
Decrease of Pneumococcal Community-Acquired Pneumonia Hospitalization and Associated Complications in Children after the Implementation of the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) in Taiwan



Abstract
1. Introduction
2. Materials and Methods
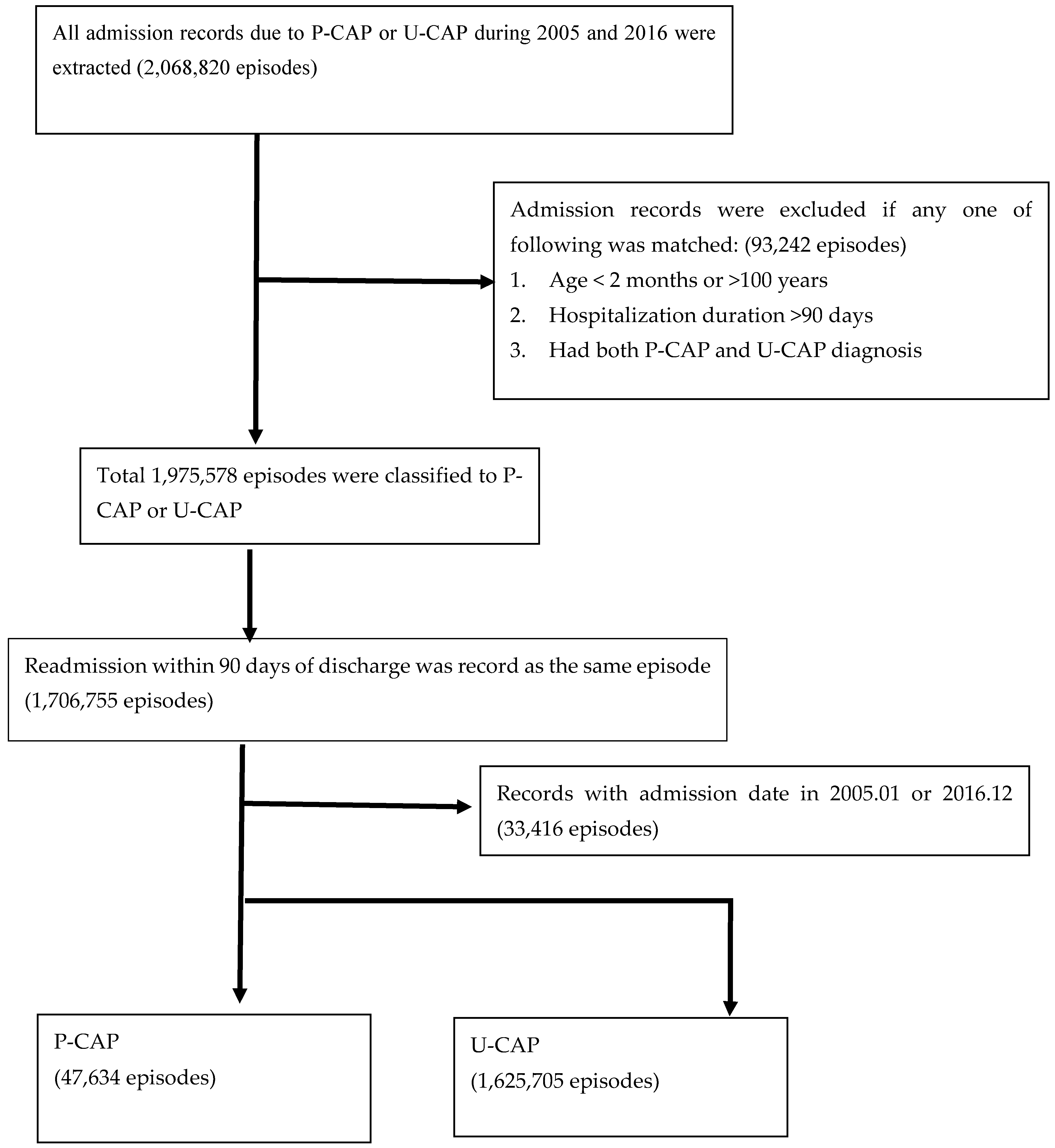
2.1. Data Source
2.2. Definitions of CAP Admissions and Clinical Outcomes
2.3. Statistical Analyses
3. Results
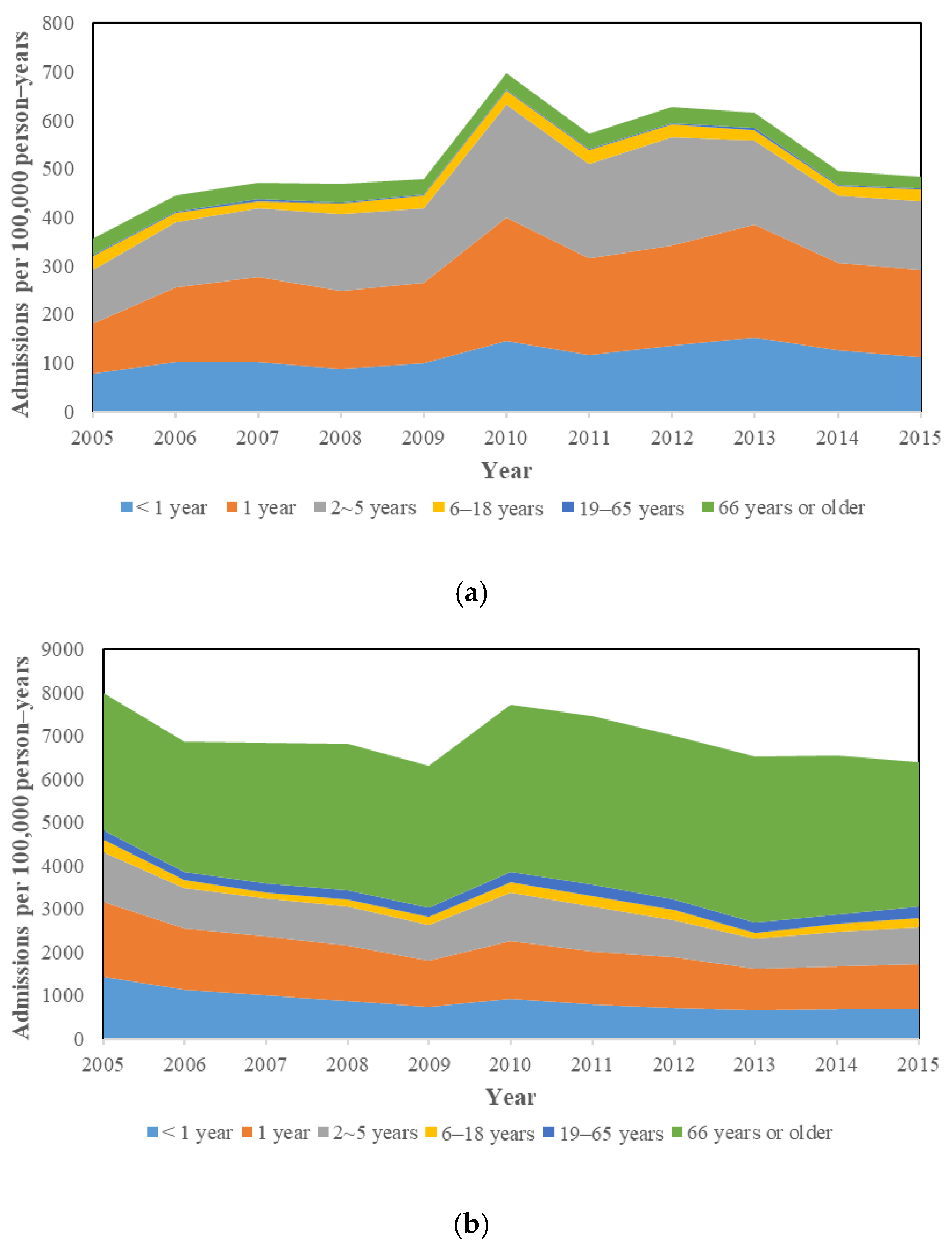
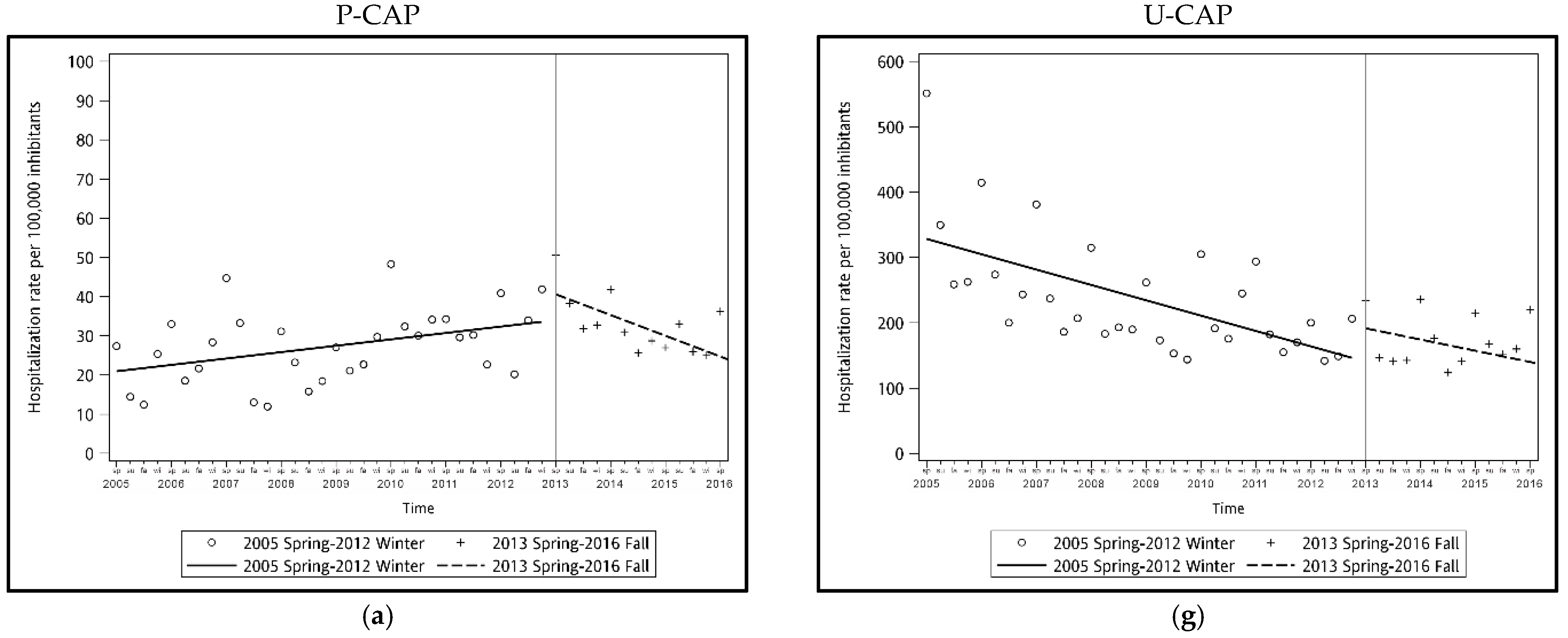
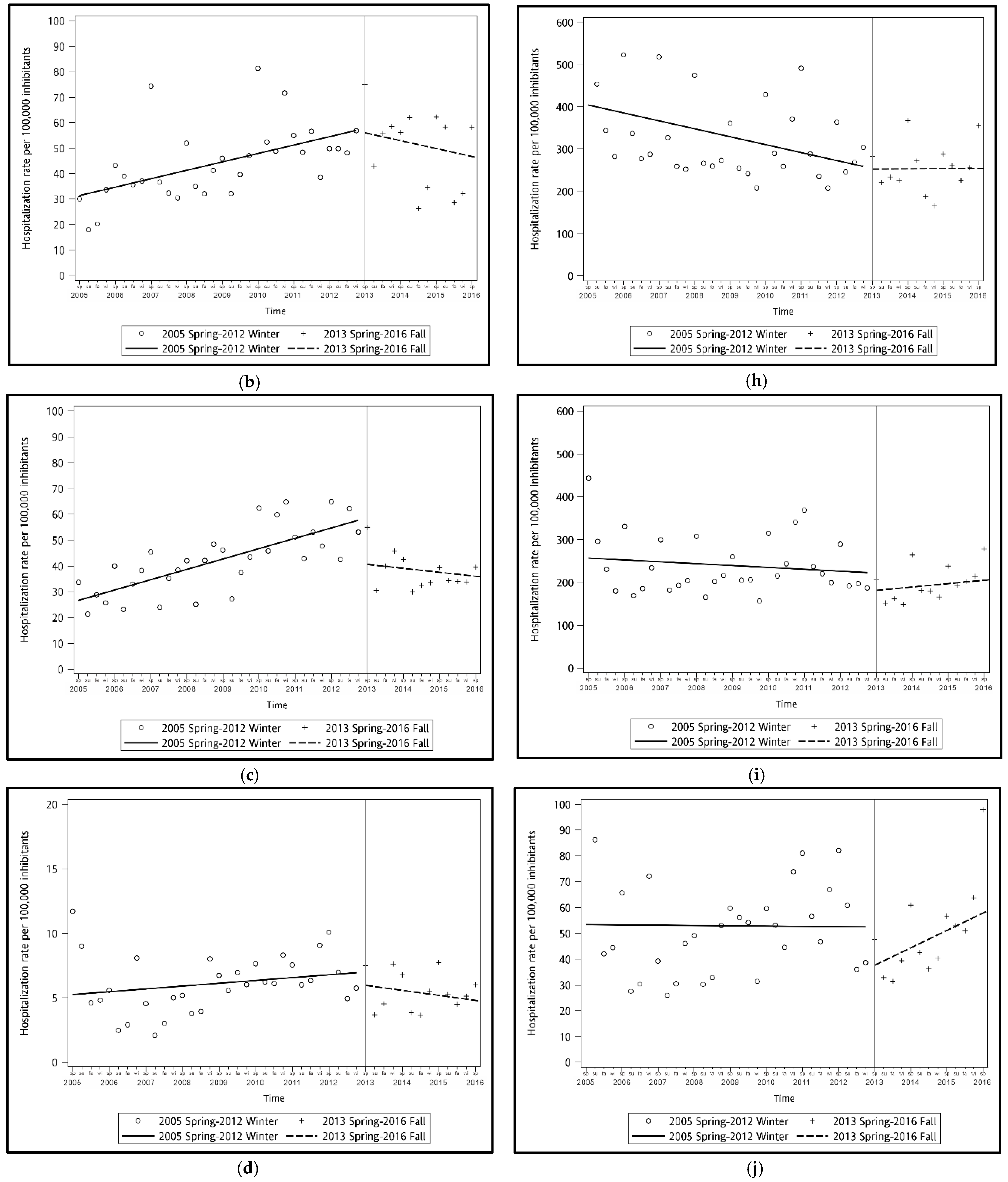
