
Age-Specific Seasonal Influenza Vaccine Effectiveness against Different Influenza Subtypes in the Hospitalized Population in Lithuania during the 2015–2019 Influenza Seasons

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Objectives
2.2. Study Design, Population, Setting, and Recruitment Procedure
2.3. Outcome
2.4. Exposure
2.5. Covariates
2.6. Laboratory Analysis
2.7. Statistical Analysis
2.8. Ethical Considerations
2.9. Sample Size Calculation
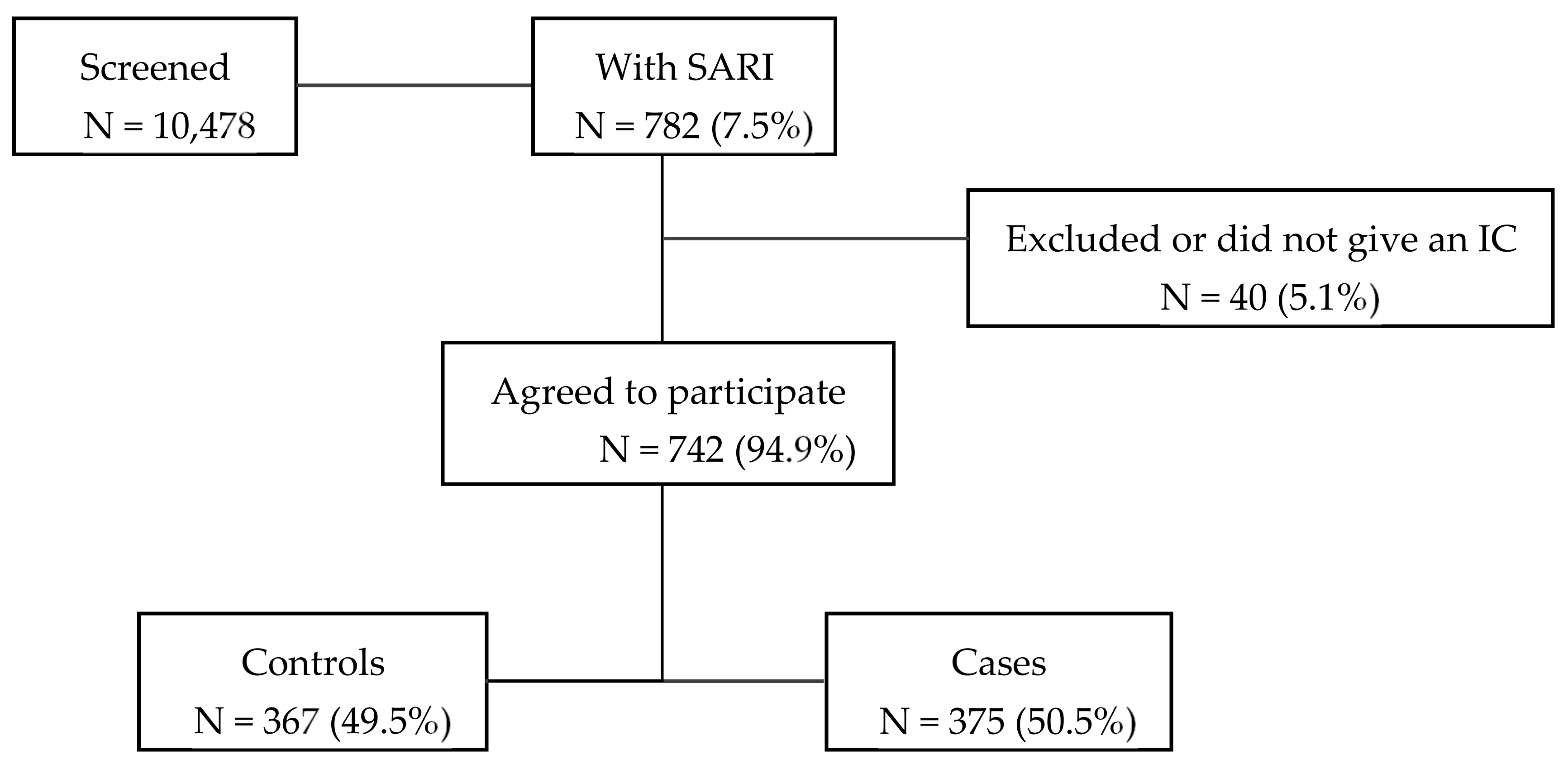
2.10. Sample
3. Results
Vaccine Effectiveness Analysis
4. Discussion
Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
| Chronic Underlying Conditions | ICD-10 Codes |
|---|---|
| Anemia, Spleen pathology | D50–75 S36.0 Q89.01,09 |
| Cancer | C00–96 C7A, B |
| Cardiovascular conditions | A52.01 |
| G46 | |
| I00–I09 I20 I21–I23 I24.0,1,8,9 I25 I27–28 134–37 124.1–9 143–6 148 I49 I50 I51–2 O90.3 Q20–28 | |
| Cirrhosis | K74 |
| Dementia, stroke | F01–06 F10 F19 G30.9 G31.01,1,09 G91.0–1 G35 G36.0 G37.0–3,5,8,9; G93.0-2,4,5,41,49 I60–64 I67.83 I69 |
| Endocrine disorders, diabetes | E10 E11–14 E15 E16.0–3 E16.8–9 E20–32 E35 E70–79 E83–5,7,8 E89.1 |
| Immunocompromised conditions | D80.0–4,8,9 K71–77, excl. K74 E06.3–5,9 E07 E90 M11 M83 Z94.0–2,5–7 Z95.3 B20–24 R75 Z21 |
| Lung diseases | A15.0 C30.0 C31–2 C33–4 C38.1-4 C39 C45.0,7 D14.0–4 D19.0 I26 J33 J34.1–3,8 J38–9 J43–4 J45–6 J47 J60–70 J80–2,4 J90–1 J92–3,6,8,9 J94 M40–1 M43.8–9 Q30–34 Q65–79 R09.1 Z90.2 |
| Nutritional deficiency | E32.0,1,8,9 E24.0,2,3,8,9 E25.0,8,9 E26.01,102,09,9,81 E34.0 E40,41,43–6 E50,51 |
| Obesity | E65–68 |
| Renal diseases | I12.0,9 M10.30 N00.3,8–9 N01.3 N02.2 N03.2–3,5,8 N04.0,3–4 N05 N07–8 N10–11 N13.30,721,729 N14 N15.0,8 N16 N17–19 N25 N27 N28.9 Q60–4 |
| Rheumatologic diseases | M05.00,10 M06.4,9 M08.00,40 M15.0–2,9 M12,00 M30–31 M32–35 |
References
- Flu News Europe. Joint ECDC—WHO/Europe Weekly Influenza Update. Summary Weeks 33–39/2019 (12 August–29 September 2019) 2018–2019 Season Overview; World Health Organization, European Centre for Disease Prevention and Control: Denmark, Sweden, 2019; pp. 1–9. [Google Scholar]
- World Health Organization. Influenza (Seasonal). Available online: https://www.who.int/news-room/fact-sheets/detail/influenza- (accessed on 3 March 2021).
- Sambhara, S.; McElhaney, J.E. Immunosenescence and Influenza Vaccine Efficacy. Curr. Top. Microbiol. Immunol. 2009, 333, 413–429. [Google Scholar] [CrossRef]
