
Modalities of Left Ventricle Decompression during VA-ECMO Therapy

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Mechanisms of LV Distention
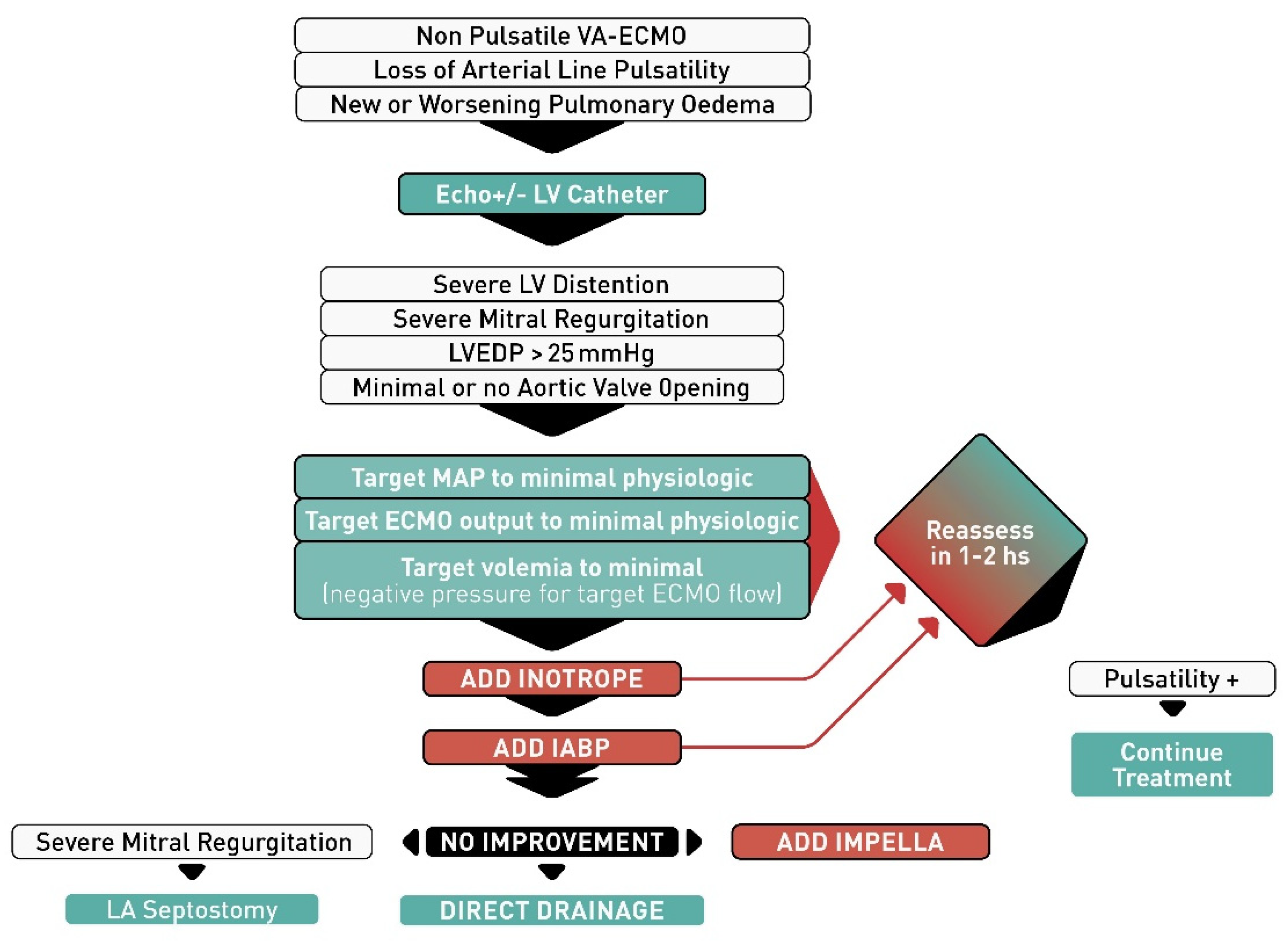
3. Monitoring and How to Recognize LV Distention and Pulmonary Congestion in Patients with VA-ECMO
4. Therapeutic Strategies for LV Distention
4.1. Inotropic Support and Volemic Status Optimization
4.2. Intra-Aortic Balloon Pump
4.3. Balloon Atrial Septostomy
4.4. Impella
4.5. Surgical Decompression Cannula
4.6. Percutaneous Decompression Cannula
5. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Wayangankar, S.A.; Bangalore, S.; McCoy, L.A.; Jneid, H.; Latif, F.; Karrowni, W.; Charitakis, K.; Feldman, D.N.; Dakik, H.A.; Mauri, L.; et al. Temporal Trends and Outcomes of Patients Undergoing Percutaneous Coronary Interventions for Cardiogenic Shock in the Setting of Acute Myocardial Infarction: A Report from the CathPCI Registry. JACC Cardiovasc. Interv. 2016, 9, 341–351. [Google Scholar] [CrossRef]
- Bartlett, R.H.; Gazzaniga, A.B.; Fong, S.W.; Jefferies, M.R.; Roohk, H.V.; Haidu, N. Extracorporeal membrane oxygenator support for cardiopulmonary failure. Experience in 28 cases. J. Thorac. Cardiovasc. Surg. 1977, 73, 375–386. [Google Scholar] [CrossRef]
- Martin, G.B.; Rivers, E.P.; Paradis, N.A.; Goetting, M.G.; Morris, D.C.; Nowak, R.M. Emergency department cardiopulmonary bypass in the treatment of human cardiac arrest. Chest 1998, 113, 743–751. [Google Scholar] [CrossRef]
- Martin, G.R.; Short, B.L. Doppler echocardiographic evaluation of cardiac performance in infants on prolonged extracorporeal membrane oxygenation. Am. J. Cardiol. 1988, 62, 929–934. [Google Scholar] [CrossRef]
- Bavaria, J.E.; Ratcliffe, M.B.; Gupta, K.B.; Wenger, R.K.; Bogen, D.K.; Edmunds, L.H., Jr. Changes in left ventricular systolic wall stress during biventricular circulatory assistance. Ann. Thorac. Surg. 1988, 45, 526–532. [Google Scholar] [CrossRef]
- Burkhoff, D.; Sayer, G.; Doshi, D.; Uriel, N. Hemodynamics of mechanical circulatory support. J. Am. Coll. Cardiol. 2015, 66, 2663–2674. [Google Scholar] [CrossRef] [PubMed]
- Donker, D.W.; Brodie, D.; Henriques, J.P.S.; Broomé, M. Left ventricular unloading during veno-arterial ECMO: A simulation study. ASAIO J. 2019, 65, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Roumy, A.; Liaudet, L.; Rusca, M.; Marcucci, C.; Kirsch, M. Pulmonary complications associated with veno-arterial extra-corporeal membrane oxygenation: A comprehensive review. Crit. Care 2020, 24, 212. [Google Scholar] [CrossRef]
- Truby, L.K.; Takeda, K.; Mauro, C.; Yuzefpolskaya, M.; Garan, A.R.; Kirtane, A.J.; Topkara, V.K.; Abrams, D.; Brodie, D.; Colombo, P.C.; et al. Incidence and Implications of Left Ventricular Distention during Venoarterial Extracorporeal Membrane Oxygenation Support. ASAIO J. 2017, 63, 257–265. [Google Scholar] [CrossRef] [PubMed]
