Abstract
Background: Children with disabilities, particularly in low- and middle-income countries (LMICs), face heightened risks of vaccine-preventable diseases due to a range of systemic and social barriers. Although immunization is a fundamental human right and a proven public health intervention, this vulnerable group is often overlooked in policy and practice. Understanding the factors compromising vaccine equity for these children is critical to reducing zero-dose prevalence and improving health outcomes. Methods: This scoping review examined peer-reviewed, gray literature from 2010 to 2024. Searches were conducted in PubMed, Google Scholar, and relevant organizational reports (WHO, UNICEF). Studies addressing children with disabilities and focusing on immunization barriers, interventions, or lessons learned were selected. English-language publications were screened in title/abstract and full-text stages. Key data extracted included population, barriers, and immunization outcomes. Since this review focused on articles in English, this is a key limitation. Results were synthesized thematically to identify recurring patterns and to guide improved interventions and policies. Results: Twelve articles met the inclusion criteria. Key barriers identified were inadequate healthcare infrastructure, insufficient provider training, limited follow-up services in rural regions, societal stigma, and pervasive misconceptions around both disability and vaccines. Factors such as maternal education, logistical support for caregivers, and using low-sensory, inclusive vaccination settings were consistently linked with better outcomes. Effective strategies included mobile vaccination units, tailored interventions (e.g., distraction or sedation techniques), school-based immunization programs, and robust community engagement to address stigma. Lessons learned underscored the importance of flexible, individualized care plans and empowering families through transparent communication. Conclusions: Children with disabilities continue to experience significant gaps in immunization coverage, driven by intersecting barriers at the individual, health system, and societal levels. Scaling tailored interventions, inclusive policies, strengthened infrastructure, and ongoing research can help ensure these children receive equitable access to life-saving vaccinations.
1. Introduction
Immunization is widely recognized as one of the most effective public health interventions to prevent infectious diseases, particularly among children [1]. Vaccines have been critical in reducing mortality and morbidity from vaccine-preventable diseases, significantly improving global health outcomes. However, achieving high immunization coverage remains a challenge, especially in low- and middle-income countries (LMICs) [2], where barriers such as geographical remoteness, poverty, limited healthcare infrastructure, and resource constraints hinder access to life-saving vaccines [3]. Within these populations, certain groups face even more significant obstacles, including children with disabilities, who are often excluded from mainstream health services due to systemic gaps and societal stigma [4,5,6].
Children with disabilities face significant barriers to accessing healthcare, including immunization, due to physical, environmental, and cultural challenges. In LMICs, these children are less likely to receive timely vaccinations, partly because of inadequate healthcare facilities, a lack of disability-inclusive services, logistics, and societal discrimination. For example, Thota et al. revealed that research on improving access to healthcare for children with disabilities in LMICs is lacking in several critical areas, including the provision of general health services and the accessibility of healthcare settings [7]. Their evidence and gap mapping highlighted the need for more effective interventions in areas such as non-discrimination, tackling harmful stereotypes, and ensuring access to essential services like water, sanitation, and hygiene [7]. The study also identified gaps in policies and programs that promote inclusion and participation, which are essential for ensuring that children with disabilities can fully enjoy their rights, including the right to health, as outlined in international frameworks like the Convention on the Rights of the Child (CRC). Immunization, as a fundamental human right, must be accessible to all children, including those with disabilities, to protect them from preventable diseases and reduce their disproportionate health risks.
Numerous studies reveal significant gaps in immunization coverage between children with disabilities and their non-disabled peers, even in countries with robust health systems and strong immunization programs. For example, in the UK, Emerson et al. found that children with intellectual disabilities were less likely to be fully vaccinated compared to their peers without disabilities [8]. The study, which analyzed data from the Millennium Cohort Study, showed that vaccination rates for children with intellectual disabilities were lower at the ages of nine months and three years, with these children being more than twice as likely to be non-vaccinated compared to non-disabled children [8]. This disparity persisted despite adjustments for socioeconomic factors. Similarly, O’Neill et al.’s review highlighted that 78% of studies across various countries, including the USA and the UK, found lower immunization uptake in children with disabilities [6]. The review emphasized that these vulnerabilities were often linked to various factors, including inadequate access to healthcare services, logistical barriers, and the broad and inconsistent definitions of disability used in different studies. For example, while some studies from the USA suggested no significant difference in vaccine uptake among children with special healthcare needs, other studies found that specific populations, such as children with spina bifida or autism, had notably lower vaccination rates [6]. These disparities, occurring even in high-income countries with established immunization programs, underscore the urgency of addressing this challenge, specifically in LMICs, where healthcare access and systems may be even more constrained.
This scoping review examined the factors contributing to disparities in immunization coverage for children with disabilities. We also aimed to identify effective strategies for designing and prioritizing immunization interventions to ensure that children with disabilities are included, aiming to reduce zero-dose children and reach underserved communities in LMICs. Additionally, the review assessed key lessons learned from past initiatives in delivering immunization programs to children with disabilities in LMICs.
2. Methods
2.1. Study Design
A scoping review of the available literature was conducted. The review was guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analysis Protocols (PRISMA-P) guidelines [9] and aligned with the Centre for Reviews and Dissemination (CRD) guidance for undertaking systematic reviews in healthcare [10].
2.2. Research Question and Study Eligibility
The population–concept–context (PCC) framework (Table 1) was used to set the eligibility criteria for the review question following recommendations from the Joanna Briggs Institute [11].

Table 1.
Population–concept–context framework for this scoping review.
This review addresses the two research questions outlined below.
1. What are the key barriers and systemic factors contributing to inequities in immunization coverage for children with disabilities globally?
2. What strategies have been identified or implemented to ensure children with disabilities are not left out by immunization programs?
2.3. Literature Sources
A search was conducted on the PubMed and Google Scholar electronic databases. Additional sources, such as grey literature and reports from WHO, UNICEF, and other relevant international organizations, were also consulted for relevant publications reporting routine immunization service delivery among children with disabilities.
2.4. Inclusion Criteria
This review included peer-reviewed publications on immunization access for children with disabilities published between 2010 and 2024. To be eligible, articles were required to focus on either barriers to immunization or strategies for improving access for children with disabilities. Only articles published in English were considered eligible. Studies were excluded if they did not address children with disabilities or did not relate to immunization access.
To address the varying definitions of disability across studies, this scoping review adopted the World Health Organization’s International Classification of Functioning, Disability, and Health (ICF) as its conceptual framework [12,13]. The ICF defines disability as an umbrella term encompassing impairments, activity limitations, and participation restrictions, where a health condition interacts with personal and environmental factors. In line with this holistic view, we included studies focusing on a broad range of physical, sensory, intellectual, and developmental disabilities. This approach is intended to capture the diverse experiences and needs of children who may face barriers to immunization due to their functional limitations or social/environmental constraints.
2.4.1. Operational Criteria
Physical disabilities: Conditions significantly limiting mobility or motor functions (e.g., cerebral palsy).
Sensory disabilities: Vision or hearing impairments that require specific accommodations (e.g., Braille materials, sign language interpretation).
Intellectual disabilities: Diagnosed conditions affecting cognitive functioning, such as Down syndrome or global developmental delay.
Developmental disabilities: Neurodevelopmental conditions like autism spectrum disorder (ASD), attention deficit hyperactivity disorder (ADHD), or other pervasive developmental delays.
2.4.2. Handling Varied Definitions During Screening
Inclusive Screening: We used broad search terms (e.g., “children with disabilities”, “special healthcare needs”, “neurodevelopmental disorders”, “physical impairment”) to capture studies even if they employed alternative or narrower definitions of disability.
Cross-Checking Against ICF: In cases where authors used non-standardized definitions (e.g., “children with learning difficulties” or “children with special needs”), we compared these descriptions against the ICF framework to verify whether the study population fit our overall criteria of functional impairment and potential participation restrictions.
