
Erectile Dysfunction Is the Main Correlate of Depression in Men with Chronic Spinal Cord Injury

 ,
,
Abstract
1. Introduction
2. Materials and Methods
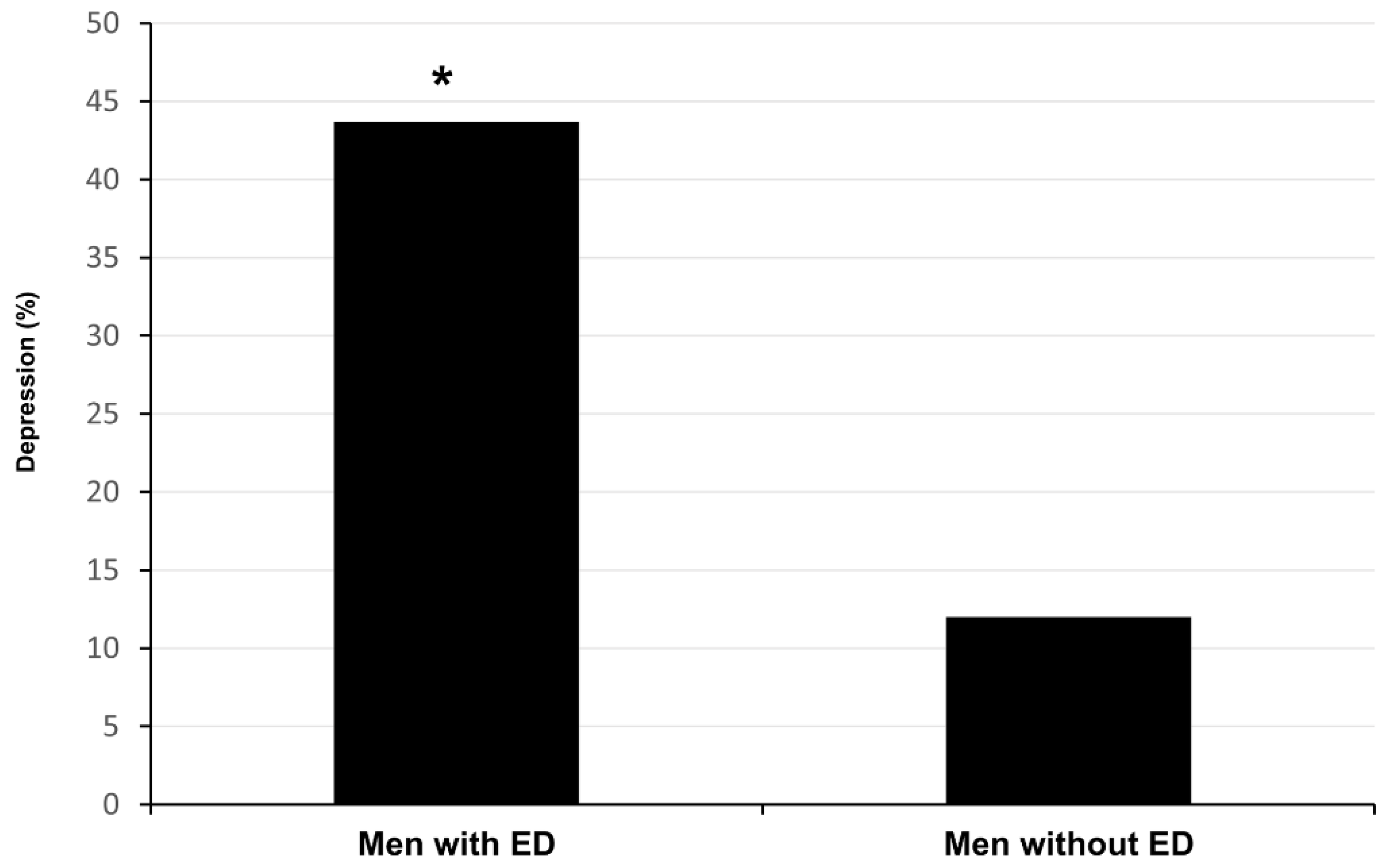
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bombardier, C.H.; Richards, J.S.; Krause, J.S.; Tulsky, D.; Tate, D.G. Symptoms of major depression in people with spinal cord injury: Implications for screening. Arch. Phys. Med. Rehabil. 2004, 85, 1749–1756. [Google Scholar] [CrossRef] [PubMed]
- Craig, A.; Tran, Y.; Middleton, J. Psychological morbidity and spinal cord injury: A systematic review. Spinal Cord 2009, 47, 108–114. [Google Scholar] [CrossRef] [PubMed]
- Kessler, R.C.; Chiu, W.T.; Demler, O.; Merikangas, K.R.; Walters, E.E. Prevalence, severity, and comorbidity of 12-month DSM-IV disorders in the National Comorbidity Survey Replication. Arch. Gen. Psychiatry 2005, 62, 617–627. [Google Scholar] [CrossRef]
- January, A.M.; Zebracki, K.; Chlan, K.M.; Vogel, L.C. Mental health and risk of secondary medical complications in adults with pediatric-onset spinal cord injury. Top. Spinal Cord Inj. Rehabil. 2014, 20, 1–12. [Google Scholar] [CrossRef]
- Arango-Lasprilla, J.C.; Ketchum, J.M.; Starkweather, A.; Nicholls, E.; Wilk, A.R. Factors predicting depression among persons with spinal cord injury 1 to 5 years post injury. Neuro Rehabil. 2011, 29, 9–21. [Google Scholar] [CrossRef]
- Hartoonian, N.; Hoffman, J.M.; Kalpakjian, C.Z.; Taylor, H.B.; Krause, J.K.; Bombardier, C.H. Evaluating a spinal cord injury-specific model of depression and quality of life. Arch. Phys. Med. Rehabil. 2014, 95, 455–465. [Google Scholar] [CrossRef] [PubMed]
- Krause, J.S.; Carter, R.E.; Pickelsimer, E.E.; Wilson, D. A prospective study of health and risk of mortality after spinal cord injury. Arch. Phys. Med. Rehabil. 2008, 89, 1482–1491. [Google Scholar] [CrossRef]
- DeVivo, M.J.; Black, K.J.; Richards, S.; Stover, S.L. Suicide following spinal cord injury. Paraplegia 1991, 29, 620–627. [Google Scholar] [CrossRef]
- Judd, F.K.; Brown, D.J. Suicide following acute traumatic spinal cord injury. Paraplegia 1992, 30, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.T.; Wilson, C.S.; Heinemann, A.W.; Lazowski, L.E.; Fann, J.R.; Bombardier, C.H. PRISMS Investigators. Identifying depression severity risk factors in persons with traumatic spinal cord injury. Rehabil. Psychol. 2014, 59, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Kraft, R.; Dorstyn, D. Psychosocial correlates of depression following spinal injury: A systematic review. J. Spinal Cord Med. 2015, 38, 571–583. [Google Scholar] [CrossRef] [PubMed][Green Version]
- de Roon-Cassini, T.A.; Mancini, A.D.; Rusch, M.D.; Bonanno, G.A. Psychopathology and resilience following traumatic injury: A latent growth mixture model analysis. Rehabil. Psychol. 2010, 55, 1–11. [Google Scholar] [CrossRef]
