The Impact of COVID-19 and the Practical Importance of Vaccinations and Nirmatrelvir/Ritonavir for Patients with Cardiovascular Disease

 ,
,  ,
,  , , , ,
, , , ,  and
and
Abstract
1. Background
2. The Impact of COVID-19 on Death Rates
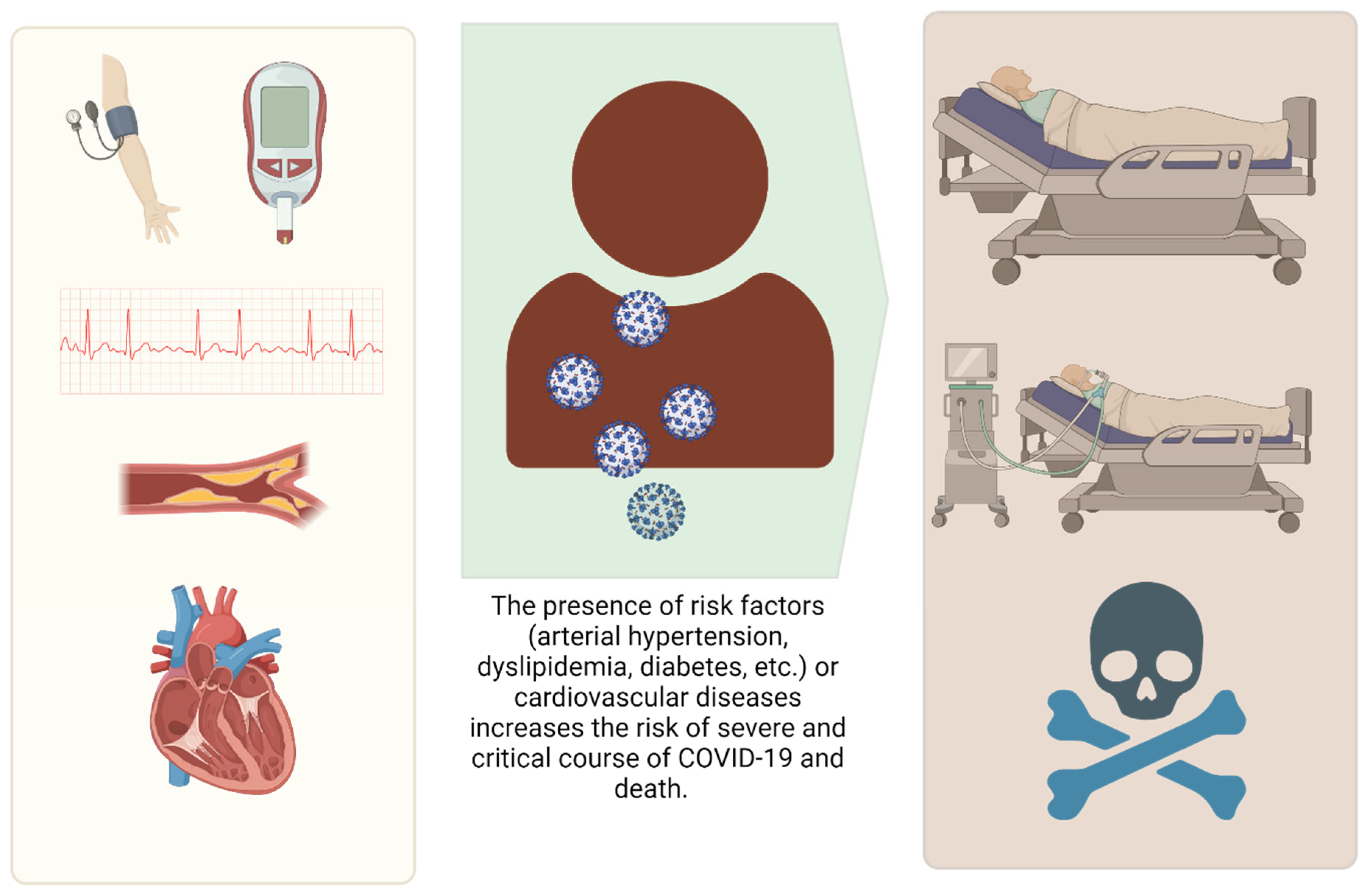
3. Cardiovascular Diseases and the Risk of Illness and a Severe Course of COVID-19
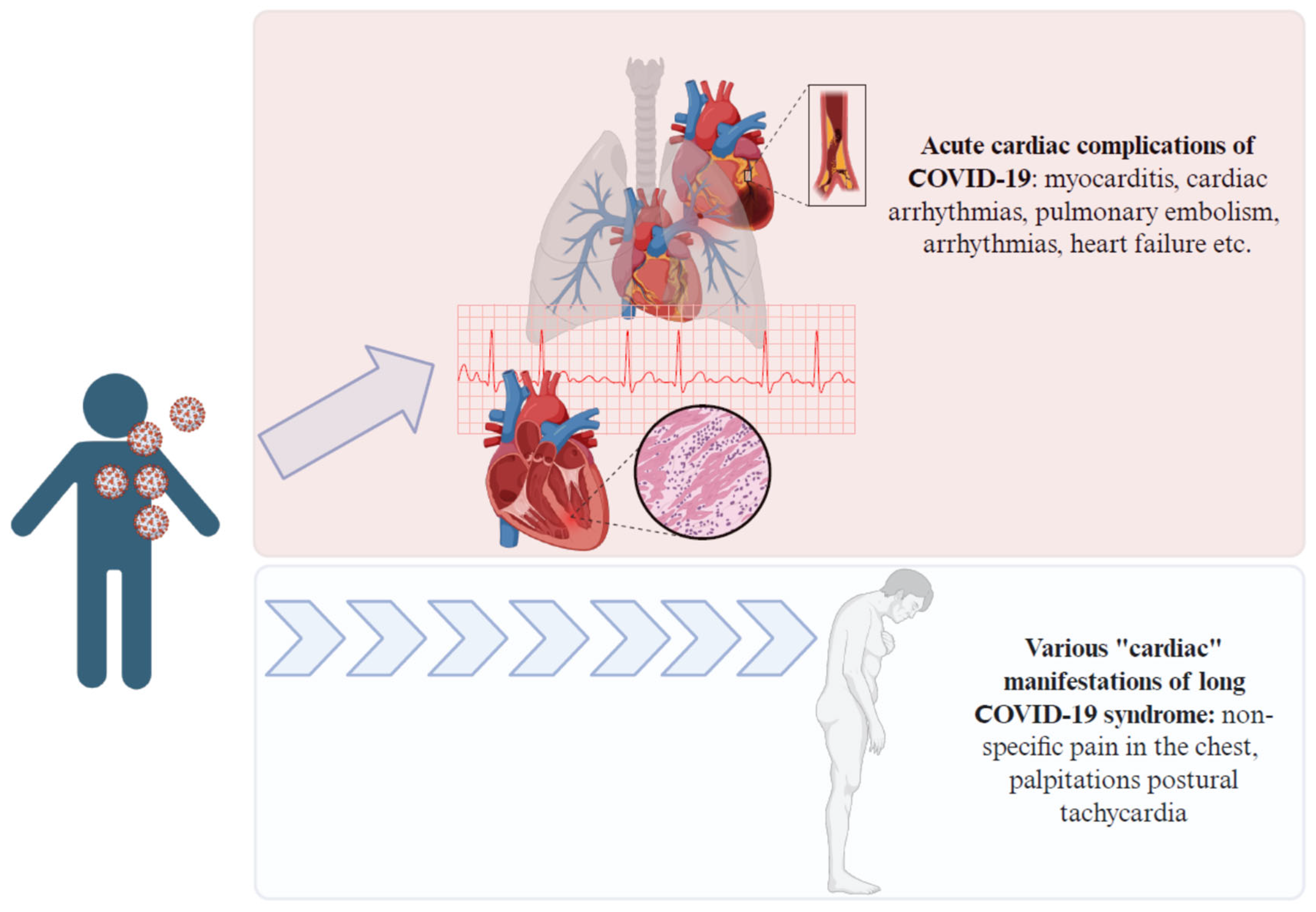
4. Cardiovascular Complications of COVID-19
5. Current Recommendations Regarding Vaccinations Against COVID-19
6. Safety and Effectiveness of Vaccinations Against COVID-19