Contextual Judgement: When an article’s definition of disability was ambiguous, we reviewed the detailed methods and population characteristics to determine alignment with the ICF perspective. If the study population overlapped substantially with the recognized categories of disability outlined above, the article was retained.
2.4.3. Rationale
By grounding our inclusion criteria in the ICF, we aimed to avoid overly restrictive or overly broad definitions of disability, thus maximizing relevance and comparability among included studies. This ensures we capture the multifaceted nature of disability (biological, psychological, social) and retain studies that reflect the diverse obstacles and facilitators to immunization.
This clear operationalization allows for a consistent interpretation of “children with disabilities” and mitigates the risk of excluding relevant subgroups who might not neatly fit a single diagnostic label. It also promotes transparency in how we approached articles that used differing or less-formalized disability definitions.
2.5. Search Strategy
The search strategy was co-developed and pilot-tested with the assistance of a senior health science librarian and pediatrician. The search strategy accounted for the number of terms used to describe disability, incorporating broad descriptors and specific diagnoses to ensure a comprehensive search of disability literature. The search terms included a combination of keywords and medical subject headings (MeSH), such as “children with disabilities”, “immunization”, “health equity”, “vaccination access”, and “zero-dose children”. The strategy was tailored to each database to ensure comprehensive retrieval of relevant studies. The search dates included 2010 to 2024.
2.6. Title, Abstract, and Full-Text Screening
Two independent reviewers screened titles, abstracts, and full-text articles for eligibility. Studies identified through database searches were exported to EndNote [14]. Duplicate articles were removed. Studies were then exported from EndNote to the Covidence systematic review management platform [15]. This desk review followed the PRISMA-P guidelines.
2.7. Data Abstraction and Analysis
A customized data extraction form was developed to systematically collect information from each eligible study. Extracted data points included author(s), publication year, study design, study location, population characteristics, barriers identified, strategies implemented, key findings, and conclusions. The extracted data were analyzed thematically to identify common patterns and recurring themes related to immunization coverage and access for children with disabilities. These themes were then categorized under the PCC framework to better understand the interplay between systemic barriers, strategies for improvement, and the context of immunization programs. The analysis also considered lessons learned from past initiatives, focusing on actionable insights that can inform future interventions to improve immunization equity for children with disabilities.
2.8. Justification of Exclusion Criteria
The exclusion of 102 articles during the screening process was based on rigorous criteria to ensure relevance and quality. At the abstract level, studies were excluded if they did not specifically address immunization for children with disabilities or if the focus was unrelated to barriers, strategies, or lessons learned in improving vaccine access. For example, articles discussing general healthcare systems without mentioning vaccination programs or disability-inclusive practices were excluded. At the full-text level, studies were excluded if they lacked primary data, provided only anecdotal evidence, or did not meet quality appraisal benchmarks, such as unclear methodologies or small, unrepresentative sample sizes. For instance, a study focusing on adult vaccination programs with a brief mention of childhood immunization was excluded due to insufficient relevance. These exclusion criteria were applied consistently to maintain the integrity and focus of the review.
3. Results
3.1. Characteristics of Included Studies
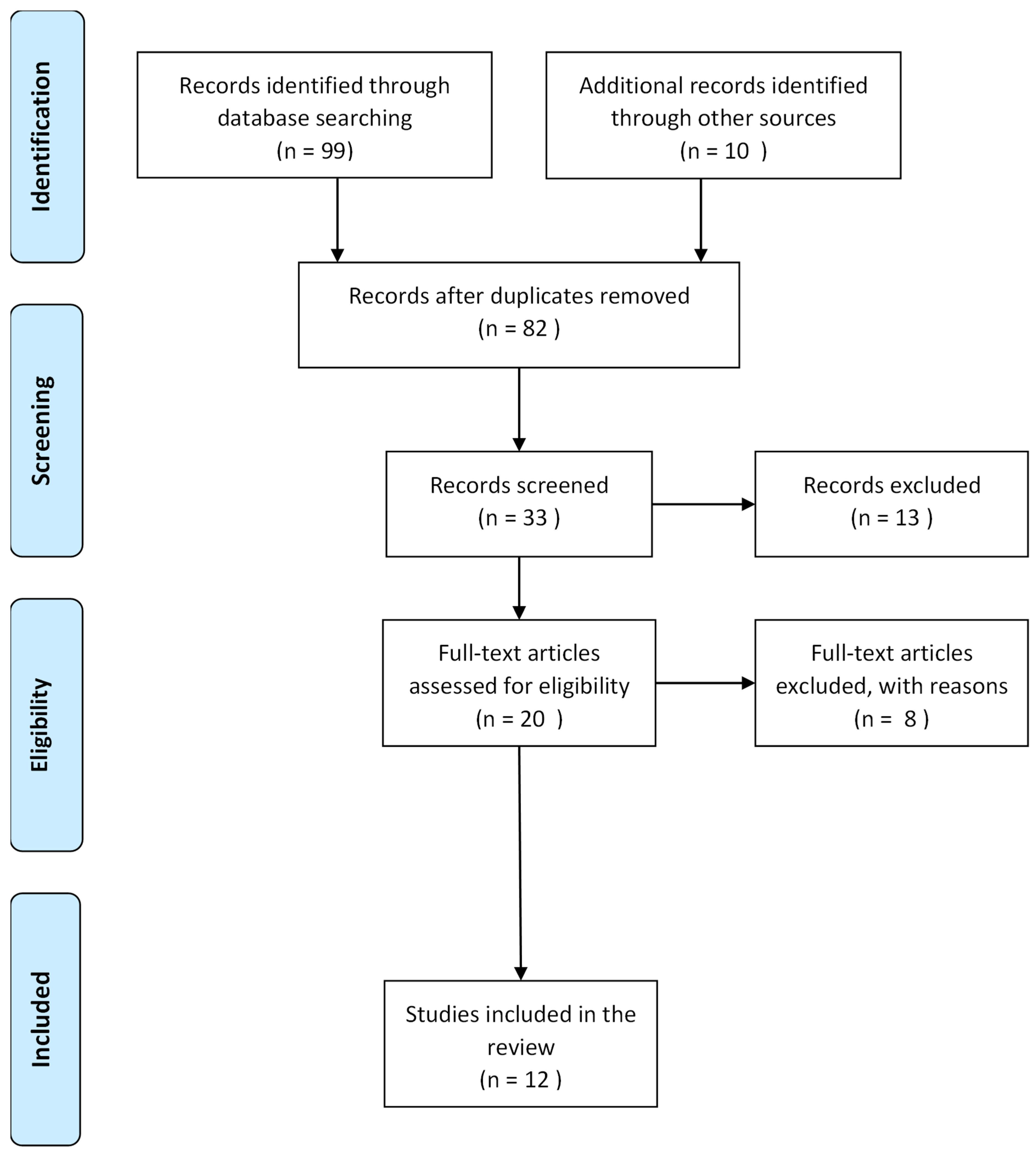
Our search retrieved 109 articles. After removing duplicates, 82 articles remained. Upon screening, 49 articles were removed at the title screening stage, 13 at the abstract screening stage, and another eight at the full-text screening stage, leaving 12 articles for inclusion in this scoping review [16,17,18,19,20,21,22,23,24,25,26,27] (Figure 1). Table 2 provides more details on the characteristics of the included articles. The data were synthesized into three themes, and Table 3 provides more details.
