

Immunogenicity of SARS-CoV-2 Vaccination Schedules Including a Booster Dose in Patients with Systemic Lupus Erythematosus: Data from a Prospective Multicenter Study
 , , , , , , , , , , , , , , , , , , , , , , , , , and
on behalf of the SAFER-Study Group Task Forceadd
Show full author list
, , , , , , , , , , , , , , , , , , , , , , , , , and
on behalf of the SAFER-Study Group Task Forceadd
Show full author list
Abstract
1. Introduction
2. Materials and Methods
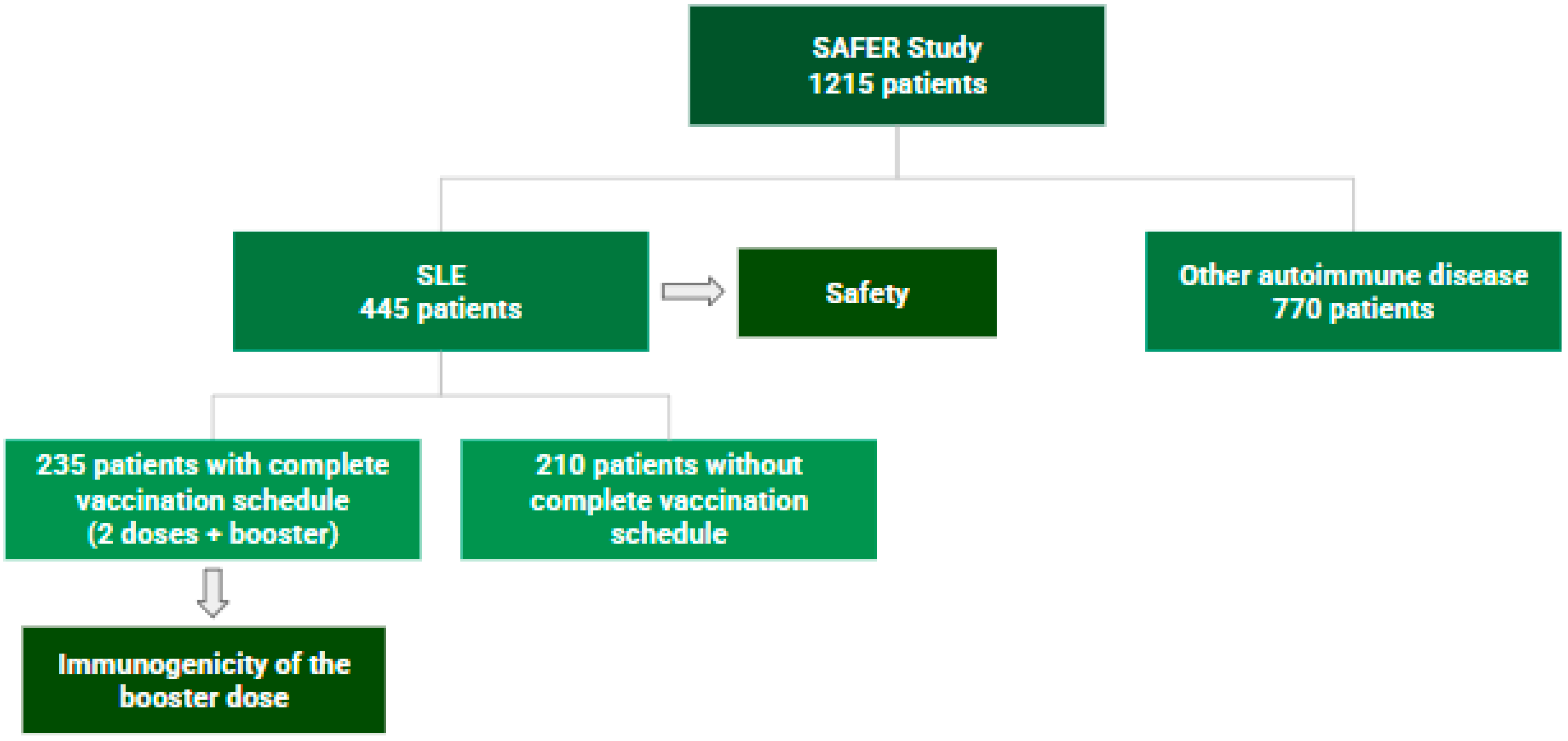
2.1. Study Design and Population
2.2. Variables of Interest
2.3. Statistical Analysis
2.4. Ethical Aspects
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Danza, A.; Ruiz-Irastorza, G. Infection risk in systemic lupus erythematosus patients: Susceptibility factors and preventive strategies. Lupus 2013, 22, 1286–1294. [Google Scholar] [CrossRef]
- Rao, M.; Mikdashi, J. A Framework to Overcome Challenges in the Management of Infections in Patients with Systemic Lupus Erythematosus. Open Access Rheumatol. 2023, 15, 125–137. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Urowitz, M.B.; Bookman, A.A.; Koehler, B.E.; Gordon, D.A.; Smythe, H.A.; Ogryzlo, M.A. The bimodal mortality pattern of systemic lupus erythematosus. Am. J. Med. 1976, 60, 221–225. [Google Scholar] [CrossRef] [PubMed]
- E Moss, K.; Ioannou, Y.; Sultan, S.M.; Haq, I.; A Isenberg, D. Outcome of a cohort of 300 patients with systemic lupus erythematosus attending a dedicated clinic for over two decades. Ann. Rheum. Dis. 2002, 61, 409–413. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Herrinton, L.J.; Liu, L.; Goldfien, R.; Michaels, M.A.; Tran, T.N. Risk of Serious Infection for Patients with Systemic Lupus Erythematosus Starting Glucocorticoids with or without Antimalarials. J. Rheumatol. 2016, 43, 1503–1509. [Google Scholar] [CrossRef] [PubMed]
- Fu, X.-L.; Qian, Y.; Jin, X.-H.; Yu, H.-R.; Du, L.; Wu, H.; Chen, H.-L.; Shi, Y.-Q. COVID-19 in patients with systemic lupus erythematosus: A systematic review. Lupus 2022, 31, 684–696. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gianfrancesco, M.; Hyrich, K.L.; Al-Adely, S.; Carmona, L.; Danila, M.I.; Gossec, L.; Izadi, Z.; Jacobsohn, L.; Katz, P.; Lawson-Tovey, S.; et al. Characteristics associated with hospitalisation for COVID-19 in people with rheumatic disease: Data from the COVID-19 global rheumatology alliance physician- reported registry. Ann. Rheum. Dis 2020, 79, 859–866. [Google Scholar] [CrossRef] [PubMed]
