
Diversity of Acupuncture Point Selections According to the Acupuncture Styles and Their Relations to Theoretical Elements in Traditional Asian Medicine: A Data-Mining-Based Literature Study

 ,
,  and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Document Selection
2.2. Data Preprocessing
2.3. Similarity Analysis between AP Prescriptions
2.3.1. Hierarchical Clustering
2.3.2. Dimensionality Reduction and Visualization
2.3.3. Network Analysis
2.3.4. Permutation Test
2.3.5. Contribution Score Calculation by Random Forest Classifiers
2.4. Software
3. Results
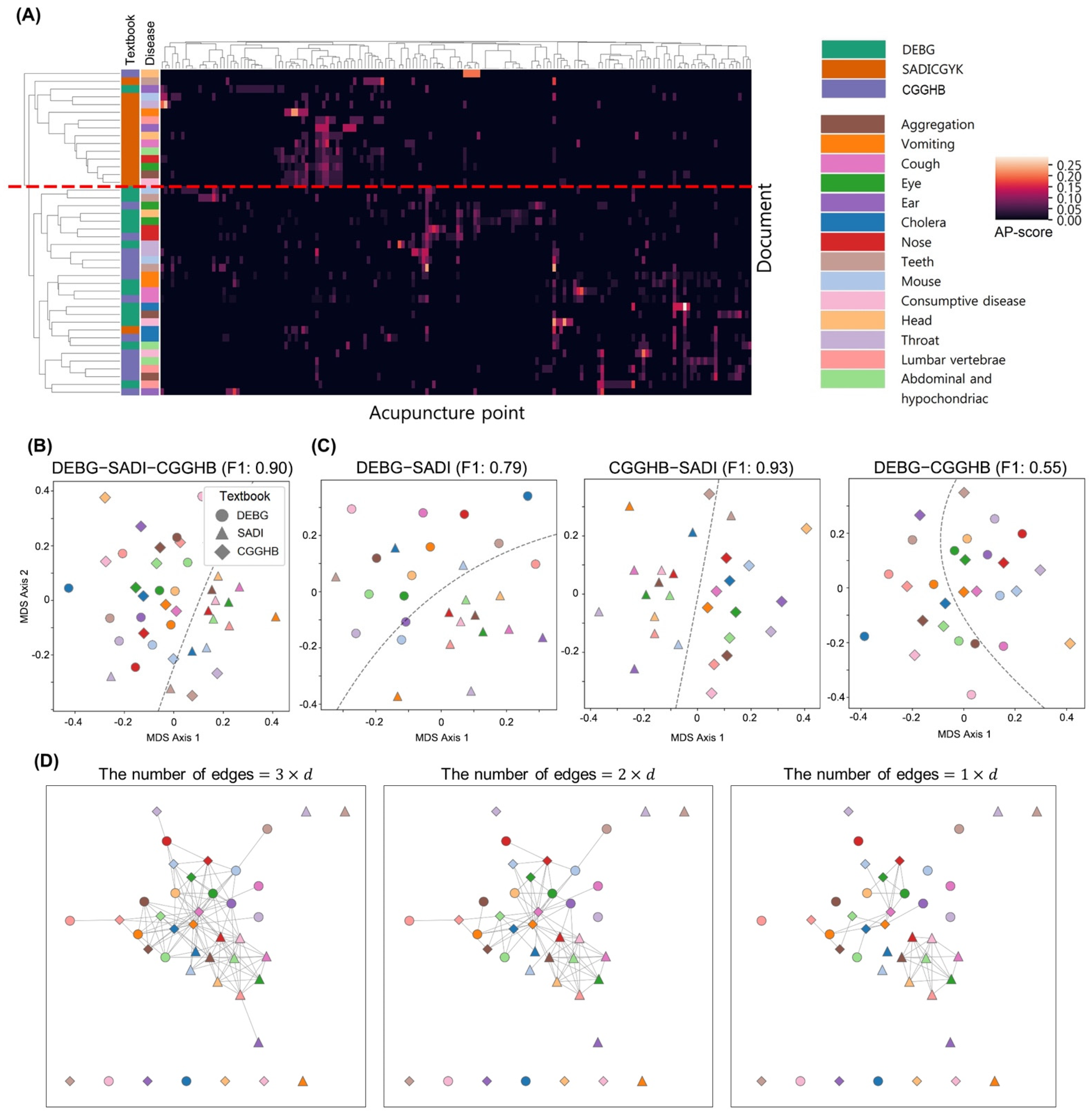
3.1. AP Prescriptions Similarity in DEBG, SADI, and CGGHB
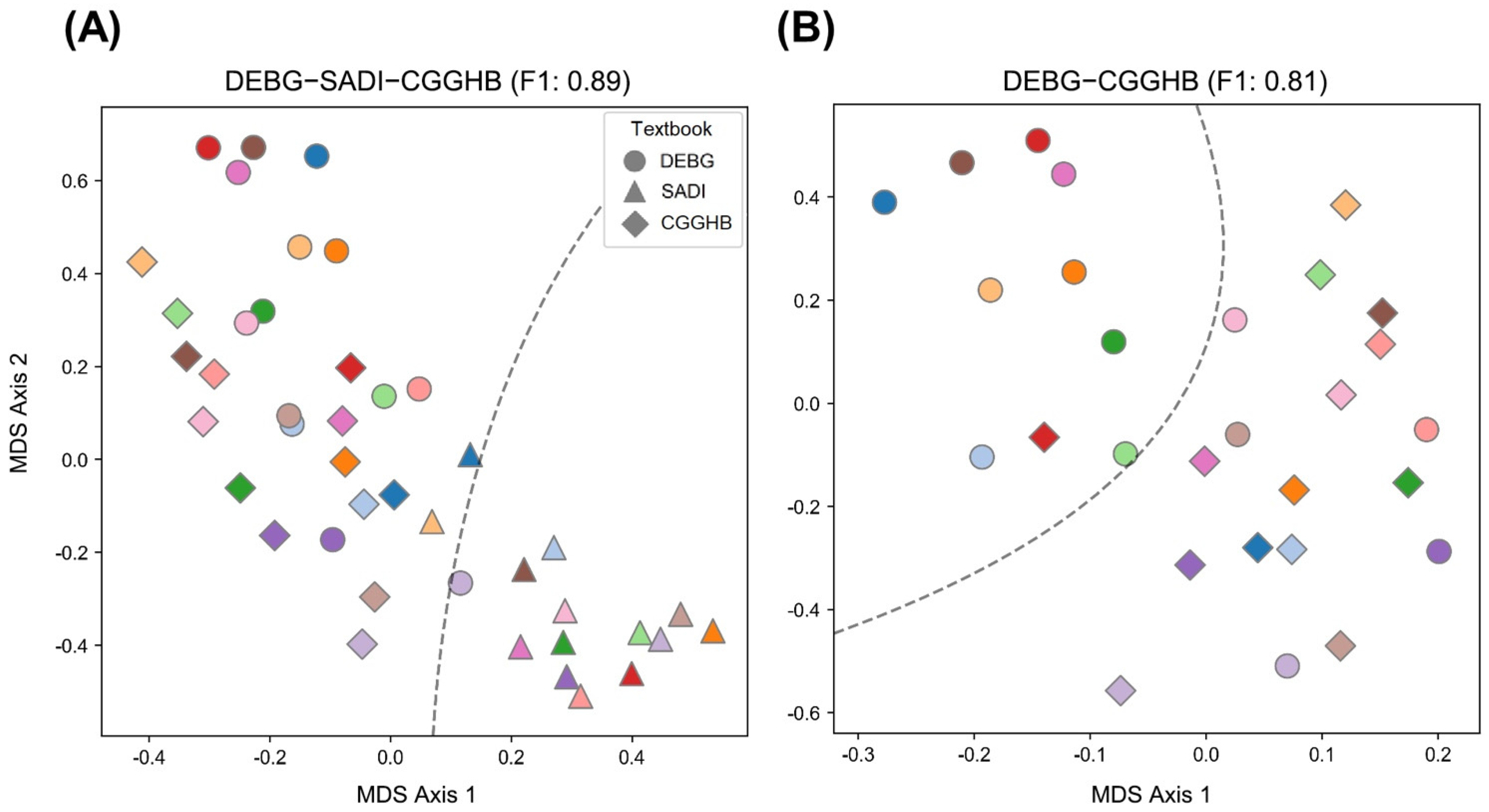
3.2. Quantitative Analysis of Similarity of AP Prescriptions in DEBG, SADI, and CGGHB
3.3. AP Attribute Preference in DEBG, SADI, and CGGHB
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berman, B.M.; Langevin, H.M.; Witt, C.M.; Dubner, R. Acupuncture for Chronic Low Back Pain. N. Engl. J. Med. 2010, 363, 454–461. [Google Scholar] [CrossRef]
- Lim, T.-K.; Ma, Y.; Berger, F.; Litscher, G. Acupuncture and Neural Mechanism in the Management of Low Back Pain—An Update. Medicines 2018, 5, 63. [Google Scholar] [CrossRef]
- Avis, N.E.; Coeytaux, R.R.; Isom, S.; Prevette, K.; Morgan, T. Acupuncture in Menopause (AIM) study: A pragmatic, randomized controlled trial. Menopause 2016, 23, 626–637. [Google Scholar] [CrossRef] [PubMed]
- Chien, T.-J.; Hsu, C.-H.; Liu, C.-Y.; Fang, C.-J. Effect of acupuncture on hot flush and menopause symptoms in breast cancer—A systematic review and meta-analysis. PLoS ONE 2017, 12, e0180918. [Google Scholar] [CrossRef] [PubMed]
- Chavez, L.M.; Huang, S.-S.; Macdonald, I.; Lin, J.-G.; Lee, Y.-C.; Chen, Y.-H. Mechanisms of Acupuncture Therapy in Ischemic Stroke Rehabilitation: A Literature Review of Basic Studies. Int. J. Mol. Sci. 2017, 18, 2270. [Google Scholar] [CrossRef]
- Lee, S.-H.; Lim, S.M. Acupuncture for insomnia after stroke: A systematic review and meta-analysis. BMC Complement. Altern. Med. 2016, 16, 228. [Google Scholar] [CrossRef] [PubMed]