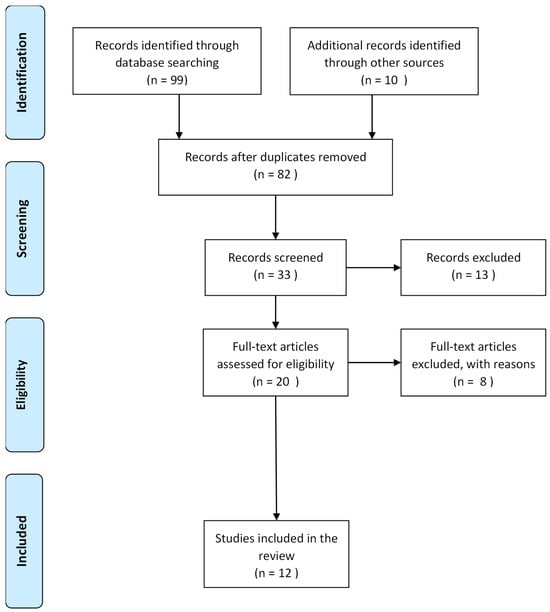
Figure 1.
PRISMA flow chart of the selection of studies included in the analysis.
Table 2.
Characteristics of studies included in the analysis.
Table 3.
Barriers and systemic factors that contribute to inequities in immunization coverage for children with disabilities.
3.2. Barriers and Systemic Factors That Contribute to Inequities in Immunization Coverage for Children with Disabilities
The findings from the studies on immunization coverage inequities for children with disabilities were categorized into two primary themes: barriers related to healthcare systems and social factors, and the influence of education, stigma, and misconceptions. These themes reflect the multifaceted nature of inequities in vaccination access for children with disabilities and highlight systemic and societal challenges that contribute to lower immunization rates. Both themes highlight the intersectionality of healthcare accessibility and societal attitudes, which contribute to the inequities faced by children with disabilities in accessing immunization services. Our review revealed that barriers and systemic factors contributing to inequities in immunization coverage for children with disabilities include healthcare system challenges and social factors, such as the failure to obtain parental consent, logistical issues in schools with limited resources, and a lack of staff expertise in managing children’s anxiety and disruptive behavior during immunization. The absence of follow-up protocols and insufficient communication with parents further complicate the process. Additionally, geographical and financial constraints limit access to immunization services, particularly in rural or underserved areas, while humanitarian efforts often overlook the special needs of children with disabilities. Education-related factors also play a significant role, as misconceptions, such as the belief that vaccines cause autism, can lead to delayed or missed vaccinations. Stigma surrounding disabilities and the low educational attainment of caregivers, especially mothers, contribute to lower vaccination rates, as does the lack of awareness about available rehabilitation services. These systemic challenges combine to create significant barriers to equitable vaccination for children with disabilities.
- A.
- Barriers related to healthcare systems and social factors
The first theme, barriers related to healthcare systems and social factors, is deeply rooted in the accessibility and responsiveness of health services. One key issue is the lack of resources and preparation in health facilities, which often fails to accommodate the specific needs of children with disabilities. Studies by Ong et al. (2024) [18] and Tuckerman (2024) [17] identify inadequate staff training and lack of preparation techniques as significant obstacles, particularly in LMICs with limited healthcare infrastructure. For instance, children with needle phobia, common in those with autism and ADHD, experience heightened anxiety and unsuccessful vaccination attempts, which further discourage participation in immunization programs. Additionally, the inconsistency in follow-up services, especially in rural areas, creates a barrier to maintaining vaccination schedules. Ong et al. (2024) also point out the absence of specialized services tailored for children with disabilities, which exacerbates the challenge of ensuring equitable access to immunization [18]. This systemic neglect can lead to physical and psychological barriers, such as failed vaccination attempts and the resultant avoidance of vaccination by parents and children. Furthermore, such problems as the miscategorization of symptoms, particularly in children with severe disabilities like cerebral palsy or epilepsy, contribute to lower vaccination uptake, as documented in Okoro’s study [22]. These healthcare-system-related inadequate healthcare resources and the lack of stable, accessible services in many LMICs compound barriers.
- B.
- The influence of education, stigma, and misconceptions
The included studies underscored how societal attitudes and knowledge gaps exacerbate inequities in immunization coverage. Okoro et al. [22] highlighted that maternal education levels strongly correlate with higher vaccination rates, suggesting that a lack of knowledge about the benefits and safety of vaccines is a key driver of inequity. In many cases, parents’ limited understanding, compounded by misinformation or myths about vaccines, particularly those related to intellectual disabilities, leads to delayed or omitted vaccinations. Rosenberg (2013) discusses how parents of children with autism spectrum disorder (ASD) may delay vaccinations due to misconceptions about vaccines causing autism [19]. This mistrust is more prevalent among highly educated mothers, who may be more susceptible to misinformation. Similarly, Tuckerman (2024) identifies that parents from culturally and linguistically diverse (CALD) backgrounds may face difficulties navigating vaccination systems, resulting in a lower immunization uptake for their children with disabilities [17]. Stigma also plays a significant role, as children with more visible disabilities, such as cerebral palsy, often face social exclusion and discrimination, leading to lower vaccination rates. In comparison, children with less-visible disabilities tend to have higher vaccination rates [22]. This stigma can affect both the willingness of parents to seek vaccinations for their children and the attitude of healthcare providers toward these children.
3.3. Strategies That Have Been Identified or Implemented to Ensure Children with Disabilities Are Reached by Immunization Programs, and How These Can Be Scaled or Improved
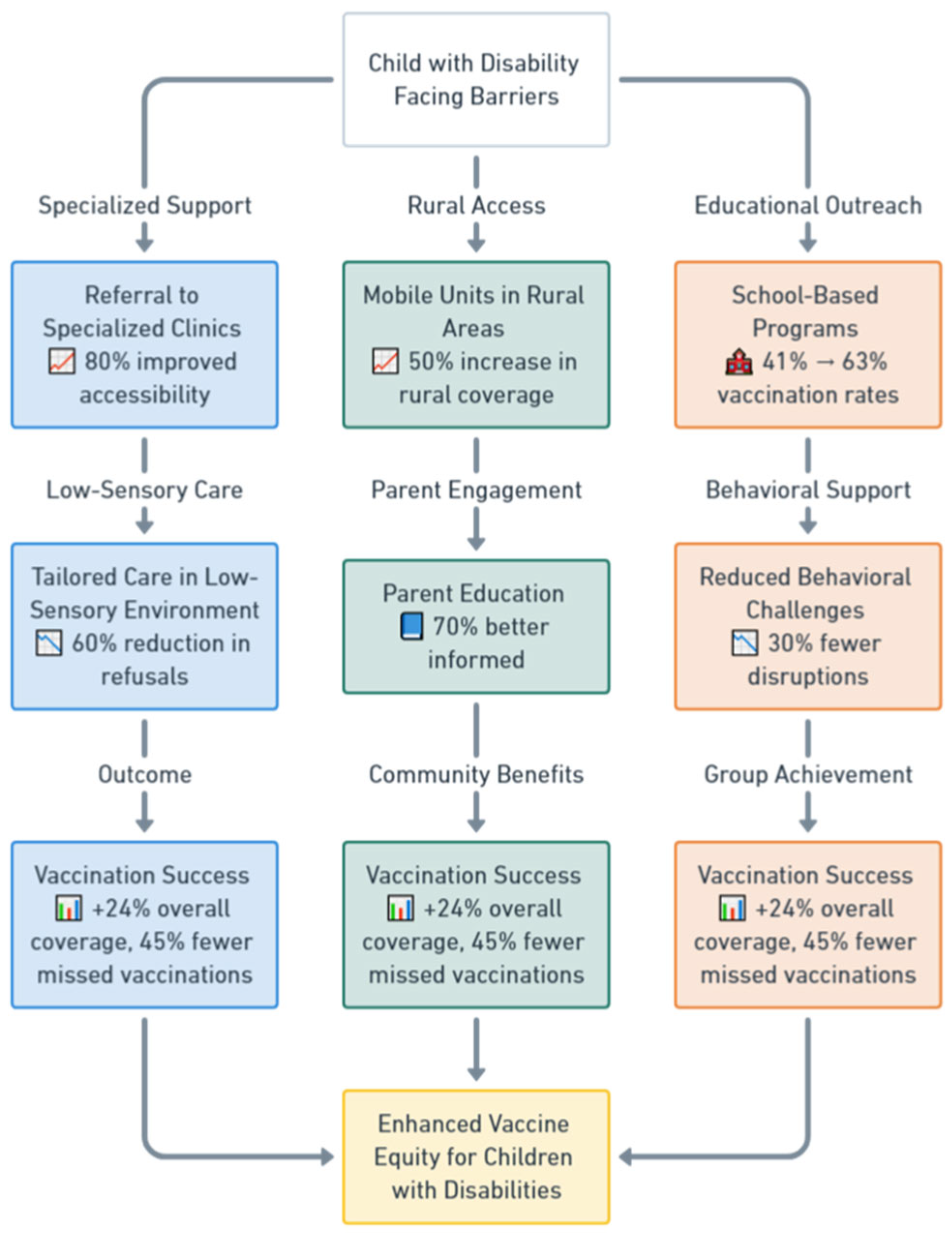
The strategies identified in the studies to improve immunization coverage for children with disabilities and reduce the number of zero-dose children were categorized into three primary themes: enhancing healthcare accessibility and service delivery, implementing tailored interventions for children with disabilities, and addressing societal factors like stigma and education (Table 4). Each theme had sub-themes that could be scaled and improved to ensure more children with disabilities are reached by immunization programs. Figure 2 illustrates a flowchart describing the tailored immunization pathways for children with disabilities.