- Marques, C.D.L.; Kakehasi, A.M.; Pinheiro, M.M.; Mota, L.M.H.; Albuquerque, C.P.; Silva, C.R.; Santos, G.P.J.; Reis-Neto, E.T.; Matos, P.; Devide, G.; et al. High levels of immunosuppression are related to unfavourable outcomes in hospitalised patients with rheumatic diseases and COVID-19: First results of ReumaCoV Brasil registry. RMD Open 2021, 7, e001461, Erratum in RMD Open 2021, 7, e001461corr1. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fernandez-Ruiz, R.; Masson, M.; Kim, M.Y.; Myers, B.; Haberman, R.H.; Castillo, R.; Scher, J.U.; Guttmann, A.; Carlucci, P.M.; Deonaraine, K.K.; et al. Leveraging the United States Epicenter to Provide Insights on COVID-19 in Patients with Systemic Lupus Erythematosus. Arthritis Rheumatol. 2020, 72, 1971–1980. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Luz, K.R.; da Souza, D.C.C.; de Ciconelli, R.M. Vacinação em pacientes imunossuprimidos e com doenças reumatológicas auto-imunes. Rev. Bras. Reumatol. 2007, 47, 106–113. [Google Scholar] [CrossRef]
- Avery, R.K. Vaccination of the immunosuppressed adult patient with rheumatologic disease. Rheum. Dis. Clin. N. Am. 1999, 25, 567–584, viii. [Google Scholar] [CrossRef] [PubMed]
- van Assen, S.; Agmon-Levin, N.; Elkayam, O.; Cervera, R.; Doran, M.F.; Dougados, M.; Emery, P.; Geborek, P.; Ioannidis, J.P.; Jayne, D.R.; et al. Update of EULAR recommendations for vaccination in adult patients with autoimmune inflammatory rheumatic diseases. Ann. Rheum. Dis. 2020, 79, 39–52. [Google Scholar]
- Garg, M.; Mufti, N.; Palmore, T.N.; Hasni, S.A. Recommendations and barriers to vaccination in systemic lupus erythematosus. Autoimmun. Rev. 2018, 17, 990–1001. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liao, Z.; Tang, H.; Xu, X.; Liang, Y.; Xiong, Y.; Ni, J. Immunogenicity and Safety of Influenza Vaccination in Systemic Lupus Erythematosus Patients Compared with Healthy Controls: A Meta-Analysis. PLoS ONE 2016, 11, e0147856. [Google Scholar] [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. European League Against Rheumatism/American College of Rheumatology Classification Criteria for Systemic Lupus Erythematosus. Arthritis Rheumatol. 2019, 71, 1400–1412. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pileggi, G.S.; Da Mota, L.M.H.; Kakehasi, A.M.; De Souza, A.W.; Rocha, A.; de Melo, A.K.G.; da Fonte, C.A.M.; Bortoletto, C.; Brenol, C.V.; Marques, C.D.L.; et al. Brazilian recommendations on the safety and effectiveness of the yellow fever vaccination in patients with chronic immune-mediated inflammatory diseases. AdvRheumatol 2019, 59, 17. [Google Scholar] [CrossRef]