- Fan, A.Y.; Faggert, S. Distribution of licensed acupuncturists and educational institutions in the United States in early 2015. J. Integr. Med. 2018, 16, 1–5. [Google Scholar] [CrossRef]
- Borud, E.K.; Alræk, T.; White, A.; Grimsgaard, S. The Acupuncture Treatment for Postmenopausal Hot Flushes (Acuflash) Study: Traditional Chinese Medicine Diagnoses and Acupuncture Points Used, and Their Relation to the Treatment Response. Acupunct. Med. 2009, 27, 101–108. [Google Scholar] [CrossRef]
- Kwon, S.; Seo, B.-K.; Kim, S. Acupuncture points for treating Parkinson’s disease based on animal studies. Chin. J. Integr. Med. 2016, 22, 723–727. [Google Scholar] [CrossRef]
- Lee, S.-H.; Kim, C.-E.; Lee, I.-S.; Jung, W.-M.; Kim, H.-G.; Jang, H.; Kim, S.-J.; Lee, H.; Park, H.-J.; Chae, Y. Network Analysis of Acupuncture Points Used in the Treatment of Low Back Pain. Evid.-Based Complement. Altern. Med. 2013, 2013, 402180. [Google Scholar] [CrossRef] [PubMed]
- Kalauokalani, D.; Sherman, K.J.; Cherkin, D.C. Acupuncture for chronic low back pain: Diagnosis and treatment patterns among acupuncturists evaluating the same patient. South. Med. J. 2001, 94, 486–492. [Google Scholar] [CrossRef] [PubMed]
- Napadow, V.; Liu, J.; Kaptchuk, T.J. A systematic study of acupuncture practice: Acupoint usage in an outpatient setting in Beijing, China. Complement. Ther. Med. 2004, 12, 209–216. [Google Scholar] [CrossRef] [PubMed]
- Mac Pherson, H.; Thorpe, L.; Thomas, K.; Campbell, M.; Campbell, M. Acupuncture for low back pain: Traditional diagnosis and treatment of 148 patients in a clinical trial. Complement. Ther. Med. 2004, 12, 38–44. [Google Scholar] [CrossRef]
- Lee, Y.-S.; Ryu, Y.; Yoon, D.-E.; Kim, C.-H.; Hong, G.; Hwang, Y.-C.; Chae, Y. Commonality and Specificity of Acupuncture Point Selections. Evid.-Based Complement. Altern. Med. 2020, 2020, 2948292. [Google Scholar] [CrossRef] [PubMed]
- Manheimer, E.; White, A.; Berman, B.; Forys, K.; Ernst, E. Meta-Analysis: Acupuncture for Low Back Pain. Ann. Intern. Med. 2005, 142, 651–663. [Google Scholar] [CrossRef] [PubMed]
- Sherman, K.; Hogeboom, C.; Cherkin, D. How traditional Chinese medicine acupuncturists would diagnose and treat chronic low back pain: Results of a survey of licensed acupuncturists in Washington State. Complement. Ther. Med. 2001, 9, 146–153. [Google Scholar] [CrossRef]