Table 4.
Strategies that have been identified or implemented to ensure children with disabilities are reached by immunization programs, and how can these be scaled or improved.
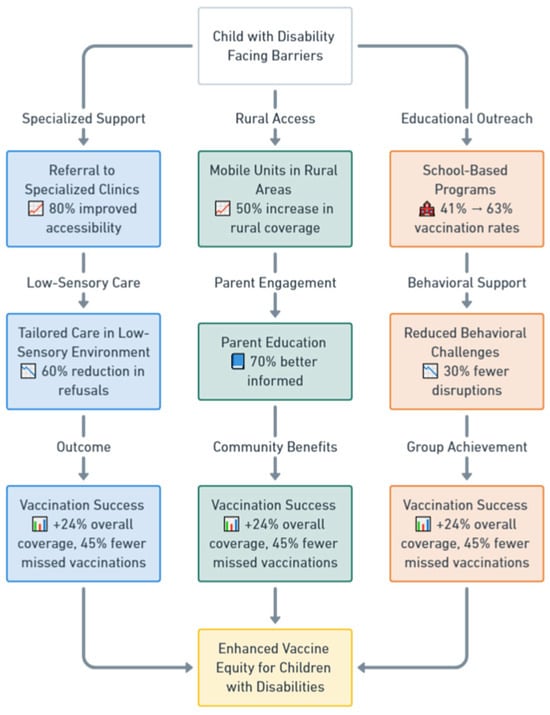
Figure 2.
The flowchart illustrates the tailored immunization pathways for children with disabilities, starting with the central challenge, “Child with Disability Facing Barriers”. It features three main pathways: Specialized Support, Rural Access, and Educational Outreach. The Specialized Support pathway includes referrals to specialized clinics with 80% improved accessibility, leading to tailored care in low-sensory environments, which reduces vaccination refusals by 60%, and culminates in vaccination success, marked by + 24% overall coverage and 45% fewer missed vaccinations. The Rural Access pathway utilizes mobile units in rural areas, achieving a 50% increase in rural vaccination coverage, followed by parent education initiatives, where 70% of parents report being better informed, resulting in similar vaccination success outcomes. The Educational Outreach pathway employs school-based programs, improving vaccination rates in specialist schools from 41% to 63%, coupled with behavioral support that reduces disruptions by 30%, ultimately leading to vaccination success. The pathways converge on the goal of Enhanced Vaccine Equity for Children with Disabilities. Icons enhance clarity, such as a hospital symbol for specialized clinics, a book for parent education, and a school for school-based programs. Metrics, such as “80% improved accessibility” and “70% better informed”, are based on study findings. At the same time, the color coding—blue for specialized support, green for rural access, and orange for educational outreach—helps differentiate pathways visually. The outcome emphasizes significant improvements in coverage and equity for children with disabilities.
- A.
- Enhancing healthcare accessibility and service delivery
The first theme, enhancing healthcare accessibility and service delivery, highlights the importance of creating systems that accommodate the specific needs of children with disabilities. The included studies emphasized the need for better service infrastructure, particularly in underserved and rural areas. Tuckerman (2024) suggests that creating individualized approaches for children, including supporting parents to navigate the vaccination process, can help address gaps in follow-up services [17]. Similarly, Ong et al. (2024) highlight the value of mobile units or temporary vaccination clinics to bring services closer to families, thereby overcoming logistical barriers to accessing immunization [18]. This is complemented by Fong (2024) [20], who recommends administering vaccines in low-sensory environments to minimize anxiety and discomfort. These strategies ensure that children with disabilities are not excluded from immunization programs due to geographical, logistical, or environmental challenges.
- B.
- Implementing tailored interventions for children with disabilities
The second theme, implementing tailored interventions for children with disabilities, focuses on making the vaccination process more manageable for children and parents. Several studies propose using distraction and sedation techniques to reduce anxiety and pain during vaccination. Ong et al. (2024) describe a “Difficult to Vaccinate” clinical pathway, which includes these strategies and ensures that children with disabilities are not excluded due to their unique needs [18]. Bray (2022) also identifies various distraction techniques, such as using handheld devices for entertainment, music therapy, or squeezing soft objects, which have proven effective in reducing anxiety [21]. Moreover, the involvement of parents in the vaccination process can significantly improve outcomes. Parental involvement, as emphasized in both Bray (2022) [21] and Okoro (2015) [22], not only provides emotional security for children but also empowers parents to make informed decisions about vaccination, such as whether to use sedatives or other techniques.
- C.
- Addressing societal factors like stigma and education
Addressing societal factors like stigma and education, the third theme emphasizes tackling misconceptions and promoting understanding about disabilities and vaccines. Okoro (2015) suggests that healthcare workers should be trained to avoid misclassifying disabilities as contraindications to vaccination, which often leads to missed opportunities for immunization [22]. Regular health education campaigns are also recommended to dispel myths and build trust in vaccination programs. Tuckerman (2024) further underscores the need for accessible and understandable information for parents, especially those with low literacy or intellectual disabilities, to ensure they can navigate the vaccination process [17]. Additionally, addressing socioeconomic disparities, as highlighted by Okoro (2015), is crucial in ensuring equitable access to immunization for all children [22]. Policies that promote maternal education and provide financial support can help improve vaccine uptake, particularly in families with lower incomes or those from disadvantaged backgrounds [16].
3.4. Lessons Learned in Ensuring Equitable Access for Children with Disabilities
The included studies highlighted several vital lessons that were grouped into three key themes: creating supportive and inclusive environments, empowering families and children, and tailoring immunization services to individual needs (Table 5).
Table 5.
Lessons learned in ensuring equitable access for children with disabilities.
- A.
- Creating supportive and inclusive environments
The first theme, creating supportive and inclusive environments, emphasizes ensuring vaccination settings are accessible and welcoming for children with disabilities. Tuckerman (2024) highlights that involving school staff in the vaccination process can create a supportive environment, as schools are often seen as “safe spaces” by both parents and children, making them an ideal setting for vaccinations [17]. The physical environment also plays a crucial role, as children with disabilities, particularly those with sensory sensitivities, can experience heightened anxiety during vaccinations. Creating a calm, quiet, and non-threatening space is essential to reduce this anxiety. Bray (2022) underscores the significance of offering comforting techniques, such as allowing a parent to be present or using engaging distractions like toys or music, to alleviate stress and encourage vaccination [21]. Additionally, Ong et al. (2024) stress the importance of flexible and individualized care, where the needs of the child, such as sensory sensitivities or past negative experiences, are considered when designing vaccination procedures [18]. This approach ensures that children are more likely to undergo successful vaccinations without unnecessary distress.