- Jochum, S.; Kirste, I.; Hortsch, S.; Grunert, V.P.; Legault, H.; Eichenlaub, U.; Basel, K.; Pajon, R. Clinical utility of Elecsys Anti-SARS-CoV-2 S assay in COVID-19 vaccination: An exploratory analysis of the mRNA-1273 phase 1 trial. medRxiv 2021, 12, 798117, Update in Front. Immunol. 2022, 12, 798117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Westra, J.; Rondaan, C.; van Assen, S.; Bijl, M. Vaccination of patients with autoimmune inflammatory rheumatic diseases. Nat. Rev. Rheumatol. 2015, 11, 135–145. [Google Scholar] [CrossRef] [PubMed]
- Cordtz, R.; Kristensen, S.; Dalgaard, L.P.H.; Westermann, R.; Duch, K.; Lindhardsen, J.; Torp-Pedersen, C.; Dreyer, L. Incidence of COVID-19 Hospitalisation in Patients with Systemic Lupus Erythematosus: A Nationwide Cohort Study from Denmark. J. Clin. Med. 2021, 10, 3842. [Google Scholar] [CrossRef] [PubMed]
- Jiang, X.; Sparks, J.; Wallace, Z.; Deng, X.; Li, H.; Lu, N.; Xie, D.; Wang, Y.; Zeng, C.; Lei, G.; et al. Risk of COVID-19 among unvaccinated and vaccinated patients with systemic lupus erythematosus: A general population study. RMD Open 2023, 9, e002839. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Alquraan, L.; Alzoubi, K.H.; Rababa’h, S.Y. Mutations of SARS-CoV-2 and their impact on disease diagnosis and severity. Inform. Med. Unlocked 2023, 39, 101256. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- BRASIL. Ministério da Saúde. Secretaria de Vigilância em Saúde. COVID-19: Boletim Epidemiológico 71; Semana Epidemiológica 27 (4/7 a 10/7); BRASIL: Brasília, Brasil, 2021. [Google Scholar]
- Bijlsma, J.W. EULAR December 2020 view points on SARS-CoV-2 vaccination in patients with RMDs. Ann. Rheum. Dis. 2021, 80, 411–412. [Google Scholar] [CrossRef] [PubMed]
- Tan, S.Y.S.; Yee, A.M.; Sim, J.J.L.; Lim, C.C. COVID-19 vaccination in systemic lupus erythematosus: A systematic review of its effectiveness, immunogenicity, flares and acceptance. Rheumatology 2023, 62, 1757–1772. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Medeiros-Ribeiro, A.C.; Aikawa, N.E.; Saad, C.G.S.; Yuki, E.F.N.; Pedrosa, T.; Fusco, S.R.G.; Rojo, P.T.; Pereira, R.M.R.; Shinjo, S.K.; Andrade, D.C.O.; et al. Immunogenicity and safety of the CoronaVac inactivated vaccine in patients with autoimmune rheumatic diseases: A phase 4 trial. Nat. Med. 2021, 27, 1744–1751. [Google Scholar] [CrossRef]
- Yuki, E.F.N.; Borba, E.F.; Pasoto, S.G.; Seguro, L.P.; Lopes, M.; Saad, C.G.S.; Medeiros-Ribeiro, A.C.; Silva, C.A.; de Andrade, D.C.O.; Kupa, L.d.V.K.; et al. Impact of Distinct Therapies on Antibody Response to SARS-CoV-2 Vaccine in Systemic Lupus Erythematosus. Arthritis Care Res. 2022, 74, 562–571. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Izmirly, P.M.; Kim, M.Y.; Samanovic, M.; Fernandez-Ruiz, R.; Ohana, S.; Deonaraine, K.K.; Engel, A.J.; Masson, M.; Xie, X.; Cornelius, A.R.; et al. Evaluation of Immune Response and Disease Status in Systemic Lupus Erythematosus Patients Following SARS-CoV-2 Vaccination. Arthritis Rheumatol. 