
Understanding Soaring Coronavirus Cases and the Effect of Contagion Policies in the UK



{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods
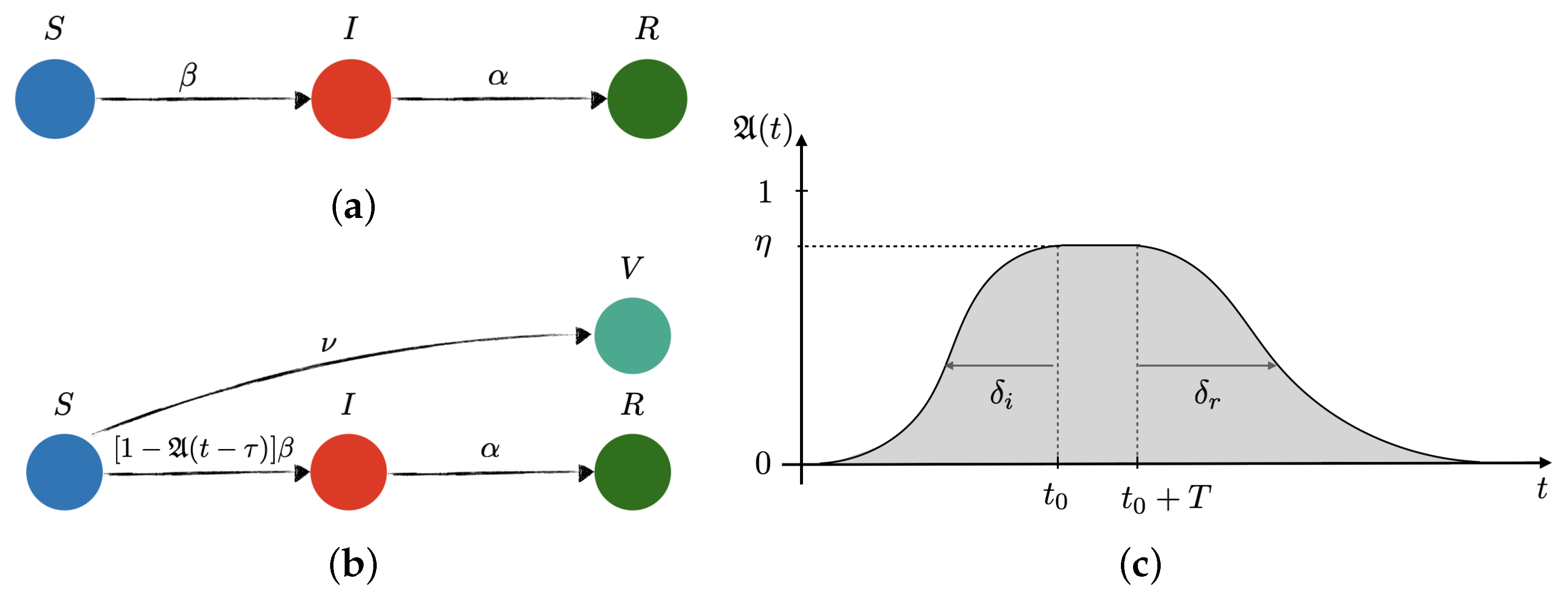
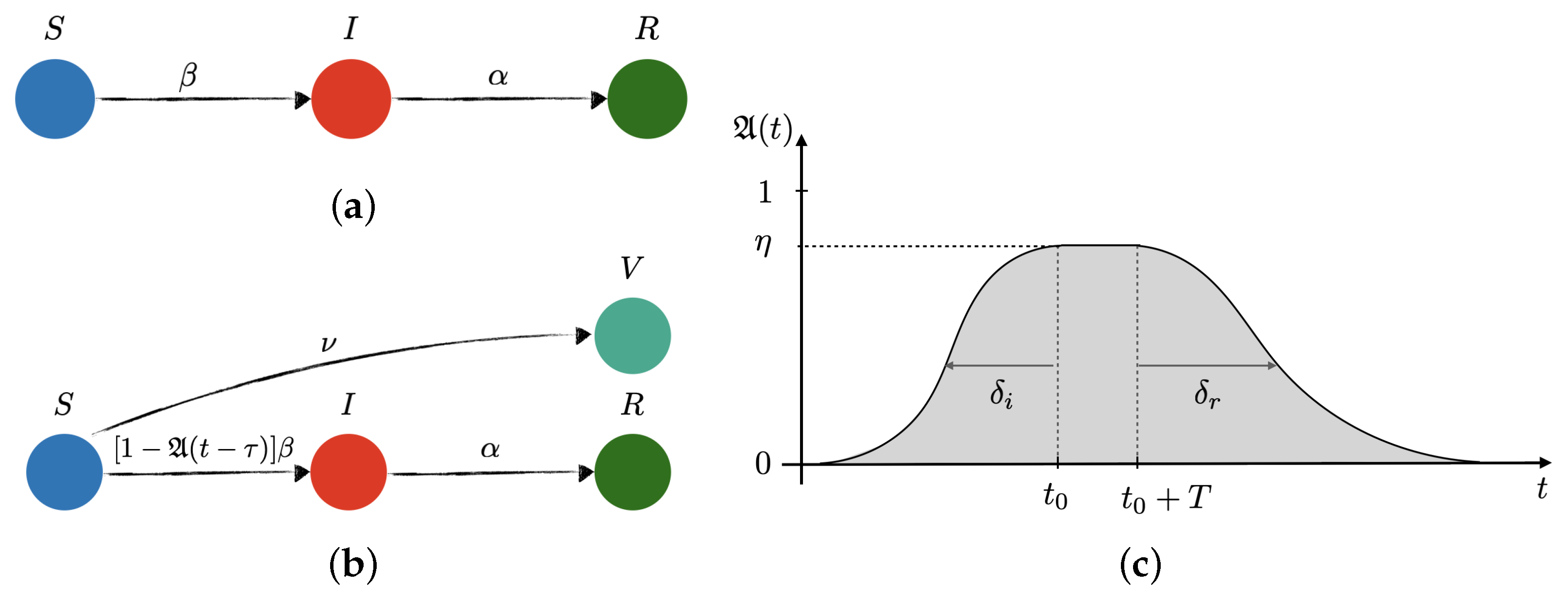
2.1. Population Dynamics
2.2. Training and Testing the Model
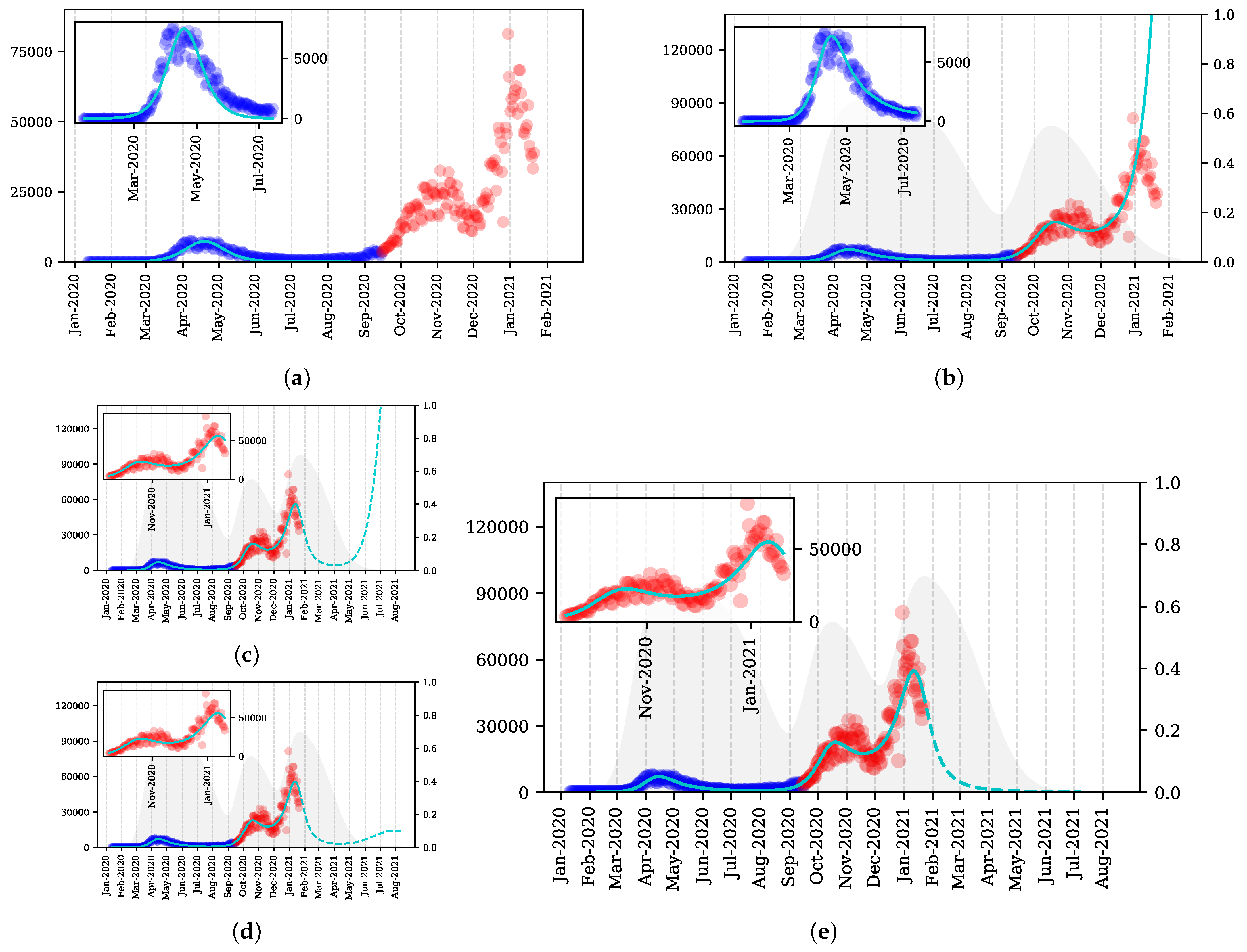
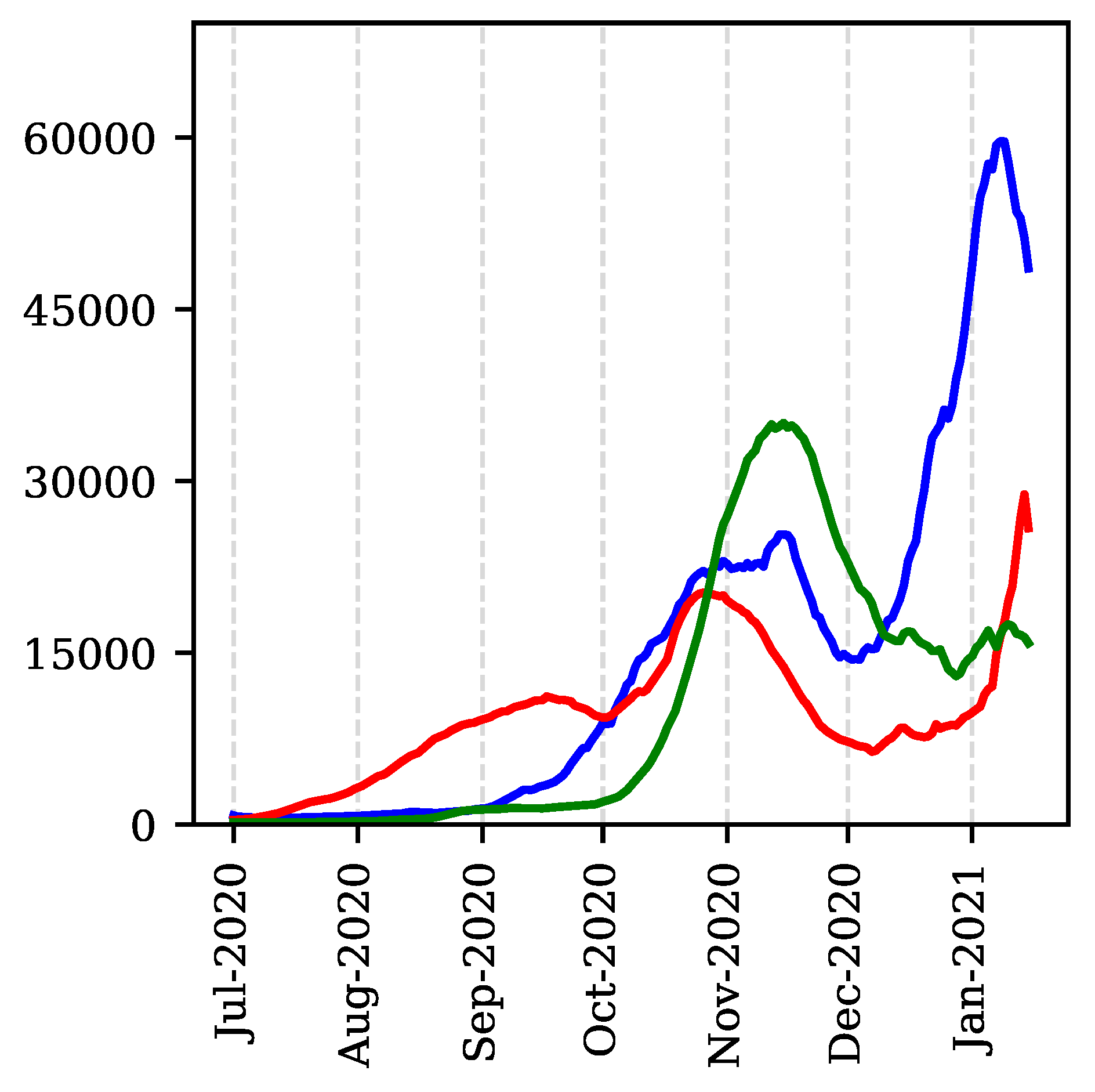
3. Results and Discussion
4. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kermack, W.O.; McKendrick, A.G. A Contribution to the Mathematical Theory of Epidemics. Proc. R. Soc. A 1927, 115, 700–721. [Google Scholar]