- B.
- Empowering families and children
The findings of this review revealed that empowering families and children, focusing on the importance of involving parents in the vaccination process, and providing them with the tools and knowledge to advocate for their children’s needs were key to the program’s success. Ong et al. (2024) note that parental empowerment is a key strategy, where parents feel more confident and capable when they are provided with clear information and involved in decision-making, especially when it comes to the use of techniques like distraction or sedation [18]. This empowerment helps address vaccine hesitancy, as parents are better informed and more comfortable with the vaccination process. Bray (2022) also highlights the value of communication, noting that honest and transparent conversations between healthcare providers and parents are essential for building trust and reducing anxiety [21]. Parents can feel better equipped to manage their child’s healthcare needs in the long term when provided with ongoing support and addressing concerns about future vaccinations. This sense of empowerment can also extend to the children themselves, as preparing them with appropriate information and expectations can help them cope better with the vaccination process [16,18,21].
- C.
- Tailoring immunization services to individual needs
This review also revealed that tailoring immunization services to individual needs emphasizes the necessity of adapting healthcare practices to accommodate the unique challenges faced by children with disabilities and is key to program success. Bray (2022) advocates for a neurodiversity-sensitive approach, where healthcare providers are educated about the specific needs of children with conditions such as autism or ADHD [21]. This ensures that healthcare providers respect individual differences and provide care that is not only effective but also compassionate. Tailoring immunization strategies, such as distraction techniques or providing sensory-friendly environments, can help children with neurodevelopmental disorders feel more comfortable and less anxious. Furthermore, both Tuckerman (2024) and Ong et al. (2024) point out that individualized planning, including offering multiple preparation options for both parents and children, increases the likelihood of successful vaccination [17,18]. These personalized approaches, whether through social stories or flexibility in the vaccination setting, ensure that children with disabilities are not excluded from immunization programs due to their unique needs.
4. Discussion
This review identifies key barriers and strategies for improving immunization coverage among children with disabilities and reducing zero-dose children, particularly in underserved and marginalized communities. The findings highlight the complex, multifaceted nature of the issue and offer valuable insights into how immunization programs can be designed and improved to ensure that children with disabilities are not excluded.
The barriers identified in this review emphasize the critical gaps in healthcare systems, social support, and societal attitudes toward disabilities. These barriers include inadequate healthcare resources, lack of staff training, and inconsistencies in healthcare service delivery, especially in rural areas. Misunderstandings about disabilities and their medical implications can lead to misclassification as vaccine contraindications, further discouraging vaccination efforts [17,22]. Furthermore, inadequate follow-up care and logistical challenges like unclear clinic locations and access issues contribute to missed vaccinations. These barriers underscore the need for comprehensive strategies at multiple health system levels. Strategies to address these barriers focus on enhancing accessibility and service delivery, particularly in underserved regions. Mobile vaccination units and strengthening infrastructure in rural areas are essential for reaching remote communities [18]. Logistical support, including clear signage and support for parents to navigate the vaccination process, is critical for reducing barriers to vaccination [21]. Moreover, creating low-sensory environments for vaccination, which alleviate anxiety for children with disabilities, is another essential strategy for improving immunization outcomes [18]. At the health facility level, offering individualized care through distraction and sedation techniques and the involvement of parents in decision-making can significantly increase vaccination uptake [21].
Designing immunization programs to reduce zero-dose children and ensure equitable access requires addressing the systemic and social factors that prevent children with disabilities from receiving vaccines [6]. The findings suggest that creating supportive and inclusive environments is key to improving immunization rates. Involving school staff in vaccination planning can help provide a safe and trusted space for both children and parents, making vaccination efforts more accessible [17]. Schools can be critical in ensuring a supportive environment, especially when parents perceive them as safe spaces [28,29]. Health systems should adapt to provide calm, non-threatening vaccination spaces, especially for children with sensory sensitivities, and use comforting techniques like toys or music to reduce anxiety [30].
This review revealed empowering families, particularly parents, as another critical strategy. Similarly, earlier work highlighted that providing parents with the knowledge and support to navigate the vaccination process, alongside involving them in decision-making regarding vaccination techniques, can reduce vaccine hesitancy and increase confidence in vaccination programs [31]. Transparent communication addresses concerns and ensures families feel supported throughout the vaccination journey [32]. The need for tailored, individualized care was a recurrent theme in this review. This includes designing personalized vaccination pathways considering each child’s medical, psychological, and developmental needs. Previous research by Leask 2006 and Helps 2019 highlighted the need for healthcare providers to receive training on neurodiversity to offer more respectful and accommodating care for children with neurodevelopmental disorders like autism or ADHD [33,34]. Tailoring immunization strategies to address the specific needs of these children is essential for improving vaccination outcomes.
4.1. Intersecting Stigma, Socioeconomic Disparities, and Disability
According to our review, stigma and socioeconomic disparities might intersect with disability to create compounded barriers to immunization. Stigma associated with disability often results in social exclusion, which limits access to healthcare services, including vaccination programs. Families of children with disabilities may face discrimination within their communities, further deterring them from seeking healthcare. This stigma is amplified in lower socioeconomic settings, where families may lack the financial resources to navigate systemic barriers or afford transportation to healthcare facilities. Additionally, limited parental education and cultural misconceptions about both disability and vaccines exacerbate these challenges, leading to reduced awareness of immunization benefits. For example, families living in poverty may prioritize immediate financial needs over healthcare, while stigma can prevent them from accessing community-based interventions. Addressing these intersecting issues requires a multi-faceted approach that includes anti-stigma campaigns, socioeconomic support programs, and culturally tailored community engagement initiatives. Such efforts can promote inclusive environments where families feel supported and empowered to seek immunization for their children, regardless of disability or economic status.
The intersection of disability with other identities, such as gender and ethnicity, compounds barriers to immunization access. Girls with disabilities, for instance, often face heightened discrimination due to societal biases that prioritize male children for healthcare resources in specific cultural contexts. Similarly, ethnic minority groups, such as Indigenous populations in Latin America or tribal communities in South Asia, may experience systemic exclusion from healthcare services. When combined with disability, these factors exacerbate inequities, leading to lower vaccination rates among these subgroups. Language barriers, geographic isolation, and mistrust in healthcare systems further hinder access for ethnically marginalized children with disabilities. For example, Indigenous children with disabilities may lack access to culturally tailored immunization programs, reinforcing health disparities. Addressing these intersecting barriers requires intersectional approaches that account for these populations’ unique needs and experiences, such as culturally sensitive outreach campaigns, gender-inclusive policies, and partnerships with community leaders to foster trust and inclusivity.
4.2. Practical Implementation, Scaling, and Evaluation of Identified Strategies
4.2.1. Tailored Interventions
To implement tailored interventions, healthcare providers can adopt strategies such as individualized vaccination plans and low-sensory environments in clinics. Training workshops and simulation exercises for healthcare workers can ensure sensitivity to the needs of children with disabilities. These interventions can be scaled through partnerships with organizations specializing in disability care, enabling consistent support across multiple regions.
4.2.2. Mobile Vaccination Units
Mobile units can address geographic barriers by bringing vaccines directly to underserved communities. These units should be equipped with accessibility features, such as ramps and quiet areas, and staffed by personnel trained in disability-inclusive care. Government funding and donor partnerships can help expand such programs nationally, with clear targets for reaching rural and marginalized populations.
4.2.3. Community Engagement
Local leaders, disability advocacy groups, and parent associations can co-design culturally sensitive education campaigns. These initiatives should include testimonials, visual aids, and multilingual materials to combat stigma and misconceptions. Pilot programs can test effectiveness before scaling to larger communities, with adjustments based on feedback from local stakeholders.