- World Health Organization. Influenza vaccination. Available online: http://www.euro.who.int/en/health-topics/communicable-diseases/influenza/vaccination (accessed on 3 March 2021).
- Lietuvos Respublikos Sveiktos Apsaugos Ministras. Įsakymas Dėl Nacionalinės Imunoprofilaktikos 2019–2023 Metų Programos Patvirtinimo. Available online: https://e-seimas.lrs.lt/portal/legalAct/lt/TAD/a88940c123b911e9b246d9cc49389932 (accessed on 24 February 2021).
- World Health Organization. The Fifty-sixth World Health Assembly. Prevention and Control of Influenza Pandemics and Annual Epidemics. Available online: https://apps.who.int/iris/handle/10665/259836 (accessed on 3 March 2021).
- European Centre for Disease Prevention and Control (ECDC). Seasonal Influenza Vaccination and Antiviral Use in EU/EEA Member States. Overview of Vaccine Recommendations for 2017–2018 and Vaccination Coverage Rates for 2015–2016 and 2016–2017 Influenza Seasons; European Centre for Disease Prevention and Control: Stockholm, Sweden, 2018. [Google Scholar]
- Martirosyan, L.; Paget, W.J.; Jorgensen, P.; Brown, C.S.; Meerhoff, T.J.; Pereyaslov, D.; Mott, J.A. The Community Impact of the 2009 Influenza Pandemic in the WHO European Region: A Comparison with Historical Seasonal Data from 28 Countries. BMC Infect. Dis. 2012, 12, 36. [Google Scholar] [CrossRef] [PubMed]
- Statistics Dissemination and Communication Division. Statistics Lithuania. Available online: https://www.stat.gov.lt/home (accessed on 26 January 2021).
- Institute of Hygiene. Available online: https://www.hi.lt/structure-and-contacts.html (accessed on 26 January 2021).
- Cech, D.J.; Martin, S.T. Chapter 5—Evaluation of Function, Activity. In Functional Movement Development Across the Life Span, 3rd ed.; W.B. Saunders: Saint Louis, MI, USA, 2012; pp. 88–104. [Google Scholar] [CrossRef]
- Kuliese, M.; Jancoriene, L.; Grimalauskaite, R.; Zablockiene, B.; Damuleviciene, G.; Velyvyte, D.; Lesauskaite, V.; Ambrozaitis, A.; Mickiene, A.; Gefenaite, G. Seasonal Influenza Vaccine Effectiveness against Laboratory-Confirmed Influenza in 2015–2016: A Hospital-Based Test-Negative Case-Control Study in Lithuania. BMJ Open 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- Republic of Lithuania. Law Amending Law No VIII-1679 on Ethics of Biomedical Research. Available online: https://e-seimas.lrs.lt/portal/legalAct/lt/TAD/76582f93e9c811e59b76f36d7fa634f8?jfwid=181l7lijfh (accessed on 3 May 2021).