- Kapur, N.K.; Zisa, D.C. Veno-arterial extracorporeal membrane oxygenation (VA-ECMO) fails to solve the haemodynamic support equation in cardiogenic shock. EuroIntervention 2016, 11, 1337–1339. [Google Scholar] [CrossRef] [PubMed]
- Rupprecht, L.; Florchinger, B.; Schopka, S.; Schmid, C.; Philipp, A.; Lunz, D.; Muller, T.; Camboni, D. Cardiac decompression on extracorporeal life support: A review and discussion of the literature. ASAIO J. 2013, 59, 547–553. [Google Scholar] [CrossRef] [PubMed]
- Bréchot, N.; Demondion, P.; Santi, F.; Lebreton, G.; Pham, T.; Dalakidis, A.; Gambotti, L.; Luyt, C.E.; Schmidt, M.; Hekimian, G.; et al. Intra-aortic balloon pump protects against hydrostatic pulmonary oedema during peripheral venoarterial-extracorporeal membrane oxygenation. Eur. Heart J. Acute Cardiovasc. Care 2018, 7, 62–69. [Google Scholar] [CrossRef]
- Petroni, T.; Harrois, A.; Amour, J.; Lebreton, G.; Brechot, N.; Tanaka, S.; Luyt, C.E.; Trouillet, J.L.; Chastre, J.; Leprince, P.; et al. Intra-aortic balloon pump effects on macrocirculation and microcirculation in cardiogenic shock patients supported by venoarterial extracorporeal membrane oxygenation*. Crit. Care Med. 2014, 42, 2075–2082. [Google Scholar] [CrossRef]
- Madershahian, N.; Wippermann, J.; Liakopoulos, O.; Wittwer, T.; Kuhn, E.; Er, F.; Hoppe, U.; Wahlers, T. The acute effect of IABP-induced pulsatility on coronary vascular resistance and graft flow in critical ill patients during ECMO. J. Cardiovasc. Surg. 2011, 52, 411–418. [Google Scholar]
- Samadi, B.; Nguyen, D.; Rudham, S.; Barnett, Y. Spinal Cord Infarct during Concomitant Circulatory Support with Intra-Aortic Balloon Pump and Veno-Arterial Extracorporeal Membrane Oxygenation. Crit. Care Med. 2016, 44, e101–e105. [Google Scholar] [CrossRef] [PubMed]
- Belohlavek, J.; Mlcek, M.; Huptych, M.; Svoboda, T.; Havranek, S.; Ost’adal, P.; Boucek, T.; Kovarnik, T.; Mlejnsky, F.; Mrazek, V.; et al. Coronary versus carotid blood flow and coronary perfusion pressure in a pig model of prolonged cardiac arrest treated by different modes of venoarterial ECMO and intraaortic balloon counterpulsation. Crit. Care 2012, 16, R50. [Google Scholar] [CrossRef]
- Yang, F.; Jia, Z.; Xing, J.; Wang, Z.; Liu, Y.; Hao, X.; Jiang, C.J.; Wang, H.; Jia, M.; Hou, X.T. Effects of intra-aortic balloon pump on cerebral blood flow during peripheral venoarterial extracorporeal membrane oxygenation support. J. Transl. Med. 2014, 12, 106. [Google Scholar] [CrossRef] [PubMed]
- Ro, S.K.; Kim, J.B.; Jung, S.H.; Choo, S.J.; Chung, C.H.; Lee, J.W. Extracorporeal life support for cardiogenic shock: Influence of concomitant intra-aortic balloon counterpulsation. Eur. J. Cardiothorac. Surg. 2014, 46, 186–192. [Google Scholar] [CrossRef] [PubMed]
- Rastan, A.J.; Dege, A.; Mohr, M.; Doll, N.; Falk, V.; Walther, T.; Mohr, F.W. Early and late outcomes of 517 consecutive adult patients treated with extracorporeal membrane oxygenation for refractory postcardiotomy cardiogenic shock. J. Thorac. Cardiovasc. Surg. 2010, 139, 302–311.e1. [Google Scholar] [CrossRef]