7. Current Options for Pharmacotherapy of SARS-CoV-2 Infection
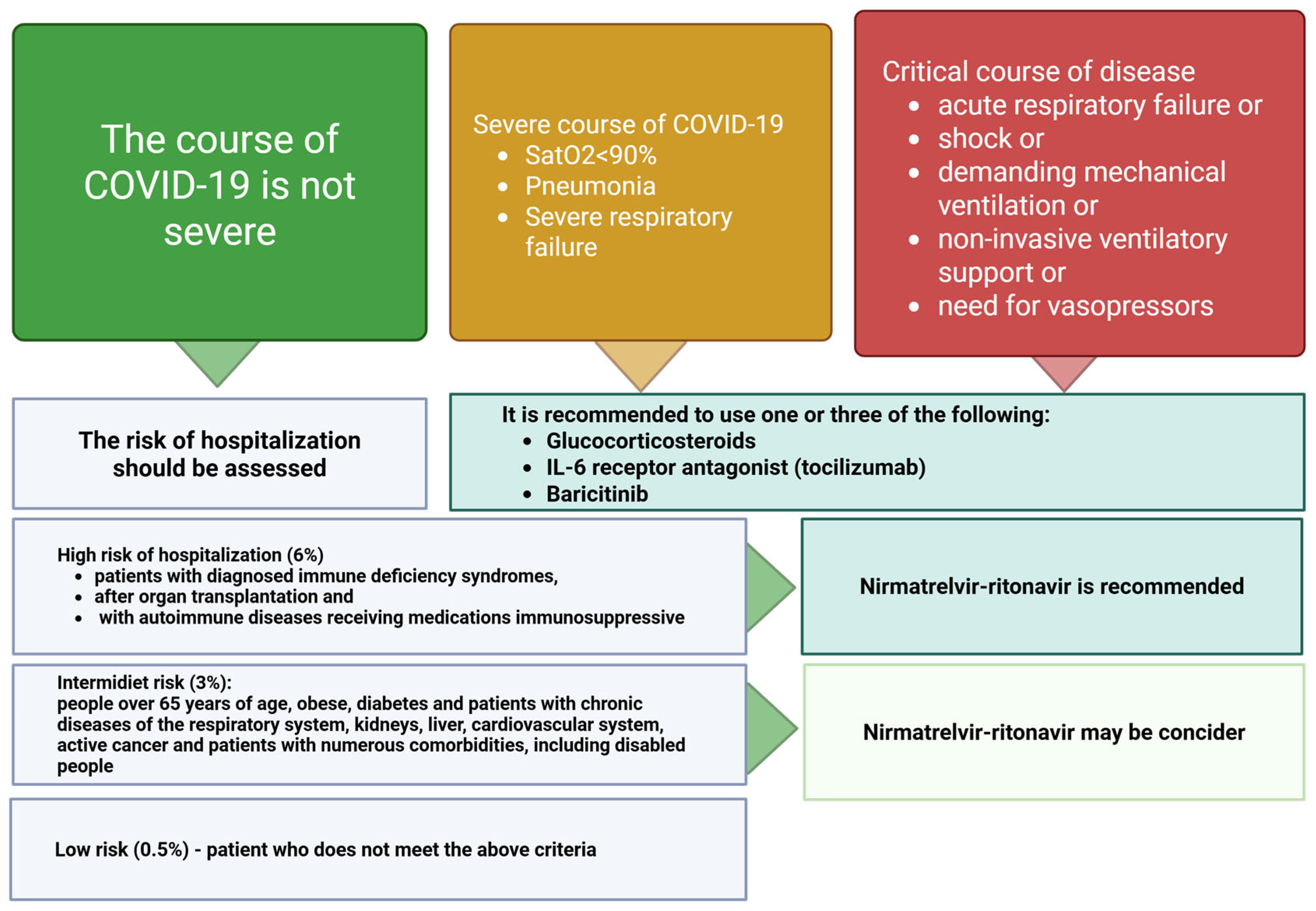
- Critical, understood as involving acute respiratory failure, shock, and need for mechanical ventilation or non-invasive ventilatory support or vasopressors;
- Severe, with oxygen saturation declining to <90% when breathing atmospheric oxygen, pneumonia, or signs of severe respiratory effort (one condition is enough);
- Non-severe, understood as not meeting any of the criteria for a severe and critical course.