- World Medical Association. Declaration of Helsinki, Ethical Principles for Scientific Requirements and Research Protocols. Available online: https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/ (accessed on 3 May 2021).
- Broberg, E.; Melidou, A.; Prosenc, K.; Bragstad, K.; Hungnes, O. Region, on behalf of the WHO European Region and the European Influenza Surveillance Network members of the reporting countries. Predominance of Influenza A(H1N1)Pdm09 Virus Genetic Subclade 6B.1 and Influenza B/Victoria Lineage Viruses at the Start of the 2015/16 Influenza Season in Europe. Eur. Surveill 2016, 21. [Google Scholar] [CrossRef]
- Melidou, A.; Hungnes, O.; Pereyaslov, D.; Adlhoch, C.; Segaloff, H.; Robesyn, E.; Penttinen, P.; Olsen, S.J. Predominance of Influenza Virus A(H3N2) 3C.2a1b and A(H1N1)Pdm09 6B.1A5A Genetic Subclades in the WHO European Region, 2018–2019. Vaccine 2020, 38, 5707–5717. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Chung, J.; Smith, E.R.; Talbot, H.K.; Trabue, C.H.; Zimmerman, R.K.; Silveira, F.P.; Gaglani, M.; Murthy, K.; Monto, A.S.; et al. Influenza Vaccine Effectiveness in Inpatient and Outpatient Settings in the United States, 2015–2018. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020. [Google Scholar] [CrossRef]
- Stuurman, A.L.; Bollaerts, K.; Alexandridou, M.; Biccler, J.; Díez Domingo, J.; Nohynek, H.; Rizzo, C.; Turunen, T.; Riera-Montes, M. Vaccine Effectiveness against Laboratory-Confirmed Influenza in Europe—Results from the DRIVE Network during Season 2018/19. Vaccine 2020, 38, 6455–6463. [Google Scholar] [CrossRef]
- Castilla, J.; Portillo, M.E.; Casado, I.; Pozo, F.; Navascués, A.; Adelantado, M.; Gómez Ibáñez, C.; Ezpeleta, C.; Martínez-Baz, I. Effectiveness of the Current and Prior Influenza Vaccinations in Northern Spain, 2018–2019. Vaccine 2020, 38, 1925–1932. [Google Scholar] [CrossRef]
- Puig-Barbera, J.; Guglieri-Lopez, B.; Tortajada-Girbes, M.; Lopez-Labrador, F.X.; Carballido-Fernandez, M.; Mollar-Maseres, J.; Schwarz-Chavarri, G.; Baselga-Moreno, V.; Mira-Iglesias, A.; Diez-Domingo, J. Low Influenza Vaccine Effectiveness and the Effect of Previous Vaccination in Preventing Admission with A(H1N1)Pdm09 or B/Victoria-Lineage in Patients 60 Years Old or Older during the 2015/2016 Influenza Season. Vaccine 2017, 35, 7331–7338. [Google Scholar] [CrossRef]
- Davies, J.R.; Grilli, E.A. Natural or Vaccine-Induced Antibody as a Predictor of Immunity in the Face of Natural Challenge with Influenza Viruses. Epidemiol. Infect. 1989, 102, 325–333. [Google Scholar] [CrossRef] [PubMed]
- European Centre for Disease Prevention and Control. Influenza Virus Characterisation, Summary Europe, 2017; Stockholm. 2017. Available online: https://www.ecdc.europa.eu/en/publications-data/influenza-virus-characterisation-summary-europe-july-2017#no-link (accessed on 26 January 2021).