2022, 74, 284–294. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Assawasaksakul, T.; Sathitratanacheewin, S.; Vichaiwattana, P.; Wanlapakorn, N.; Poovorawan, Y.; Avihingsanon, Y.; Assawasaksakul, N.; Kittanamongkolchai, W. Immunogenicity of the third and fourth BNT162b2 mRNA COVID-19 boosters and factors associated with immune response in patients with SLE and rheumatoid arthritis. Lupus Sci. Med. 2022, 9, e000726. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Furer, V.; Eviatar, T.; Zisman, D.; Peleg, H.; Paran, D.; Levartovsky, D.; Zisapel, M.; Elalouf, O.; Kaufman, I.; Meidan, R.; et al. Immunogenicity and safety of the BNT162b2 mRNA COVID-19 vaccine in adult patients with autoimmune inflammatory rheumatic diseases and in the general population: A multicentre study. Ann. Rheum. Dis. 2021, 80, 1330–1338. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Total N = 235 | CoronaVac + BNT162b2 N = 116 | ChadOx-1+ BNT162b2 N = 87 | BNT162b2 + BNT162b2 N = 32 | p | |
|---|---|---|---|---|---|
| Sex | 0.540 | ||||
| Female | 210 (89.36) | 101 (87.07) | 79 (90.80) | 30 (93.75) | |
| Age, mean (SD) | 38.0 (29.0–46.0) | 35.5 (28.0–45.0) | 40.0 (31.0–47.0) | 37.5 (32.0–46.0) | 0.095 |
| Skin color | 0.300 | ||||
| White | 87 (37.02) | 51 (43.97) | 27 (31.03) | 9 (28.13) | |
| Black | 33 (14.04) | 15 (12.93) | 14 (16.09) | 4 (12.50) | |
| Brown | 109 (46.38) | 46 (39.66) | 45 (51.72) | 18 (56.25) | |
| Disease in years, median (IQR) | 10 (5–16) | 8 (4–15) | 12 (7–18) | 7.7 (4–14) | 0.006 |
| Smoking | 15 (6.38) | 11 (9.48) | 4 (4.60) | 0 (0.00) | 0.130 |
| No comorbidities | 92 (39.15) | 59 (50.86) | 23 (26.44) | 10 (31.25) | 0.001 |
| Heart disease | 10 (4.26) | 5 (4.31) | 2 (2.30) | 3 (9.38) | 0.220 |
| Diabetes | 11 (4.68) | 6 (5.17) | 4 (4.60) | 1 (3.13) | 1.000 |
| Lung disease | 7 (2.98) | 1 (0.86) | 2 (2.30) | 4 (12.50) | 0.007 |
| Kidney disease | 4 (1.70) | 2 (1.72) | 2 (2.30) | 0 (0.00) | 1.000 |
| Hypertension | 64 (27.23) | 26 (22.41) | 29 (33.33) | 9 (28.13) | 0.220 |
| Obesity | 27 (11.49) | 12 (10.34) | 10 (11.49) | 5 (15.63) | 0.710 |
| Other comorbidities * | 95 (40.43) | 37 (31.90) | 44 (50.57) | 14 (43.75) | 0.025 |
| APS | 19 (8.09) | 11 (9.48) | 6 (6.90) | 2 (6.25) | 0.800 |
| Previous thrombosis | 32 (13.62) | 14 (12.07) | 11 (12.64) | 7 (21.88) | 0.340 |
| Disease activity | 0.056 | ||||
| Remission | 90/225 (40) | 45/109 (41.28) | 30/84 (35.71) | 15/32 (46.88) | |
| Low activity | 73/225 (32.44) | 28/109 (25.69) | 37/84 (44.05) | 8/32 (25.00) | |
| Moderate-to-high activity | 62/225 (27.56) | 36/109 (33.03) | 17/84 (20.24) | 9/32 (28.13) | |
