
Epidemiological and Clinical Observations of Gonococcal Infections in Women and Prevention Strategies

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Eligibility and Enrollment
2.2.1. Exclusion Criteria
2.2.2. Inclusion Criteria
2.3. Specimens Collected
2.4. N. gonorrhoeae Infection Diagnosis
2.5. Routine Diagnosis of Other STIs
2.6. Data Collection
2.6.1. Questionnaire
2.6.2. Clinical Parameters Examined at Enrollment
2.7. Statistical Analyses
3. Results
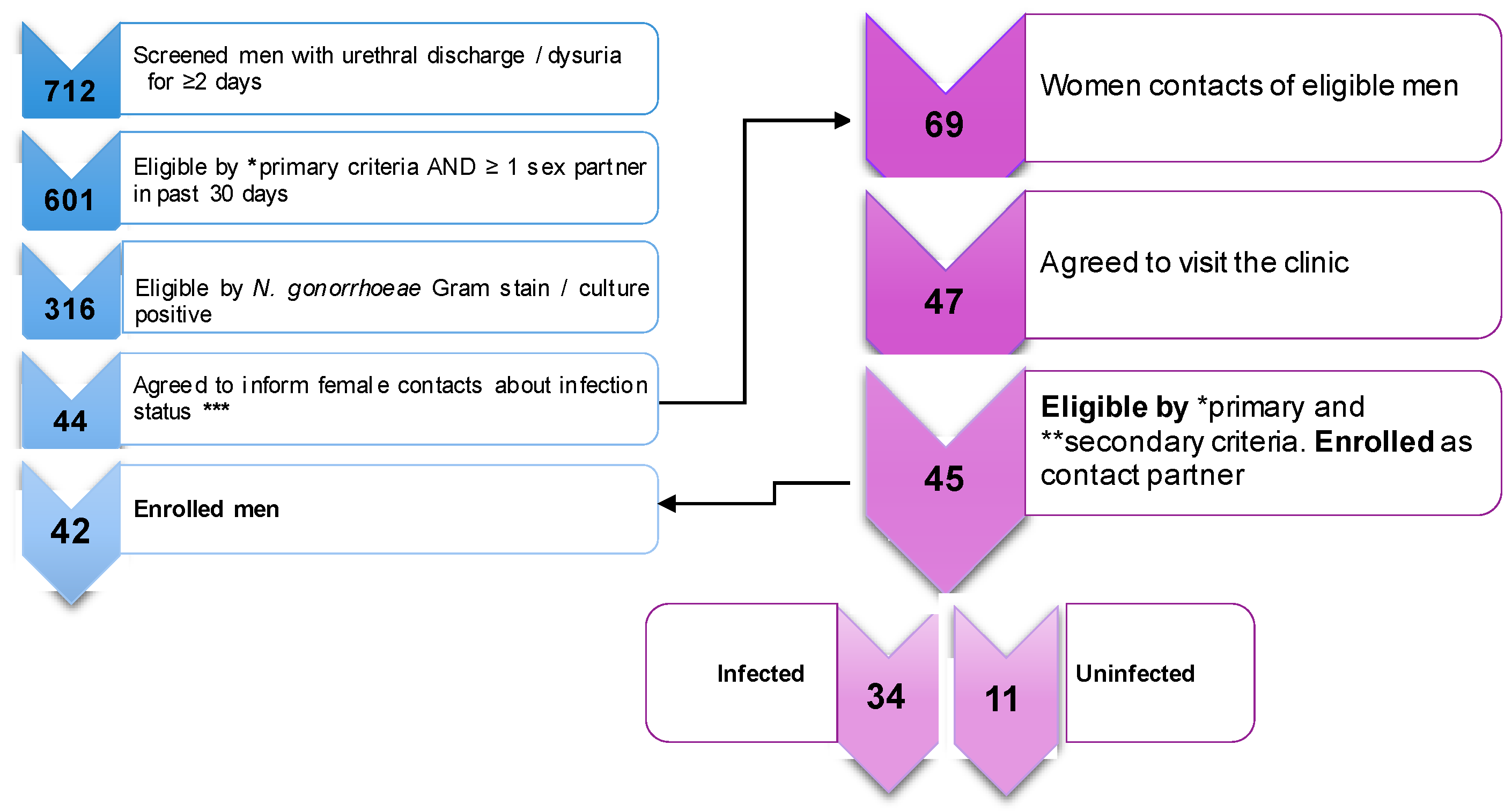
3.1. Study Cohort
3.2. Assessment of Gonococcal Infection
3.3. Epidemiology Observations from the Questionnaire
3.3.1. Demographics
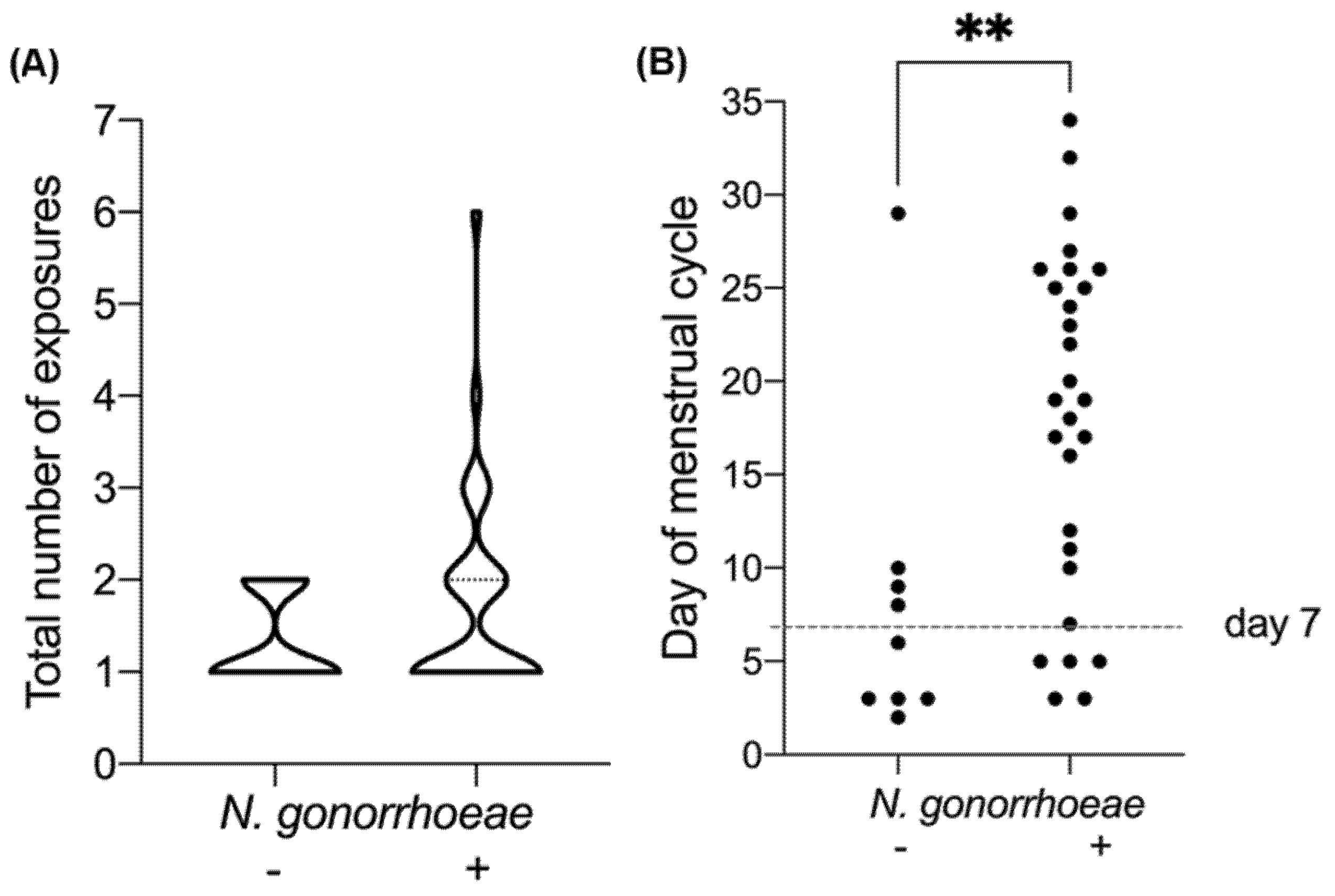
3.3.2. Chronology of N. gonorrhoeae Exposure
3.3.3. Physiological Parameters Relative to Exposure
Contraception Methods Relative to Exposure
3.3.4. Self-Reported Signs and Symptoms
3.3.5. History of STIs
3.4. Clinical Evaluation at NCSTD
3.4.1. Clinical Signs
3.4.2. Diagnosed Co-Infections
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Unemo, M.; Seifert, H.S.; Hook, E.W.; Hawkes, S.; Ndowa, F.; Dillon, J.-A.R. Gonorrhoea. Nat. Rev. Dis. Prim. 2019, 5, 1–23. [Google Scholar] [CrossRef]
- Shaughnessy, J.; Ram, S.; Rice, P.A. Biology of the Gonococcus: Disease and Pathogenesis. Methods Mol. Biol. 2019, 1997, 1–27. [Google Scholar] [CrossRef]
