. Results
3.1. Metabolic Characteristics of the Ansan/Ansung and Urban Hospital-Based Cohorts
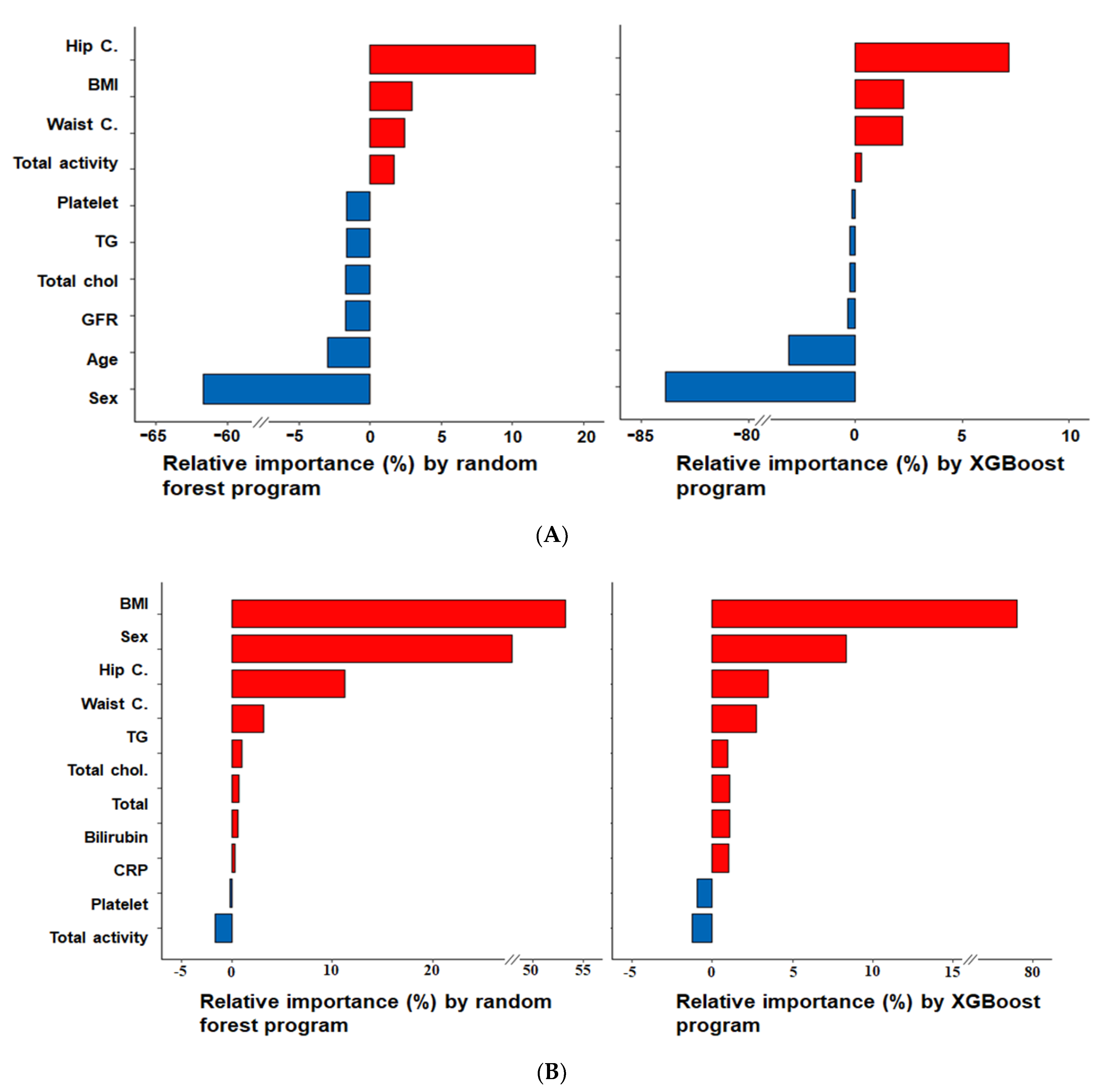
3.2. Relative Importance of Parameters in the Random Forest and XGBoost Prediction Models
3.3. Accuracies of the Predictive Models for SMM and FM Using XGBoost and ANN Algorithm in the Test Set
3.4. Anthropometric and Metabolic Parameters According to Predicted SMM and FM in Men and Women in the Urban Hospital-Based Cohort
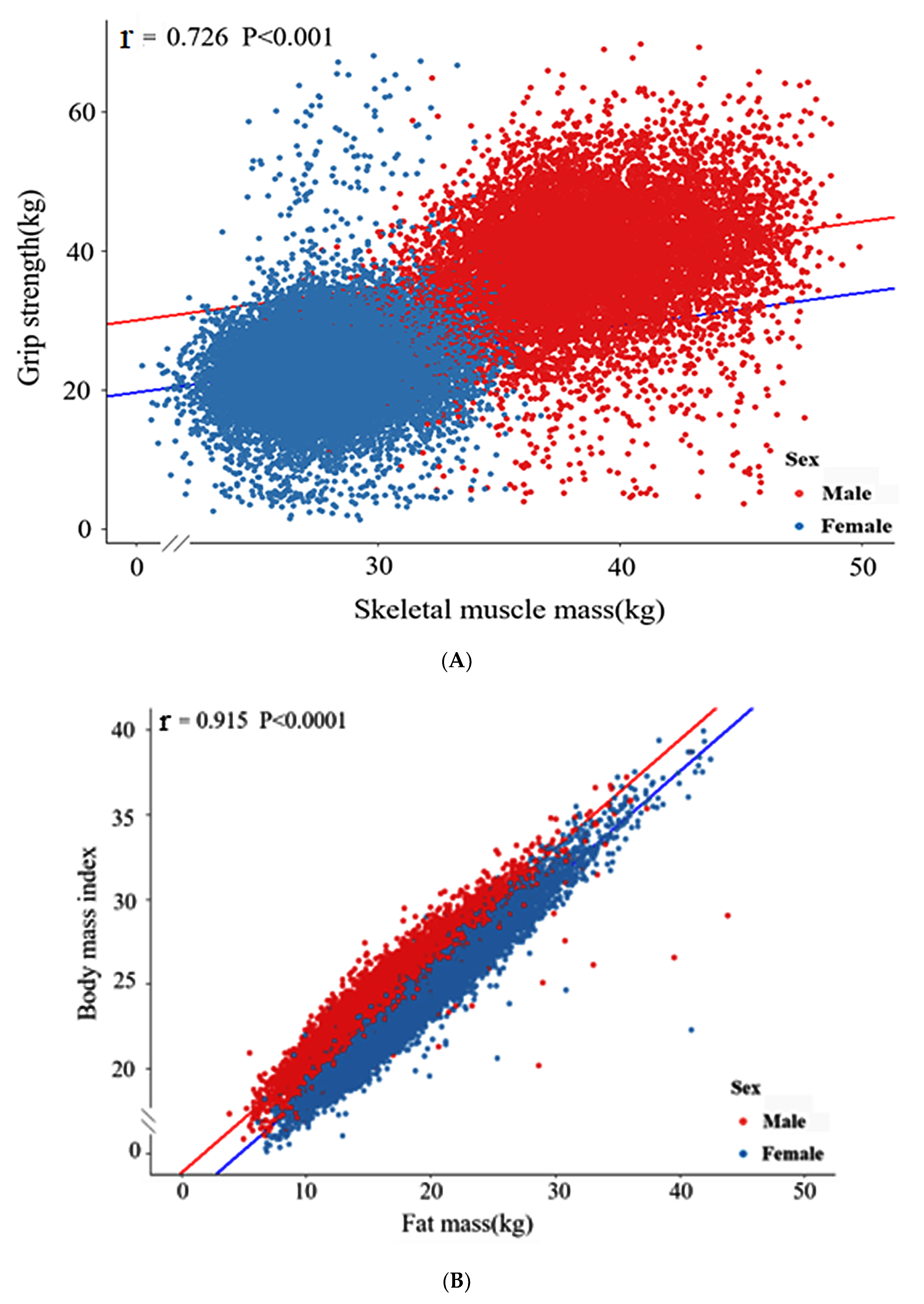
3.5. Linear Relationship between SMM and Grip Strength in the Urban Hospital-Based Cohort
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kwon, I.; Kim, J.-S.; Shin, C.-H.; Park, Y.; Kim, J.-H. Associations Between Skeletal Muscle Mass, Grip Strength, and Physical and Cognitive Functions in Elderly Women: Effect of Exercise with Resistive Theraband. J. Exerc. Nutr. Biochem. 2019, 23, 50–55. [Google Scholar] [CrossRef] [PubMed]
- Syddall, H.E.; Westbury, L.D.; Dodds, R.; Dennison, E.; Cooper, C.; Sayer, A.A. Mortality in the Hertfordshire Ageing Study: Association with level and loss of hand grip strength in later life. Age Ageing 2017, 46, 407–412. [Google Scholar] [CrossRef] [PubMed]
- Bonaccorso, G. Machine Learning Algorithms; Packt Publishing Ltd: London, UK, 2017. [Google Scholar]
- Epstein, D.H.; Tyburski, M.; Kowalczyk, W.J.; Burgess-Hull, A.J.; Phillips, K.A.; Curtis, B.L.; Preston, K.L. Prediction of stress and drug craving ninety minutes in the future with passively collected GPS data. NPJ Digit. Med. 2020, 3, 1–12. [Google Scholar] [CrossRef]
- Lee, H.-S.; Park, T.-J.; Kim, J.-M.; Yun, J.H.; Yu, H.-Y.; Kim, Y.-J.; Kim, B.-J. Identification of metabolic markers predictive of prediabetes in a Korean population. Sci. Rep. 2020, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Salami, D.; Sousa, C.A.; Martins, M.D.R.O.; Capinha, C. Predicting dengue importation into Europe, using machine learning and model-agnostic methods. Sci. Rep. 2020, 10, 9689. [Google Scholar] [CrossRef]