- Melidou, A.; Broberg, E. Predominance of Influenza A(H3N2) Virus Genetic Subclade 3C.2a1 during an Early 2016/17 Influenza Season in Europe—Contribution of Surveillance Data from World Health Organization (WHO) European Region to the WHO Vaccine Composition Consultation for No. Vaccine 2017, 35, 4828–4835. [Google Scholar] [CrossRef] [PubMed]
- Trebbien, R.; Fischer, T.K.; Krause, T.G.; Nielsen, L.; Nielsen, X.C.; Weinreich, L.S.; Lis-Tønder, J.; Skov, M.N.; Christiansen, C.B.; Emborg, H.-D. Changes in Genetically Drifted H3N2 Influenza A Viruses and Vaccine Effectiveness in Adults 65 Years and Older during the 2016/17 Season in Denmark. J. Clin. Virol. 2017, 94, 1–7. [Google Scholar] [CrossRef]
- Castilla, J.; Martinez-Baz, I.; Navascues, A.; Casado, I.; Aguinaga, A.; Diaz-Gonzalez, J.; Delfrade, J.; Guevara, M.; Ezpeleta, C. Comparison of Influenza Vaccine Effectiveness in Preventing Outpatient and Inpatient Influenza Cases in Older Adults, Northern Spain, 2010/11 to 2015/16. Eur. Surveill. Bull. Eur. Sur Les Mal. Transm. Eur. Commun. Dis. Bull. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Mira-Iglesias, A.; López-Labrador, F.X.; Guglieri-López, B.; Tortajada-Girbés, M.; Baselga-Moreno, V.; Cano, L.; Mollar-Maseres, J.; Carballido-Fernández, M.; Schwarz-Chavarri, G.; Díez-Domingo, J.; et al. Influenza Vaccine Effectiveness in Preventing Hospitalisation of Individuals 60 Years of Age and over with Laboratory-Confirmed Influenza, Valencia Region, Spain, Influenza Season 2016/17. Eur. Surveill. Bull. Eur. Sur Les Mal. Transm. Eur. Commun. Dis. Bull. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Rizzo, C.; Gesualdo, F.; Loconsole, D.; Pandolfi, E.; Bella, A.; Orsi, A.; Guarona, G.; Panatto, D.; Icardi, G.; Napoli, C.; et al. Moderate Vaccine Effectiveness against Severe Acute Respiratory Infection Caused by A(H1N1)Pdm09 Influenza Virus and No Effectiveness against A(H3N2) Influenza Virus in the 2018/2019 Season in Italy. Vaccines 2020, 8. [Google Scholar] [CrossRef]
- Wu, N.C.; Zost, S.J.; Thompson, A.J.; Oyen, D.; Nycholat, C.M.; McBride, R.; Paulson, J.C.; Hensley, S.E.; Wilson, I.A. A Structural Explanation for the Low Effectiveness of the Seasonal Influenza H3N2 Vaccine. PLoS Pathog. 2017, 13, e1006682. [Google Scholar] [CrossRef]
- Gherasim, A.; Martinez-Baz, I.; Castilla, J.; Pozo, F.; Larrauri, A. Effect of Previous and Current Vaccination against Influenza A(H1N1)Pdm09, A(H3N2), and B during the Post-Pandemic Period 2010–2016 in Spain. PLoS ONE 2017, 12, e0179160. [Google Scholar] [CrossRef] [PubMed]
- McLean, H.Q.; Thompson, M.G.; Sundaram, M.E.; Meece, J.K.; McClure, D.L.; Friedrich, T.C.; Belongia, E.A. Impact of Repeated Vaccination on Vaccine Effectiveness against Influenza A(H3N2) and B during 8 Seasons. Clin. Infect. Dis. 2014, 59, 1375–1385. [Google Scholar] [CrossRef]
- Castilla, J.; Navascués, A.; Casado, I.; Pérez-García, A.; Aguinaga, A.; Ezpeleta, G.; Pozo, F.; Ezpeleta, C.; Martínez-Baz, I. Interim Effectiveness of Trivalent Influenza Vaccine in a Season Dominated by Lineage Mismatched Influenza B, Northern Spain, 2017/18. Eur. Surveill. Bull. Eur. Sur Les Mal. Transm. Eur. Commun. Dis. Bull. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Chan, Y.D.; Wong, M.; Au, K.; Chuang, S. Seasonal Influenza Vaccine Effectiveness at Primary Care Level, Hong Kong SAR, 2017/2018 Winter. Hum. Vaccin. Immunother. 2019, 15, 97–101. [Google Scholar] [CrossRef]
- Rolfes, M.A.; Flannery, B.; Chung, J.R.; O’Halloran, A.; Garg, S.; Belongia, E.A.; Gaglani, M.; Zimmerman, R.K.; Jackson, M.L.; Monto, A.S.; et al. Effects of Influenza Vaccination in the United States During the 2017-2018 Influenza Season. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2019, 69, 1845–1853. [Google Scholar] [CrossRef] [PubMed]
- Pebody, R.; Djennad, A.; Ellis, J.; Andrews, N.; Marques, D.F.P.; Cottrell, S.; Reynolds, A.J.; Gunson, R.; Galiano, M.; Hoschler, K.; et al. End of Season Influenza Vaccine Effectiveness in Adults and Children in the United Kingdom in 2017/18. Eur. Surveill. Bull. Eur. Sur Les Mal. Transm. Eur. Commun. Dis. Bull. 2019, 24. [Google Scholar] [CrossRef]
- European Centre for Disease Prevention and Control. Influenza in Europe, Summary of the Season 2017–2018. Available online: https://www.ecdc.europa.eu/en/seasonal-influenza/season-2017-18 (accessed on 8 February 2021).
