1. Introduction
Smoking is a strong risk factor for cardiovascular disease, including stroke, and secondhand smoke (SHS) also increases stroke risk [
1]. Many countries and regions across the world have implemented public smoking bans to improve public health, and these seem effective in reducing myocardial infarctions [
2,
3]. However, data on stroke occurrence in this setting are more limited [
3,
4,
5]. Previous data showed that smoking causes subarachnoid hemorrhage (SAH), the incidence of which has steadily declined in Finland along with decreasing smoking prevalence [
6,
7].
A nationwide workplace smoking ban in Finland was enacted in 1995 and extended to cover restaurant workers in 2000. The latest extension came on 1 June 2007, when smoking was prohibited indoors in all public places (a transition time until June 2009 was offered for large restaurants, but only 5% used this opportunity). This extension was associated with reduced rates of smoking, SHS exposure, and myocardial infarction (MI) [
8,
9]. We investigated if there was also a change in stroke occurrence.
2. Methods
All admissions to neurological, neurosurgical, and intensive care wards with acute stroke (ICD-10 codes I60.X-I63.X) as the primary diagnosis between 1 May 2005 and 30 June 2009 were identified from the Care Register for Health Care (CRHC), a mandatory database for all public health care hospital discharges in Finland. All hospitals that provide acute stroke care in mainland Finland were included. Only one annual admission per patient was included. Patients under 18 years of age and patients with concurrent ICD-10 diagnosis codes of rehabilitation (Z50.X) were excluded. Occurrence of stroke admissions was analyzed with count regression. Analysis of the whole study period was adjusted for month to account for seasonality in stroke occurrence. Due to overdispersion, negative binomial modeling was applied. The logarithm of population at risk for each calendar year (total number of 20,923,720 person-years) was used as an offset parameter. Stroke occurrence before and after the restaurant smoking ban within and 7 and 30 days and the whole study period was studied.
Furthermore,
p-values of less than 0.05 were considered significant. IBM SPSS Statistics version 26 (IBM SPSS, Chicago, IL, USA) and SAS version 9.4 (SAS Institute, Cary, NC, USA) were used for statistical analyses. Since stroke occurrence is seasonal and the ban was instituted at the beginning of June, a separate visualization of only May and June admissions was also performed [