- Doll, N.; Kiaii, B.; Borger, M.; Bucerius, J.; Kramer, K.; Schmitt, D.V.; Walther, T.; Mohr, F.W. Five-year results of 219 consecutive patients treated with extracorporeal membrane oxygenation for refractory postoperative cardiogenic shock. Ann. Thorac. Surg. 2004, 77, 151–157. [Google Scholar] [CrossRef]
- Cheng, R.; Hachamovitch, R.; Makkar, R.; Ramzy, D.; Moriguchi, J.D.; Arabia, F.A.; Esmailian, F.; Azarbal, B. Lack of Survival Benefit Found With Use of Intraaortic Balloon Pump in Extracorporeal Membrane Oxygenation: A Pooled Experience of 1517 Patients. J. Invasive Cardiol. 2015, 27, 453–458. [Google Scholar]
- Russo, J.J.; Aleksova, N.; Pitcher, I.; Couture, E.; Parlow, S.; Faraz, M.; Visintini, S.; Simard, T.; Di Santo, P.; Mathew, R.; et al. Left Ventricular Unloading During Extracorporeal Membrane Oxygenation in Patients With Cardiogenic Shock. J. Am. Coll. Cardiol. 2019, 73, 654–662. [Google Scholar] [CrossRef]
- Kowalewski, M.; Malvindi, P.G.; Zielinski, K.; Martucci, G.; Slomka, A.; Suwalski, P.; Lorusso, R.; Meani, P.; Arcadipane, A.; Pilato, M.; et al. Left Ventricle Unloading with Veno-Arterial Extracorporeal Membrane Oxygenation for Cardiogenic Shock. Systematic Review and Meta-Analysis. J. Clin. Med. 2020, 9, 1039. [Google Scholar] [CrossRef]
- Al-Fares, A.A.; Randhawa, V.K.; Englesakis, M.; McDonald, M.A.; Nagpal, A.D.; Estep, J.D.; Soltesz, E.G.; Fan, E. Optimal strategy and timing of left ventricular venting during veno-arterial extracorporeal life support for adults in cardiogenic shock: A systematic review and meta-analysis. Circ. Heart Fail. 2019, 12, e006486. [Google Scholar] [CrossRef]
- Baruteau, A.E.; Barnetche, T.; Morin, L.; Jalal, Z.; Boscamp, N.S.; Le Bret, E.; Thambo, J.B.; Vincent, J.A.; Fraisse, A.; Torres, A.J. Percutaneous balloon atrial septostomy on top of venoarterial extracorporeal membrane oxygenation results in safe and effective left heart decompression. Eur. Heart J. Acute Cardiovasc. Care. 2018, 7, 70–79. [Google Scholar] [CrossRef] [PubMed]
- Alhussein, M.; Osten, M.; Horlick, E.; Ross, H.; Fan, E.; Rao, V.; Billia, F. Percutaneous left atrial decompression in adults with refractory cardiogenic shock supported with veno-arterial extracorporeal membrane oxygenation. J. Card. Surg. 2017, 32, 396–401. [Google Scholar] [CrossRef] [PubMed]
- Eastaugh, L.J.; Thiagarajan, R.R.; Darst, J.R.; McElhinney, D.B.; Lock, J.E.; Marshall, A.C. Percutaneous left atrial decompression in patients supported with extracorporeal membrane oxygenation for cardiac disease. Pediatric Crit. Care Med. 2015, 16, 59–65. [Google Scholar] [CrossRef]
- Seib, P.M.; Faulkner, S.C.; Erickson, C.C.; Van Devanter, S.H.; Harrell, J.E.; Fasules, J.W.; Frazier, E.A.; Morrow, W.R. Blade and balloon atrial septostomy for left heart decompression in patients with severe ventricular dysfunction on extracorporeal membrane oxygenation. Catheter Cardiovasc. Interv. 1999, 46, 179–186. [Google Scholar] [CrossRef]