- Carson, J.A.; Manolagas, S.C. Effects of sex steroids on bones and muscles: Similarities, parallels, and putative interactions in health and disease. Bone 2015, 80, 67–78. [Google Scholar] [CrossRef]
- Rosa-Caldwell, M.E.; Greene, N.P. Muscle metabolism and atrophy: Let’s talk about sex. Biol. Sex Differ. 2019, 10, 1–14. [Google Scholar] [CrossRef]
- Pöllänen, E.; Kangas, R.; Horttanainen, M.; Niskala, P.; Kaprio, J.; Butler-Browne, G.; Mouly, V.; Sipilä, S.; Kovanen, V. Intramuscular sex steroid hormones are associated with skeletal muscle strength and power in women with different hormonal status. Aging Cell 2015, 14, 236–248. [Google Scholar] [CrossRef]
- Tiidus, P.M.; Lowe, D.A.; Brown, M. Estrogen replacement and skeletal muscle: Mechanisms and population health. J. Appl. Physiol. 2013, 115, 569–578. [Google Scholar] [CrossRef]
- Lizcano, F.; Guzmán, G. Estrogen Deficiency and the Origin of Obesity during Menopause. BioMed Res. Int. 2014, 2014, 1–11. [Google Scholar] [CrossRef]
- Molnar, C. Interpretable Machine Learning; Lulu Press Inc: Morrisville, NC, USA, 2020. [Google Scholar]
- Zhai, Q.; Lin, Z.; Ge, H.; Liang, Y.; Li, N.; Ma, Q.; Ye, C. Using machine learning tools to predict outcomes for emergency department intensive care unit patients. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Bray, G.A.; Heisel, W.E.; Afshin, A.; Jensen, M.D.; Dietz, W.H.; Long, M.; Kushner, R.F.; Daniels, S.R.; Wadden, T.A.; Tsai, A.G.; et al. The Science of Obesity Management: An Endocrine Society Scientific Statement. Endocr. Rev. 2018, 39, 79–132. [Google Scholar] [CrossRef]
- Schaap, L.A.; Koster, A.; Visser, M. Adiposity, Muscle Mass, and Muscle Strength in Relation to Functional Decline in Older Persons. Epidemiol. Rev. 2012, 35, 51–65. [Google Scholar] [CrossRef] [PubMed]