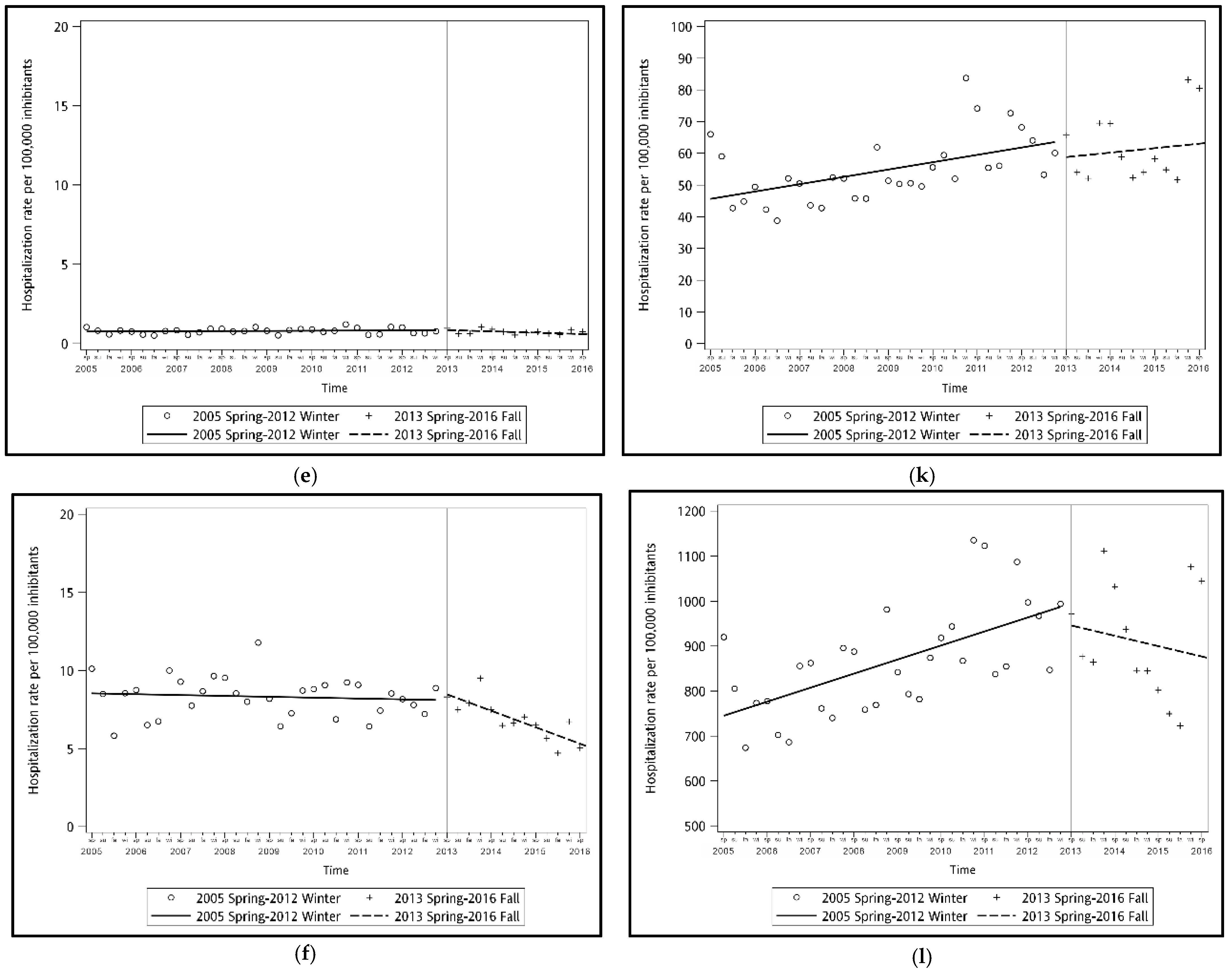
3.1. The Trend of Hospitalization Rates before and after PVC13 Introduction
3.2. PCV13-Associated Reductions in the Clinical Outcomes
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Denny, F.W.; Clyde, W.A., Jr. Acute lower respiratory tract infections in nonhospitalized children. J. Pediatr. 1986, 108, 635–646. [Google Scholar] [CrossRef]
- World Health Organization. Pneumonia. Available online: https://www.who.int/news-room/fact-sheets/detail/pneumonia (accessed on 31 May 2021).