- National Spinal Cord Injury Statistical Center. Facts and Figures at a Glance; University of Alabama at Birmingham: Birmingham, AL, USA, 2020. [Google Scholar]
- Anderson, K.D.; Borisoff, J.F.; Johnson, R.D.; Stiens, S.A.; Elliott, S.L. The impact of spinal cord injury on sexual function: Concerns of the general population. Spinal Cord 2007, 45, 328–337. [Google Scholar] [CrossRef] [PubMed]
- Barbonetti, A.; Cavallo, F.; Felzani, G.; Francavilla, S.; Francavilla, F. Erectile dysfunction is the main determinant of psychological distress in men with spinal cord injury. J. Sex. Med. 2012, 9, 830–836. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, S.; Minaldi, E.; Castellini, C.; Cavallo, F.; Felzani, G.; Francavilla, S.; Francavilla, F.; Barbonetti, A. Independent Association of Erectile Dysfunction and Low Testosterone Levels with Life Dissatisfaction in Men with Chronic Spinal Cord Injury. J. Sex. Med. 2020, 17, 911–918. [Google Scholar] [CrossRef] [PubMed]
- NIH Consensus Conference. Impotence. NIH Consensus Development Panel on Impotence. JAMA 1993, 270, 83–90. [Google Scholar] [CrossRef]
- Zarrouf, F.A.; Artz, S.; Griffith, J.; Sirbu, C.; Kommor, M. Testosterone and depression: Systematic review and meta-analysis. J. Psychiatr. Pract. 2009, 15, 289–305. [Google Scholar] [CrossRef]
- Ganji, V.; Milone, C.; Cody, M.M.; McCarty, F.; Wang, Y.T. Serum vitamin D concentrations are related to depression in young adult US population: The Third National Health and Nutrition Examination Survey. Int. Arch. Med. 2010, 3, 29. [Google Scholar] [CrossRef]
- Lee, D.M.; Tajar, A.; O’Neill, T.W.; O’Connor, D.B.; Bartfai, G.; Boonen, S.; Bouillon, R.; Casanueva, F.F.; Finn, J.D.; Forti, G.; et al. Lower vitamin D levels are associated with depression among community-dwelling European men. J. Psychopharmacol. 2011, 25, 1320–1328. [Google Scholar] [CrossRef] [PubMed]
- Barbonetti, A.; Cavallo, F.; D’Andrea, S.; Muselli, M.; Felzani, G.; Francavilla, S.; Francavilla, F. Lower Vitamin D Levels Are Associated with Depression in People with Chronic Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2017, 98, 940–946. [Google Scholar] [CrossRef]
- Maynard, F.M., Jr.; Bracken, M.B.; Creasey, G.; Ditunno, J.F., Jr.; Donovan, W.H.; Ducker, T.B.; Garber, S.L.; Marino, R.J.; Stover, S.L.; Tator, C.H.; et al. International Standards for Neurological and Functional Classification of Spinal Cord Injury. American Spinal Injury Association. Spinal Cord 1997, 35, 266–274. [Google Scholar] [CrossRef]
- Kirshblum, S.C.; Burns, S.P.; Biering-Sorensen, F.; Donovan, W.; Graves, D.E.; Jha, A.; Johansen, M.; Jones, L.; Krassioukov, A.; Mulcahey, M.J.; et al. International standards for neurological classification of spinal cord injury (revised 2011). J. Spinal Cord Med. 2011, 34, 535–546. [Google Scholar] [CrossRef]