- Edwards, J.L.; Butler, E.K. The Pathobiology of Neisseria gonorrhoeae Lower Female Genital Tract Infection. Front. Microbiol. 2011, 2, 102. [Google Scholar] [CrossRef] [PubMed]
- CDC. Antibiotic Resistance Threats in the United States. 2019. Available online: www.cdc.gov/DrugResistance/Biggest-Threats.html (accessed on 2 December 2020).
- Russell, M.W.; Jerse, A.E.; Gray-Owen, S.D. Progress toward a Gonococcal Vaccine: The Way Forward. Front. Immunol. 2019, 10, 2417. [Google Scholar] [CrossRef]
- Wetzler, L.M.; Feavers, I.M.; Gray-Owen, S.D.; Jerse, A.E.; Rice, P.A.; Deal, C.D. Summary and Recommendations from the National Institute of Allergy and Infectious Diseases (NIAID) Workshop “Gonorrhea Vaccines: The Way Forward”. Clin. Vaccine Immunol. 2016, 23, 656–663. [Google Scholar] [CrossRef]
- Greenberg, L.; Diena, B.B.; Ashton, F.A.; Wallace, R.; Kenny, C.P.; Znamirowski, R.; Ferrari, H.; Atkinson, J. Gonococcal vaccine studies in Inuvik. Can. J. Public Health 1974, 65, 29–33. [Google Scholar] [PubMed]
- Rice, P.A.; Shafer, W.M.; Ram, S.; Jerse, A.E. Neisseria gonorrhoeae: Drug Resistance, Mouse Models, and Vaccine Development. Annu. Rev. Microbiol. 2017, 71, 665–686. [Google Scholar] [CrossRef]