- Wilkinson, D.; Piasecki, M.; Atherton, P. The age-related loss of skeletal muscle mass and function: Measurement and physiology of muscle fibre atrophy and muscle fibre loss in humans. Ageing Res. Rev. 2018, 47, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Hellberg, M.; Svensson, P.; Höglund, P.; Clyne, N. Sarcopenia and relationships between muscle mass, measured glomerular filtration rate and physical function in patients with chronic kidney disease stages 3–5. Nephrol. Dial. Transplant. 2018, 33, 342–348. [Google Scholar] [CrossRef] [PubMed]
- Scully, D.; Naseem, K.M.; Matsakas, A. Platelet biology in regenerative medicine of skeletal muscle. Acta Physiol. 2018, 223, e13071. [Google Scholar] [CrossRef]
- Santilli, F.; Vazzana, N.; Liani, R.; Guagnano, M.T.; Davì, G. Platelet activation in obesity and metabolic syndrome. Obes. Rev. 2011, 13, 27–42. [Google Scholar] [CrossRef] [PubMed]
- Shah, B.; Sha, D.; Xie, D.; Mohler, E.R.; Berger, J.S. The Relationship Between Diabetes, Metabolic Syndrome, and Platelet Activity as Measured by Mean Platelet Volume: The National Health and Nutrition Examination Survey, 1999-2004. Diabetes Care 2012, 35, 1074–1078. [Google Scholar] [CrossRef] [PubMed]
- Mika, A.; Sledzinski, T. Alterations of specific lipid groups in serum of obese humans: A review. Obes. Rev. 2016, 18, 247–272. [Google Scholar] [CrossRef]
- Hinds, T.D., Jr.; Creeden, J.F.; Gordon, D.M.; Stec, D.F.; Donald, M.C.; Stec, D.E. Bilirubin nanoparticles reduce diet-induced hepatic steatosis, improve fat utilization, and increase plasma β-hydroxybutyrate. Front. Pharmacol. 2020, 11, 594574. [Google Scholar] [CrossRef]
- Akyea, R.K.; Qureshi, N.; Kai, J.; Weng, S.F. Performance and clinical utility of supervised machine-learning approaches in detecting familial hypercholesterolaemia in primary care. NPJ Digit. Med. 2020, 3, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ma, X.; Ng, M.; Xu, S.; Xu, Z.; Qiu, H.; Liu, Y.; Lyu, J.; You, J.; Zhao, P.; Wang, S.; et al. Development and validation of prognosis model of mortality risk in patients with COVID-19. Epidemiol. Infect. 2020, 148, 1–25. [Google Scholar] [CrossRef] [PubMed]