- Catz, A.; Itzkovich, M.; Agranov, E.; Ring, H.; Tamir, A. SCIM—Spinal cord independence measure: A new disability scale for patients with spinal cord lesions. Spinal Cord 1997, 35, 850–856. [Google Scholar] [CrossRef] [PubMed]
- Anderson, K.; Aito, S.; Atkins, M.; Biering-Sørensen, F.; Charlifue, S.; Curt, A.; Ditunno, J.; Glass, C.; Marino, R.; Marshall, R.; et al. Functional recovery measures for spinal cord injury: An evidence-based review for clinical practice and research. J. Spinal Cord Med. 2008, 31, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Ginis, K.A.; Hicks, A.L.; Latimer, A.E.; Warburton, D.E.; Bourne, C.; Ditor, D.S.; Goodwin, D.L.; Hayes, K.C.; McCartney, N.; McIlraith, A.; et al. The development of evidence-informed physical activity guidelines for adults with spinal cord injury. Spinal Cord 2011, 49, 1088–1096. [Google Scholar] [CrossRef]
- Williams, T.L.; Smith, B.; Papathomas, A. The barriers, benefits and facilitators of leisure time physical activity among people with spinal cord injury: A meta-synthesis of qualitative findings. Health Psychol. Rev. 2014, 8, 404–425. [Google Scholar] [CrossRef] [PubMed]
- Barbonetti, A.; Vassallo, M.R.; Felzani, G.; Francavilla, S.; Francavilla, F. Association between 25(OH)-vitamin D and testosterone levels: Evidence from men with chronic spinal cord injury. J. Spinal Cord Med. 2016, 39, 246–252. [Google Scholar] [CrossRef]
- Barbonetti, A.; Sperandio, A.; Micillo, A.; D’Andrea, S.; Pacca, F.; Felzani, G.; Francavilla, S.; Francavilla, F. Independent Association of Vitamin D with Physical Function in People with Chronic Spinal Cord Injury. Arch. Phys. Med. Rehabil. 2016, 97, 726–732. [Google Scholar] [CrossRef]
- Barbonetti, A.; Vassallo, M.R.; Pacca, F.; Cavallo, F.; Costanzo, M.; Felzani, G.; Francavilla, S.; Francavilla, F. Correlates of low testosterone in men with chronic spinal cord injury. Andrology 2014, 2, 721–728. [Google Scholar] [CrossRef]
- Bryce, T.N.; Budh, C.N.; Cardenas, D.D.; Dijkers, M.; Felix, E.R.; Finnerup, N.B.; Kennedy, P.; Lundeberg, T.; Richards, J.S.; Rintala, D.H.; et al. Pain after spinal cord injury: An evidence-based review for clinical practice and research. Report of the National Institute on Disability and Rehabilitation Research Spinal Cord Injury Measures meeting. J. Spinal Cord Med. 2007, 30, 421–440. [Google Scholar] [CrossRef] [PubMed]
- Charlson, M.; Szatrowski, T.P.; Peterson, J.; Gold, J. Validation of a combined comorbidity index. J. Clin. Epidemiol. 1994, 47, 1245–1251. [Google Scholar] [CrossRef]
- Rosen, R.C.; Cappelleri, J.C.; Smith, M.D.; Lipsky, J.; Peña, B.M. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int. J. Impot Res. 1999, 11, 319–326. [Google Scholar] [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G.K. Manual for the Beck Depression Inventory-II; Psychological Corporation: San Antonio, TX, USA, 1996. [Google Scholar]