- Rice, P.A.; Gulati, S.; McQuillen, D.P.; Ram, S. Is there protective immunity to gonococcal disease? In Proceedings of the 10th International Pathogenic Neisseria Conferences, Baltimore, MD, USA, 8–13 September 1996. [Google Scholar]
- Boslego, J.W.; Tramont, E.C.; Chung, R.C.; McChesney, D.G.; Ciak, J.; Sadoff, J.C.; Piziak, M.V.; Brown, J.D.; Brintonjr, C.; Wood, S.W. Efficacy trial of a parenteral gonococcal pilus vaccine in men. Vaccine 1991, 9, 154–162. [Google Scholar] [CrossRef]
- Hobbs, M.M.; Sparling, P.F.; Cohen, M.S.; Shafer, W.M.; Deal, C.D.; Jerse, A.E. Experimental Gonococcal Infection in Male Volunteers: Cumulative Experience with Neisseria gonorrhoeae Strains FA1090 and MS11mkC. Front. Microbiol. 2011, 2, 123. [Google Scholar] [CrossRef]
- Li, Y.; Su, X.; Le, W.; Li, S.; Yang, Z.; Chaisson, C.; Madico, G.; Gong, X.; Reed, G.W.; Wang, B.; et al. Mycoplasma genitalium in Symptomatic Male Urethritis: Macrolide Use Is Associated with Increased Resistance. Clin. Infect. Dis. 2020, 70, 805–810. [Google Scholar] [CrossRef] [PubMed]
- Coleman, J.S.; Gaydos, C.A. Molecular Diagnosis of Bacterial Vaginosis: An Update. J. Clin. Microbiol. 2018, 56. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Epi Info 7.2.; Centers for Disease Control and Prevention: Atlanta, GA, USA, 2019.
