
Targeted Vaccine Allocation Could Increase the COVID-19 Vaccine Benefits Amidst Its Lack of Availability: A Mathematical Modeling Study in Indonesia





Abstract
1. Introduction
2. Materials and Methods
2.1. Context
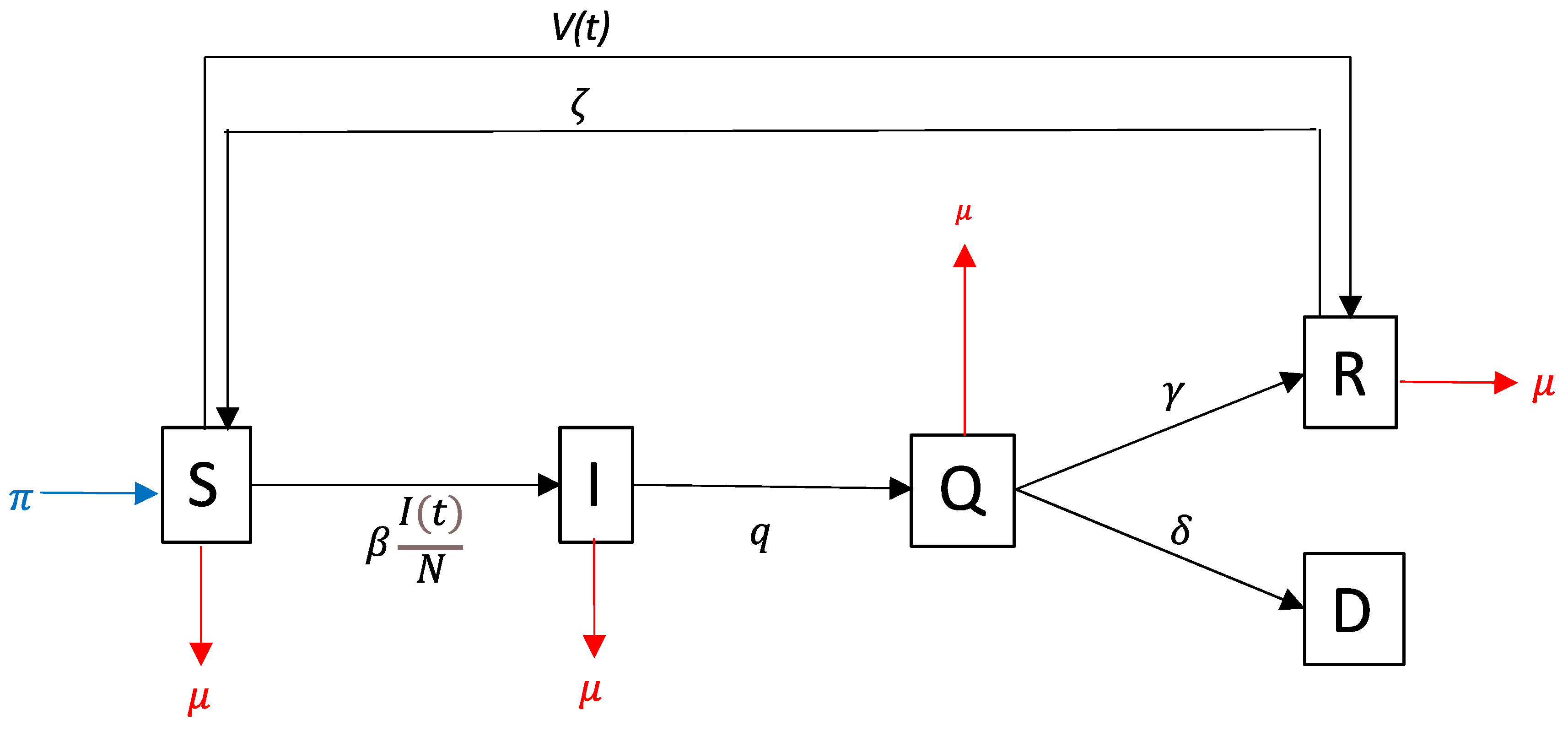
2.2. Model of Disease Transmission
2.3. Time-Period Scenarios
2.4. Targeted Allocation Scenarios
3. Results
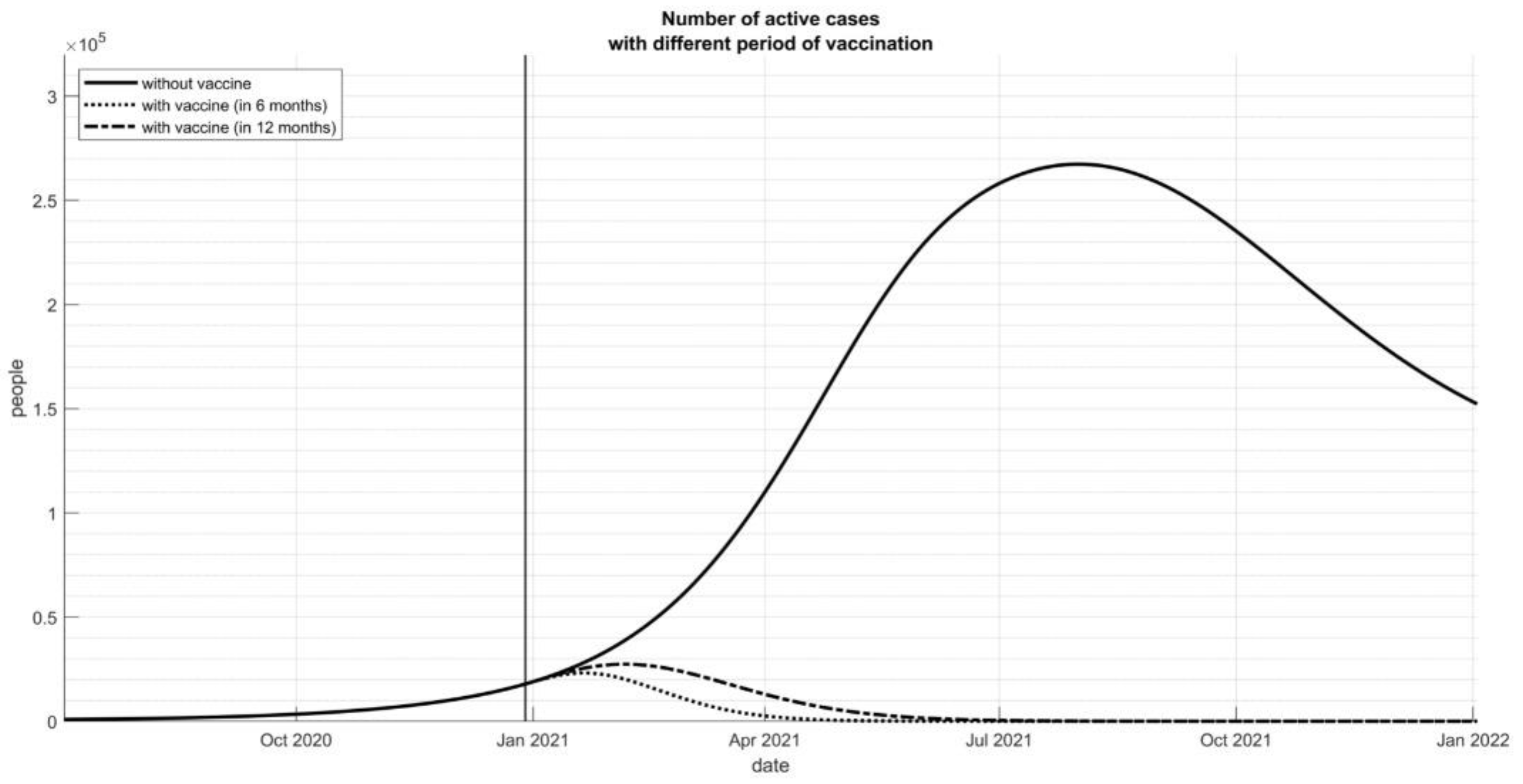
3.1. Time-Period Scenarios
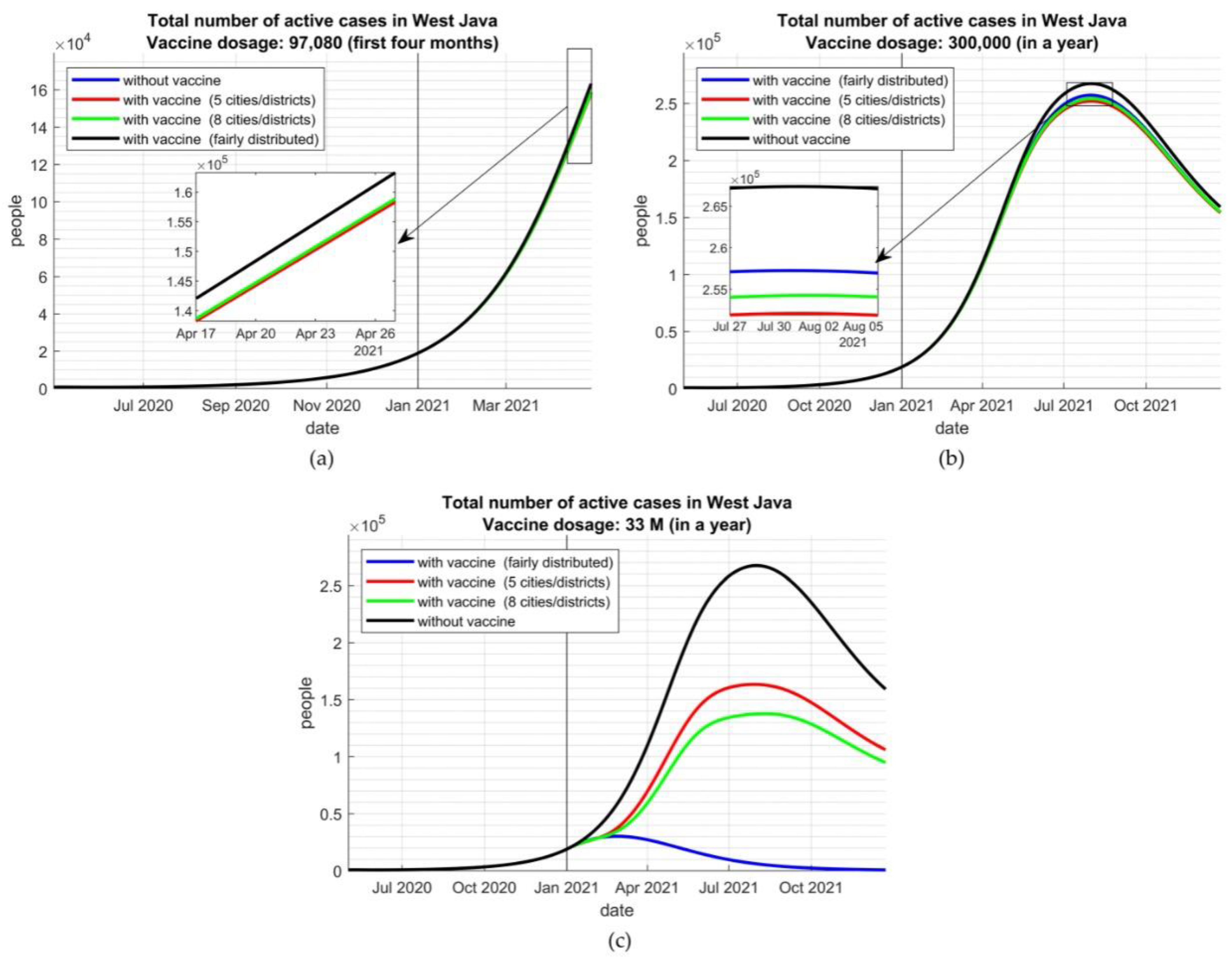
3.2. Targeted Allocation Scenarios
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Symbols | Description | Unit | Values |
|---|---|---|---|
| # of the susceptible population at time- | person | Estimated | |
| # of the infected population at time- | person | Estimated | |
| # of the quarantined population at time- | person | Estimated | |
| # of the immune population at time- | person | Estimated | |
| # of deaths at time- | person | Estimated | |
| Transmission rate | 1/day | Estimated | |
| The recovery rate of COVID-19 | 1/day | Estimated | |