- Segal, D.L.; Coolidge, F.L.; Cahill, B.S.; O’Riley, A.A. Psychometric properties of the Beck Depression Inventory II (BDI-II) among community-dwelling older adults. Behav. Modif. 2008, 32, 3–20. [Google Scholar] [CrossRef]
- Ataoğlu, E.; Tiftik, T.; Kara, M.; Tunç, H.; Ersöz, M.; Akkuş, S. Effects of chronic pain on quality of life and depression in patients with spinal cord injury. Spinal Cord 2013, 51, 23–26. [Google Scholar] [CrossRef]
- Xue, S.; Arya, S.; Embuldeniya, A.; Narammalage, H.; da Silva, T.; Williams, S.; Ravindran, A. Perceived functional impairment and spirituality/religiosity as predictors of depression in a Sri Lankan spinal cord injury patient population. Spinal Cord 2016, 54, 1158–1163. [Google Scholar] [CrossRef] [PubMed]
- Vermeulen, A.; Verdonck, L.; Kaufman, J.M. A critical evaluation of simple methods for the estimation of free testosterone in serum. J. Clin. Endocrinol. Metab. 1999, 84, 3666–3672. [Google Scholar] [CrossRef]
- Derogatis, L.R.; Meyer, J.K.; King, K.M. Psychopathology in individuals with sexual dysfunction. Am. J. Psychiatry 1981, 138, 757–763. [Google Scholar] [PubMed]
- Mallis, D.; Moysidis, K.; Nakopoulou, E.; Papaharitou, S.; Hatzimouratidis, K.; Hatzichristou, D. Psychiatric morbidity is frequently undetected in patients with erectile dysfunction. J. Urol. 2005, 174, 1913–1916. [Google Scholar] [CrossRef]
- Liu, Q.; Zhang, Y.; Wang, J.; Li, S.; Cheng, Y.; Guo, J.; Tang, Y.; Zeng, H.; Zhu, Z. Erectile Dysfunction and Depression: A Systematic Review and Meta-Analysis. J. Sex. Med. 2018, 15, 1073–1082. [Google Scholar] [CrossRef] [PubMed]
- Williams, R.; Murray, A. Prevalence of depression after spinal cord injury: A meta-analysis. Arch. Phys. Med. Rehabil. 2015, 96, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Oh, S.J.; Shin, H.I.; Paik, N.J.; Yoo, T.; Ku, J.H. Depressive symptoms of patients using clean intermittent catheterization for neurogenic bladder secondary to spinal cord injury. Spinal Cord 2006, 44, 757–762. [Google Scholar] [CrossRef][Green Version]
- Migliorini, C.E.; New, P.W.; Tonge, B.J. Comparison of depression, anxiety and stress in persons with traumatic and non-traumatic post-acute spinal cord injury. Spinal Cord 2009, 47, 783–788. [Google Scholar] [CrossRef] [PubMed]
- Fann, J.R.; Bombardier, C.H.; Richards, J.S.; Tate, D.G.; Wilson, C.S.; Temkin, N.; PRISMS Investigators. Depression after spinal cord injury: Comorbidities, mental health service use, and adequacy of treatment. Arch. Phys. Med. Rehabil. 2011, 92, 352–360. [Google Scholar] [CrossRef]