- Cheung, M.M.; Goldman, A.P.; Shekerdemian, L.S.; Brown, K.L.; Cohen, G.A.; Redington, A.N. Percutaneous left ventricular "vent" insertion for left heart decompression during extracorporeal membrane oxygenation. Pediatric Crit. Care Med. 2003, 4, 447–449. [Google Scholar] [CrossRef]
- Kotani, Y.; Chetan, D.; Rodrigues, W.; Sivarajan, V.B.; Gruenwald, C.; Guerguerian, A.M.; Van Arsdell, G.S.; Honjo, O. Left atrial decompression during venoarterial extracorporeal membrane oxygenation for left ventricular failure in children: Current strategy and clinical outcomes. Artif. Organs 2013, 37, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Haynes, S.; Kerber, R.E.; Johnson, F.L.; Lynch, W.R.; Divekar, A. Left heart decompression by atrial stenting during extracorporeal membrane oxygenation. Int. J. Artif. Organs 2009, 32, 240–242. [Google Scholar] [CrossRef] [PubMed]
- Veeram Reddy, S.R.; Guleserian, K.J.; Nugent, A.W. Transcatheter removal of atrial septal stent placed to decompress left atrium with VA ECMO. Catheter. Cardiovasc. Interv. 2015, 85, 1021–1025. [Google Scholar] [CrossRef] [PubMed]
- Colombo, T.; Garatti, A.; Bruschi, G.; Lanfranconi, M.; Russo, C.; Milazzo, F.; Catena, E.; Frigerio, M.; Vitali, E. First successful bridge to recovery with the Impella Recover 100 left ventricular assist device for fulminant acute myocarditis. Ital. Heart J. 2003, 4, 642–645. [Google Scholar]
- Lim, H.S. The Effect of Impella CP on Cardiopulmonary Physiology during Venoarterial Extracorporeal Membrane Oxygenation Support. Artif. Organs 2017, 41, 1109–1112. [Google Scholar] [CrossRef] [PubMed]
- Eliet, J.; Gaudard, P.; Zeroual, N.; Rouviere, P.; Albat, B.; Mourad, M.; Colson, P.H. Effect of Impella During Veno-Arterial Extracorporeal Membrane Oxygenation on Pulmonary Artery Flow as Assessed by End-Tidal Carbon Dioxide. ASAIO J. 2018, 64, 502–507. [Google Scholar] [CrossRef]
- Karatolios, K.; Chatzis, G.; Markus, B.; Luesebrink, U.; Richter, A.; Schieffer, B. Biventricular unloading in patients with refractory cardiogenic shock. Int. J. Cardiol. 2016, 222, 247–252. [Google Scholar] [CrossRef]
- Pappalardo, F.; Schulte, C.; Pieri, M.; Schrage, B.; Contri, R.; Soeffker, G.; Greco, T.; Lembo, R.; Mullerleile, K.; Colombo, A.; et al. Concomitant implantation of Impella(R) on top of veno-arterial extracorporeal membrane oxygenation may improve survival of patients with cardiogenic shock. Eur. J. Heart Fail. 2017, 19, 404–412. [Google Scholar] [CrossRef] [PubMed]
- Schrage, B.; Burkhoff, D.; Rubsamen, N.; Becher, P.M.; Schwarzl, M.; Bernhardt, A.; Grahn, H.; Lubos, E.; Soffker, G.; Clemmensen, P.; et al. Unloading of the Left Ventricle During Venoarterial Extracorporeal Membrane Oxygenation Therapy in Cardiogenic Shock. JACC Heart Fail. 2018, 6, 1035–1043. [Google Scholar] [CrossRef]