- Choe, Y.; Jeong, J.; Kim, Y. Grip strength mediates the relationship between muscle mass and frailty. J. Cachex. Sarcopenia Muscle 2019, 11, 441–451. [Google Scholar] [CrossRef] [PubMed]
- Bowen, J.; Luscombe-Marsh, N.D.; Stonehouse, W.; Tran, C.; Rogers, G.B.; Johnson, N.; Thompson, C.H.; Brinkworth, G.D. Effects of almond consumption on metabolic function and liver fat in overweight and obese adults with elevated fasting blood glucose: A randomised controlled trial. Clin. Nutr. ESPEN 2019, 30, 10–18. [Google Scholar] [CrossRef]
- Verma, S.; Hussain, M.E. Obesity and diabetes: An update. Diabetes Metab. Syndr. Clin. Res. Rev. 2017, 11, 73–79. [Google Scholar] [CrossRef]
- Sherwani, S.I.; Khan, H.A.; Ekhzaimy, A.; Masood, A.; Sakharkar, M.K. Significance of HbA1c Test in Diagnosis and Prognosis of Diabetic Patients. Biomark. Insights 2016, 11, 95–104. [Google Scholar] [CrossRef]
- Alpar, R. Applied Statistic and Validation-Reliability; Detay Publishing: Ankara, Turkey, 2010. [Google Scholar]
- Lundberg, S.M.; Nair, B.; Vavilala, M.S.; Horibe, M.; Eisses, M.J.; Adams, T.; Liston, D.E.; Low, D.K.-W.; Newman, S.-F.; Kim, J.; et al. Explainable machine-learning predictions for the prevention of hypoxaemia during surgery. Nat. Biomed. Eng. 2018, 2, 749–760. [Google Scholar] [CrossRef] [PubMed]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Ansan/Ansung Cohort | Urban Hospital-Based Cohort | ||
|---|---|---|---|---|
| Men (3216) | Women (3441) | Men (n = 10,370) | Women (n = 20,655) | |
| Age (years) | 50.6 ± 8.46 | 51.8 ± 8.88 *** | 55.2 ± 8.30 | 53.1 ± 7.75 *** |
| Body mass index (kg/m2) | 24.4 ± 2.86 | 24.8 ± 3.24 *** | 24.5 ± 2.71 | 23.6 ± 2.98 *** |