- Myint, T.T.; Madhava, H.; Balmer, P.; Christopoulou, D.; Attal, S.; Menegas, D.; Sprenger, R.; Bonnet, E. The impact of 7-valent pneumococcal conjugate vaccine on invasive pneumococcal disease: A literature review. Adv. Ther. 2013, 30, 127–151. [Google Scholar] [CrossRef]
- Isturiz, R.; Sings, H.L.; Hilton, B.; Arguedas, A.; Reinert, R.R.; Jodar, L. Streptococcus pneumoniae serotype 19A: Worldwide epidemiology. Expert Rev. Vaccines 2017, 16, 1007–1027. [Google Scholar] [CrossRef] [PubMed]
- Hammitt, L.L.; Bruden, D.L.; Butler, J.C.; Baggett, H.C.; Hurlburt, D.A.; Reasonover, A.; Hennessy, T.W. Indirect effect of conjugate vaccine on adult carriage of Streptococcus pneumoniae: An explanation of trends in invasive pneumococcal disease. J. Infect. Dis. 2006, 193, 1487–1494. [Google Scholar] [CrossRef]
- Hsieh, Y.C.; Lin, P.Y.; Chiu, C.H.; Huang, Y.C.; Chang, K.Y.; Liao, C.H.; Chiu, N.C.; Chuang, Y.C.; Chen, P.Y.; Chang, S.C.; et al. National survey of invasive pneumococcal diseases in Taiwan under partial PCV7 vaccination in 2007: Emergence of serotype 19A with high invasive potential. Vaccine 2009, 27, 5513–5518. [Google Scholar] [CrossRef]
- Su, V.Y.; Liu, C.J.; Wang, H.K.; Wu, L.A.; Chang, S.C.; Perng, D.W.; Su, W.J.; Chen, Y.M.; Lin, E.Y.; Chen, T.J.; et al. Sleep apnea and risk of pneumonia: A nationwide population-based study. CMAJ 2014, 186, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Economic Affairs. Regulations Governing Fees for Commodity Inspection. Available online: https://law.moea.gov.tw/EngLawContent.aspx?id=10459 (accessed on 4 September 2021).