- Schrage, B.; Becher, P.M.; Bernhardt, A.; Bezerra, H.; Blankenberg, S.; Brunner, S.; Colson, P.; Cudemus Deseda, G.; Dabboura, S.; Eckner, D.; et al. Left Ventricular Unloading Is Associated With Lower Mortality in Patients With Cardiogenic Shock Treated With Venoarterial Extracorporeal Membrane Oxygenation: Results from an International, Multicenter Cohort Study. Circulation 2020, 142, 2095–2106. [Google Scholar] [CrossRef]
- Hlavacek, A.M.; Atz, A.M.; Bradley, S.M.; Bandisode, V.M. Left atrial decompression by percutaneous cannula placement while on extracorporeal membrane oxygenation. J. Thorac. Cardiovasc. Surg. 2005, 130, 595–596. [Google Scholar] [CrossRef]
- Yamamoto, M.; Oshima, Y.; Matsuhisa, H.; Higuma, T.; Iwaki, R.; Matsushima, S.; Murakami, Y. Left Atrial Decompression by Minithoracotomy during Extracorporeal Life Support. Ann. Thorac. Surg. 2019, 107, e227–e228. [Google Scholar] [CrossRef] [PubMed]
- Rao, P.; Mosier, J.; Malo, J.; Dotson, V.; Mogan, C.; Smith, R.; Keller, R.; Slepian, M.; Khalpey, Z. Peripheral VA-ECMO with direct biventricular decompression for refractory cardiogenic shock. Perfusion 2018, 33, 493–495. [Google Scholar] [CrossRef] [PubMed]
- Guirgis, M.; Kumar, K.; Menkis, A.H.; Freed, D.H. Minimally invasive left-heart decompression during venoarterial extracorporeal membrane oxygenation: An alternative to a percutaneous approach. Interact Cardiovasc. Thorac. Surg. 2010, 10, 672–674. [Google Scholar] [CrossRef]
- Fumagalli, R.; Bombino, M.; Borelli, M.; Rossi, F.; Colombo, V.; Osculati, G.; Ferrazzi, P.; Pesenti, A.; Gattinoni, L. Percutaneous bridge to heart transplantation by venoarterial ECMO and transaortic left ventricular venting. Int. J. Artif. Organs 2004, 27, 410–413. [Google Scholar] [CrossRef] [PubMed]
- Barbone, A.; Malvindi, P.G.; Ferrara, P.; Tarelli, G. Left ventricle unloading by percutaneous pigtail during extracorporeal membrane oxygenation. Interact Cardiovasc. Thorac. Surg. 2011, 13, 293–295. [Google Scholar] [CrossRef]
- Tepper, S.; Masood, M.F.; Baltazar Garcia, M.; Pisani, M.; Ewald, G.A.; Lasala, J.M.; Bach, R.G.; Singh, J.; Balsara, K.R.; Itoh, A. Left Ventricular Unloading by Impella Device Versus Surgical Vent During Extracorporeal Life Support. Ann. Thorac. Surg. 2017, 104, 861–867. [Google Scholar] [CrossRef]
- Sandrio, S.; Springer, W.; Karck, M.; Gorenflo, M.; Weymann, A.; Ruhparwar, A.; Loukanov, T. Extracorporeal life support with an integrated left ventricular vent in children with a low cardiac output. Cardiol. Young 2014, 24, 654–660. [Google Scholar] [CrossRef]
- Weymann, A.; Schmack, B.; Sabashnikov, A.; Bowles, C.T.; Raake, P.; Arif, R.; Verch, M.; Tochertermann, U.; Roggenbach, J.; Popov, A.F.; et al. Central extracorporeal life support with left ventricular decompression for the treatment of refractory cardiogenic shock and lung failure. J. Cardiothorac. Surg. 2014, 9, 60. [Google Scholar] [CrossRef]