| Waist circumferences (cm) | 83.6 ± 7.51 | 80.6 ± 9.49 *** | 85.5 ± 7.49 | 77.8 ± 8.05 *** |
| Hip circumferences (cm) | 94.4 ± 5.54 | 94.1 ± 5.96 | 95.4 ± 5.71 | 92.8 ± 5.8 *** |
| Skeletal muscle mass (kg) | 37.7 ± 4.51 | 28.3 ± 3.21 *** | - | - |
| Fat mass (kg) | 15.2 ± 4.81 | 19.0 ± 5.29 *** | - | - |
| Grip strength (kg) | - | - | 38.5 ± 0.09 | 23.3 ± 0.04 *** |
| Serum glucose (mg/dL) | 116 ± 16.3 | 115 ± 19.2 | 100 ± 22.9 | 93.8 ± 18.1 *** |
| Blood HbA1c (%) | 5.78 ± 0.02 | 5.73 ± 0.01 | 5.78 ± 0.01 | 5.68 ± 0.005 *** |
| SBP (mmHg) | 75.8 ± 11.4 | 72.9 ± 11.9 *** | 38.5 ± 0.09 | 23.3 ± 0.04 *** |
| DBP (mmHg) | 91.1 ± 24.4 | 85.2 ± 20.3 *** | 100 ± 22.9 | 93.8 ± 18.1 *** |
| Serum triglyceride (mg/dL) | 177 ± 118 | 146 ± 86.5 *** | 148 ± 102 | 114 ± 74.0 *** |
| Serum HDL (mg/dL) | 43.4 ± 9.69 | 45.9 ± 10.2 *** | 50.2 ± 12.3 | 57.6 ± 13.7 *** |
| Serum total cholesterol (mg/dL) | 194 ± 36.3 | 192 ± 36.2 ** | 193 ± 35.9 | 201 ± 36.3 *** |
| Serum CRP (mg/dL) | 0.23 ± 0.44 | 0.21 ± 0.41 | 0.16 ± 0.44 | 0.13 ± 0.38 *** |
| Serum total bilirubin (mg/dL) | 0.73 ± 0.37 | 0.54 ± 0.26 *** | 0.83 ± 0.34 | 0.67 ± 0.26 *** |
| Blood platelet (103/µL) | 259 ± 64.9 | 271 ± 63.6 *** | 237 ± 54.1 | 262 ± 59.8 *** |
| GFR (mL/min) | 77.7 ± 8.97 | 83.7 ± 15.7 *** | 84.3 ± 14.8 | 120 ± 20.9 *** |
| Energy intake (EER%) | 96.4 ± 32.3 | 104 ± 38.6 *** | 90.8 ± 25.9 | 101 ± 32.9 *** |
| CHO intake (energy%) | 69.1 ± 6.48 | 71.5 ± 6.77 *** | 71.0 ± 7.03 | 71.8 ± 7.14 *** |
| Protein intake (energy%) | 13.9 ± 2.29 | 13.6 ± 2.37 *** | 13.4 ± 2.54 | 13.4 ± 2.57 |
| Fat intake (energy%) | 15.7 ± 4.98 | 13.8 ± 5.26 *** | 14.5 ± 5.49 | 13.9 ± 5.56 *** |
| Machine Learning Algorithm | Prediction of SMM | Prediction of FM | ||||
|---|---|---|---|---|---|---|
| MSE a | MAE b | R² c | MSE a | MAE b | R² c | |
| Linear regression | 2.60 | 2.03 | 0.82 | 1.86 | 1.48 | 0.89 |
| Support Vector Machines | 2.71 | 2.12 | 0.80 | 1.98 | 1.52 | 0.87 |