| The death rate of COVID-19 | 1/day | Estimated | |
| Quarantine rate a | 1/day | 0.4 | |
| Vaccination rate | 1/day | Estimated | |
| Vaccine efficacy b | - | 0.8 | |
| Reinfection rate c | 1/day | 0.00035 | |
| Natural birth rate d | 1/day | 0.00004 | |
| Natural death rate | 1/day | 0.00004 |
| No. | City/District | # of Population | # of Total Infections | |
|---|---|---|---|---|
| 1 | Bekasi City | 26,729 | 2,932,000 | 1.24 |
| 2 | Depok City | 25,430 | 1,869,998 | 0.72 |
| 3 | Bekasi District | 14,798 | 2,829,000 | 1.69 |
| 4 | Bandung City | 10,219 | 2,395,000 | 1.37 |
| 5 | Karawang District | 9192 | 2,288,000 | 1.17 |
| 6 | Bogor City | 8621 | 950,334 | 3.27 |
| 7 | Bandung District | 7671 | 3,418,000 | 0.96 |
| 8 | Bogor District | 6835 | 5,715,009 | 0.74 |
| 9 | Garut District | 6588 | 2,547,000 | 0.77 |
| 10 | Cirebon District | 4973 | 2,126,000 | 0.71 |
| 11 | Sukabumi District | 3838 | 2,434,000 | 1.06 |
| 12 | Cimahi City | 3652 | 561,386 | 0.95 |