- Bombardier, C.H.; Fann, J.R.; Tate, D.G.; Richards, J.S.; Wilson, C.S.; Warren, A.M.; Temkin, N.R.; Heinemann, A.W.; PRISMS Investigators. An exploration of modifiable risk factors for depression after spinal cord injury: Which factors should we target? Arch. Phys. Med. Rehabil. 2012, 93, 775–781. [Google Scholar] [CrossRef]
- Gerhart, K.A.; Koziol-McLain, J.; Lowenstein, S.R.; Whiteneck, G.G. Quality of life following spinal cord injury: Knowledge and attitudes of emergency care providers. Ann. Emerg. Med. 1994, 23, 807–812. [Google Scholar] [CrossRef]
- Stensman, R. Adjustment to traumatic spinal cord injury. A longitudinal study of self-reported quality of life. Paraplegia 1994, 32, 416–422. [Google Scholar] [CrossRef] [PubMed][Green Version]
- McColl, M.A. Expectations of health, independence, and quality of life among aging spinal cord-injured adults. Assist. Technol. 1999, 11, 130–136. [Google Scholar] [CrossRef] [PubMed]
- Benevento, B.T.; Sipski, M.L. Neurogenic bladder, neurogenic bowel, and sexual dysfunction in people with spinal cord injury. Phys. Ther. 2002, 82, 601–612. [Google Scholar] [CrossRef]
- Liu, C.W.; Huang, C.C.; Chen, C.H.; Yang, Y.H.; Chen, T.W.; Huang, M.H. Prediction of severe neurogenic bowel dysfunction in persons with spinal cord injury. Spinal Cord 2010, 48, 554–559. [Google Scholar] [CrossRef] [PubMed]
- Wu, F.C.; Tajar, A.; Beynon, J.M.; Pye, S.R.; Silman, A.J.; Finn, J.D.; O’Neill, T.W.; Bartfai, G.; Casanueva, F.F.; Forti, G.; et al. Identification of late-onset hypogonadism in middle-aged and elderly men. N. Engl. J. Med. 2010, 363, 123–135. [Google Scholar] [CrossRef]
- Alexander, M.S.; Brackett, N.L.; Bodner, D.; Elliott, S.; Jackson, A.; Sonksen, J.; National Institute on Disability and Rehabilitation Research. Measurement of sexual functioning after spinal cord injury: Preferred instruments. J. Spinal Cord Med. 2009, 32, 226–236. [Google Scholar] [CrossRef] [PubMed]
- Morrison, B.F.; White-Gittens, I.; Smith, S.; St John, S.; Bent, R.; Dixon, R. Evaluation of sexual and fertility dysfunction in spinal cord-injured men in Jamaica. Spinal Cord Ser. Cases 2017, 3, 17026. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | Beck Depression Inventory-II Score | p Value | |
|---|---|---|---|
| <14 (Not Depressed) N = 40 | ≥14 (Depressed) N = 17 | ||
| Demographic and lifestyle variables | |||
| Age (years) | 41.5 (21.0–81.0) | 52.0 (20.0–76.0) | 0.5 |
| Education—n (%) | |||
| Primary school | 11 (27.5) | 7 (41.2) | 0.6 |
| High school | 24 (60.0) | 9 (53.0) | |
| University | 5 (12.5) | 1 (5.8) | |
| Marital/partner status—n (%) | |||
| Single | 18 (45.0) | 6 (35.3) | 0.7 |
| Married | 16 (40.0) | 7 (41.3) | |
| Divorced/separeted | 4 (10.0) | 2 (11.7) | |
| Widowed | 2 (5.0) | 2 (11.7) | |
| LTPA (min/week) | 560 (35–1225) | 245 (35–1015) | 0.08 |
| Clinical and injury-related characteristics | |||
| BMI (Kg/m2) | 24.6 (15.2–37.2) | 25.4 (12.3–32.7) | 0.5 |