- Ahn, A.C.; Bennani, T.; Freeman, R.; Hamdy, O.; Kaptchuk, T.J. Two Styles of Acupuncture for Treating Painful Diabetic Neuropathy—A Pilot Randomised Control Trial. Acupunct. Med. 2007, 25, 11–17. [Google Scholar] [CrossRef]
- Itoh, K.; Katsumi, Y.; Hirota, S.; Kitakoji, H. Randomised trial of trigger point acupuncture compared with other acupuncture for treatment of chronic neck pain. Complement. Ther. Med. 2007, 15, 172–179. [Google Scholar] [CrossRef] [PubMed]
- Donnellan, C.P.; Shanley, J. Comparison of the effect of two types of acupuncture on quality of life in secondary progressive multiple sclerosis: A preliminary single-blind randomized controlled trial. Clin. Rehabil. 2007, 22, 195–205. [Google Scholar] [CrossRef] [PubMed]
- MacPherson, H.; Altman, D.G.; Hammerschlag, R.; Youping, L.; Taixiang, W.; White, A.D.; Moher, D. Revised STandards for Reporting Interventions in Clinical Trials of Acupuncture (STRICTA): Extending the CONSORT Statement. PLoS Med. 2010, 7, e1000261. [Google Scholar] [CrossRef]
- World Health Organization. WHO International Standard Terminologies on Traditional Medicine in the Western Pacific Region; World Health Organization: Manila, Philippines, 2007. [Google Scholar]
- Yu, S.; Yang, J.; Yang, M.; Gao, Y.; Chen, J.; Ren, Y.; Zhang, L.; Chen, L.; Liang, F.; Hu, Y. Application of Acupoints and Meridians for the Treatment of Primary Dysmenorrhea: A Data Mining-Based Literature Study. Evid.-Based Complement. Altern. Med. 2015, 2015, 752194. [Google Scholar] [CrossRef] [PubMed]
- Lee, T.; Jung, W.-M.; Lee, I.-S.; Lee, Y.-S.; Lee, H.; Park, H.-J.; Kim, N.; Chae, Y. Data Mining of Acupoint Characteristics from the Classical Medical Text: DongUiBoGam of Korean Medicine. Evid.-Based Complement. Altern. Med. 2014, 2014, 329563. [Google Scholar] [CrossRef]
- Mead, A. Review of the Development of Multidimensional Scaling Methods. J. R. Stat. Soc. Ser. D 1992, 41, 27–39. [Google Scholar] [CrossRef]
- Alvim, D.T.; Ferreira, A.S. Inter-expert agreement and similarity analysis of traditional diagnoses and acupuncture prescriptions in textbook- and pragmatic-based practices. Complement. Ther. Clin. Pract. 2018, 30, 38–43. [Google Scholar] [CrossRef]