8. Nirmatrelvir/Ritonavir
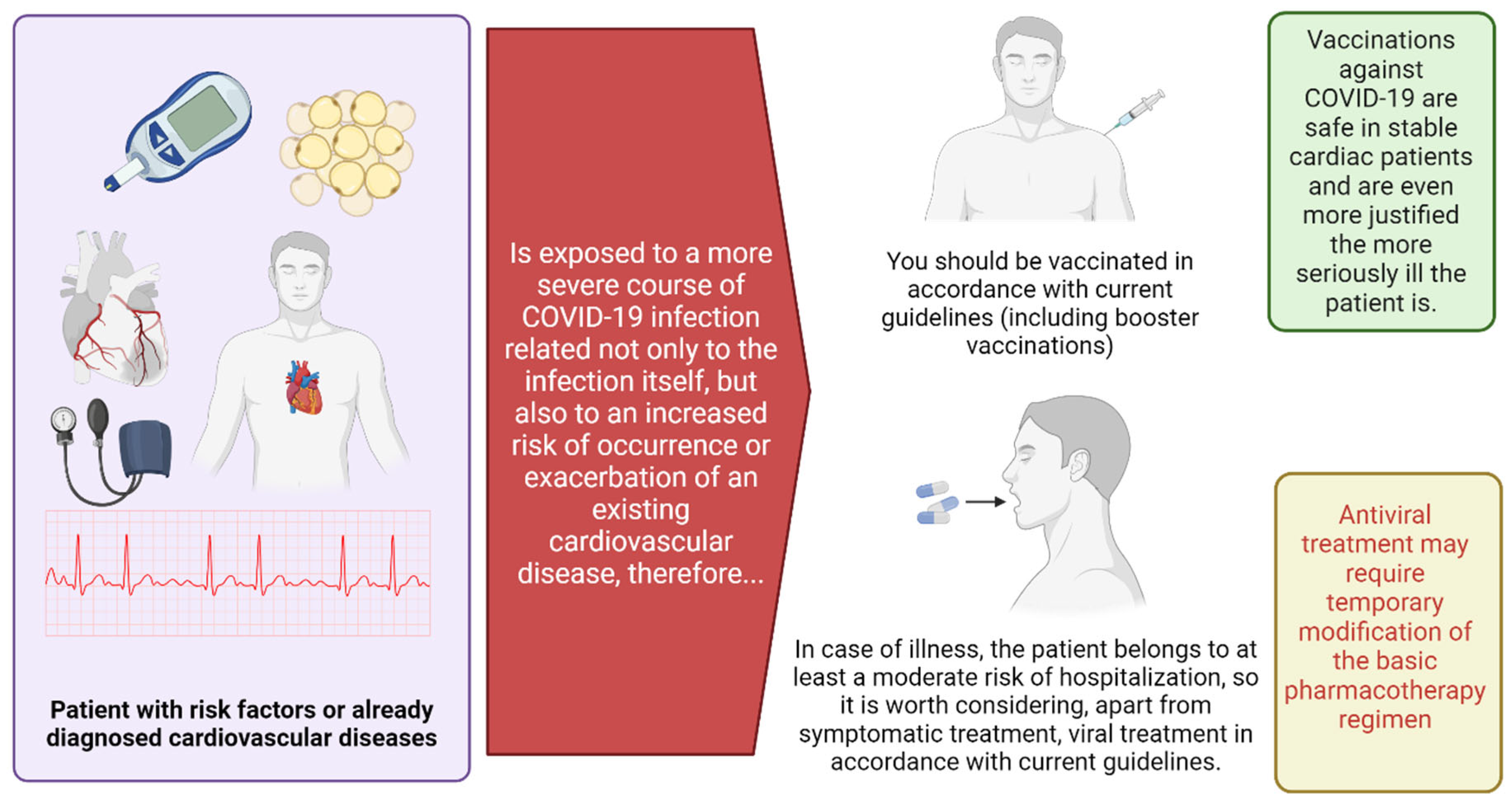
- In the case of COVID-19 diagnosis in a patient with symptoms of infection, assess the group at increased risk of severe disease (Figure 3)
- If the patient qualifies for nirmatrelvir/ritonavir, analyze the chronic pharmacotherapy regimen in the context of potentially significant drug interactions (Table 3).
- Drug coadministration:
- In the absence of a risk of interaction, propose the use of nirmatrelvir/ritonavir regardless of vaccination status.
- In the case of a significant risk of interaction, consider the possibility of temporary modification of the pharmacotherapy regimen (Table 4).
9. Limitations
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Professionals. Available online: https://www.cdc.gov/covid/hcp/clinical-care/underlying-conditions.html (accessed on 19 February 2024).
- Smaga, A.; Waśko, B.; Wojtyniak, B. Sytuacja Zdrowotna Ludności Polski i jej Uwarunkowania 2022; Wojtyniaka, B., Goryńskiego, P., Eds.; Narodowy Instytut Zdrowia Publicznego PZH—Państwowy Insytut Badawczy: Warszawa, Poland, 2022. [Google Scholar]
- Bae, S.; Kim, S.R.; Kim, M.N.; Shim, W.J.; Park, S.M. Impact of cardiovascular disease and risk factors on fatal outcomes in patients with COVID-19 according to age: A systematic review and meta-analysis. Heart 2021, 107, 373–380. [Google Scholar] [CrossRef] [PubMed]
- Cannata, A.; Watson, S.A.; Daniel, A.; Giacca, M.; Shah, A.M.; McDonagh, T.A.; Scott, P.A.; Bromage, D.I. Impact of the COVID-19 pandemic on in-hospital mortality in cardiovascular disease: A meta-analysis. Eur. J. Prev. Cardiol. 2022, 29, 1266–1274. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dessie, Z.G.; Zewotir, T. Mortality-related risk factors of COVID-19: A systematic review and meta-analysis of 42 studies and 423,117 patients. BMC Infect. Dis. 2021, 21, 855. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hessami, A.; Rezaei, N. Cardiovascular diseases burden in COVID-19. Am. J. Emerg. Med. 2021, 50, 790. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liang, C.; Zhang, W.; Li, S.; Qin, G. Coronary heart disease and COVID-19: A meta-analysis. Med. Clin. 2021, 156, 547–554. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gerotziafas, G.T.; Catalano, M.; Colgan, M.P.; Pecsvarady, Z.; Wautrecht, J.C.; Fazeli, B.; Olinic, D.M.; Farkas, K.; Elalamy, I.; Falanga, A.; et al. Scientific Reviewer Committee Guidance for the Management of Patients with Vascular Disease or Cardiovascular Risk Factors and COVID-19: Position Paper from VAS-European Independent Foundation in Angiology/Vascular Medicine. Thromb. Haemost. 2020, 120, 1597–1628. [Google Scholar] [CrossRef]
- Raj, K.; Yeruva, K.; Jyotheeswara Pillai, K.; Kumar, P.; Agrawal, A.; Chandna, S.; Khuttan, A.; Tripathi, S.; Akella, R.; Gudi, T.R.; et al. Population Risk Factors for Severe Disease and Mortality in COVID-19 in the United States during the Pre-Vaccine Era: A Retrospective Cohort Study of National Inpatient Sample. Med. Sci. 2022, 10, 67. [Google Scholar] [CrossRef]
- Meister, T.; Pisarev, H.; Kolde, R.; Kalda, R.; Suija, K.; Milani, L.; Karo-Astover, L.; Piirsoo, M.; Uusküla, A. Clinical characteristics and risk factors for COVID-19 infection and disease severity: A nationwide observational study in Estonia. PLoS ONE. 2022, 17, e0270192. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Niedziela, J.T.; Jaroszewicz, J.; Wita, K.; Cieśla, D.; Gąsior, M. High in-hospital and post-discharge mortality in patients with a pre-existing diagnosis of heart failure hospitalized due to COVID-19. Kardiol. Pol. 2022, 80, 90. [Google Scholar] [CrossRef]
- Yonas, E.; Alwi, I.; Pranata, R.; Huang, I.; Lim, M.A.; Gutierrez, E.J.; Yamin, M.; Siswanto, B.B.; Virani, S.S. Effect of heart failure on the outcome of COVID-19—A meta analysis and systematic review. Am. J. Emerg. Med. 2021, 46, 204–211. [Google Scholar] [CrossRef]
- Alvarez-Garcia, J.; Lee, S.; Gupta, A.; Cagliostro, M.; Joshi, A.A.; Rivas-Lasarte, M.; Contreras, J.; Mitter, S.S.; LaRocca, G.; Tlachi, P.; et al. Prognostic Impact of Prior Heart Failure in Patients Hospitalized with COVID-19. J. Am. Coll. Cardiol. 2020, 76, 2334–2348. [Google Scholar] [CrossRef] [PubMed]
- Kałużna-Oleksy, M.; Gackowski, A.; Jankowska, E.A.; Kukulski, T.; Lelonek, M.; Nessler, J.; Pawlak, A.; Rozentryt, P.; Rubiś, P.; Straburzyńska-Migaj, E.; et al. The patient with heart failure in the face of the coronavirus disease 2019 pandemic: An expert opinion of the Heart Failure Working Group of the Polish Cardiac Society. Kardiol. Pol. 2020, 78, 618–631. [Google Scholar] [CrossRef]
- Tomasoni, D.; Inciardi, R.M.; Lombardi, C.M.; Tedino, C.; Agostoni, P.; Ameri, P.; Barbieri, L.; Bellasi, A.; Camporotondo, R.; Canale, C.; et al. Impact of heart failure on the clinical course and outcomes of patients hospitalized for COVID-19. Results of the Cardio-COVID-Italy multicentre study. Eur. J. Heart Fail. 2020, 22, 2238–2247. [Google Scholar] [CrossRef]
- Gąsior, M.; Jaroszewicz, J.; Wita, K.; Cieśla, D.; Hudzik, B. High postdischarge mortality in hospitalized COVID-19 patients with cardiovascular comorbidities. Pol. Arch. Intern. Med. 2021, 131, 749–751. [Google Scholar] [CrossRef]