4.2.4. School-Based Vaccination Programs
Schools are ideal settings for reaching children with disabilities, particularly in specialized education environments. Policies supporting routine vaccination days, with individualized care plans and consent protocols, can streamline implementation. Scaling such programs requires collaboration between health and education ministries, alongside regular evaluations of student and caregiver satisfaction.
4.2.5. Adapting High-Income Country Strategies for Low- and Middle-Income Countries
High-income countries (HICs) have successfully implemented school-based vaccination programs, digital health records, and targeted outreach campaigns to improve immunization coverage among children with disabilities. For instance, school-based vaccination in specialist education settings in Australia has shown significant success by addressing behavioral challenges and reducing access barriers [28,35]. Similarly, using electronic health records in countries like Denmark and the United States enables efficient tracking of vaccine coverage and identification of under-vaccinated groups [36,37]. However, these approaches require adaptation to fit the unique challenges of LMICs. Resource limitations, infrastructural gaps, and cultural differences necessitate cost-effective modifications, such as using mobile vaccination units to reach underserved areas and employing community health workers for targeted outreach. By adopting lessons from HICs while incorporating the local context, LMICs can develop scalable, sustainable immunization programs that address the needs of children with disabilities effectively.
4.2.6. Monitoring and Evaluation (M&E)
The success of immunization programs in high-income and low- and middle-income countries underscores the importance of robust M&E frameworks. For instance, Australia’s school-based vaccination programs incorporate real-time electronic tracking systems that monitor vaccine coverage rates among students with disabilities, providing actionable data for targeted interventions [28,38]. In contrast, Uganda’s community health worker (CHW) model includes regular household surveys to assess immunization uptake and identify gaps in rural and underserved areas [39]. Metrics used in these programs include vaccination completion rates, caregiver satisfaction levels, and reductions in missed vaccination appointments. Additionally, participatory approaches, such as involving caregivers and disability advocates in program evaluations, ensure that M&E systems address the specific needs of children with disabilities. Incorporating these practices into future frameworks can enhance accountability and guide continuous improvement, particularly in resource-constrained settings.
4.2.7. Funding and Policy Advocacy
Securing sustainable funding is critical for scaling. Policymakers should allocate specific budget lines for disability-inclusive immunization programs, with international agencies offering technical and financial support. Advocacy campaigns can build momentum for inclusive immunization policies, leveraging the documented benefits of these strategies to demonstrate value.
4.3. Limitations of the Study
- A.
- Addressing data gaps
This review identified several critical data gaps that hinder a comprehensive understanding of immunization barriers for children with disabilities in LMICs. Notably, there is a lack of longitudinal studies that track vaccination coverage and health outcomes over time, making it difficult to assess the long-term effectiveness of interventions. Additionally, certain disability types, such as sensory impairments or rare developmental conditions, are underrepresented in the literature. This underrepresentation limits the generalizability of findings and may result in overlooked barriers or ineffective strategies for these subgroups. Furthermore, geographic disparities in research focus exist, with limited data from rural settings where systemic challenges are often more pronounced. To address these gaps, future research should prioritize inclusive study designs that encompass diverse disability types and settings, incorporate longitudinal methodologies, and focus on equity-driven outcomes to inform targeted and effective immunization policies.
Bridging the identified data gaps requires adopting innovative methodologies and forging strategic partnerships. Participatory action research (PAR) offers a promising approach, actively involving children with disabilities, their caregivers, and community stakeholders in designing and implementing studies [40]. This approach ensures that research questions and interventions are informed by lived experiences, fostering relevance and inclusivity. Additionally, longitudinal cohort studies can provide insights into the long-term effectiveness of strategies, such as tracking vaccination uptake and health outcomes across different disability types and settings. Partnerships with disability advocacy organizations, community health workers, and international agencies like WHO and UNICEF can facilitate resource sharing and capacity building, particularly in low- and middle-income countries. Leveraging technology, such as digital health records and geospatial mapping, can improve data collection, monitor immunization disparities, and identify underserved populations. By adopting these methodologies and partnerships, researchers can generate robust evidence to inform policy and practice, advancing equitable immunization coverage for all children.
- B.
- Methodological limitations and potential biases
The reviewed studies revealed several methodological limitations that may have influenced our findings. A significant issue was the reliance on convenience sampling, which often led to unrepresentative study populations, a lack of standard error measures, and selection bias. For example, families with greater access to healthcare or higher awareness of vaccination programs may have been more likely to participate, potentially overestimating vaccination coverage and underrepresenting those facing severe barriers. Additionally, many studies relied on self-reported data from caregivers, which is prone to recall bias and social desirability bias. Caregivers might overstate vaccine uptake to align with perceived social norms or expectations, especially when vaccination campaigns are highly promoted. Furthermore, variations in data collection methods and outcome definitions across studies make it challenging to compare results or draw generalizable conclusions. Addressing these biases in future research will require rigorous sampling techniques, standardized data collection tools, and the inclusion of diverse perspectives, particularly from underrepresented disability groups (i.e., sampling design).
Since only articles published in English were reviewed, it is possible that useful articles in other languages were excluded. It is important to note that this review did not examine whether vaccines were provided free of charge or if parents had to pay for them at the health facility. Additionally, only electronically available manuscripts were included in this review.
Another notable limitation is that this review utilized a search strategy that included only two electronic databases, PubMed and Google Scholar. While these databases are widely recognized for their extensive coverage of health-related literature, limiting the search to them may have excluded relevant studies indexed in other databases. Additionally, while efforts were made to enhance the robustness of the search by including gray literature from reputable organizations such as UNICEF and the World Health Organization, some pertinent studies may have been overlooked. Future reviews could benefit from a more comprehensive search strategy that includes multiple databases and a wider range of information sources to capture the full spectrum of relevant literature. Finally, a formal assessment of the risk of bias was not conducted due to the limited number of studies retrieved. This limitation suggests that the findings should be interpreted cautiously, as unexamined biases may influence the reported outcomes.
- C.
- Broader methodological discussion
A critique of the methodologies used in the reviewed studies reveals several notable limitations and biases within the field. Many studies relied heavily on cross-sectional designs, which provide only a snapshot of immunization barriers and outcomes. While helpful in identifying immediate issues, these designs fail to capture longitudinal trends, such as vaccine uptake changes over time or interventions’ long-term impacts. Additionally, the reliance on convenience sampling was prevalent, often resulting in unrepresentative study populations. For instance, children with severe or less-visible disabilities might have been underrepresented, as caregivers facing significant barriers may not participate in studies.
Another methodological limitation is information bias, which lies in inconsistent data collection tools and metrics. Studies varied widely in how they measured outcomes, such as vaccine coverage rates or caregiver perceptions, complicating comparisons across findings. Some studies used self-reported data from caregivers, which may introduce recall bias, while others lacked standard definitions for key concepts like “accessibility” or “barriers”.
Lastly, geographic and cultural contexts were often insufficiently addressed. Many studies conducted in LMICs lacked region-specific adaptations to account for unique barriers such as cultural stigma or infrastructural deficits. Similarly, limited participatory research approaches meant that the perspectives of children with disabilities and their families were not always incorporated into study designs or analyses. Addressing these methodological issues is crucial for developing robust, generalizable evidence for inclusive immunization programs.
- D.
- Inconsistencies in definitions
The variability in the definition of “disability” across the included studies posed challenges for both inclusion and analysis. Some studies defined disability narrowly, focusing on specific conditions such as intellectual disabilities or autism spectrum disorders, while others used broader definitions that included physical, sensory, and developmental disabilities. This inconsistency affected the comparability of findings, as interventions effective for one subgroup may not apply to others. For example, studies targeting children with physical disabilities emphasized environmental accessibility, whereas those involving neurodevelopmental disorders often focused on behavioral support and family engagement. These differing definitions also influenced the inclusion process; studies that lacked a clear or comprehensive definition of disability were excluded to maintain methodological rigor. Addressing this variability required careful thematic analysis to synthesize findings while acknowledging the heterogeneity in the study populations and outcomes.