| 13 | Kuningan District | 3231 | 1,055,000 | 0.19 |
| 14 | West Bandung District | 3138 | 1,624,000 | 0.46 |
| 15 | Tasikmalaya City | 3083 | 808,506 | 0.8 |
| 16 | Indramayu District | 2971 | 1,789,000 | 7.06 |
| 17 | Purwakarta District | 2854 | 916,912 | 1.83 |
| 18 | Sukabumi City | 2640 | 326,282 | 0.37 |
| 19 | Cirebon City | 2438 | 296,389 | 1.33 |
| 20 | Subang District | 1925 | 1,529,000 | 0.7 |
| 21 | Ciamis District | 1760 | 1,389,000 | 1.14 |
| 22 | Majalengka District | 1719 | 182,000 | 0.32 |
| 23 | Tasikmalaya District | 1649 | 1,736,000 | 4.94 |
| 24 | Cianjur District | 1631 | 2,829,000 | 0.76 |
| 25 | Sumedang District | 1535 | 1,176,000 | 1.29 |
| 26 | Banjar City | 530 | 182,819 | 0.91 |
| 27 | Pangandaran District | 510 | 422,586 | 1.34 |
References
- Bubar, K.M.; Reinholt, K.; Kissler, S.M.; Lipsitch, M.; Cobey, S.; Grad, Y.H.; Larremore, D.B. Model-informed COVID-19 vaccine prioritization strategies by age and serostatus. Science 2021, 371, 916. [Google Scholar] [CrossRef]
- Foy, B.H.; Wahl, B.; Mehta, K.; Shet, A.; Menon, G.I.; Britto, C. Comparing COVID-19 vaccine allocation strategies in India: A mathematical modelling study. Int. J. Infect. Dis. 2021, 103, 431–438. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.H.; Marks, F.; Clemens, J.D. Looking beyond COVID-19 vaccine phase 3 trials. Nat. Med. 2021, 27, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Coalition for Epidemic Preparedness Innovations. CEPI Survey Assesses Potential COVID-19 Vaccine Manufacturing Capacity; CEPI: Oslo, Norway, 2020. [Google Scholar]
- Piot, P.; Larson, H.J.; O’Brien, K.L.; N’kengasong, J.; Ng, E.; Sow, S.; Kampmann, B. Immunization: Vital progress, unfinished agenda. Nature 2019, 575, 119–129. [Google Scholar] [CrossRef] [PubMed]
- Sekretariat Kabinet Republik Indonesia Menkes: Vaksinasi COVID-19 Bagi Tenaga Kesehatan Capai Satu Juta. Available online: https://setkab.go.id/menkes-vaksinasi-covid-19-bagi-tenaga-kesehatan-capai-satu-juta/ (accessed on 5 March 2021).