- Zhao, Y.H.; Zhao, L.; Yang, X.C.; Wang, P. Cardiovascular complications of SARS-CoV-2 infection (COVID-19): A systematic review and meta-analysis. Rev. Cardiovasc. Med. 2021, 22, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Dennis, A.; Wamil, M.; Alberts, J.; Oben, J.; Cuthbertson, D.J.; Wootton, D.; Crooks, M.; Gabbay, M.; Brady, M.; Hishmeh, L.; et al. COVERSCAN study investigators Multiorgan impairment in low-risk individuals with post-COVID-19 syndrome: A prospective, community-based study. BMJ Open 2021, 11, e048391. [Google Scholar] [CrossRef]
- Ortega-Paz, L.; Talasaz, A.H.; Sadeghipour, P.; Potpara, T.S.; Aronow, H.D.; Jara-Palomares, L.; Sholzberg, M.; Angiolillo, D.J.; Lip, G.Y.H.; Bikdeli, B. COVID-19-Associated Pulmonary Embolism: Review of the Pathophysiology, Epidemiology, Prevention, Diagnosis, and Treatment. Semin. Thromb. Hemost. 2023, 49, 816–832. [Google Scholar] [CrossRef] [PubMed]
- Suh, Y.J.; Hong, H.; Ohana, M.; Bompard, F.; Revel, M.P.; Valle, C.; Gervaise, A.; Poissy, J.; Susen, S.; Hékimian, G.; et al. Pulmonary Embolism and Deep Vein Thrombosis in COVID-19: A Systematic Review and Meta-Analysis. Radiology 2021, 298, E70–E80. [Google Scholar] [CrossRef]
- Lewczuk, T.; Kazimierczyk, R.; Sobkowicz, B.; Lisowska, A. Pulmonary embolism in COVID-19 pneumonia patients admitted to temporary hospital—The follow-up study. Adv. Med. Sci. 2023, 68, 270–275. [Google Scholar] [CrossRef] [PubMed]
- Zuin, M.; Barco, S.; Giannakoulas, G.; Engelen, M.M.; Hobohm, L.; Valerio, L.; Vandenbriele, C.; Verhamme, P.; Vanassche, T.; Konstantinides, S.V. Risk of venous thromboembolic events after COVID-19 infection: A systematic review and meta-analysis. J. Thromb. Thrombolysis 2023, 55, 490–498. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Desai, A.D.; Lavelle, M.; Boursiquot, B.C.; Wan, E.Y. Long-term complications of COVID-19. Am. J. Physiol. Cell Physiol. 2022, 322, C1–C11. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Task Force for the Management of COVID-19 of the European Society of Cardiology. European Society of Cardiology guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: Part 1-epidemiology, pathophysiology, and diagnosis. Eur. Heart J. 2022, 43, 1033–1058, Erratum in Eur. Heart J. 2022, 43, 1776. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Task Force for the Management of COVID-19 of the European Society of Cardiology. ESC guidance for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic: Part 2-care pathways, treatment, and follow-up. Eur. Heart J. 2022, 43, 1059–1103, Erratum in Eur. Heart J. 2021, 43, 1776. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Available online: https://ptmr.info.pl/szczepienia/ (accessed on 21 February 2024).
- Komunikat nr 34 Ministra Zdrowia w Sprawie Realizacji Szczepień Przeciw COVID-19 w Sezonie 2023/2024. Available online: https://www.gov.pl/web/zdrowie/komunikat-ministra-zdrowia-w-sprawie-realizacji-szczepien-przeciw-covid-19-w-sezonie-20232024 (accessed on 21 February 2024).
- WHO. WHO Roadmap on Uses of COVID-19 Vaccines in the Context of Omicron and High Population Immunity. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-Vaccines-SAGE-Prioritization-2023.2 (accessed on 21 February 2024).
- ECDC. Available online: https://www.ecdc.europa.eu/sites/default/files/documents/covid-19-vaccines-composition-variants-statement-ECDC-EMA_0.pdf (accessed on 21 February 2024).
- EMA. Available online: https://www.ema.europa.eu/en/news/ema-recommends-approval-adapted-nuvaxovid-covid-19-vaccine-targeting-omicron-xbb15 (accessed on 21 February 2024).
- Available online: https://www.ema.europa.eu/en/homepage (accessed on 21 February 2024).
- Dobrowolska, K.; Brzdęk, M.; Zarębska-Michaluk, D.; Rzymski, P.; Rogalska, M.; Moniuszko-Malinowska, A.; Szymanek-Pasternak, A.; Jaroszewicz, J.; Dutkiewicz, E.; Kowalska, J.; et al. Differences between the course of SARS-CoV-2 infections in the periods of the Delta and Omicron variant dominance in Poland. Pol. Arch. Intern. Med. 2023, 133, 16403. [Google Scholar] [CrossRef]
- Nyberg, T.; Ferguson, N.M.; Nash, S.G.; Webster, H.H.; Flaxman, S.; Andrews, N.; Hinsley, W.; Bernal, J.L.; Kall, M.; Bhatt, S.; et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: A cohort study. Lancet 2022, 399, 1303–1312. [Google Scholar] [CrossRef]
- Available online: https://szczepienia.pzh.gov.pl/szczepionki/covid-19-2/ (accessed on 20 May 2025).
- Cai, C.; Peng, Y.; Shen, E.; Huang, Q.; Chen, Y.; Liu, P.; Guo, C.; Feng, Z.; Gao, L.; Zhang, X.; et al. A comprehensive analysis of the efficacy and safety of COVID-19 vaccines. Mol. Ther. 2021, 29, 2794–2805. [Google Scholar] [CrossRef]
- Writing Committee; Gluckman, T.J.; Bhave, N.M.; Allen, L.A.; Chung, E.H.; Spatz, E.S.; Ammirati, E.; Baggish, A.L.; Bozkurt, B.; Cornwell, W.K., III; et al. 2022 ACC Expert Consensus Decision Pathway on Cardiovascular Sequelae of COVID-19 in Adults: Myocarditis and Other Myocardial Involvement, Post-Acute Sequelae of SARS-CoV-2 Infection, and Return to Play: A Report of the American College of Cardiology Solution Set Oversight Committee. J. Am. Coll. Cardiol. 2022, 79, 1717–1756. [Google Scholar] [CrossRef]
- Block, J.P.; Boehmer, T.K.; Forrest, C.B.; Carton, T.W.; Lee, G.M.; Ajani, U.A.; Christakis, D.A.; Cowell, L.G.; Draper, C.; Ghildayal, N.; et al. Cardiac Complications After SARS-CoV-2 Infection and mRNA COVID-19 Vaccination—PCORnet, United States, January 2021-January 2022. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 517–523. [Google Scholar] [CrossRef]
- Advisory Committee on Immunization Practices (ACIP). Update on Myocarditis Following mRNA COVID-19 Vaccination. 23 June 2022. Available online: https://stacks.cdc.gov/view/cdc/118585 (accessed on 13 March 2023).