10]. Being the days when restaurants, pubs, and nightclubs are most often visited, Friday and Saturday admissions in May and June were also investigated separately.
This study was approved by the Finnish Institute for Health and Welfare (THL, permission no: THL/2245/5.05.00/2019). This was a retrospective register study, and thus, no informed consent was required, and the participants were not contacted.
3. Results
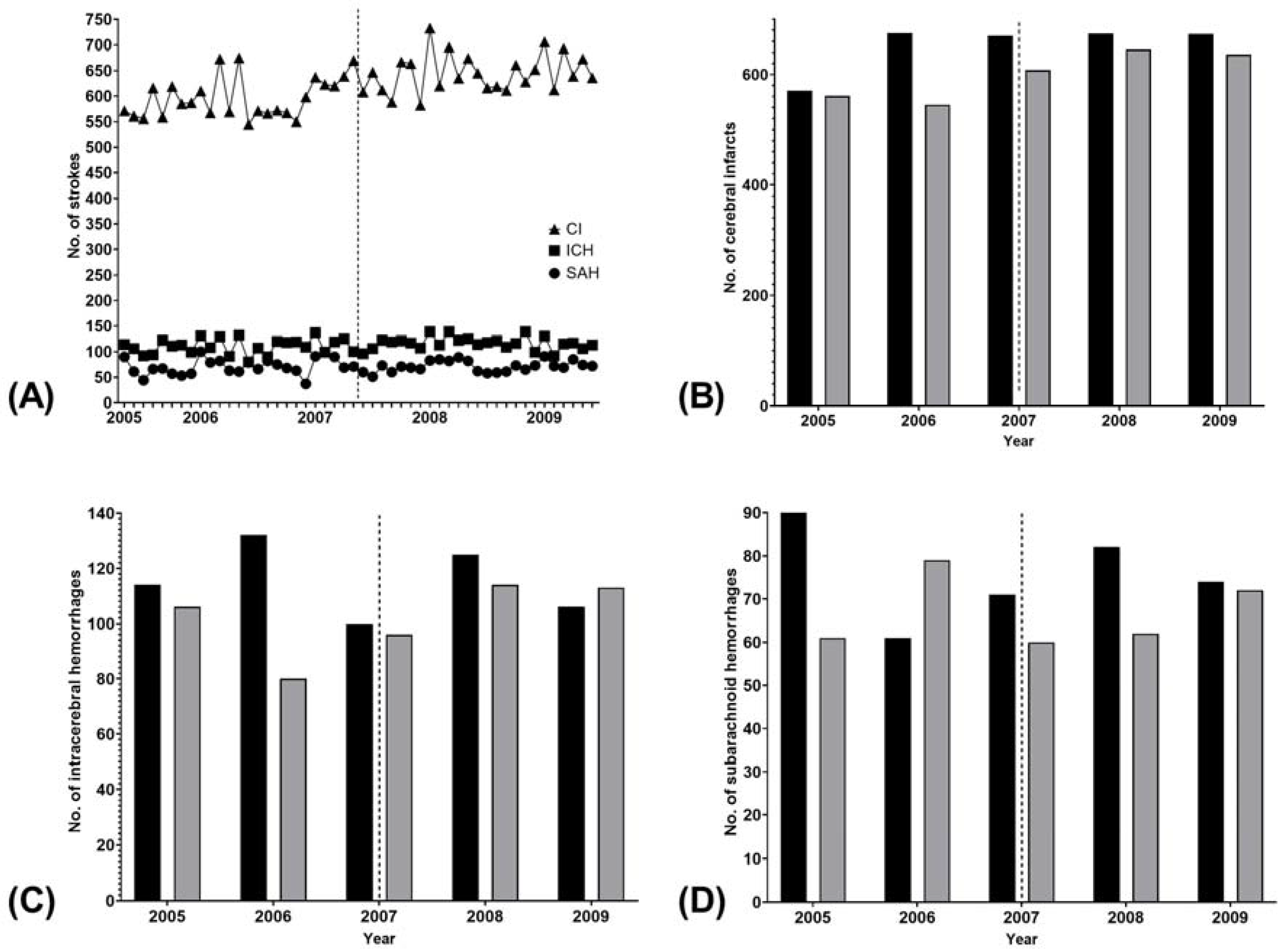
There were 31,023 admissions for cerebral infarction, 5680 admissions for intracerebral hemorrhage (ICH), and 3555 admissions for SAH during the study period (
Figure 1A). There was no difference in stroke occurrence before and after the smoking ban within 7 days (
p = 0.217), 30 days (
p = 0.176), or the whole study period (
p = 0.998) (
Table 1). The results were consistent in all stroke subtypes (
p ≥ 0.102 for all) (
Table 1). The visual inspection revealed a trend for lower numbers of all stroke types in June 2007 compared to May 2007, but this pattern did not differ from the years preceding and following the smoking ban (
Figure 1B–D). Moreover, all strokes occurred at least as frequently in both May and June of 2008 as in the respective months in 2007.
No difference in Friday or Saturday stroke admissions before vs. after the smoking ban was observed within the study period (p = 0.101). Compared to May 2007, June admissions were indeed slightly more numerous on Fridays and Saturdays for all stroke types in June 2007 (data not shown).
4. Discussion
These data show no clear reduction in any type of acute stroke associated with the nationwide restaurant smoking ban enacted in Finland. Previous studies on the subject have usually reported decreased stroke admissions after smoking ban implementations [
3]. On the other hand, although admissions for MI decreased in both New York, United States, and Geneva, Switzerland, there was no change in stroke occurrence in either [
5,
11]. These differences may be related to differences in the study methodologies, background stroke risk and occurrence rates as well as smoking prevalence. Moreover, in Ontario, Canada, the existence and extent of previous smoking bans affected the results [
12]. Finland had already enacted a limited public smoking ban in 1995 and tightened it in 2000 (see above). In comparison, only some areas in Arizona, for example, had a smoking ban of one kind or another in place before the introduction of a statewide ban [
4]. It seems that the effect smoking bans have on stroke occurrence depends on their extent and the environment in which they are enacted.