- Ayinde, O.; Tan, W.; Hepburn, T.; Ross, J.D.C. Factors associated with time to presentation for individuals with symptomatic uncomplicated genital gonorrhoea: A cross sectional cohort study of GToG trial participants. Sex. Transm. Infect. 2020, 96, 251–257. [Google Scholar] [CrossRef]
- McLaughlin, S.E.; Ghanem, K.G.; Zenilman, J.M.; Griffiss, J.M. Risk of Gonococcal Infection during Vaginal Exposure is Associated with High Vaginal pH and Active Menstruation. Sex. Transm. Dis. 2019, 46, 86–90. [Google Scholar] [CrossRef]
- Platt, R.; Rice, P.A.; McCormack, W.M. Risk of Acquiring Gonorrhea and Prevalence of Abnormal Adnexal Findings Among Women Recently Exposed to Gonorrhea. JAMA 1983, 250, 3205–3209. [Google Scholar] [CrossRef]
- Lycke, E.; Lowhagen, G.-B.; Hallhagen, G.; Johannisson, G.; Ramstedt, K. The Risk of Transmission of Genital Chlamydia trachomatis Infection Is Less than That of Genital Neisseria gonorrhoeae Infection. Sex. Transm. Dis. 1980, 7, 6–10. [Google Scholar] [CrossRef]
- Lin, J.L.; Donegan, S.P.; Heeren, T.C.; Greenberg, M.; Flaherty, E.E.; Haivanis, R.; Su, X.; Dean, D.; Newhall, W.J.; Knapp, J.S.; et al. Transmission of Chlamydia trachomatis and Neisseria gonorrhoeae among Men with Urethritis and Their Female Sex Partners. J. Infect. Dis. 1998, 178, 1707–1712. [Google Scholar] [CrossRef]
- Chang, S.-X.; Chen, K.-K.; Liu, X.-T.; Xia, N.; Xiong, P.-S.; Cai, Y.-M. Cross-sectional study of asymptomatic Neisseria gonorrhoeae and Chlamydia trachomatis infections in sexually transmitted disease related clinics in Shenzhen, China. PLoS ONE 2020, 15, e0234261. [Google Scholar] [CrossRef] [PubMed]
- CDC. Sexually Transmitted Disease Surveillance 2018; U.S. Department of Health and Human Services: Atlanta, GA, USA, 2019.