- WHO: No Evidence COVID-19 Vaccines Increase Risk of Strokes in Older People. Available online: https://www.voanews.com/a/6927473.html (accessed on 21 February 2023).
- Available online: https://www.marketscreener.com/news/latest/EU-drug-regulator-has-not-seen-signal-of-possible-Pfizer-COVID-shot-stroke-link--42761448/ (accessed on 21 February 2023).
- CDC and FDA Identify Preliminary COVID-19 Vaccine Safety Signal for Persons Aged 65 Years and Older and CDC. Available online: https://www.fda.gov/vaccines-blood-biologics/safety-availability-biologics/cdc-and-fda-identify-preliminary-covid-19-vaccine-safety-signal-persons-aged-65-years-and-older (accessed on 21 February 2023).
- Available online: https://pubmed.ncbi.nlm.nih.gov/36404170/ (accessed on 21 February 2023).
- Xie, C.; Vincent, L.; Chadwick, A.; Peschl, H. COVID-19 vaccine induced prothrombotic immune thrombocytopenia. Eur. Heart J. 2021, 42, ehab237. [Google Scholar] [CrossRef]
- Varona, J.F.; García-Isidro, M.; Moeinvaziri, M.; Ramos-López, M.; Fernández-Domínguez, M. Primary adrenal insufficiency associated with Oxford-AstraZeneca ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia (VITT). Eur. J. Intern. Med. 2021, 91, 90–92. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Turi, M.C.; Spitaleri, F.; Gori, A.M.; Parruti, G.; Rogolino, A.A.; Albani, A.; Giusti, B.; Agostinone, L.; Cesari, F.; Ranalli, P.; et al. A case of vaccine-induced immune thrombotic thrombocytopenia with massive artero-venous thrombosis. Blood Transfus. 2021, 19, 343–346. [Google Scholar] [CrossRef]
- Taylor, P.; Allen, L.; Shrikrishnapalasuriyar, N.; Stechman, M.; Rees, A. Vaccine-induced thrombosis and thrombocytopenia with bilateral adrenal haemorrhage. Clin. Endocrinol. (Oxf.) 2021, 97, 26–27. [Google Scholar] [CrossRef] [PubMed]
- Sangli, S.; Virani, A.; Cheronis, N.; Vannatter, B.; Minich, C.; Noronha, S.; Bhagavatula, R.; Speredelozzi, D.; Sareen, M.; Kaplan, R.B. Thrombosis with Thrombocytopenia After the Messenger RNA-1273 Vaccine. Ann. Intern. Med. 2021, 174, L21-0244. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Malik, B.; Kalantary, A.; Rikabi, K.; Kunadi, A. Pulmonary embolism, transient ischaemic attack and thrombocytopenia after the Johnson & Johnson COVID-19 vaccine. BMJ Case Rep. 2021, 14, e243975. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jones, M.; Boisvert, A.; Landry, J.; Petrasek, P.F. Limb ischemia and pulmonary artery thrombosis afer the ChAdOx1 nCoV-19 (Oxford-AstraZeneca) vaccine: A case of vaccine-induced immune thrombotic thrombocytopenia. CMAJ 2021, 193, E906–E910. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guetl, K.; Gary, T.; Raggam, R.B.; Schmid, J.; Wölfler, A.; Brodmann, M. SARS-CoV-2 vaccine-induced immune thrombotic thrombocytopenia treated with immunoglobulin and argatroban. Lancet 2021, 397, e19. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- George, G.; Friedman, K.D.; Curtis, B.R.; Lind, S.E. Successful treatment of thrombotic thrombocytopenia with cerebral sinus venous thrombosis following Ad26.COV2.S vaccination. Am. J. Hematol. 2021, 96, E301–E303. [Google Scholar] [CrossRef] [PubMed]
- Cliff-Patel, N.; Moncrieff, L.; Ziauddin, V. Renal Vein Thrombosis and Pulmonary Embolism Secondary to Vaccine-induced Thrombotic Thrombocytopenia (VITT). Eur. J. Case Rep. Intern. Med. 2021, 8, 002692. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Clark, R.T.; Johnson, L.; Billotti, J.; Foulds, G.; Ketels, T.; Heard, K.; Calvello Hynes, E. Early Outcomes of Bivalirudin Therapy for Thrombotic Thrombocytopenia and Cerebral Venous Sinus Thrombosis After Ad26.COV2.S Vaccination. Ann. Emerg. Med. 2021, 78, 511–514. [Google Scholar] [CrossRef]
- Bourguignon, A.; Arnold, D.M.; Warkentin, T.E.; Smith, J.W.; Pannu, T.; Shrum, J.M.; Al Maqrashi, Z.A.A.; Shroff, A.; Lessard, M.C.; Blais, N.; et al. Adjunct Immune Globulin for Vaccine-Induced Thrombotic Thrombocytopenia. N. Engl. J. Med. 2021, 385, 720–728. [Google Scholar] [CrossRef] [PubMed]
- Bersinger, S.; Lagarde, K.; Marlu, R.; Pernod, G.; Payen, J.F. Using Nonheparin Anticoagulant to Treat a Near-Fatal Case with Multiple Venous Thrombotic Lesions During ChAdOx1 nCoV-19 Vaccination-Related Vaccine-Induced Immune Thrombotic Thrombocytopenia. Crit. Care Med. 2021, 49, e870–e873. [Google Scholar] [CrossRef] [PubMed]
- Bano, F.; Badugama, B.; Chandra, D. Thrombosis and thrombocytopaenia after ChAdOx1 nCoV-19 vaccination: A single UK centre experience. BMJ Case Rep. 2021, 14, e243894. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Al-Mayhani, T.; Saber, S.; Stubbs, M.J.; Losseff, N.A.; Perry, R.J.; Simister, R.J.; Gull, D.; Jäger, H.R.; Scully, M.A.; Werring, D.J. Ischaemic stroke as a presenting feature of ChAdOx1 nCoV-19 vaccine-induced immune thrombotic thrombocytopenia. J. Neurol. Neurosurg. Psychiatry 2021, 92, 1247–1248. [Google Scholar] [CrossRef] [PubMed]