The restaurant smoking ban in Finland has previously been associated with decreases in hospitalizations and in-hospital mortality for MI [
8]. The fact that this study showed no immediate association between the ban and stroke hospitalizations is probably related to the fact that smoking raises the risk of MI more than it does the risk of stroke. In addition, smoking cessation also lowers the risk of MI more than that of stroke [
13,
14]. Moreover, patients with ischemic stroke and ICH are older than those with MI in Finland and, thus, are unlikely to visit areas covered by the ban as frequently [
8,
10]. However, as SHS has been shown to be an independent risk factor for stroke, reductions in stroke occurrence are also likely to occur in the long term after a widespread reduction in SHS exposure and are by no means excluded by the current results [
1].
Naturally, since this is a retrospective registry study, there are caveats concerning the validity of the data. However, the registry is reliable concerning primary diagnoses, which we used here, and there were no relevant changes in treatment or coding practices during the study period [
15]. Confounding by unmeasured factors such as climate and economic and social factors remains possible and should be considered when comparing the results obtained elsewhere. Lastly, incidence was only estimated roughly because of the unavailability of monthly population size and composition. However, since the size of the population >18 years of age increased by only 2.6% in Finland during the study period, with only a marginal change in the age structure, and since it seems unlikely that there was any meaningful change between May and June 2007, a more exact analysis would probably have yielded similar results. Thus, if the ban would have had a large effect, it should have been observable between these months, although the inter-year variability may have masked a moderate effect.
In conclusion, despite its effect on MI hospitalizations, the nationwide restaurant smoking ban Finland was not associated with any immediately observable effects on stroke occurrence.
Author Contributions
Conceptualization, J.O.T.S. and V.K.; methodology, J.O.T.S. and V.K.; formal analysis, J.O.T.S. and V.K.; investigation J.O.T.S., J.O.R., J.P.P. and V.K.; resources, P.R. and V.K.; data curation, V.K.; writing—original draft preparation, J.O.T.S.; writing—review and editing, J.O.R., J.P.P., P.R. and V.K.; visualization, J.O.T.S.; supervision, P.R. and V.K.; project administration, V.K.; funding acquisition, P.R. and V.K. All authors have read and agreed to the published version of the manuscript.
Funding
The study was supported by the government’s Special Financial Transfer tied to academic research in Health Sciences (Finland), grant funding from the Academy of Finland (#17379), and grant funding of the Finnish Cultural Foundation and the Paulo Foundation. The funding sources had no role in in study design; in the collection, analysis and interpretation of data; in the writing of the report; and in the decision to submit the article for publication.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
This manuscript is based on third-party data. Access to data is regulated by Finnish law and THL. The disclosure of data to third parties without explicit permission from THL is prohibited. Only those fulfilling the requirements established by Finnish law and THL for viewing confidential data can access the data. We confirm that the authors did not have any special access privileges that others would not have. The legal basis for processing personal data is public interest and scientific research (EU General Data Protection Regulation 2016/679 (GDPR), Article 6(1)(e) and Article 9(2)(j); Data Protection Act, Sections 4 and 6).
Conflicts of Interest
Jussi Sipilä has received honoraria (Merck, Pfizer, Sanofi), consultancy fees (Rinnekoti Foundation, Medaffcon), travel grants, and congress sponsorship (Abbvie, Orion Pharma, Merck Serono, Sanquin, Lundbeck, Novartis) and holds shares (Orion Corporation). Jori Ruuskanen has received scientific consultancy fees (Merck, Sandoz), speaker fees (Merck, Biogen Idec, UCB Pharma, Bayer), and travel grants and congress sponsorship (BMS, Sanofi-Genzyme, TEVA, Bayer). Jussi Posti has received speaker fees (Finnish Medical Association); Päivi Rautava declares no conflict of interest; Ville Kytö has received scientific consultancy fees (AstraZeneca), speaker fees (Bayer, Boehringer-Ingelheim, Roche), and travel grants and congress sponsorship (AstraZeneca, Boehringer-Ingelheim, Bayer, Pfizer).