- Volz, E.; Mishra, S.; Chand, M.; Barrett, J.C.; Johnson, R.; Geidelberg, L.; Hinsley, W.R.; Laydon, D.J.; Dabrera, G.; O’Toole, Á.; et al. Transmission of SARS-CoV-2 Lineage B.1.1.7 in England: Insights from Linking Epidemiological and Genetic Data, Preprint. Available online: https://www.medrxiv.org/content/early/2021/01/04/2020.12.30.20249034.1 (accessed on 28 April 2021).
- KatulI, G.G.; Mrad, A.; Bonetti, S.; Manoli, G.; Parolari, A.J. Global convergence of COVID-19 basic reproduction number and estimation from early-time SIR dynamics. PLoS ONE 2020, 15, E0239800. [Google Scholar] [CrossRef] [PubMed]
- Nguemdjo, U.; Meno, F.; Dongfack, A.; Ventelou, B. Simulating the progression of the COVID-19 disease in Cameroon using SIR models. PLoS ONE 2020, 15, E0237832. [Google Scholar] [CrossRef] [PubMed]
- Cooper, I.; Mondal, A.; Antonopoulos, C.G. A SIR model assumption for the spread of COVID-19 in different communities. Chaos Soliton. Fract. 2020, 139, 110057. [Google Scholar] [CrossRef] [PubMed]
- Weitz, J.S.; Beckett, S.J.; Coenen, A.R.; Demory, D.; Dominguez-Mirazo, M.; Dushoff, J.; Leung, C.-Y.; Li, G.; Măgălie, A.; Park, S.W.; et al. Modeling shield immunity to reduce COVID-19 epidemic spread. Nat. Med. 2020, 26, 849–854. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, J. New Covid Strain UK: What Are the Symptoms of the New Coronavirus Variant—And Will the Vaccine Still Work? The Scotsman, 11 January 2021. Available online: https://www.scotsman.com/health/coronavirus/new-covid-strain-uk-what-are-symptoms-new-coronavirus-variant-and-will-vaccine-still-work-3068541 (accessed on 28 April 2021).