- Al-Maqbali, J.S.; Al Rasbi, S.; Kashoub, M.S.; Al Hinaai, A.M.; Farhan, H.; Al Rawahi, B.; Al Alawi, A.M. A 59-Year-Old Woman with Extensive Deep Vein Thrombosis and Pulmonary Thromboembolism 7 Days Following a First Dose of the Pfizer-BioNTech BNT162b2 mRNA COVID-19 Vaccine. Am. J. Case Rep. 2021, 22, e932946. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abou-Ismail, M.Y.; Moser, K.A.; Smock, K.J.; Lim, M.Y. Vaccine-induced thrombotic thrombocytopenia following Ad26.COV2.S vaccine in a man presenting as acute venous thromboembolism. Am. J. Hematol. 2021, 96, E346–E349. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Scully, M.; Singh, D.; Lown, R.; Poles, A.; Solomon, T.; Levi, M.; Goldblatt, D.; Kotoucek, P.; Thomas, W.; Lester, W. Pathologic Antibodies to Platelet Factor 4 after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2202–2211. [Google Scholar] [CrossRef]
- Schultz, N.H.; Sørvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattør, T.H.; Tjønnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021, 384, 2124–2130. [Google Scholar] [CrossRef]
- Thiele, T.; Ulm, L.; Holtfreter, S.; Schönborn, L.; Kuhn, S.O.; Scheer, C.; Warkentin, T.E.; Bröker, B.M.; Becker, K.; Aurich, K.; et al. Frequency of positive anti-PF4/polyanion antibody tests after COVID-19 vaccination with ChAdOx1 nCoV-19 and BNT162b2. Blood 2021, 138, 299–303. [Google Scholar] [CrossRef]
- Watson, O.J.; Barnsley, G.; Toor, J.; Hogan, A.B.; Winskill, P.; Ghani, A.C. Global impact of the first year of COVID-19 vaccination: A mathematical modelling study. Lancet Infect. Dis. 2022, 22, 1293–1302, Erratum in Lancet Infect. Dis. 2023, 23, e400. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pietrzak, Ł.; Polok, K.; Halik, R.; Szuster-Ciesielska, A.; Szczeklik, W. Effectiveness of the BNT162b2 vaccine in preventing COVID-19-associated deaths in Poland. Pol. Arch. Intern. Med. 2023, 133, 16453. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, A.; Iwagami, M.; Yasuhara, J.; Takagi, H.; Kuno, T. Protective effect of COVID-19 vaccination against long COVID syndrome: A systematic review and meta-analysis. Vaccine 2023, 41, 1783–1790. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wytyczne ESC 2021 Dotyczące Diagnostyki i Leczenia Ostrej i Przewlekłej Niewydolności Serca. Available online: https://ptkardio.pl/wytyczne/44-wytyczne_esc_2021_dotyczace_diagnostyki_i_leczenia_ostrej_i_przewleklej_niewydolnosci_serca (accessed on 15 March 2023).
- ESC/ERS Guidelines for the Diagnosis and Treatment of Pulmonary Hypertension. 2022. Available online: https://academic.oup.com/eurheartj/article/43/38/3618/6673929?login=true (accessed on 15 March 2023).
- Available online: https://ptwakc.org.pl/wp-content/uploads/2024/02/6.-Pacjenci-z-chorobami-ukladu-sercowo-naczyniowego.png (accessed on 25 February 2024).
- World Health Organization. Therapeutics and COVID-19: Living Guideline; World Health Organization: Geneva, Switzerland, 2023; Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-therapeutics-2023.2 (accessed on 21 February 2024).
- Eastman, R.T.; Roth, J.S.; Brimacombe, K.R.; Simeonov, A.; Shen, M.; Patnaik, S.; Hall, M.D. Remdesivir: A Review of Its Discovery and Development Leading to Emergency Use Authorization for Treatment of COVID-19. ACS Cent. Sci. 2020, 6, 672–683. [Google Scholar] [CrossRef] [PubMed]
- Hammond, J.; Leister-Tebbe, H.; Gardner, A.; Abreu, P.; Bao, W.; Wisemandle, W.; Baniecki, M.; Hendrick, V.M.; Damle, B.; Simón-Campos, A.; et al. EPIC-HR Investigators Oral Nirmatrelvir for High-Risk, Nonhospitalized Adults with COVID-19. N. Engl. J. Med. 2022, 386, 1397–1408. [Google Scholar] [CrossRef]
- Najjar-Debbiny, R.; Gronich, N.; Weber, G.; Khoury, J.; Amar, M.; Stein, N.; Goldstein, L.H.; Saliba, W. Effectiveness of Paxlovid in Reducing Severe Coronavirus Disease 2019 and Mortality in High-Risk Patients. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2023, 76, e342–e349. [Google Scholar] [CrossRef]
- Zhou, X.; Kelly, S.P.; Liang, C.; Li, L.; Shen, R.; Leister-Tebbe, H.K.; Terra, S.G.; Gaffney, M.; Russo, L. Real-World Effectiveness of Nirmatrelvir/Ritonavir in Preventing Hospitalization Among Patients with COVID-19 at High Risk for Severe Disease in the United States: A Nationwide Population-Based Cohort Study. medRxiv 2022. [Google Scholar] [CrossRef]
- Aggarwal, N.R.; Molina, K.C.; Beaty, L.E.; Bennett, T.D.; Carlson, N.E.; Mayer, D.A.; Peers, J.L.; Russell, S.; Wynia, M.K.; Ginde, A.A. Real-world use of nirmatrelvir-ritonavir in outpatients with COVID-19 during the era of omicron variants including BA.4 and BA.5 in Colorado, USA: A retrospective cohort study. Lancet Infect. Dis. 2023, 23, 696–705. [Google Scholar] [CrossRef]
- Wai, A.K.; Chan, C.Y.; Cheung, A.W.; Wang, K.; Chan, S.C.; Lee, T.T.; Luk, L.Y.; Yip, E.T.; Ho, J.W.; Tsui, O.W.; et al. Association of Molnupiravir and Nirmatrelvir-Ritonavir with preventable mortality, hospital admissions and related avoidable healthcare system cost among high-risk patients with mild to moderate COVID-19. The Lancet regional health. West. Pac. 2023, 30, 100602. [Google Scholar] [CrossRef]
- Liverpool COVID-19 Drug Interaction Checker. Available online: https://www.covid19-druginteractions.org/checker (accessed on 20 May 2025).