- Centers for Disease Control and Prevention (CDC). Progress in introduction of pneumococcal conjugate vaccine—worldwide, 2000–2012. MMWR Morb. Mortal. Wkly. Rep. 2013, 62, 308–311. [Google Scholar]
- Nuorti, J.P.; Whitney, C.G.; Centers for Disease Control and Prevention (CDC). Prevention of pneumococcal disease among infants and children—use of 13-valent pneumococcal conjugate vaccine and 23-valent pneumococcal polysaccharide vaccine—recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Recomm. Rep. 2010, 59, 1–18. [Google Scholar] [PubMed]
- Castiglia, P. Recommendations for pneumococcal immunization outside routine childhood immunization programs in Western Europe. Adv. Ther. 2014, 31, 1011–1044. [Google Scholar] [CrossRef] [PubMed]
- Poirier, B.; De Wals, P.; Petit, G.; Erickson, L.J.; Pepin, J. Cost-effectiveness of a 3-dose pneumococcal conjugate vaccine program in the province of Quebec, Canada. Vaccine 2009, 27, 7105–7109. [Google Scholar] [CrossRef]
- Su, W.J.; Lo, H.Y.; Chang, C.H.; Chang, L.Y.; Chiu, C.H.; Lee, P.I.; Lu, C.Y.; Hsieh, Y.C.; Lai, M.S.; Lin, T.Y. Effectiveness of Pneumococcal Conjugate Vaccines of Different Valences Against Invasive Pneumococcal Disease Among Children in Taiwan: A Nationwide Study. Pediatr. Infect. Dis. J. 2016, 35, e124–e133. [Google Scholar] [CrossRef]
- Lu, C.Y.; Chiang, C.S.; Chiu, C.H.; Wang, E.T.; Chen, Y.Y.; Yao, S.M.; Chang, L.Y.; Huang, L.M.; Lin, T.Y.; Chou, J.H. Successful Control of Streptococcus pneumoniae 19A Replacement With a Catch-up Primary Vaccination Program in Taiwan. Clin. Infect. Dis. 2019, 69, 1581–1587. [Google Scholar] [CrossRef]
- Shen, C.F.; Wang, S.M.; Chi, H.; Huang, Y.C.; Huang, L.M.; Huang, Y.C.; Lin, H.C.; Ho, Y.H.; Hsiung, C.A.; Liu, C.C.; et al. The potential role of pneumococcal conjugate vaccine in reducing acute respiratory inflammation in community-acquired pneumococcal pneumonia. J. Biomed. Sci. 2020, 27, 88. [Google Scholar] [CrossRef]
- Lindstrand, A.; Bennet, R.; Galanis, I.; Blennow, M.; Ask, L.S.; Dennison, S.H.; Rinder, M.R.; Eriksson, M.; Henriques-Normark, B.; Ortqvist, A.; et al. Sinusitis and pneumonia hospitalization after introduction of pneumococcal conjugate vaccine. Pediatrics 2014, 134, e1528–e1536. [Google Scholar] [CrossRef]
- Nair, H.; Watts, A.T.; Williams, L.J.; Omer, S.B.; Simpson, C.R.; Willocks, L.J.; Cameron, J.C.; Campbell, H. Pneumonia hospitalisations in Scotland following the introduction of pneumococcal conjugate vaccination in young children. BMC Infect. Dis. 2016, 16, 390. [Google Scholar] [CrossRef] [PubMed]
- Alicino, C.; Paganino, C.; Orsi, A.; Astengo, M.; Trucchi, C.; Icardi, G.; Ansaldi, F. The impact of 10-valent and 13-valent pneumococcal conjugate vaccines on hospitalization for pneumonia in children: A systematic review and meta-analysis. Vaccine 2017, 35, 5776–5785. [Google Scholar] [CrossRef] [PubMed]
- Falkenhorst, G.; Remschmidt, C.; Harder, T.; Hummers-Pradier, E.; Wichmann, O.; Bogdan, C. Effectiveness of the 23-Valent Pneumococcal Polysaccharide Vaccine (PPV23) against Pneumococcal Disease in the Elderly: Systematic Review and Meta-Analysis. PLoS ONE 2017, 12, e0169368. [Google Scholar] [CrossRef]