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Smith, J.; Lipsitch, M.; Almond, J.W. Vaccine production, distribution, access, and uptake. Lancet 2011, 378, 428–438. [Google Scholar] [CrossRef]
- World Health Organization. COVID-19 Vaccine Acceptance Survey in Indonesia; WHO: Geneva, Switzerland, November 2020. [Google Scholar]
- Satgas COVID-19 Peta Sebaran. Available online: https://covid19.go.id/ (accessed on 5 March 2021).
- Lloyd-Sherlock, P.; Muljono, P.; Ebrahim, S. Ageism in Indonesia’s national covid-19 vaccination programme. BMJ 2021, 372, n299. [Google Scholar] [CrossRef] [PubMed]
- Nuraini, N.; Khairudin, K.; Hadisoemarto, P.; Susanto, H.; Hasan, A.; Sumarti, N. Mathematical models for assessing vaccination scenarios in several provinces in Indonesia. medRxiv 2020. [Google Scholar] [CrossRef]
- Li, Q.; Tang, B.; Bragazzi, N.L.; Xiao, Y.; Wu, J. Modeling the impact of mass influenza vaccination and public health interventions on COVID-19 epidemics with limited detection capability. Math. Biosci. 2020, 325, 108378. [Google Scholar] [CrossRef]
- Hattaf, K.; Lashari, A.; Louartassi, Y.; Yousfi, N. A delayed SIR epidemic model with a general incidence rate. Electron. J. Qual. Theory Differ. Equ. 2013, 2013, 1–9. [Google Scholar] [CrossRef]
- McAllister, S.; Wiem Lestari, B.; Sujatmiko, B.; Siregar, A.; Sihaloho, E.D.; Fathania, D.; Dewi, N.F.; Koesoemadinata, R.C.; Hill, P.C.; Alisjahbana, B. Feasibility of two active case finding approaches for detection of tuberculosis in Bandung City, Indonesia. Public Health Action 2017, 7, 206–211. [Google Scholar] [CrossRef][Green Version]
- Figueroa, J.P.; Bottazzi, M.E.; Hotez, P.; Batista, C.; Ergonul, O.; Gilbert, S.; Gursel, M.; Hassanain, M.; Kim, J.H.; Lall, B.; et al. Urgent needs of low-income and middle-income countries for COVID-19 vaccines and therapeutics. Lancet 2021, 397, 562–564. [Google Scholar] [CrossRef]
- Goldstein, J.R.; Cassidy, T.; Wachter, K.W. Vaccinating the oldest against COVID-19 saves both the most lives and most years of life. Proc. Natl. Acad. Sci. USA 2021, 118, e2026322118. [Google Scholar] [CrossRef]
- Schwartz, J.L. Evaluating and deploying Covid-19 vaccines—The importance of transparency, scientific integrity, and public trust. N. Engl. J. Med. 2020, 383, 1703–1705. [Google Scholar] [CrossRef] [PubMed]
- Gayle, H.; Brown, W.F.L.; Kahn, B. Framework for Equitable Allocation of COVID-19 Vaccine; The National Academy Press: Washington, DC, USA, 2020; Volume 10. [Google Scholar]
- World Health Organization. COVAX: Working for Global Equitable Access to COVID-19 Vaccines; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Fuady, A. Arsitektur Jaminan Kesehatan Indonesia: Capaian, Kritik, dan Tantangan masa Depan; Sagung Seto: Jakarta, Indonesia, 2019. [Google Scholar]
- Tomlin, J.; Dalgleish-Warburton, B.; Lamph, G. Psychosocial support for healthcare workers during the COVID-19 pandemic. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef]