- Wan, D.W.L.; Wang, Y.; Xue, C.; Wang, L.; Liang, F.; Zheng, Z. Local and distant acupuncture points stimulation for chronic musculoskeletal pain: A systematic review on the comparative effects. Eur. J. Pain 2015, 19, 1232–1247. [Google Scholar] [CrossRef]
- Matsubara, T.; Arai, Y.-C.P.; Shiro, Y.; Shimo, K.; Nishihara, M.; Sato, J.; Ushida, T. Comparative Effects of Acupressure at Local and Distal Acupuncture Points on Pain Conditions and Autonomic Function in Females with Chronic Neck Pain. Evid.-Based Complement. Altern. Med. 2010, 2011, 543291. [Google Scholar] [CrossRef]
- Lu, D.P.; Lu, G.P. A Comparison of the Clinical Effectiveness of Various Acupuncture Points in Reducing Anxiety to Facilitate Hypnotic Induction. Int. J. Clin. Exp. Hypn. 2013, 61, 271–281. [Google Scholar] [CrossRef]
- Oliveira, I.J.D.A.S.; Ferreira, A.D.S. Effects of Diagnostic Errors in Pattern Differentiation and Acupuncture Prescription: A Single-Blinded, Interrater Agreement Study. Evid.-Based Complement. Altern. Med. 2015, 2015, 469675. [Google Scholar] [CrossRef]
- Huang, P.; Shi, J.; Luo, L.; Xi, S.; Yi, W. [Exploration on the treatment of xiaoke in terms of the conception vessel]. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2016, 36, 1309–1310. [Google Scholar]
- Kim, S.; Song, B.-K.; Won, J.-H. Historical Medical Value of Donguibogam. J. Pharmacopunct. 2016, 19, 16–20. [Google Scholar] [CrossRef]
- Sun, Z.; Zhang, J. [Ancient identification and modern categorization of the governor vessel disorders]. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2017, 37, 1077–1080. [Google Scholar]
- Chapple, W. Proposed Catalog of the Neuroanatomy and the Stratified Anatomy for the 361 Acupuncture Points of 14 Channels. J. Acupunct. Meridian Stud. 2013, 6, 270–274. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Mirescu, Ş.C.; Ciobanu, L.; Andreica, V.; Rosioru, C.L. The electrical resistance of acupuncture source points as a relevant factor for inner organ status. Stud. Univ. Babes-Bolyai Biol. 2010, 1, 103–110. [Google Scholar]