- Adlhoch, C.; Snacken, R.; Melidou, A.; Ionescu, S.; Penttinen, P. Dominant Influenza A(H3N2) and B/Yamagata Virus Circulation in EU/EEA, 2016/17 and 2017/18 Seasons, Respectively. Eur. Surveill. Bull. Eur. Sur Les Mal. Transm. Eur. Commun. Dis. Bull. 2018, 23. [Google Scholar] [CrossRef] [PubMed]
- Skowronski, D.M.; Chambers, C.; De Serres, G.; Sabaiduc, S.; Winter, A.-L.; Dickinson, J.A.; Gubbay, J.B.; Drews, S.J.; Fonseca, K.; Charest, H.; et al. Vaccine Effectiveness Against Lineage-Matched and -Mismatched Influenza B Viruses Across 8 Seasons in Canada, 2010-2011 to 2017–2018. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2019, 68, 1754–1757. [Google Scholar] [CrossRef]
- McLean, H.Q.; Thompson, M.G.; Sundaram, M.E.; Kieke, B.A.; Gaglani, M.; Murthy, K.; Piedra, P.A.; Zimmerman, R.K.; Nowalk, M.P.; Raviotta, J.M.; et al. Influenza Vaccine Effectiveness in the United States during 2012–2013: Variable Protection by Age and Virus Type. J. Infect. Dis. 2015, 211, 1529–1540. [Google Scholar] [CrossRef]
- Tricco, A.C.; Chit, A.; Soobiah, C.; Hallett, D.; Meier, G.; Chen, M.H.; Tashkandi, M.; Bauch, C.T.; Loeb, M. Comparing Influenza Vaccine Efficacy against Mismatched and Matched Strains: A Systematic Review and Meta-Analysis. BMC Med. 2013, 11, 153. [Google Scholar] [CrossRef] [PubMed]
- Esposito, S.; Bonanni, P.; Maggi, S.; Tan, L.; Ansaldi, F.; Lopalco, P.L.; Dagan, R.; Michel, J.-P.; van Damme, P.; Gaillat, J.; et al. Recommended Immunization Schedules for Adults: Clinical Practice Guidelines by the Escmid Vaccine Study Group (EVASG), European Geriatric Medicine Society (EUGMS) and the World Association for Infectious Diseases and Immunological Disorders (WAidid). Hum. Vaccin. Immunother. 2016, 5515, 1–18. [Google Scholar] [CrossRef] [PubMed]
- Reber, A.J.; Chirkova, T.; Kim, J.H.; Cao, W.; Biber, R.; Shay, D.K.; Sambhara, S. Immunosenescence and Challenges of Vaccination against Influenza in the Aging Population. Aging Dis. 2012, 3, 68–90. [Google Scholar]
- DiazGranados, C.A.; Dunning, A.J.; Kimmel, M.; Kirby, D.; Treanor, J.; Collins, A.; Pollak, R.; Christoff, J.; Earl, J.; Landolfi, V.; et al. Efficacy of High-Dose versus Standard-Dose Influenza Vaccine in Older Adults. N. Engl. J. Med. 2014, 371, 635–645. [Google Scholar] [CrossRef]
- Darvishian, M.; van den Heuvel, E.R.; Bissielo, A.; Castilla, J.; Cohen, C.; Englund, H.; Gefenaite, G.; Huang, W.-T.; la Bastide-van Gemert, S.; Martinez-Baz, I.; et al. Effectiveness of Seasonal Influenza Vaccination in Community-Dwelling Elderly People: An Individual Participant Data Meta-Analysis of Test-Negative Design Case-Control Studies. Lancet. Respir. Med. 2017, 5, 200–211. [Google Scholar] [CrossRef]
- Russell, K.; Chung, J.R.; Monto, A.S.; Martin, E.T.; Belongia, E.A.; McLean, H.Q.; Gaglani, M.; Murthy, K.; Zimmerman, R.K.; Nowalk, M.P.; et al. Influenza Vaccine Effectiveness in Older Adults Compared with Younger Adults over Five Seasons. Vaccine 2018, 36, 1272–1278. [Google Scholar] [CrossRef] [PubMed]
- Suess, T.; Remschmidt, C.; Schink, S.B.; Schweiger, B.; Heider, A.; Milde, J.; Nitsche, A.; Schroeder, K.; Doellinger, J.; Braun, C.; et al. Comparison of Shedding Characteristics of Seasonal Influenza Virus (Sub)Types and Influenza A(H1N1)Pdm09; Germany, 2007–2011. PLoS ONE 2012, 7, 2007–2011. [Google Scholar] [CrossRef]