- Rizk, J.G.; Lazo, J.G., Jr.; Gupta, A.; Lavie, C.J.; Effron, M.B. Proposal for a Simple Algorithmic Approach to Manage Drug-Drug Interactions of Oral Anticoagulants with Nirmatrelvir/Ritonavir in COVID-19 Outpatients. Semin. Thromb. Hemost. 2023, 49, 85–88. [Google Scholar] [CrossRef]
- Cox, D.S.; Rehman, M.; Khan, T.; Ginman, K.; Salageanu, J.; LaBadie, R.R.; Wan, K.; Damle, B. Effects of nirmatrelvir/ritonavir on midazolam and dabigatran pharmacokinetics in healthy participants. Br. J. Clin. Pharmacol. 2023, 89, 3352–3363. [Google Scholar] [CrossRef]
- Wang, Z.; Chan, E.C.Y. Physiologically-Based Pharmacokinetic Modeling-Guided Dose Management of Oral Anticoagulants when Initiating Nirmatrelvir/Ritonavir (Paxlovid) for COVID-19 Treatment. Clin. Pharmacol. Ther. 2022, 112, 803–807. [Google Scholar] [CrossRef]
- Hammond, J.; Yunis, C.; Fountaine, R.J.; Luscan, G.; Burr, A.M.; Zhang, W.; Wisemandle, W.; Soares, H.; Baniecki, M.L.; Hendrick, V.M.; et al. Oral Nirmatrelvir-Ritonavir as Postexposure Prophylaxis for COVID-19. N. Engl. J. Med. 2024, 391, 224–234. [Google Scholar] [CrossRef] [PubMed]
- Abraham, S.; Nohria, A.; Neilan, T.G.; Asnani, A.; Saji, A.M.; Shah, J.; Lech, T.; Grossman, J.; Abraham, G.M.; McQuillen, D.P.; et al. Cardiovascular Drug Interactions with Nirmatrelvir/Ritonavir in Patients with COVID-19: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2022, 80, 1912–1924. [Google Scholar] [CrossRef]
- Marzolini, C.; Kuritzkes, D.R.; Marra, F.; Boyle, A.; Gibbons, S.; Flexner, C.; Pozniak, A.; Boffito, M.; Waters, L.; Burger, D.; et al. Prescribing Nirmatrelvir-Ritonavir: How to Recognize and Manage Drug-Drug Interactions. Ann. Intern. Med. 2022, 175, 744–746. [Google Scholar] [CrossRef]
- Di Lenarda, A.; Ferri, N.; Lanzafame, M.; Montuori, E.A.; Pacelli, L. Cardiovascular Drug Interactions with Nirmatrelvir/Ritonavir for COVID-19: Considerations for Daily Practice. Eur. Cardiol. 2024, 19, e15. [Google Scholar] [CrossRef]
- Hendrick, V.; Pohorylo, E.; Merchant, L.; Gerhart, J.; Arham, I.N.; Draica, F.; Quercia, R.; Ayoub, A.; Mehta, R. Pharmacovigilance of Drug-Drug Interactions with Nirmatrelvir/Ritonavir. Infect. Dis. Ther. 2024, 13, 2545–2561. [Google Scholar] [CrossRef]
- Gerhart, J.; Cox, D.S.; Singh, R.S.P.; Chan, P.L.S.; Rao, R.; Allen, R.; Shi, H.; Masters, J.C.; Damle, B. A Comprehensive Review of the Clinical Pharmacokinetics, Pharmacodynamics, and Drug Interactions of Nirmatrelvir/Ritonavir. Clin. Pharmacokinet. 2024, 63, 27–42. [Google Scholar] [CrossRef]
- Graham, B.S. Rapid COVID-19 vaccine development. Science 2020, 368, 945–946. [Google Scholar] [CrossRef]
- Van den Ouweland, F.; Charpentier, N.; Türeci, Ö.; Rizzi, R.; Mensa, F.J.; Lindemann, C.; Pather, S. Safety and reactogenicity of the BNT162b2 COVID-19 vaccine: Development, post-marketing surveillance, and real-world data. Hum. Vaccin. Immunother. 2024, 20, 2315659. [Google Scholar] [CrossRef]
- Stowe, J.; Miller, E.; Andrews, N.; Whitaker, H.J. Risk of myocarditis and pericarditis after a COVID-19 mRNA vaccine booster and after COVID-19 in those with and without prior SARS-CoV-2 infection: A self-controlled case series analysis in England. PLoS Med. 2023, 20, e1004245. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic thrombocytopenia after ChAdOx1 nCov-19 vaccination. N. Engl. J. Med. 2021, 384, 2092–2101. [Google Scholar] [CrossRef]
- Heath, P.T.; Galiza, E.P.; Baxter, D.N.; Boffito, M.; Browne, D.; Burns, F.; Chadwick, D.R.; Clark, R.; Cosgrove, C.; Galloway, J.; et al. Safety and efficacy of NVX-CoV2373 COVID-19 vaccine. N. Engl. J. Med. 2021, 385, 1172–1183. [Google Scholar] [CrossRef]
- Flisiak, R.; Jaroszewicz, J.; Kozielewicz, D.; Kuchar, E.; Parczewski, M.; Pawłowska, M.; Piekarska, A.; Rzymski, P.; Simon, K.; Tomasiewicz, K.; et al. Management of SARS-CoV-2 Infection-Clinical Practice Guidelines of the Polish Association of Epidemiologists and Infectiologists, for 2025. J. Clin. Med. 2025, 14, 2305. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Comorbidities | Age | Severe Course of COVID-19 | Death from COVID-19 | Death from or Severe Course of COVID-19 |
|---|---|---|---|---|
| OR (95% CI) | ||||
| Arterial hypertension | <50 r. ż | 3.14 (2.16–4.55) | 6.13 (4.01–9.39) | 3.49 (2.49–4.88) |
| 50–60 r. ż | 2.43 (1.72–3.44) | 2.81 (1.97–4.01) | 2.61 (2.03–3.37) | |
| ≥60 r. ż. | 1.54 (1.35–1.76) | 2.10 (1.67–2.64) | 1.86 (1.55–2.23) | |
| all | 2.42 (1.98–2.96) | 2.60 (2.11–3.20) | 2.50 (2.15–2.90) | |
| Diabetes | <50 r. ż | 3.24 (1.96–5.36) | 5.31 (3.22–8.26) | 3.49 (2.24–5.45) |
| 50–60 r. ż | 2.73 (1.59–4.7) | 2.22 (1.82–2.72) | 2.37 (1.83–3.08) | |
| ≥60 r. ż. | 1.44 (1.11–1.86) | 1.76 (1.27–2.44) | 1.65 (1.34–2.03) | |
| all | 2.47 (1.86–3.27) | 2.11 (1.63–2.73) | 2.25 (1.89–2.69) | |
| CVD | <50 r. ż | 4.87 (3.31–7.16) | 7.80 (4.06–15.00) | 5.66 (4.12–7.79) |
| 50–60 r. ż | 3.09 (2.30–4.17) | 3.14 (1.12–8.78) | 3.30 (2.16–5.05) | |
| ≥60 r. ż. | 1.73 (1.01–2.90) | 2.46 (1.91–3.17) | 2.10 (1.68–2.61) | |
| all | 3.15 (2.34–4.25) | 3.23 (2.26–4.57) | 3.11 (2.55–3.79) | |
| Analyzed Effect | 2 Doses of the Vaccine vs. Unvaccinated OR (95% CI) | 2 vs. 1 Dose of the Vaccine OR (95% CI) | 1 Dose of the Vaccine vs. Unvaccinated OR (95% CI) |
|---|---|---|---|
| Long-COVID syndrome | 0.64 (0.45–0.92) | 0.60 (0.43–0.83) | 0.90 (0.80–1.01) |
| Chronic fatigue | 0.62 (0.41–0.93) | ||
| Respiratory disorders | 0.50 (0.47–0.52) | ||
| Cardiovascular disorders | 0.59 (0.23–1.49) | ||
| Gastrointestinal disorders | 0.62 (0.35–1.10) | ||
| Metabolic disorders | 0.58 (0.24–1.41) | ||
| Musculoskeletal disorders | 0.63 (0.26–1.52) | ||
| Neurological disorders | 0.61(0.31–1.20) | ||
| Cognitive disorders | 0.49 (0.15–1.62) | ||
| Baricitinib | Nirmatrelvir/Ritonavir (5 Days) | Remdesivir | Tocilizumab | |
|---|---|---|---|---|
| Acenocoumarol | ||||
| Amiodarone | Possible increase in amiodarone concentration | |||
| Amlodipin | ||||
| Apixaban | ||||
| Acetylsalicylic acid | ||||
| Atorvastatin | ||||
| Candesartan | ||||
| Clopidogrel | Possible increase in active metabolite of clopidogrel concentration | |||
| Dabigatran | ||||
| Dalteparin | ||||
| Digoxin | ||||
| Doxazosin | ||||
| Empagliflozin | ||||
| Enalapril | ||||