- Bielicki, J.A.; Duval, X.; Gobat, N.; Goossens, H.; Koopmans, M.; Tacconelli, E.; van der Werf, S. Monitoring approaches for health-care workers during the COVID-19 pandemic. Lancet Infect. Dis. 2020, 20, e261–e267. [Google Scholar] [CrossRef]
- Olivares, A.; Staffetti, E. Uncertainty quantification of a mathematical model of COVID-19 transmission dynamics with mass vaccination strategy. ChaosSolitons Fractals 2021, 146, 110895. [Google Scholar] [CrossRef] [PubMed]
- Rappuoli, R.; Black, S.; Bloom, D.E. Vaccines and global health: In search of a sustainable model for vaccine development and delivery. Sci. Transl. Med. 2019, 11, eaaw2888. [Google Scholar] [CrossRef]
- Liu, Y.; Salwi, S.; Drolet, B.C. Multivalue ethical framework for fair global allocation of a COVID-19 vaccine. J. Med. Ethics 2020, 46, 499. [Google Scholar] [CrossRef] [PubMed]
- Burgos, R.M.; Badowski, M.E.; Drwiega, E.; Ghassemi, S.; Griffith, N.; Herald, F.; Johnson, M.; Smith, R.O.; Michienzi, S.M. The race to a COVID-19 vaccine: Opportunities and challenges in development and distribution. Drugs Context 2021, 10, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Motta, M.; Sylvester, S.; Callaghan, T.; Lunz-Trujillo, K. Encouraging COVID-19 vaccine uptake through effective health communication. Front. Political Sci. 2021, 3, 1–12. [Google Scholar] [CrossRef]



| Variables | Availability | Targeted Time-Period | |||
|---|---|---|---|---|---|
| 6 Months | 12 Months | ||||
| # of targeted inoculation | 33,500,000 | ||||
| # of vaccine dosage a | 67,000,000 | ||||
| # of healthcare staff | 1094 | 29,000 | 14,500 | 14,500 | 7250 |
| # of vaccinator | 365 | 9667 | 4833 | 4833 | 2417 |
| Duration (minute/person) | 10 | 10 | 5 | 10 | 5 |
| Inoculation per day b | 48 | 48 | 96 | 48 | 96 |
| # of vaccine per day | 17,504 | 464,000 | 464,000 | 232,000 | 232,000 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fuady, A.; Nuraini, N.; Sukandar, K.K.; Lestari, B.W. Targeted Vaccine Allocation Could Increase the COVID-19 Vaccine Benefits Amidst Its Lack of Availability: A Mathematical Modeling Study in Indonesia. Vaccines 2021, 9, 462. https://doi.org/10.3390/vaccines9050462
Fuady A, Nuraini N, Sukandar KK, Lestari BW. Targeted Vaccine Allocation Could Increase the COVID-19 Vaccine Benefits Amidst Its Lack of Availability: A Mathematical Modeling Study in Indonesia. Vaccines. 2021; 9(5):462. https://doi.org/10.3390/vaccines9050462
Chicago/Turabian StyleFuady, Ahmad, Nuning Nuraini, Kamal K. Sukandar, and Bony W. Lestari. 2021. "Targeted Vaccine Allocation Could Increase the COVID-19 Vaccine Benefits Amidst Its Lack of Availability: A Mathematical Modeling Study in Indonesia" Vaccines 9, no. 5: 462. https://doi.org/10.3390/vaccines9050462
APA StyleFuady, A., Nuraini, N., Sukandar, K. K., & Lestari, B. W. (2021). Targeted Vaccine Allocation Could Increase the COVID-19 Vaccine Benefits Amidst Its Lack of Availability: A Mathematical Modeling Study in Indonesia. Vaccines, 9(5), 462. https://doi.org/10.3390/vaccines9050462