- Du, T.; Ren, Y.; Sun, T.; Lai, Z.; Liang, F. [Exploration of action and significance of yuan-source point for clinical diagnosis based on literature metrology]. Zhongguo Zhen Jiu = Chin. Acupunct. Moxibustion 2016, 36, 831–834. [Google Scholar]
- Wang, X.; Liu, B.; Wang, S.; Sui, M. Effects of acupuncture at Shu, Yuan, and Mu acupoints on blood serum uric acid and xanthine oxidase levels in a rat model of gout and hyperuricemia. J. Tradit. Chin. Med. 2017, 37, 841–845. [Google Scholar] [CrossRef]
- Sun, B.-G.; Meng, J.; Xiang, T.; Chen, Z.-X.; Zhang, S.-J. Acupuncture of the Five Shu Acupoints in spleen meridian to lower blood uric acid level. Ann. Palliat. Med. 2014, 3, 22–27. [Google Scholar] [PubMed]
- Jeong, Y.J.; Kwon, H.J.; Park, Y.S.; Kwon, O.C.; Shin, I.H.; Park, S.H. Treatment of Lymphedema with Saam Acupuncture in Patients with Breast Cancer: A Pilot Study. Med. Acupunct. 2015, 27, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Kim, S. A Modern Clinical Approach of the Traditional Korean Saam Acupuncture. Evid.-Based Complement. Altern. Med. 2015, 2015, 703439. [Google Scholar] [CrossRef]
- Ahn, C.-B.; Jang, K.-J.; Yoon, H.-M.; Kim, C.-H.; Min, Y.-K.; Song, C.-H.; Lee, J.-C. A Study of the Sa-Ahm Five Element Acupuncture Theory. J. Acupunct. Meridian Stud. 2009, 2, 309–320. [Google Scholar] [CrossRef][Green Version]
- Ahn, C.-B.; Jang, K.-J.; Yoon, H.-M.; Kim, C.-H.; Min, Y.-K.; Song, C.-H.; Lee, J.-C. Sa-Ahm Five Element Acupuncture. J. Acupunct. Meridian Stud. 2010, 3, 203–213. [Google Scholar] [CrossRef]
- Wang, Q.; Deng, H.; Cheng, K.; Huang, Z.; Yin, X.; Zhou, Y.; Yang, Y.; Shen, W.; Zhao, L.; Shen, X. Manual acupuncture for the infertile female with polycystic ovary syndrome (PCOS): Study protocol for a randomized sham-controlled trial. Trials 2019, 20, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.-H.; Yoon, D.-E.; Lee, Y.-S.; Jung, W.-M.; Kim, J.-H.; Chae, Y. Revealing Associations between Diagnosis Patterns and Acupoint Prescriptions Using Medical Data Extracted from Case Reports. J. Clin. Med. 2019, 8, 1663. [Google Scholar] [CrossRef]
- Hwang, Y.-C.; Lee, I.-S.; Ryu, Y.; Lee, Y.-S.; Chae, Y. Identification of Acupoint Indication from Reverse Inference: Data Mining of Randomized Controlled Clinical Trials. J. Clin. Med. 2020, 9, 3027. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Textbooks | Type | Observed Similarity | Expected Similarity | Empirical p-Value |