References
- Malek, A.M.; Cushman, M.; Lackland, D.T.; Howard, G.; McClure, L.A. Secondhand Smoke Exposure and Stroke: The Reasons for Geographic and Racial Differences in Stroke (REGARDS) Study. Am. J. Prev. Med. 2015, 49, e89–e97. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, P.N.; Fry, J.S.; Thornton, A.J. Updating the evidence relating smoking bans to incidence of heart disease. Regul. Toxicol. Pharmacol. 2019, 101, 172–186. [Google Scholar] [CrossRef] [PubMed]
- Frazer, K.; Callinan, J.E.; McHugh, J.; van Baarsel, S.; Clarke, A.; Doherty, K.; Kelleher, C. Legislative smoking bans for reducing harms from secondhand smoke exposure, smoking prevalence and tobacco consumption. Cochrane Database Syst. Rev. 2016, 2, CD005992. [Google Scholar] [CrossRef] [PubMed]
- Herman, P.M.; Walsh, M.E. Hospital Admissions for Acute Myocardial Infarction, Angina, Stroke, and Asthma After Implementation of Arizona’s Comprehensive Statewide Smoking Ban. Am. J. Public Health 2011, 101, 491–496. [Google Scholar] [CrossRef] [PubMed]
- Humair, J.P.; Garin, N.; Gerstel, E.; Carballo, S.; Carballo, D.; Keller, P.F.; Guessous, I. Acute respiratory and cardiovascular admissions after a public smoking ban in Geneva, Switzerland. PLoS ONE 2014, 9, e90417. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Korja, M.; Lehto, H.; Juvela, S.; Kaprio, J. Incidence of subarachnoid hemorrhage is decreasing together with decreasing smoking rates. Neurology 2016, 87, 1118–1123. [Google Scholar] [CrossRef] [Green Version]
- Rautalin, I.; Korja, M.; Kaprio, J. Smoking Causes Fatal Subarachnoid Hemorrhage A Case-Control Study of Finnish Twins. Stroke 2020, 51, 3018–3022. [Google Scholar] [CrossRef] [PubMed]
- Sipilä, J.O.; Gunn, J.M.; Kauko, T.; Rautava, P.; Kytö, V. Association of restaurant smoking ban and the incidence of acute myocardial infarction in Finland. BMJ Open 2016, 6, e009320. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reijula, J.P.; Johnsson, T.S.; Kaleva, P.S.; Reijula, K.E. Exposure to tobacco smoke and prevalence of symptoms decreased among Finnish restaurant workers after the smoke-free law. Am. J. Ind. Med. 2012, 55, 37–43. [Google Scholar] [CrossRef] [PubMed]
- Sipilä, J.O.; Ruuskanen, J.O.; Kauko, T.; Rautava, P.; Kytö, V. Seasonality of stroke in Finland. Ann. Med. 2017, 49, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Juster, H.R.; Loomis, B.R.; Hinman, T.M.; Farrelly, M.C.; Hyland, A.; Bauer, U.E.; Birkhead, G.S. Declines in Hospital Admissions for Acute Myocardial Infarction in New York State After Implementation of a Comprehensive Smoking Ban. Am. J. Public Health 2007, 97, 2035–2039. [Google Scholar] [CrossRef] [PubMed]
- Naiman, A.; Glazier, R.H.; Moineddin, R. Association of anti-smoking legislation with rates of hospital admission for cardiovascular and respiratory conditions. CMAJ 2010, 182, 761–767. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Banks, E.; Joshy, G.; Korda, R.J.; Stavreski, B.; Soga, K.; Egger, S.; Day, C.; Clarke, N.E.; Lewington, S.; Lopez, A.D. Tobacco smoking and risk of 36 cardiovascular disease subtypes: Fatal and non-fatal outcomes in a large prospective Australian study. BMC Med. 2019, 17, 128. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, Y.M.; Cho, H.J. Risk of Stroke and Myocardial Infarction after Reduction or Cessation of Cigarette Smoking: A Cohort Study in Korean Men. Stroke 2018, 29, 2432–2438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sund, R. Quality of the Finnish Hospital Discharge Register: A systematic review. Scand J. Public Health 2012, 40, 505–515. [Google Scholar] [CrossRef] [PubMed]
| Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).


 ,
, 



{kind=link}