- Khoury, J.; Szwarcwort, M.; Kra-Oz, Z.; Saffuri, M.; Seh, K.; Yahalomi, T.; Braun, E.; Azzam, Z.S.; Paul, M.; Neuberger, A. Duration of Viral Shedding and Factors Associated with Prolonged Shedding among Inpatients with Influenza Treated with Oseltamivir: A Prospective Cohort Study. Eur. J. Clin. Microbiol. Infect. Dis. Off. Publ. Eur. Soc. Clin. Microbiol. 2018, 37, 319–323. [Google Scholar] [CrossRef]
- De Serres, G.; Skowronski, D.M.; Wu, X.W.; Ambrose, C.S. The Test-Negative Design: Validity, Accuracy and Precision of Vaccine Efficacy Estimates Compared to the Gold Standard of Randomised Placebo-Controlled Clinical Trials. Eur. Surveill. 2013, 18, 20585. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.G.; Feng, S.; Cowling, B.J. Potential of the Test-Negative Design for Measuring Influenza Vaccine Effectiveness: A Systematic Review. Expert Rev. Vaccines 2014, 13, 1571–1591. [Google Scholar] [CrossRef] [PubMed]
- Foppa, I.M.; Haber, M.; Ferdinands, J.M.; Shay, D.K. The Case Test-Negative Design for Studies of the Effectiveness of Influenza Vaccine. Vaccine 2013, 31, 3104–3109. [Google Scholar] [CrossRef] [PubMed]

| Influenza Season | Vaccine Composition | Vaccine Type |
|---|---|---|
| 2015–2016 | - California/7/2009(H1N1)-like - A/Switzerland/9715293/2013(H3N2)-like - B/Phuket/3073/2013-like (B/Yamagata lineage) | Trivalent inactivated influenza vaccine, non-adjuvanted |
| 2016–2017 | - California/7/2009(H1N1)-like - A/Hong Kong/4801/2014(H3N2)-like - B/Brisbane/60/2008-like (B/Victoria lineage) | Trivalent inactivated influenza vaccine, non-adjuvanted |
| 2017–2018 | - A/Michigan/45/2015 (H1N1)pdm09-like - A/Hong Kong/4801/2014 (H3N2)-like - B/Brisbane/60/2008-like (B/Victoria lineage) | Trivalent inactivated influenza vaccine, non-adjuvanted |
| 2018–2019 | - A/Michigan/45/2015 (H1N1)pdm09-like - A/Singapore/INFIMH-16-0019/2016 (H3N2)-like - B/Colorado/06/2017-like (B/Victoria/2/87-lineage) | Trivalent inactivated influenza vaccine, non-adjuvanted |
| Influenza Season | Controls | A(H1N1pdm09) | A(H3N2) | A (Untyped) | B/Yamagata | B/Victoria | B (Untyped) |
|---|---|---|---|---|---|---|---|
| N (%) | N (%) | N (%) | N (%) | N (%) | N (%) | N(%) | |
| Season 2015–2016 | 91 (55.8) | 50 (30.7) | – | 14 (8.6) | – | 7 (4.3) | 1 (0.6) |
| Season 2016–2017 | 104 (53.9) | – | 83 (54.6) | – | 5 (2.6) | – | 1 (0.5) |
| Season 2017–2018 | 91 (42.9) | 5 (2.4) | 8 (3.8) | 2 (0.9) | 97 (45.8) | 2 (0.9) | 7 (3.3) |
| Season 2018–2019 | 81 (46.6) | 29 (16.7) | 61 (35.1) | 3 (1.7) | – | – | – |
| All seasons | 367 (49.5) | 84 (11.3) | 152 (20.5) | 19 (2.6) | 102 (13.7) | 9 (1.2) | 9 (1.2) |
| Variables | Age Group 18–64 | p-Value | Age Group ≥65 | p-Value | ||
|---|---|---|---|---|---|---|
| Influenza-Positive N = 121 (40.1%) | Influenza-Negative N = 81 (59.9%) | Influenza-Positive N = 254 (47.0%) | Influenza-Negative N = 286 (53.0%) | |||
| Influenza season | ||||||
| Season 2015–2016 | 40 (33.1) | 31 (38.3) | 0.057 a | 32 (12.6) | 60 (21.0) | 0.052 a |
| Season 2016–2017 | 17 (14.0) | 21 (25.9) | 72 (28.3) | 83 (29.0) | ||
| Season 2017–2018 | 38 (31.4) | 15 (18.5) | 83 (32.7) | 76 (26.6) | ||
| Season 2018–2019 | 26 (21.5) | 14 (17.3) | 67 (26.4) | 67 (23.4) | ||
| Male | 61 (50.4) | 40 (49.4) | 0.886 a | 108 (42.5) | 131 (45.8) | 0.443 a |
| Urban | 84 (69.4) | 51 (75.3) | 0.362 a | 195 (76.8) | 237 (82.9) | 0.077 a |
| Age (median, min; max) | 54.0 (19; 64) | 54.0 (21; 64) | 0.692 d | 77.0 (65; 96) | 76.0 (65; 92) | 0.274 d |