- ECDC. Gonorrhoea. In Annual Epidemiological Report for 2018; ECDC: Stockholm, Sweden, 2020. [Google Scholar]
- Ravel, J.; Brotman, R.M.; Gajer, P.; Ma, B.; Nandy, M.; Fadrosh, D.W.; Sakamoto, J.; Koenig, S.S.; Fu, L.; Zhou, X.; et al. Daily temporal dynamics of vaginal microbiota before, during and after episodes of bacterial vaginosis. Microbiome 2013, 1, 29. [Google Scholar] [CrossRef] [PubMed]
- McLaughlin, S.E.; Griffiss, J.M. How to Identify Exposed Women Who Are Infected with Neisseria gonorrhoeae. Breast Cancer 2019, 1997, 29–36. [Google Scholar] [CrossRef]
- Brabin, L. Hormonal markers of susceptibility to sexually transmitted infections: Are we taking them seriously? BMJ 2001, 323, 394–395. [Google Scholar] [CrossRef][Green Version]
- Berger, G.S.; Keith, L.; Moss, W. Prevalence of gonorrhoea among women using various methods of contraception. Sex. Transm. Infect. 1975, 51, 307–309. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Gursahaney, P.R.; Meyn, L.A.; Hillier, S.L.; Sweet, R.L.; Wiesenfeld, H.C. Combined Hormonal Contraception May Be Protective Against Neisseria gonorrhoeae Infection. Sex. Transm. Dis. 2010, 37, 356–360. [Google Scholar] [CrossRef]
- Hook, E.W. Gender Differences in Risk for Sexually Transmitted Diseases. Am. J. Med. Sci. 2012, 343, 10–11. [Google Scholar] [CrossRef]
- Johnson, M.B.; Criss, A.K. Resistance of Neisseria Gonorrhoeae to Neutrophils. Front. Microbiol. 2011, 2, 77. [Google Scholar] [CrossRef] [PubMed]
- Workowski, K.A.; Bolan, G.A. Sexually transmitted diseases treatment guidelines, 2015. MMWR. Recomm. Rep. 2015, 64, 1–137. [Google Scholar]
- Plummer, E.L.; Vodstrcil, L.A.; Bodiyabadu, K.; Murray, G.L.; Doyle, M.; Latimer, R.L.; Fairley, C.K.; Payne, M.; Chow, E.P.F.; Garland, S.M.; et al. Are Mycoplasma hominis, Ureaplasma urealyticum and Ureaplasma parvum associated with specific genital symptoms and clinical signs in non-pregnant women? Clin. Infect. Dis. 2021, ciab061. [Google Scholar] [CrossRef] [PubMed]
- Bautista, C.T.; Wurapa, E.; Sateren, W.B.; Morris, S.M.; Hollingsworth, B.P.; Sanchez, J.L. Bacterial vaginosis: A synthesis of the literature on etiology, prevalence, risk factors, and relationship with chlamydia and gonorrhea infections. Mil. Med. Res. 2016, 3, 1–10. [Google Scholar] [CrossRef]
- Viscardi, R.M. Ureaplasma species: Role in neonatal morbidities and outcomes. Arch. Dis. Child. Fetal Neonatal. Ed. 2013, 99, F87–F92. [Google Scholar] [CrossRef]
- Horner, P.; Donders, G.; Cusini, M.; Gomberg, M.; Jensen, J.; Unemo, M. Should we be testing for urogenital Mycoplasma hominis, Ureaplasma parvum and Ureaplasma urealyticum in men and women?—A position statement from the European STI Guidelines Editorial Board. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1845–1851. [Google Scholar] [CrossRef]
- Cattley, C.; Massari, P.; Genco, C.A. Incidence of Gonorrhea and Chlamydia in Urban Settings: The Case for Neighborhood Level Analysis in Boston. Adv. Infect. Dis. 2015, 5. [Google Scholar] [CrossRef][Green Version]