| XGBoost | 2.56 | 2 | 0.82 | 1.82 | 1.43 | 0.89 |
| Decision Tree | 2.81 | 2.22 | 0.78 | 2.21 | 1.75 | 0.84 |
| Random Forest | 2.65 | 2.09 | 0.81 | 1.80 | 1.41 | 0.89 |
| K-Nearest Neighbor (KNN) | 3.08 | 2.4 | 0.74 | 2.16 | 1.68 | 0.85 |
| Artificial neural network (ANN) | 2.57 | 2 | 0.82 | 1.79 | 1.4 | 0.89 |
| Metabolic Parameters | HMLF (n = 4448) | HMHF (n = 3201) | LMLF (n = 2517) | LMHF (n = 231) |
|---|---|---|---|---|
| Predicted SMM (kg) | 38.7 ± 0.03 b | 41.3 ± 0.05 a | 34.3 ± 0.03 d | 35.0 ± 0.06 c |
| Predicted FM (%) | 22.4 ± 0.03 c | 27.3 ± 0.04 a | 20.1 ± 0.06 d | 26.6 ± 0.15 b |
| Body mass index (kg/m2) | 24.1 ± 0.02 c | 27.0 ± 0.04 a | 21.8 ± 0.04 d | 24.6 ± 0.10 b |
| Waist circumferences (cm) | 84.7 ± 0.08 c | 92.5 ± 0.10 a | 78.3 ± 0.11 d | 85.4 ± 0.29 b |
| Hip circumferences (cm) | 95.6 ± 0.05 b | 100 ± 0.09 a | 89.2 ± 0.07 d | 91.8 ± 0.17 c |
| Grip strength (kg) | 39.9 ± 0.13 a | 38.6 ± 0.17 b | 36.3 ± 0.16 c | 33.8 ± 0.54 d |
| Serum glucose (mg/dL) | 98.6 ± 0.33 b | 102 ± 0.40 a | 98.6 ± 0.46 b | 102 ± 1.94 a |
| Blood HBA1C (%) | 5.70 ± 0.01 b | 5.93 ± 0.01 a | 5.72 ± 0.02 b | 5.91 ± 0.06 a |
| Serum triglyceride (mg/dL) | 141 ± 1.56 b | 177 ± 1.87 a | 124 ± 1.73 b | 173 ± 6.90 a |
| Serum HDL (mg/dL) | 50.2 ± 0.18 b | 46.9 ± 0.18 c | 54.3 ± 0.27 a | 49.2 ± 0.82 b |
| GFR (mL/min) | 84.0 ± 0.22 bc | 82.9 ± 0.27 c | 86.3 ± 0.29 a | 85.4 ± 0.93 ab |
| Alcohol intake (g/day) | 39.0 ± 1.09 a | 39.8 ± 1.06 a | 29.1 ± 0.77b | 32.7 ± 3.24 b |
| Metabolic parameters | HMLF (n = 5220) | HMHF (n = 10,522) | LMLF (n = 3615) | LMHF (n = 1368) |
|---|---|---|---|---|
| Predicted SMM (kg) | 27.8 ± 0.02 b | 29.3 ± 0.02 a | 25.0 ± 0.02 d | 25.4 ± 0.02 c |
| Predicted FM (%) | 27.6 ± 0.03 c | 34.0 ± 0.03 a | 26.2 ± 0.04 d | 32.2 ± 0.06 b |
| Body mass index (kg/m2) | 21.8 ± 0.02 c | 25.5 ± 0.02 a | 20.6 ± 0.03 d | 23.4 ± 0.04 b |