4.4. Future Research Directions
Despite the insights gained from this review, multiple knowledge gaps hinder the development of inclusive immunization strategies for children with disabilities in LMICs. Addressing these gaps requires a concerted effort to expand the scope and improve the rigor of future research:
- A.
- Longitudinal and Rigorous Study Designs
Long-term impact: Current evidence on the effectiveness of interventions often relies on cross-sectional or short-term studies. Future studies should adopt longitudinal designs (e.g., cohort or panel studies) that track children over time, assessing how immunization uptake and caregiver attitudes evolve as children progress through various stages of the vaccination schedule.
Rigorous sampling: Many studies rely on convenience or opportunistic sampling methods, potentially excluding the most marginalized populations. Probability-based sampling and targeted outreach strategies (e.g., partnering with community health workers) can help capture more diverse participants, including those in remote rural settings.
- B.
- Understudied Disability Types
Visual and hearing impairments: Most existing studies focus on intellectual or physical disabilities, while sensory impairments, such as blindness or deafness, remain underexplored. These populations may face unique barriers to immunization, including communication challenges, inaccessible health education materials, and stigma or misconceptions.
Complex/multiple disabilities: Children with co-occurring conditions (e.g., autism spectrum disorder plus a physical disability) often have complex healthcare needs but are rarely included in research. Future investigations should aim to capture the intersectional experiences of these children, offering a more detailed understanding of how overlapping disabilities multiply barriers to immunization.
- C.
- Participatory and Community-Engaged Methods
Participatory action research (PAR): Engaging caregivers, children (where appropriate), community leaders, and disability advocates in designing and implementing studies can yield richer, more context-specific insights. This approach can also foster community ownership, improving the likelihood that recommended interventions are both practical and culturally acceptable.
Stakeholder involvement: Collaboration with local health authorities, schools, and NGOs specializing in disability services can ensure that interventions are feasible and sustainable within specific cultural and resource contexts.
- D.
- Standardization of Definitions and Outcome Measures
Adoption of the WHO ICF: Building on the work of this review, future studies should use the International Classification of Functioning, ICF, to operationalize disability consistently, thereby improving comparability across different research settings.
Aligned reporting of outcomes: Standardizing immunization coverage metrics (e.g., consistently defining “fully immunized”, “zero-dose”, and “dropout”) facilitates meta-analyses and cross-study comparisons. Clear outcome reporting also supports better monitoring and evaluation of interventions over time.
By prioritizing longitudinal research, inclusive sampling, standardized definitions, and participatory methods, the field can generate a more robust evidence base to inform policy and practice. These steps will not only deepen our understanding of immunization barriers experienced by children with diverse disability types but also drive the development of targeted, equitable, and sustainable solutions in low- and middle-income contexts.
5. Conclusions
In conclusion, the strategies to improve immunization coverage for children with disabilities include healthcare system reforms, tailored interventions, and societal awareness campaigns. Enhancing accessibility to services, adapting vaccination procedures to meet the needs of children with disabilities, and addressing stigma and education gaps were identified as essential strategies to ensure immunization programs can be more inclusive and effective in reaching children with disabilities. Scaling these strategies requires a concerted effort to adapt healthcare systems, train healthcare providers, and engage communities in creating a supportive environment for children with disabilities.
Call to Action for Inclusive Immunization
This study underscores the urgent need for governments, non-governmental organizations (NGOs), and researchers to prioritize inclusive immunization programs for children with disabilities. Governments should enact policies mandating disability-inclusive practices, allocate dedicated funding for tailored interventions, and incorporate accessibility metrics into national health surveys. NGOs can play a key role in implementing community-based programs, conducting caregiver education campaigns, and advocating for systemic change at local and global levels. Researchers must address data gaps by designing longitudinal studies, developing standardized definitions of disability, and ensuring the representation of under-served populations, including those with sensory impairments or living in rural areas.
Collaboration between these stakeholders is critical to scaling successful strategies, such as mobile vaccination units, low-sensory environments, and school-based programs, while promoting an evidence-based culture of continuous improvement. By taking these steps, the global health community can advance equitable vaccine access and strengthen healthcare systems to serve all children, regardless of their abilities.
Author Contributions
Conceptualization, G.M.; methodology, P.G.I. and O.M.; software, D.F.C. and F.D.M.; validation, O.M. and T.D. (Tapiwa Dhliwayo); writing—original draft preparation, G.M., D.F.C. and Z.M.; writing—review and editing, T.D. (Tapiwa Dhliwayo), P.G.I., O.M. and T.D. (Tafadzwa Dzinamarira); supervision, T.D. (Tafadzwa Dzinamarira). All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Acknowledgments
Authors acknowledge Pierre Gashema and Eric Saramba for their support with database searches.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Feikin, D.R.; Karron, R.A.; Saha, S.K.; Sparrow, E.; Srikantiah, P.; Weinberger, D.M.; Zar, H.J. The full value of immunisation against respiratory syncytial virus for infants younger than 1 year: Effects beyond prevention of acute respiratory illness. Lancet Infect. Dis. 2024, 24, e318–e327. [Google Scholar] [PubMed]
- Zhu, J.; Cole, C.B.; Fihman, J.; Adjagba, A.; Dasic, M.; Cernuschi, T. Opportunities to accelerate immunization progress in middle-income countries. Vaccine 2024, 42, S98–S106. [Google Scholar]
- Thaheem, A.K.; Qureshi, A.U.; Sarkar, A.; Liu, G. The Ripple Effect of Vaccines: Health, Economic, and Social Dimensions. J. Soc. Inform. Glob. Health 2023, 2, 40–48. [Google Scholar]
- Rice, I.; Opondo, C.; Nyesigomwe, L.; Ekude, D.; Magezi, J.; Kalanzi, A.; Kerac, M.; Hayes, J.; Robello, M.; Halfman, S. Children with disabilities lack access to nutrition, health and WASH services: A secondary data analysis. Matern. Child Nutr. 2024, 20, e13642. [Google Scholar]
- Mwangi, L.W.; Abuga, J.A.; Cottrell, E.; Kariuki, S.M.; Kinyanjui, S.M.; Newton, C.R. Barriers to access and utilization of healthcare by children with neurological impairments and disability in low-and middle-income countries: A systematic review. Wellcome Open Res. 2022, 6, 61. [Google Scholar]
- O’Neill, J.; Newall, F.; Antolovich, G.; Lima, S.; Danchin, M. Vaccination in people with disability: A review. Hum. Vaccines Immunother. 2020, 16, 7–15. [Google Scholar]
- Thota, A.B.; Mogo, E.I.; Igbelina, C.D.; Sheaf, G.S.; Mustafa, R.; Bakrania, S.; Encalada, A.V.; Wood, G.A. Inclusion Matters: Inclusive Interventions for Children with Disabilities—An Evidence and Gap Map from Low-and Middle-Income Countries; UNICEF Office of Research-Innocenti: Florence, Italy, 2022. [Google Scholar]
- Emerson, E.; Robertson, J.; Baines, S.; Hatton, C. Vaccine coverage among children with and without intellectual disabilities in the UK: Cross sectional study. BMC Public Health 2019, 19, 748. [Google Scholar]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar]
- Akers, J.; Aguiar-Ibáñez, R.; Baba-Akbari, A. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care; Centre for Reviews and Dissemination, University of York: York, UK, 2009. [Google Scholar]
- Robertson-Malt, S. JBI’s systematic reviews: Presenting and interpreting findings. AJN Am. J. Nurs. 2014, 114, 49–54. [Google Scholar]
- Kostanjsek, N.F.I. Use of The International Classification of Functioning, Disability and Health (ICF) as a conceptual framework and common language for disability statistics and health information systems. BMC Public Health 2011, 11, S3. [Google Scholar]
- Leonardi, M.; Lee, H.; Kostanjsek, N.; Fornari, A.; Raggi, A.; Martinuzzi, A.; Yáñez, M.; Almborg, A.-H.; Fresk, M.; Besstrashnova, Y. 20 years of ICF—International classification of functioning, disability and health: Uses and applications around the world. Int. J. Environ. Res. Public Health 2022, 19, 11321. [Google Scholar] [CrossRef]
- Team, T.E. EndNote, EndNote X9; Clarivate: Philadelphia, PA, USA, 2013. [Google Scholar]
- Covidence Systematic Review Software, Veritas Health Innovation, Melbourne, Australia. Available online: www.covidence.org (accessed on 3 January 2025).