- Su, W.J.; Chuang, P.H.; Chang, L.Y.; Lo, H.Y.; Chiang, C.S.; Wang, E.T.; Yang, C.H. Application of the screening and indirect cohort methods to evaluate the effectiveness of pneumococcal vaccination program in adults 75 years and older in Taiwan. BMC Infect. Dis. 2021, 21, 45. [Google Scholar] [CrossRef] [PubMed]
- García-Vázquez, E.; Marcos, M.A.; Mensa, J.; de Roux, A.; Puig, J.; Font, C.; Francisco, G.; Torres, A. Assessment of the usefulness of sputum culture for diagnosis of community-acquired pneumonia using the PORT predictive scoring system. Arch. Intern. Med. 2004, 164, 1807–1811. [Google Scholar] [CrossRef]
- Domínguez, J.; Blanco, S.; Rodrigo, C.; Azuara, M.; Galí, N.; Mainou, A.; Esteve, A.; Castellví, A.; Prat, C.; Matas, L.; et al. Usefulness of urinary antigen detection by an immunochromatographic test for diagnosis of pneumococcal pneumonia in children. J. Clin. Microbiol. 2003, 41, 2161–2163. [Google Scholar] [CrossRef][Green Version]
- Mandell, L.A.; Wunderink, R.G.; Anzueto, A.; Bartlett, J.G.; Campbell, G.D.; Dean, N.C.; Dowell, S.F.; File, T.M., Jr.; Musher, D.M.; Niederman, M.S.; et al. Infectious Diseases Society of America/American Thoracic Society consensus guidelines on the management of community-acquired pneumonia in adults. Clin. Infect. Dis. 2007, 44 (Suppl. 2), S27–S72. [Google Scholar] [CrossRef] [PubMed]
- Cilloniz, C.; Martin-Loeches, I.; Garcia-Vidal, C.; San Jose, A.; Torres, A. Microbial Etiology of Pneumonia: Epidemiology, Diagnosis and Resistance Patterns. Int. J. Mol. Sci. 2016, 17, 2120. [Google Scholar] [CrossRef]
- Grijalva, C.G.; Nuorti, J.P.; Arbogast, P.G.; Martin, S.W.; Edwards, K.M.; Griffin, M.R. Decline in pneumonia admissions after routine childhood immunisation with pneumococcal conjugate vaccine in the USA: A time-series analysis. Lancet 2007, 369, 1179–1186. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| P-CAP | U-CAP | |||||||
|---|---|---|---|---|---|---|---|---|
| Age Groups | Estimated Difference of Hospitalization Rate 1 | 95% CI | p Value | % of Change | Estimated Difference of Hospitalization Rate | 95% CI | p Value | % of Change |
| <1 year | −22.51 | −35.52 to −9.51 | <0.01 | 59% | 20.50 | −91.49 to 135.64 | 0.71 | 12% |
| 1 year | −20.81 | −41.55 to −0.08 | 0.06 | 39% | 62.13 | −85.94 to 219.76 | 0.4 | 27% |
| 2~5 years | −18.01 | −31.63 to −4.4 | 0.01 | 47% | 39.84 | −61.84 to 147.66 | 0.43 | 24% |
| 6–18 years | −1.97 | −5.21 to 1.26 | 0.24 | 35% | 22.31 | −9.42 to 57.46 | 0.17 | 64% |
| 19–65 years | −0.31 | −0.58 to −0.03 | 0.04 | 39% | −2.93 | −19.38 to 13.08 | 0.71 | 5% |
| 66 years or older | −3.25 | −5.11 to −1.4 | 0 < 0.01 | 41% | −176.27 | −367.43 to −12.22 | 0.04 | 20% |
| Age Groups | Length of Hospital Stay (Days, Mean ± SD) | ICU Admission (%) | Severe Pneumonia (%) | Invasive Procedure (%) | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| P-CAP Group | Pre- | Post- | p-Value | Pre- | Post- | p-Value | Pre- | Post- | p-Value | Pre- | Post- | p-Value |