| Education | ||||||
| High (college, university) | 57 (47.9) | 34 (42.5) | 0.453 a | 59 (23.4) | 64 (22.4) | 0.775 a |
| Low (primary, unfinished, secondary, professional) | 62 (52.1) | 46 (57.5) | 193 (76.6) | 222 (77.6) | ||
| Occupation | ||||||
| Intellectual or/and physical work | 62 (51.2) | 46 (56.8) | 0.438 a | 18 (7.1) | 15 (5.2) | 0.372 a |
| Retired/handicapped/jobless | 59 (48.8) | 35 (43.2) | 236 (92.9) | 271 (94.8) | ||
| Smoking | ||||||
| Never | 50 (41.3) | 35 (43.2) | 0.512 a | 172 (68.0) | 185 (64.7) | 0.447 a |
| Former | 31 (25.6) | 25 (30.9) | 60 (23.7) | 81 (28.3) | ||
| Current | 40 (33.1) | 21 (25.9) | 21 (8.3) | 20 (7.0) | ||
| Pregnant | 17 (14.0) | 4 (4.9) | 0.038 a | – | – | – |
| Chronic condition (at least 1) | 109 (90.1) | 77 (95.1) | 0.199 a | 221 (87.0) | 269 (94.1) | 0.005 a |
| At least one hospitalization due to exacerbation of underlying conditions in the previous 12 months | 22 (18.3) | 22 (27.2) | 0.138 a | 62 (24.6) | 123 (43.0) | <0.001 a |
| Cardiovascular diseases | 37 (30.6) | 37 (45.7) | 0.029 a | 167 (65.7) | 223 (78.0) | 0.002 a |
| Lung diseases | 29 (24.0) | 25 (30.9) | 0.278 a | 52 (20.5) | 87 (30.4) | 0.008 a |
| Endocrine diseases, diabetes | 23 (19.0) | 17 (21.0) | 0.729 a | 46 (18.1) | 58 (20.3) | 0.523 a |
| Renal diseases | 6 (5.0) | 2 (2.5) | 0.480 b | 27 (10.6) | 43 (15.0) | 0.128 a |
| Immunodeficiency and transplantations | 12 (9.9) | 6 (7.4) | 0.539 a | 5 (2.0) | 2 (0.7) | 0.262 b |
| Rheumatologic diseases | 6 (5.0) | 2 (2.5) | 0.480 b | 8 (3.1) | 9 (3.1) | 0.999 a |
| Dementia, stroke | 4 (3.3) | 9 (11.1) | 0.027 a | 63 (24.8) | 81 (28.3) | 0.356 a |
| Hematologic cancer | 7 (5.8) | 1 (1.2) | 0.148 b | 7 (2.8) | 9 (3.1) | 0.789 a |
| Non-hematologic cancer | 14 (11.6) | 7 (8.6) | 0.504 a | 36 (14.2) | 39 (13.6) | 0.857 a |
| Anemia, spleen pathology | 12 (9.9) | 6 (7.4) | 0.539 a | 15 (5.9) | 29 (10.1) | 0.073 a |
| Cirrhosis | 2 (1.7) | 4 (4.9) | 0.221 b | 5 (2.0) | 2 (0.7) | 0.262 b |
| Nutritional deficiency | 4 (3.3) | 0 (0.0) | 0.151 b | 6 (2.4) | 17 (5.9) | 0.040 a |
| Obesity | 38 (31.4) | 37 (45.7) | 0.040 a | 80 (31.5) | 87 (30.4) | 0.787 a |
| BMI (median, min; max) | 26.3 (17.3; 51.7) | 29.2 (18.7; 45.2) | 0.020 d | 27.4 (17.3; 43.0) | 27.8 (15.9; 50.0) | 0.468 d |
| Any antiviral use | 114 (94.2) | 48 (59.3) | <0.001 a | 204 (80.3) | 108 (37.8) | <0.001 a |
| Statin use | 8 (12.5) | 2 (6.9) | 0.419 a | 18 (12.0) | 13 (9.0) | 0.418 a |
| Other respiratory virus detected | 5 (4.1) | 14 (17.7) | 0.001 a | 6 (2.4) | 56 (19.6) | <0.001 a |
| SIV in current season | 4 (3.3) | 9 (11.1) | 0.027 a | 26 (10.2) | 42 (14.7) | 0.120 a |
| SIV in previous season | 2 (1.7) | 8 (10.1) | 0.008 a | 20 (7.9) | 30 (10.5) | 0.309 a |
| Transfer to the intensive-care unit | 10 (8.3) | 2 (2.5) | 0.088 a | 13 (5.1) | 10 (3.5) | 0.352 a |
| Length of hospitalization (mean, SD) | 6.5 (5.0) | 6.7 (3.2) | 0.721 c | 7.7 (3.9) | 9.8 (5.1) | <0.001 c |
| Barthel score before the SARI hospitalization (mean, SD) | 99.8 (1.6) | 96.3 (15.6) | 0.051 c | 94.3 (17.1) | 92.7 (16.4) | 0.267 c |
| Days between the SARI onset and swab (median, min; max) | 4.0 (0; 7) | 4.0 (0; 7) | 0.910 d | 4.0 (0; 7) | 4.0 (0; 7) | 0.126 d |
| Days between antivirals use and swab | ||||||
| 0 days | 36 (31.6) | 13 (27.1) | 0.191 a | 64 (31.4) | 26 (24.1) | 0.180 a |
| 1 day | 61 (53.5) | 22 (45.8) | 111 (54.4) | 59 (54.6) | ||