| Charlson Comorbidity Index score | 2 (0–8) | 3 (0–7) | 0.2 |
| BDI-II score | 6.5 (1–13) | 14 (14–23) | <0.0001 |
| Psychotropic drugs—n (%) | 12 (30.0) | 6 (35.3) | 0.9 |
| Duration of injury (years) | 11.2 (1.5–37.0) | 7.0 (1.1–24.0) | 0.1 |
| Lesion motor completeness—n (%) | |||
| Complete (AIS A+B) | 25 (62.5) | 14 (82.3) | 0.2 |
| Incomplete (AIS C+D) | 15 (37.5) | 3 (17.7) | |
| Level of the lesion—n (%) | |||
| Cervical Spine | 19 (47.5) | 11 (64.7) | 0.3 |
| Thoracic-lumbar Spine | 21 (52.5) | 6 (35.3) | |
| SCIM score | 38.0 (11.0–56.0) | 35.0 (10.0–69.0) | 0.4 |
| Bowel/bladder SCIM sub-score * | 22.0 (0.0–25.0) | 9.0 (0.0–20.0) | 0.001 |
| Pain Intensity (NRS score) | 3.0 (0.0–10.0) | 3.0 (0.0–8.0) | 0.9 |
| Erectile dysfunction—n (%) | 18 (45.0) | 14 (82.3) | 0.02 |
| Blood biometric measures | |||
| Total testosterone (ng/dL) | 404.5 (111.0–713.0) | 268.0 (25.0–694.0) | 0.03 |
| Calculated free testosterone (pg/mL) | 118.1 (27.8–241.1) | 65.0 (2.9–162.9) | 0.02 |
| Vitamin D (ng/mL) | 16.3 (4.1–34.4) | 11.1 (4.4–22.6) | 0.02 |
| Season of evaluation—n (%) | |||
| Autumn/winter | 24 (60.0) | 7 (41.2) | 0.3 |
| Spring/summer | 16 (40.0) | 10 (58.8) | |
| Depression (BDI-II Score ≥14) | ||
|---|---|---|
| OR (95% CI) | p Value | |
| Erectile dysfunction (IIEF-5 score ≤21) | 19.0 (3.1; 203.3) | 0.004 |
| Bowel/bladder SCIM sub-score | 0.84 (0.72; 0.94) | 0.01 |
| Calculated free testosterone (pg/mL) | 0.98 (0.96; 1.0) | 0.07 |
| Vitamin D (ng/mL) | 0.96 (0.82; 1.1) | 0.6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Barbonetti, A.; D’Andrea, S.; Castellini, C.; Totaro, M.; Muselli, M.; Cavallo, F.; Felzani, G.; Necozione, S.; Francavilla, S. Erectile Dysfunction Is the Main Correlate of Depression in Men with Chronic Spinal Cord Injury. J. Clin. Med. 2021, 10, 2090. https://doi.org/10.3390/jcm10102090
Barbonetti A, D’Andrea S, Castellini C, Totaro M, Muselli M, Cavallo F, Felzani G, Necozione S, Francavilla S. Erectile Dysfunction Is the Main Correlate of Depression in Men with Chronic Spinal Cord Injury. Journal of Clinical Medicine. 2021; 10(10):2090. https://doi.org/10.3390/jcm10102090
Chicago/Turabian StyleBarbonetti, Arcangelo, Settimio D’Andrea, Chiara Castellini, Maria Totaro, Mario Muselli, Francesca Cavallo, Giorgio Felzani, Stefano Necozione, and Sandro Francavilla. 2021. "Erectile Dysfunction Is the Main Correlate of Depression in Men with Chronic Spinal Cord Injury" Journal of Clinical Medicine 10, no. 10: 2090. https://doi.org/10.3390/jcm10102090
APA StyleBarbonetti, A., D’Andrea, S., Castellini, C., Totaro, M., Muselli, M., Cavallo, F., Felzani, G., Necozione, S., & Francavilla, S. (2021). Erectile Dysfunction Is the Main Correlate of Depression in Men with Chronic Spinal Cord Injury. Journal of Clinical Medicine, 10(10), 2090. https://doi.org/10.3390/jcm10102090