- Lauer, S.A.; Grantz, K.H.; Bi, Q.; Jones, F.K.; Zheng, Q.; Meredith, H.R.; Azman, A.S.; Reich, N.G.; Lessler, J. The Incubation Period of Coronavirus Disease 2019 (COVID-19) From Publicly Reported Confirmed Cases: Estimation and Application. Ann. Intern. Med. 2020, 172, 577–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasell, J.; Mathieu, E.; Beltekian, D.; Macdonald, B.; Giattino, C.; Ortiz-Ospina, E.; Roser, M.; Ritchie, H. A cross-country database of CoVid-19 testing. Sci. Data 2020, 7, 345. [Google Scholar] [CrossRef] [PubMed]
- Covid: UK Seeing Second Wave, Says Boris Johnson, BBC News 18 September 2020. Available online: https://www.bbc.com/news/av/uk-54213129 (accessed on 28 April 2021).
- PM Commons Statement on Coronavirus, Prime Minister’s Office, 12 October 2020. Available online: https://www.gov.uk/government/speeches/pm-commons-statement-on-coronavirus-12-october-2020 (accessed on 28 April 2021).
- Dathan, M.; Cole, H.; Ferguson, K.; Clark, N. Boris Johnson Vows to Deliver 200,000 Vaccines a Day by Next Week & Every Care Home Resident This Month, The Sun, 7 January 2021. Available online: https://www.thesun.co.uk/news/13672615/covid-vaccine-press-conference-boris-johnson-hundreds (accessed on 28 April 2021).
- Coronavirus: Hancock Concern over ’Sharp Rise’ in Cases, BBC News 8 September 2020. Available online: https://www.bbc.com/news/uk-54066831 (accessed on 28 April 2021).
- Virtanen, P.; Virtanen, P.; Gommers, R.; Oliphant, T.E.; Haberland, M.; Reddy, T.; Cournapeau, D.; Burovski, E.; Peterson, P.; Weckesser, W.; et al. SciPy 1.0: Fundamental Algorithms for Scientific Computing in Python. Nat. Methods 2020, 17, 261–272. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hindmarsh, A.C. ODEPACK, A Systematized Collection of ODE Solvers, Scientific Computing; North-Holland: Amsterdam, The Netherlands, 1983; Volume 1, pp. 55–64. [Google Scholar]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Durán-Olivencia, M.A.; Kalliadasis, S. Understanding Soaring Coronavirus Cases and the Effect of Contagion Policies in the UK. Vaccines 2021, 9, 735. https://doi.org/10.3390/vaccines9070735
Durán-Olivencia MA, Kalliadasis S. Understanding Soaring Coronavirus Cases and the Effect of Contagion Policies in the UK. Vaccines. 2021; 9(7):735. https://doi.org/10.3390/vaccines9070735
Chicago/Turabian StyleDurán-Olivencia, Miguel A., and Serafim Kalliadasis. 2021. "Understanding Soaring Coronavirus Cases and the Effect of Contagion Policies in the UK" Vaccines 9, no. 7: 735. https://doi.org/10.3390/vaccines9070735
APA StyleDurán-Olivencia, M. A., & Kalliadasis, S. (2021). Understanding Soaring Coronavirus Cases and the Effect of Contagion Policies in the UK. Vaccines, 9(7), 735. https://doi.org/10.3390/vaccines9070735