| <1 year | 6.5 (5.6) | 5.5 (3.8) | <0.0001 | 8.6 | 6.0 | 0.0187 | 25.2 | 24.1 | 0.5248 | 0.3 | 0.0 | 0.0921 |
| 1 year | 5. 9 (4.3) | 5.1 (3.2) | <0.0001 | 5.7 | 3.9 | 0.0067 | 19.2 | 17.4 | 0.1488 | 2.4 | 0.6 | <0.0001 |
| 2~5 years | 6.0 (4.4) | 5.1 (3.3) | <0.0001 | 6. 8 | 3.9 | <0.0001 | 21.7 | 14.5 | <0.0001 | 4.3 | 2.0 | <0.0001 |
| 6–18 years | 5.9 (4.7) | 5.4 (4.3) | <0.0001 | 6.3 | 5.1 | 0.2333 | 19.6 | 16.3 | 0.0002 | 2.9 | 1.9 | 0.0098 |
| 19–65 years | 11.8 (12.1) | 12.0 (12.4) | 0.4708 | 22.5 | 24.4 | 0.1143 | 59.4 | 63.6 | 0.0027 | 9.4 | 9.8 | 0.6381 |
| 66 years or older | 13. 9 (12. 9) | 13.7 (12.2) | 0.4143 | 29.9 | 27.4 | 0.0231 | 81.9 | 81.6 | 0.7571 | 11.1 | 9.7 | 0.0608 |
| U-CAP group | ||||||||||||
| <1 year | 7.1 (7.5) | 6.3 (6.3) | <0.0001 | 11.2 | 10.3 | 0.0806 | 27.5 | 26.1 | 0.0545 | 0.5 | 0.5 | 0.969 |
| 1 year | 5.5 (4.7) | 5.1 (4.3) | <0.0001 | 5.0 | 4.6 | 0.2084 | 16.3 | 18.0 | 0.0005 | 0.4 | 0.3 | 0.3849 |
| 2~5 years | 5.0 (3.7) | 4.7 (3.7) | <0.0001 | 2.8 | 3.0 | 0.1067 | 14.3 | 16.1 | <0.0001 | 0.6 | 0.3 | <0.0001 |
| 6–18 years | 5.5 (5.9) | 5.3 (5.4) | <0.0001 | 4.4 | 4.3 | 0.2516 | 16.0 | 17.6 | <0.0001 | 1.0 | 0.7 | 0.0026 |
| 19–65 years | 14.2 (15.8) | 13.1 (14.5) | <0.0001 | 24.9 | 21.7 | <0.0001 | 61.1 | 60.7 | 0.0109 | 10.1 | 8.9 | <0.0001 |
| 66 years or older | 17.2 (16.8) | 14.9 (14.4) | <0.0001 | 34.3 | 25.9 | <0.0001 | 82.3 | 80.4 | <0.0001 | 11.0 | 9.1 | <0.0001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shen, C.-F.; Chen, J.-L.; Su, C.-C.; Lin, W.-L.; Hsieh, M.-L.; Liu, C.-C.; Cheng, C.-L. Decrease of Pneumococcal Community-Acquired Pneumonia Hospitalization and Associated Complications in Children after the Implementation of the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) in Taiwan. Vaccines 2021, 9, 1043. https://doi.org/10.3390/vaccines9091043
Shen C-F, Chen J-L, Su C-C, Lin W-L, Hsieh M-L, Liu C-C, Cheng C-L. Decrease of Pneumococcal Community-Acquired Pneumonia Hospitalization and Associated Complications in Children after the Implementation of the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) in Taiwan. Vaccines. 2021; 9(9):1043. https://doi.org/10.3390/vaccines9091043
Chicago/Turabian StyleShen, Ching-Fen, Ju-Ling Chen, Chien-Chou Su, Wen-Liang Lin, Min-Ling Hsieh, Ching-Chun Liu, and Ching-Lan Cheng. 2021. "Decrease of Pneumococcal Community-Acquired Pneumonia Hospitalization and Associated Complications in Children after the Implementation of the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) in Taiwan" Vaccines 9, no. 9: 1043. https://doi.org/10.3390/vaccines9091043
APA StyleShen, C.-F., Chen, J.-L., Su, C.-C., Lin, W.-L., Hsieh, M.-L., Liu, C.-C., & Cheng, C.-L. (2021). Decrease of Pneumococcal Community-Acquired Pneumonia Hospitalization and Associated Complications in Children after the Implementation of the 13-Valent Pneumococcal Conjugate Vaccine (PCV13) in Taiwan. Vaccines, 9(9), 1043. https://doi.org/10.3390/vaccines9091043