- Lin, J.-D.; Lin, P.-Y.; Lin, L.-P. Universal hepatitis B vaccination coverage in children and adolescents with intellectual disabilities. Res. Dev. Disabil. 2010, 31, 338–344. [Google Scholar]
- Tuckerman, J.; Mohamed, Y.; Justice, F.; Andersson, T.; Wyatt, K.; Broun, K.; Bastable, A.; Overmars, I.; Kaufman, J.; Danchin, M. Stakeholder perspectives of immunisation delivery for adolescents with disability in specialist schools in Victoria, Australia:‘we need a vaccination pathway’. BMC Public Health 2024, 24, 1973. [Google Scholar]
- Ong, N.; Brogan, D.; Lucien, A.; Wolman, S.; Campbell, D.; Deng, L.; Koirala, A.; Garg, P.; Sharma, K. The development and evaluation of a vaccination pathway for children with intellectual and developmental disability and needle fear. Paediatr. Neonatal Pain 2024, 6, 1–9. [Google Scholar] [PubMed]
- Rosenberg, R.E.; Law, J.K.; Anderson, C.; Samango-Sprouse, C.; Law, P.A. Survey of vaccine beliefs and practices among families affected by autism spectrum disorders. Clin. Pediatr. 2013, 52, 871–874. [Google Scholar]
- Fong, E.; Adil, D.; Mesterman, R. 28 Vaccination experiences for children with special needs-An examination of the impact of behaviours on vaccine uptake. Paediatr. Child Health 2024, 29, e12. [Google Scholar]
- Bray, A. Vaccination Strategies to Keep Children with Special Needs Healthy. 2022. Available online: https://www.clinicaladvisor.com/features/vaccinating-children-with-special-needs/ (accessed on 1 December 2024).
- Okoro, J.; Ojinnaka, N.; Ikefuna, A.; Onyenwe, N. Sociodemographic influences on immunization of children with chronic neurological disorders in Enugu, Nigeria. Trials Vaccinol. 2015, 4, 9–13. [Google Scholar] [CrossRef]
- O’Neill, J.; Newall, F.; Antolovich, G.; Lima, S.; Danchin, M. The uptake of adolescent vaccinations through the school immunisation program in specialist schools in Victoria, Australia. Vaccine 2019, 37, 272–279. [Google Scholar] [CrossRef]
- Mactaggart, I.; Kuper, H.; Murthy, G.V.; Sagar, J.; Oye, J.; Polack, S. Assessing health and rehabilitation needs of people with disabilities in Cameroon and India. Disabil. Rehabil. 2016, 38, 1757–1764. [Google Scholar] [CrossRef]
- United Nations Children’s Fund and Leonard Cheshire Disability and Inclusive Development Centre. Disability Prevention Efforts and Disability Rights: Finding Common Ground on Immunization Efforts; UNICEF: New York, NY, USA, 2020; Available online: https://www.unicef.org/sites/default/files/2022-10/GIP02115_UNICEF_Children-with-Disabilities-Factsheet-final%20-%20accessible.pdf (accessed on 3 January 2025).
- United Nations Children’s Fund. UNICEF Humanitarian Action for Children 2024 Overview. Available online: https://www.unicef.org/media/149906/file/Humanitarian-Action-for-Children-2024-Overview.pdf (accessed on 15 January 2025).
- United Nations Children’s Fund. Children with Disabilities: UNICEF Data 2013. Available online: https://data.unicef.org/wp-content/uploads/2015/12/SOWC_2013_75.pdf (accessed on 15 January 2025).
- United Nations Children’s Fund. The State of World’s Children 2023. Available online: https://www.unicef.org/eca/reports/sowc2023-eca (accessed on 15 January 2025).
- Wang, E.; Clymer, J.; Davis-Hayes, C.; Buttenheim, A. Nonmedical exemptions from school immunization requirements: A systematic review. Am. J. Public Health 2014, 104, e62–e84. [Google Scholar]
- Elias, E.R.; Murphy, N.A.; Liptak, G.S.; Adams, R.C.; Burke, R.; Friedman, S.L.; Houtrow, A.; Kalichman, M.; Kuo, D. Home care of children and youth with complex health care needs and technology dependencies. Pediatrics 2012, 129, 996–1005. [Google Scholar]
- Ashfield, S.; Donelle, L. Parental online information access and childhood vaccination decisions in North America: Scoping review. J. Med. Internet Res. 2020, 22, e20002. [Google Scholar]
- Healy, C.M.; Pickering, L.K. How to communicate with vaccine-hesitant parents. Pediatrics 2011, 127, S127–S133. [Google Scholar] [PubMed]
- Leask, J.; Chapman, S.; Hawe, P.; Burgess, M. What maintains parental support for vaccination when challenged by anti-vaccination messages? A qualitative study. Vaccine 2006, 24, 7238–7245. [Google Scholar]
- Helps, C.; Leask, J.; Barclay, L.; Carter, S. Understanding non-vaccinating parents’ views to inform and improve clinical encounters: A qualitative study in an Australian community. BMJ Open 2019, 9, e026299. [Google Scholar]
- Ward, K.; Quinn, H.E.; Bachelor, M.A.; Bryant, V.; Campbell-Lloyd, S.; Newbound, A.; Scully, M.; Webby, R.J.; McIntyre, P.B. Adolescent school-based vaccination in Australia. Commun. Dis. Intell. Q. Rep. 2013, 37, E156–E167. [Google Scholar]
- Krause, T.G.; Jakobsen, S.S.; Haarh, M.; Mølbak, K. The Danish vaccination register. Euro Surveill. Bull. Eur. Sur Les Mal. Transm. Eur. Commun. Dis. Bull. 2012, 17, 20155. [Google Scholar]
- Murthy, N.C.; Rodgers, L.E.; Pabst, L.J.; Fiebelkorn, A.P.; Ng, T. Progress in Childhood Vaccination Data in Immunization Information Systems—United States, 2013–2016. Morb. Mortal. Wkly. Rep. 2017, 66, 1178–1181. [Google Scholar]
- Carter, A.; Klinner, C.; Young, A.; Strnadová, I.; Wong, H.; Vujovich-Dunn, C.; Newman, C.E.; Davies, C.; Skinner, S.R.; Danchin, M. “I Thought It Was Better to Be Safe than Sorry”: Factors Influencing Parental Decisions on HPV and Other Adolescent Vaccinations for Students with Intellectual Disability and/or Autism in New South Wales, Australia. Vaccines 2024, 12, 922. [Google Scholar] [CrossRef]
- Bruce, J.; Chantler, T.; Kumakech, E.; Mawanda, A.; Olorunsaiye, C.Z.; Schmucker, L.; Kiapi, L.; Landegger, J.; Webster, J. Evaluation of a data-informed community engagement strategy to increase immunisation coverage in northern Uganda: A cluster-randomised controlled trial with an embedded process evaluation. Lancet Glob. Health 2018, 6, S15. [Google Scholar]
- van der Mark, E.J.; Zuiderent-Jerak, T.; Dedding, C.W.M.; Conradie, I.M.; Broerse, J.E.W. Connecting relational wellbeing and participatory action research: Reflections on ‘unlikely’ transformations among women caring for disabled children in South Africa. J. Glob. Ethics 2023, 19, 80–104. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).