| Waist circumferences (cm) | 74.3 ± 0.07 c | 82.6 ± 0.07 a | 69.4 ± 0.09 d | 76.6 ± 0.14 b |
| Hip circumferences (cm) | 91.3 ± 0.05 b | 96.4 ± 0.05 a | 85.9 ± 0.06 d | 89.04 ± 0.08 c |
| Grip strength (kg) | 24.6 ± 0.08 a | 23.3 ± 0.06 b | 22.6 ± 0.09 c | 20.5 ± 0.13 d |
| Serum glucose (mg/dL) | 90.8 ± 0.19 d | 95.4 ± 0.19 b | 92.5 ± 0.28 c | 96.4 ± 0.70 a |
| Blood HBA1C (%) | 5.52 ± 0.01 d | 5.76 ± 0.01 b | 5.61 ± 0.01 c | 5.85 ± 0.02 a |
| Serum triglyceride (mg/dL) | 92.3 ± 0.87 d | 125 ± 0.77 b | 104 ± 1.04 c | 137 ± 2.07 a |
| Serum HDL (mg/dL) | 60.3 ± 0.19 b | 55.1 ± 0.12 c | 61.2 ± 0.25 a | 55.8 ± 0.36 c |
| GFR (mL/min) | 122 ± 0.28 a | 120 ± 0.21 b | 118 ± 0.34 c | 116 ± 0.59 d |
| Alcohol intake (g/day) | 6.89 ± 0.21 a | 6.39 ± 0.41 a | 4.81 ± 0.23 b | 3.14 ± 0.32 c |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, X.; Park, S. An Inverse Relation between Hyperglycemia and Skeletal Muscle Mass Predicted by Using a Machine Learning Approach in Middle-Aged and Older Adults in Large Cohorts. J. Clin. Med. 2021, 10, 2133. https://doi.org/10.3390/jcm10102133
Wu X, Park S. An Inverse Relation between Hyperglycemia and Skeletal Muscle Mass Predicted by Using a Machine Learning Approach in Middle-Aged and Older Adults in Large Cohorts. Journal of Clinical Medicine. 2021; 10(10):2133. https://doi.org/10.3390/jcm10102133
Chicago/Turabian StyleWu, Xuangao, and Sunmin Park. 2021. "An Inverse Relation between Hyperglycemia and Skeletal Muscle Mass Predicted by Using a Machine Learning Approach in Middle-Aged and Older Adults in Large Cohorts" Journal of Clinical Medicine 10, no. 10: 2133. https://doi.org/10.3390/jcm10102133
APA StyleWu, X., & Park, S. (2021). An Inverse Relation between Hyperglycemia and Skeletal Muscle Mass Predicted by Using a Machine Learning Approach in Middle-Aged and Older Adults in Large Cohorts. Journal of Clinical Medicine, 10(10), 2133. https://doi.org/10.3390/jcm10102133