- Na, S.J.; Yang, J.H.; Yang, J.H.; Sung, K.; Cho, J.O.; Hahn, J.Y.; Jeon, E.S.; Cho, Y.H. Left heart decompression at venoarterial extracorporeal membrane oxygenation initiation in cardiogenic shock: Prophylactic versus therapeutic strategy. J. Thorac. Dis. 2019, 11, 3746–3756. [Google Scholar] [CrossRef]
- Meani, P.; Natour, E.; Pappalardo, F.; Bidar, E.; Makhoul, M.; Raffa, G.; Heuts, S.; Gelsomino, S.; Lozekoot, P.; Johnson, D.; et al. Left ventricle unloading in veno-arterial ECMO support: Literature review for an unanswered dilemma. Eur. J. Heart Fail. 2017, 19 (Suppl. 2), 64–66. [Google Scholar]
- Avalli, L.; Maggioni, E.; Sangalli, F.; Favini, G.; Formica, F.; Fumagalli, R. Percutaneous left-heart decompression during extracorporeal membrane oxygenation: An alternative to surgical and transeptal venting in adult patients. ASAIO J. 2011, 57, 38–40. [Google Scholar] [CrossRef] [PubMed]
- Meani, P.; Gelsomino, S.; Natour, E.; Johnson, D.M.; Brunner La Rocca, H.P.; Pappalardo, F.; Bidar, E.; Makhoul, M.; Raffa, G.; Heuts, S.; et al. Modalities and Effects of Left Ventricle Unloading on Extracorporeal Life Support: A Review of the Current Literature. Eur. J. Heart Fail. 2017, 19 (Suppl. 2), 84–91. [Google Scholar] [CrossRef] [PubMed]
- Donker, D.W.; Brodie, D.; Henriques, J.P.S.; Broome, M. Left ventricular unloading during veno-arterial ECMO: A review of percutaneous and surgical unloading interventions. Perfusion 2019, 34, 98–105. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Parameters | Consequences |
|---|---|
| LV Preload | ↓ |
| LV Afterload | ↑ |
| LV End-Diastolic Volume and Pressure | ↑ |
| Myocardial Oxygen Consumption | ↑ |
| LV Stroke Volume | ↓ |
| Modality | Advantages | Disadvantages | |
|---|---|---|---|
| Passive LV Unloading | Inotropes | Simple, cheap, first gesture, no “instrumentation” | ↑ Myocardial O2 consumption, ↑ risk or arrhythmias, discrete effect on venting |
| IABP | Familiarity and simplicity of its use, ease and bedside insertion, low complication rate, enhances coronary circulation | Partial unload, limb ischemia, requires regular rhythm, contraindicated in aortic regurgitation and aneurysm | |
| Atrial Septostomy | Aspiration of blood through the RA-LA, if severe mitral regurgitation direct unloading of the LV | Risk of perforation/damage of neighbouring structures, stenting malposition, nephrotoxic contrast use, requires “resolution” after patient improvement | |
| Active LV Unloading | Impella | Direct unload, trigger not required, further enhances systemic blood flow | ↑ Risk of hemolysis, bleeding, and thrombosis, limb ischemia, contraindicated in aortic regurgitation and aneurysm, Impella 5.0 requires surgical insertion, |
| Surgical decompression cannula | Direct unload | Insertion technique complications, if catheter placed in pulmonary artery lung ischemia may occur. Surgical approach requires sternotomy or mini-thoracotomy | |