- Kirkcaldy, R.D.; Weston, E.; Segurado, A.C.; Hughes, G. Epidemiology of gonorrhoea: A global perspective. Sex. Health 2019, 16, 401–411. [Google Scholar] [CrossRef] [PubMed]
- Detels, R.; Green, A.M.; Klausner, J.D.; Katzenstein, D.; Gaydos, C.; Handsfield, H.H.; Pequegnat, W.; Mayer, K.; Hartwell, T.D.; Quinn, T.C. The Incidence and Correlates of Symptomatic and Asymptomatic Chlamydia trachomatis and Neisseria gonorrhoeae Infections in Selected Populations in Five Countries. Sex. Transm. Dis. 2011, 38, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Reekie, J.; Donovan, B.; Guy, R.; Hocking, J.S.; Kaldor, J.M.; Mak, D.B.; Pearson, S.; Preen, D.; Stewart, L.; Ward, J.; et al. Risk of Pelvic Inflammatory Disease in Relation to Chlamydia and Gonorrhea Testing, Repeat Testing, and Positivity: A Population-Based Cohort Study. Clin. Infect. Dis. 2018, 66, 437–443. [Google Scholar] [CrossRef] [PubMed]
- Ville, Y.; Leruez, M.; Glowaczower, E.; Robertson, J.N.; Ward, M.E. The role of Chlamydia trachomatis and Neisseria gonorrhoeae in the aetiology of ectopic pregnancy in Gabon. BJOG Int. J. Obstet. Gynaecol. 1991, 98, 1260–1266. [Google Scholar] [CrossRef]
- De Francesco, M.A.; Stefanelli, P.; Carannante, A.; Corbellini, S.; Giagulli, C.; Lorenzin, G.; Ronconi, M.; Arici, E.; Cadei, M.; Campora, R.; et al. Management of a Case of Peritonitis Due to Neisseria gonorrhoeae Infection Following Pelvic Inflammatory Disease (PID). Antibiotics 2020, 9, 193. [Google Scholar] [CrossRef] [PubMed]
- Lovett, A.; Duncan, J.A. Human Immune Responses and the Natural History of Neisseria gonorrhoeae Infection. Front. Immunol. 2019, 9, 3187. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Categories | Men | Women |
|---|---|---|
| n = 42 | n = 45 a | |
| Age | 38 (31–50) b | 32 (28–42) b |
| Marital status | ||
| Single c | 9 (19%) d | 11 (24%) d |
| Married | 33 (79%) | 34 (76%) |
| Education level e | ||
| School | 31 (74%) | 40 (89%) |
| Higher education | 11 (26%) | 5 (11%) |
| Exposure Relative to Male’s Symptoms | Exposed Women | Prevalence | OR | p-Value | |
|---|---|---|---|---|---|
| Positive a | Negative a | Positive a | (95% CI) | ||
| n = 34 b | n = 11 b | % | |||
| Prior | 26 (76%) | 8 (73%) | 76 | 1.22 (0.26–5.72) | 1.0 |
| After | 3 (9%) | 2 (18%) | 60 | 0.44 (0.63–3.02) | 0.58 |
| Prior and After | 5 (15%) | 1 (9%) | 84 | 1.72 (0.18–16.59) | 1.0 |
| Contraception a | Exposed Women | Prevalence | OR | p-Value | |
|---|---|---|---|---|---|
| Positive b | Negative b | Positive b | (95% CI) | ||
| n = 34 | n = 11 | % | |||
| None | 13 (38%) c | 4 (36%) c | 76 | 1.23 (0.3–4.99) | 1.0 |
| Condom | 6 (18%) | 2 (18%) | 75 | 0.96 (0.165–5.65) | 1.0 |
| IUD | 10 (30%) | 5 (45%) | 67 | 0.5 (0.12–2.0) | 0.46 |
| Hormone-based | |||||
| Pill | 3 (7%) | 0 | 100 | UN | 0.57 |
| Emergency | 1 (3%) | 0 | 100 | UN | 1.0 |
| Unknown | 1 (3%) | 0 | 100 | UN | 1.0 |
| Symptoms and Signs | Exposed Women | Prevalence | OR | p-Value | |
|---|---|---|---|---|---|
| Positive a | Negative a | Positive a | (95% CI) | ||
| n = 34 | n = 11 | % | |||
| Self-reported Signs and Symptoms b | 23 (68%) | 6 (55%) | 79% | ||