| Enoxaparin | ||||
| Eplerenone | Possible increase in eplerenone concentration | |||
| Ezetimibe | ||||
| Furosemide | ||||
| Ivabradine | Possible increase in ivabradine concentration | |||
| Labetalol | ||||
| Lisinopril | ||||
| Losartan | ||||
| Lovastatin | Possible increase in lovastatin concentration | |||
| Metoprolol | ||||
| Nebivolol | ||||
| Omega-3 | ||||
| Prasugrel | ||||
| Propafenone | Possible increase in simvastatin concentration | |||
| Ramipril | ||||
| Rivaroxaban | Increase in rivaroxaban concentration | |||
| Rosuvastatin | ||||
| Simvastatin | Possible increase in simvastatin concentration | |||
| Spironolactone | ||||
| Tadalafil | Possible increase in tadalafil concentration | |||
| Telmisartan | ||||
| Ticagrelor | Possible increase in ticagrelor concentration | |||
| Torasemide | ||||
| Valsartan | ||||
| Varfarin |
| Cardiovascular Drug | Concerns About Possible Interaction | Proposed Strategy |
|---|---|---|
| Amiodarone | There is a risk of serious toxicity AND stopping the drug does not mitigate the interaction due to amiodarone’s prolonged half-life | Do not use nirmatrelvir/ritonavir (consider a different antiviral drug, if possible and available) |
| Other antiarrhythmic drugs as propafenone, quinidine, and dronedarone | There is a risk of serious toxicity | Administrate nirmatrelvir/ritonavir ONLY if the other drug can be safely paused or replaced. Resume the other drug 3–5 days after stopping nirmatrelvir/ritonavir |
| Rivaroxaban, apixaban, ticagrelor, and clopidogrel | There is a risk of serious toxicity | Administrate nirmatrelvir/ritonavir ONLY if the other drug can be safely paused or replaced; resumption is possible 3–5 days after stopping nirmatrelvir/ritonavir. Acetylsalicylic acid and prasugrel remain safe antiplatelet drugs; low-molecular-weight heparins remain safe anticoagulant drugs |
| Warfarin (acenocumarole) and dabigatran | Toxicity is possible | If possible, before administering nirmatrelvir/ritonavir, stop and replace the other drug (low-molecular-weight heparins remain a safe alternative). Dose reduction (dabigatran) or close monitoring (VKA) remain acceptable management strategies. Resumption of cardiovascular drugs is possible 3–5 days after stopping nirmatrelvir/ritonavir |
| Lercanidipine | There is a risk of serious toxicity | Administer nirmatrelvir/ritonavir ONLY if the other drug can be safely paused or replaced; resumption is possible 3–5 days after stopping nirmatrelvir/ritonavir |
| Other calcium channel blockers than lercanidipine | Toxicity is possible | Monitoring blood pressure values (discontinuing the drug in case of excessive drop in blood pressure) seems to be an acceptable treatment strategy |
| Eplerenone | There is a risk of serious toxicity | Administer nirmatrelvir/ritonavir ONLY if the other drug can be safely paused or replaced; resumption is possible 3–5 days after stopping nirmatrelvir/ritonavir. Spironolactone remains a safe alternative |
| Lovastatin and simvastatin | There is a risk of serious toxicity | Administer nirmatrelvir/ritonavir ONLY if the other drug can be safely paused or replaced; resumption is possible 3–5 days after stopping nirmatrelvir/ritonavir. Pravastatin, fluvastatin, and pitavastatin remain safe alternatives. Ezetimibe also seems to remain safe, as does fenofibrate |
| Atorvastatin and rosuvastatin | Toxicity is possible | If possible, before administering nirmatrelvir/ritonavir, stop and replace the other drug (see above). Resumption is possible 3–5 days after stopping nirmatrelvir/ritonavir |
| Ivabradine, Ranolazine, Tadalafil, and Sildenafil (pulmonary hypertension) | There is a risk of serious toxicity | Administer nirmatrelvir/ritonavir ONLY if the other drug can be safely paused or replaced; resumption is possible 3–5 days after stopping nirmatrelvir/ritonavir. In case of ivabradine and ranolazine, temporarily discontinuing the drug seems to be a reasonable course of action. In the context of pulmonary hypertension therapy, consultation with a reference center seems to be warranted |
| Sacubitryl/valsartan, indapamid, and doxazosine | Toxicity is possible | Monitoring blood pressure values (discontinuing the drug in case of excessive drop in blood pressure) seems to be an acceptable treatment strategy |
| Rifampicine (infectious endocarditis) | There is a risk of serious toxicity AND stopping the drug does not mitigate the interaction due to prolonged half-life | Do not use nirmatrelvir/ritonavir (consider a different antiviral drug, if possible and available) |
| Digoxin | Toxicity is possible | If possible, before administering nirmatrelvir/ritonavir, stop and replace the other drug. Resumption is possible 3–5 days after stopping nirmatrelvir/ritonavir |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wełnicki, M.; Mamcarz, A.; Kuchar, E.; Mitkowski, P.; Jaroszewicz, J.; Tomasiewicz, K.; Gąsior, M.; Leszek, P.; Kamiński, K.A.; Wysocki, J. The Impact of COVID-19 and the Practical Importance of Vaccinations and Nirmatrelvir/Ritonavir for Patients with Cardiovascular Disease. Vaccines 2025, 13, 554. https://doi.org/10.3390/vaccines13060554
Wełnicki M, Mamcarz A, Kuchar E, Mitkowski P, Jaroszewicz J, Tomasiewicz K, Gąsior M, Leszek P, Kamiński KA, Wysocki J. The Impact of COVID-19 and the Practical Importance of Vaccinations and Nirmatrelvir/Ritonavir for Patients with Cardiovascular Disease. Vaccines. 2025; 13(6):554. https://doi.org/10.3390/vaccines13060554
Chicago/Turabian StyleWełnicki, Marcin, Artur Mamcarz, Ernest Kuchar, Przemysław Mitkowski, Jerzy Jaroszewicz, Krzysztof Tomasiewicz, Mariusz Gąsior, Przemysław Leszek, Karol Adam Kamiński, and Jacek Wysocki. 2025. "The Impact of COVID-19 and the Practical Importance of Vaccinations and Nirmatrelvir/Ritonavir for Patients with Cardiovascular Disease" Vaccines 13, no. 6: 554. https://doi.org/10.3390/vaccines13060554
APA StyleWełnicki, M., Mamcarz, A., Kuchar, E., Mitkowski, P., Jaroszewicz, J., Tomasiewicz, K., Gąsior, M., Leszek, P., Kamiński, K. A., & Wysocki, J. (2025). The Impact of COVID-19 and the Practical Importance of Vaccinations and Nirmatrelvir/Ritonavir for Patients with Cardiovascular Disease. Vaccines, 13(6), 554. https://doi.org/10.3390/vaccines13060554