| Percutaneous decompression cannula | Direct unload | Insertion technique complications |
| Study | Year | Indications | No. Patients ECMO | No. Patients ECMO + Unload | Weaning ECMO (%) | Weaning ECMO + Unload (%) | Mortality ECMO (%) | Mortality ECMO + Unload (%) | Reference |
|---|---|---|---|---|---|---|---|---|---|
| IABP | |||||||||
| Aso et al. | 2016 | Any CS | 1046 | 604 | 685 (65.5) | 505 (83.6) | 650 (62.1) | 287 (47.5) | doi:10.1097/ccm.0000000000001828 |
| Lin et al. | 2016 | Any CS | 227 | 302 | NR | NR | 110 (48.5) | 144 (47.7) | doi:10.1038/srep23838 |
| Bréchot et al. | 2018 | Any CS | 155 | 104 | NR | NR | 92 (59.4) | 45 (43.3) | doi:10.1177/2048872617711169 |
| Tepper et al. | 2018 | Any CS | 30 | 30 | 16 (53) | 20 (64) | 22 (73) | 15 (50) | doi:10.1097/MAT.0000000000000788 |
| Doll et al. | 2004 | Post-cardiotomy shock | 75 | 144 | 32 (42.6) | 101 (70) | 62 (82.6) | 105 (72.9) | doi:10.1016/s0003-4975(03)01329-8 |
| Wang et al. | 2013 | Post-cardiotomy shock | 46 | 41 | NR | NR | 31 (67.4) | 13 (31.7) | doi:10.1371/journal.pone.0063924 |
| Impella | |||||||||
| Pappalardo et al. | 2017 | Any CS | 42 | 21 | 16 (28) | 10 (48) | 21 (74) | 10 (48) | doi:10.1002/ejhf.668 |
| Patel et al. | 2018 | Any CS | 36 | 30 | 16 (44) | 21 (70) | 28 (78) | 17 (57) | doi:10.1097/mat.0000000000000767 |
| Fiedler et al. | 2018 | Any CS | 47 | 12 | NR | NR | 25 (53.2) | 5 (41.6) | doi:10.1053/j.jvca.2018.05.019 |
| LV Cannula | |||||||||
| Schmack et al. | 2017 | Any CS | 28 | 20 | NR | NR | 21 (75) | 9 (45) | doi:10.7717/peerj.3813 |
| Comparison between Methods | |||||||||
| Study | Year | Indications | Weaning Success ECMO + IABP (%) | Weaning Success ECMO + Septostomy (%) | Weaning Success ECMO + LV Cannula (%) | Mortality ECMO + IABP (%) | Mortality ECMO + Septostomy (%) | Mortality ECMO + LV Cannula (%) | Reference |
| Hasde et al. | 2020 | Any CS | 11 (55) | 9 (52.9) | 7 (43.7) | 11 (55) | 8 (47.1) | 9 (56.3) | doi:10.1093/icvts/ivaa284 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ricarte Bratti, J.P.; Cavayas, Y.A.; Noly, P.E.; Serri, K.; Lamarche, Y. Modalities of Left Ventricle Decompression during VA-ECMO Therapy. Membranes 2021, 11, 209. https://doi.org/10.3390/membranes11030209
Ricarte Bratti JP, Cavayas YA, Noly PE, Serri K, Lamarche Y. Modalities of Left Ventricle Decompression during VA-ECMO Therapy. Membranes. 2021; 11(3):209. https://doi.org/10.3390/membranes11030209
Chicago/Turabian StyleRicarte Bratti, Juan Pablo, Yiorgos Alexandros Cavayas, Pierre Emmanuel Noly, Karim Serri, and Yoan Lamarche. 2021. "Modalities of Left Ventricle Decompression during VA-ECMO Therapy" Membranes 11, no. 3: 209. https://doi.org/10.3390/membranes11030209
APA StyleRicarte Bratti, J. P., Cavayas, Y. A., Noly, P. E., Serri, K., & Lamarche, Y. (2021). Modalities of Left Ventricle Decompression during VA-ECMO Therapy. Membranes, 11(3), 209. https://doi.org/10.3390/membranes11030209