| Vaginal discharge | 18 (53%) c | 5 (45%) c | 78 | 1.28 (0.32–5.01) | 1.0 |
| Vaginal bleeding (other than menses) | 1 (3%) | 1 (9%) | 50 | 0.63 (0.05–7.64) | 1.0 |
| Pain | |||||
| Abdominal | 3 (9%) | 0 | 100 | UN | 0.56 |
| Urination | 6 (18%) | 2 (18%) | 75 | 0.96 (0.16–5.65) | 1.0 |
| Intercourse | 1 (3%) | 1 (9%) | 50 | 0.63 (0.05–7.64) | 1.0 |
| Sore throat | 2 (6%) | 0 | 100 | ||
| Clinical Signs d | 30 (88%) | 10 (91%) | 75% | ||
| Vaginal discharge | 30 (88%) | 9 (82%) | 76 | 1.67 (0.26–10.64) | 0.62 |
| Purulent | 16 | 4 | 80 | 1.56 (0.38–6.31) | 0.73 |
| Clear-mucoid | 6 | 4 | 60 | 0.38 (0.08–1.7) | 0.23 |
| Grey-white | 7 | 1 | 86 | 2.59 (0.28–23.8) | 0.66 |
| Curdy | 1 | 0 | 100 | UN | 1.0 |
| Cervical discharge | 27 (79%) | 9 (82%) | 74 | 0.86 (0.15–4.90) | 1.0 |
| Purulent | 20 | 6 | 77 | 1.19 (0.3–4.68) | 1.0 |
| Bloody | 3 | 0 | 100 | UN | 0.57 |
| Clear-mucoid | 2 | 2 | 50 | 0.28 (0.03–2.29) | 0.25 |
| White | 2 | 1 | 67 | 0.63 (0.05–7.64) | 1.0 |
| Cervical inflammation | 23 (68%) | 8 (73%) | 74 | 0.78 (0.17–3.55) | 1.0 |
| Moderate | 8 | 1 | 89 | 3.07 (0.33–27.86) | 0.42 |
| Minimal | 15 | 7 | 68 | 0.45 (0.11–1.83) | 0.31 |
| PMN score | 34 (100%) | 10 (91%) | |||
| None [0 cells] | 0 | 1 (9%) | 0 | UN | 0.24 |
| Low [1–4 cells] | 2 (6%) | 2 (18%) | 50 | 0.28 (0.03–2.29) | 0.25 |
| Moderate [5–9 cells] | 10 (30%) | 3 (27%) | 77 | 1.62 (0.29–8.97) | 0.70 |
| High [≥10 cells] | 22 (65%) | 5 (45%) | 81 | 1.74 (0.43–6.98) | 0.48 |
| STI b | Exposed Women | Prevalence | OR | p-Value | |
|---|---|---|---|---|---|
| Positive a | Negative a | Positive a | (95% CI) | ||
| n = 34 | n = 11 | % | |||
| C. trachomatis | 11 (33%) c | 4 (36%) c | 73 | 0.84 (0.2–3.47) | 1.0 |
| M. genitalium | 6 (18%) | 1 (9%) | 86 | UN | 1.0 |
| T. vaginalis | 2 (6%) | 2 (18%) | 50 | UN | 1.0 |
| U. urealyticum | 24 (71%) | 4 (36%) | 86 | 5.45 (0.62–47. 9) | 0.14 |
| C. albicans | 2 (6%) | 0 | 100 | UN | 1.0 |
| Bacterial vaginosis | 13 (38%) | 6 (55%) | 68 | 0.35 (0.07–1.74) | 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costa-Lourenço, A.P.R.; Su, X.; Le, W.; Yang, Z.; Patts, G.J.; Massari, P.; Genco, C.A. Epidemiological and Clinical Observations of Gonococcal Infections in Women and Prevention Strategies. Vaccines 2021, 9, 327. https://doi.org/10.3390/vaccines9040327
Costa-Lourenço APR, Su X, Le W, Yang Z, Patts GJ, Massari P, Genco CA. Epidemiological and Clinical Observations of Gonococcal Infections in Women and Prevention Strategies. Vaccines. 2021; 9(4):327. https://doi.org/10.3390/vaccines9040327
Chicago/Turabian StyleCosta-Lourenço, Ana Paula R., Xiaohong Su, Wenjing Le, Zhaoyan Yang, Gregory J. Patts, Paola Massari, and Caroline A. Genco. 2021. "Epidemiological and Clinical Observations of Gonococcal Infections in Women and Prevention Strategies" Vaccines 9, no. 4: 327. https://doi.org/10.3390/vaccines9040327
APA StyleCosta-Lourenço, A. P. R., Su, X., Le, W., Yang, Z., Patts, G. J., Massari, P., & Genco, C. A. (2021). Epidemiological and Clinical Observations of Gonococcal Infections in Women and Prevention Strategies. Vaccines, 9(4), 327. https://doi.org/10.3390/vaccines9040327