| 2 and more days | 17 (14.9) | 13 (27.1) | 29 (14.2) | 23 (21.3) | ||
| Deaths | 4 (3.3) | 0 (0.0) | 0.151 b | 4 (1.6) | 7 (2.4) | 0.474 a |
| Influenza-Positive | Influenza-Negative | Unadjusted SIVE% (95% CI) | p-Value of the Unadjusted Model | Adjusted SIVE% (95% CI) | p-Value of the Adjusted Model | R Square of the Adjusted Model | |
|---|---|---|---|---|---|---|---|
| Vaccinated/Total (%) | Vaccinated/Total (%) | ||||||
| Any influenza | |||||||
| Age 18–64 years | 4/121 (3.3) | 9/81 (11.1) | 72.7 (7.9 to 91.9) | 0.036 | 71.9 a (−1.9 to 92.2) | 0.053 | 0.090 |
| Age ≥ 65 years | 26/254 (10.2) | 42/286 (14.7) | 33.8 (−11.6 to 60.7) | 0.122 | 26.9 b (−24.4 to 57.0) | 0.249 | 0.043 |
| Influenza A | |||||||
| Age 18–64 years | 3/83 (3.6) | 9/81 (11.1) | 70.0 (−15.1 to 92.2) | 0.079 | 78.0 c (1.7 to 95.1) | 0.047 | 0.150 |
| Age ≥ 65 years | 23/173 (13.3) | 42/286 (14.7) | 10.9 (−54.0 to 48.5) | 0.679 | 22.6 d (−36.5 to 56.1) | 0.376 | 0.127 |
| Influenza A(H1N1)pdm09 | |||||||
| Age 18–64 years | 1/51 (2.0) | 9/81 (11.1) | 84.0 (−30.3 to 98.0) | 0.087 | 88.6 e (−47.4 to 99.1) | 0.096 | 0.141 |
| Age ≥ 65 years | 3/34 (8.8) | 42/286 (14.7) | 43.8 (−92.2 to 83.6) | 0.359 | N/A | N/A | N/A |
| Influenza A(H3N2) | |||||||
| Age 18–64 years | 2/31 (6.5) | 9/81 (11.1) | 44.8 (−171.0 to 88.8) | 0.464 | N/A | N/A | N/A |
| Age ≥ 65 years | 17/121 (14.0) | 42/286 (14.7) | 5.0 (−74.5 to 48.3) | 0.868 | N/A | N/A | N/A |
| Influenza B | |||||||
| Age 18–64 years | 1/38 (2.6) | 9/81 (11.1) | 78.4 (−77.2 to 97.4) | 0.216 | 74.1 f (−146.8 to 97.3) | 0.240 | 0.250 |
| Age ≥ 65 years | 3/82 (3.7) | 42/286 (14.7) | 77.9 (26.9 to 93.4) | 0.013 | 75.3 g (12.2 to 93.1) | 0.030 | 0.116 |
| Influenza B/Yamagata | |||||||
| Age 18–64 years | 1/31 (3.2) | 9/81 (11.1) | 73.3 (−119.8 to 96.8) | 0.219 | 76.8 h (−109.9 to 97.4) | 0.194 | 0.183 |
| Age ≥ 65 years | 3/71 (4.2) | 42/286 (14.7) | 74.4 (14.8 to 92.3) | 0.026 | 73.1 i (3.2 to 92.5) | 0.044 | 0.093 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kuliese, M.; Mickiene, A.; Jancoriene, L.; Zablockiene, B.; Gefenaite, G.; Study Group. Age-Specific Seasonal Influenza Vaccine Effectiveness against Different Influenza Subtypes in the Hospitalized Population in Lithuania during the 2015–2019 Influenza Seasons. Vaccines 2021, 9, 455. https://doi.org/10.3390/vaccines9050455
Kuliese M, Mickiene A, Jancoriene L, Zablockiene B, Gefenaite G, Study Group. Age-Specific Seasonal Influenza Vaccine Effectiveness against Different Influenza Subtypes in the Hospitalized Population in Lithuania during the 2015–2019 Influenza Seasons. Vaccines. 2021; 9(5):455. https://doi.org/10.3390/vaccines9050455
Chicago/Turabian StyleKuliese, Monika, Aukse Mickiene, Ligita Jancoriene, Birute Zablockiene, Giedre Gefenaite, and Study Group. 2021. "Age-Specific Seasonal Influenza Vaccine Effectiveness against Different Influenza Subtypes in the Hospitalized Population in Lithuania during the 2015–2019 Influenza Seasons" Vaccines 9, no. 5: 455. https://doi.org/10.3390/vaccines9050455
APA StyleKuliese, M., Mickiene, A., Jancoriene, L., Zablockiene, B., Gefenaite, G., & Study Group. (2021). Age-Specific Seasonal Influenza Vaccine Effectiveness against Different Influenza Subtypes in the Hospitalized Population in Lithuania during the 2015–2019 Influenza Seasons. Vaccines, 9(5), 455. https://doi.org/10.3390/vaccines9050455