|---|---|---|---|---|
| DEBG, SADI, and CGGHB | Same textbook | 0.3558 | 0.3751 | <10−8 *** |
| Same disease | 0.3628 | 0.3751 | 0.012 * | |
| DEBG and SADI | Same textbook | 0.3541 | 0.3722 | 3.2 × 10−7 *** |
| Same disease | 0.3832 | 0.3722 | 0.89 | |
| SADI and CGGHB | Same textbook | 0.3449 | 0.3680 | <10−8 *** |
| Same disease | 0.3789 | 0.3680 | 0.85 | |
| DEBG and CGGHB | Same textbook | 0.3685 | 0.3711 | 0.066 # |
| Same disease | 0.3264 | 0.3711 | 1.8 × 10−7 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jang, D.-Y.; Oh, K.-C.; Jung, E.-S.; Cho, S.-J.; Lee, J.-Y.; Lee, Y.-J.; Kim, C.-E.; Yang, I.-J. Diversity of Acupuncture Point Selections According to the Acupuncture Styles and Their Relations to Theoretical Elements in Traditional Asian Medicine: A Data-Mining-Based Literature Study. J. Clin. Med. 2021, 10, 2059. https://doi.org/10.3390/jcm10102059
Jang D-Y, Oh K-C, Jung E-S, Cho S-J, Lee J-Y, Lee Y-J, Kim C-E, Yang I-J. Diversity of Acupuncture Point Selections According to the Acupuncture Styles and Their Relations to Theoretical Elements in Traditional Asian Medicine: A Data-Mining-Based Literature Study. Journal of Clinical Medicine. 2021; 10(10):2059. https://doi.org/10.3390/jcm10102059
Chicago/Turabian StyleJang, Dong-Yeop, Ki-Chang Oh, Eun-Seo Jung, Soo-Jin Cho, Ji-Yun Lee, Yeon-Jae Lee, Chang-Eop Kim, and In-Jun Yang. 2021. "Diversity of Acupuncture Point Selections According to the Acupuncture Styles and Their Relations to Theoretical Elements in Traditional Asian Medicine: A Data-Mining-Based Literature Study" Journal of Clinical Medicine 10, no. 10: 2059. https://doi.org/10.3390/jcm10102059
APA StyleJang, D.-Y., Oh, K.-C., Jung, E.-S., Cho, S.-J., Lee, J.-Y., Lee, Y.-J., Kim, C.-E., & Yang, I.-J. (2021). Diversity of Acupuncture Point Selections According to the Acupuncture Styles and Their Relations to Theoretical Elements in Traditional Asian Medicine: A Data-Mining-Based Literature Study. Journal of Clinical Medicine, 10(10), 2059. https://doi.org/10.3390/jcm10102059