| Degree of Immunosuppression | 0.160 | ||||
| No immunosuppression | 70/232 (30.17) | 40/115 (34.78) | 25/86 (29.07) | 5/31 (16.13) | |
| Low grade | 27/232 (11.64) | 9/115 (7.83) | 12/86 (13.95) | 6/31 (19.35) | |
| High grade | 135/232 (58.19) | 66/115 (57.39) | 49/86 (56.98) | 20/31 (64.52) |
| Total N = 235 | CoronaVac + BNT162b2 N = 116 | ChadOx-1 + BNT162b2 N = 87 | BNT162b2 + BNT162b2 N = 32 | p | |
|---|---|---|---|---|---|
| Azathioprine | 54/235 (22.98) | 27/116 (23.28) | 17/87 (19.54) | 10/32 (31.25) | 0.400 |
| Oral corticosteroid | 112/235 (47.66) | 60/116 (51.72) | 38/87 (43.68) | 14/32 (43.75) | 0.470 |
| Oral corticosteroid dose | 0.007 | ||||
| Up to 5 mg/day | 54/112 (48.21) | 24/60 (40.00) | 25/38 (65.79) | 5/14 (35.71) | |
| ≥6 a 10 mg/day | 27/112 (24.11) | 14/60 (23.33) | 7/38 (18.42) | 6/14 (42.86) | |
| ≥11 a 20 mg/day | 19/112 (16.96) | 10/60 (16.67) | 6/38 (15.79) | 3/14 (21.43) | |
| >20 mg/day | 12/112 (10.71) | 12/60 (20.00) | 0/38 (0.00) | 0/14 (0.00) | |
| Hydroxychloroquine | 194/235 (82.55) | 98/116 (84.48) | 68/87 (78.16) | 28/32 (87.50) | 0.370 |
| Mycophenolate | 54/235 (22.98) | 22/116 (18.97) | 25/87 (28.74) | 7/32 (21.88) | 0.260 |
| Methotrexate | 32/235 (13.62) | 12/116 (10.34) | 14/87 (16.09) | 6/32 (18.75) | 0.330 |
| Methotrexate dose | 0.880 | ||||
| ≤20 mg/week | 23/32 (71.88) | 8/12 (66.67) | 10/14 (71.43) | 5/6 (83.33) | |
| >20 mg/week | 9/32 (28.13) | 4/12 (33.33) | 4/14 (28.57) | 1/6 (16.67) | |
| Rituximab (regular use) | 7/235 (2.98) | 2/116 (1.72) | 5/87 (5.75) | 0/32 (0.00) | 0.170 |
| COVID-19 Infection Cases | Total N = 235 | CoronaVac + BNT162b2 N = 116 | ChadOx-1 + BNT162b2 N = 87 | BNT162b2 + BNT162b2 N = 32 | p |
|---|---|---|---|---|---|
| Positive cases of SARS-CoV-2 more than 15 days after the 1st dose | 4/235 (1.70) | 3/116 (2.59) | 1/87 (1.15) | 0/32 (0.00) | 0.800 |
| Positive cases of SARS-CoV-2 more than 15 days after the 2nd dose | 6/235 (2.55) | 5/116 (4.31) | 1/87 (1.15) | 0/32 (0.00) | 0.360 |
| Positive cases of SARS-CoV-2 more than 15 days after the 3rd dose | 22/235 (9.36) | 12/116 (10.34) | 8/87 (9.20) | 2/32 (6.25) | 0.860 |
| Total N = 235 | CoronaVac + BNT162b2 N = 116 | ChadOx-1 + BNT162b2 N = 87 | BNT162b2 + BNT162b2 N = 32 | p | |
|---|---|---|---|---|---|
| Serology | |||||
| Inclusion | 90/228 (39.47) | 47/114 (41.23) | 30/84 (35.71) | 13/30 (43.33) | 0.660 |
| 28 days after the 1st dose | 162/219 (73.97) | 79/114 (69.30) | 62/78 (79.49) | 21/27 (77.78) | 0.260 |
| 28 days after 2nd dose | 200/219 (91.32) | 98/110 (89.09) | 74/79 (93.67) | 28/30 (93.33) | 0.500 |
| After 3rd dose | 201/206 (97.57) | 99/103 (96.12) | 73/74 (98.65) | 29/29 (100.00) | 0.370 |
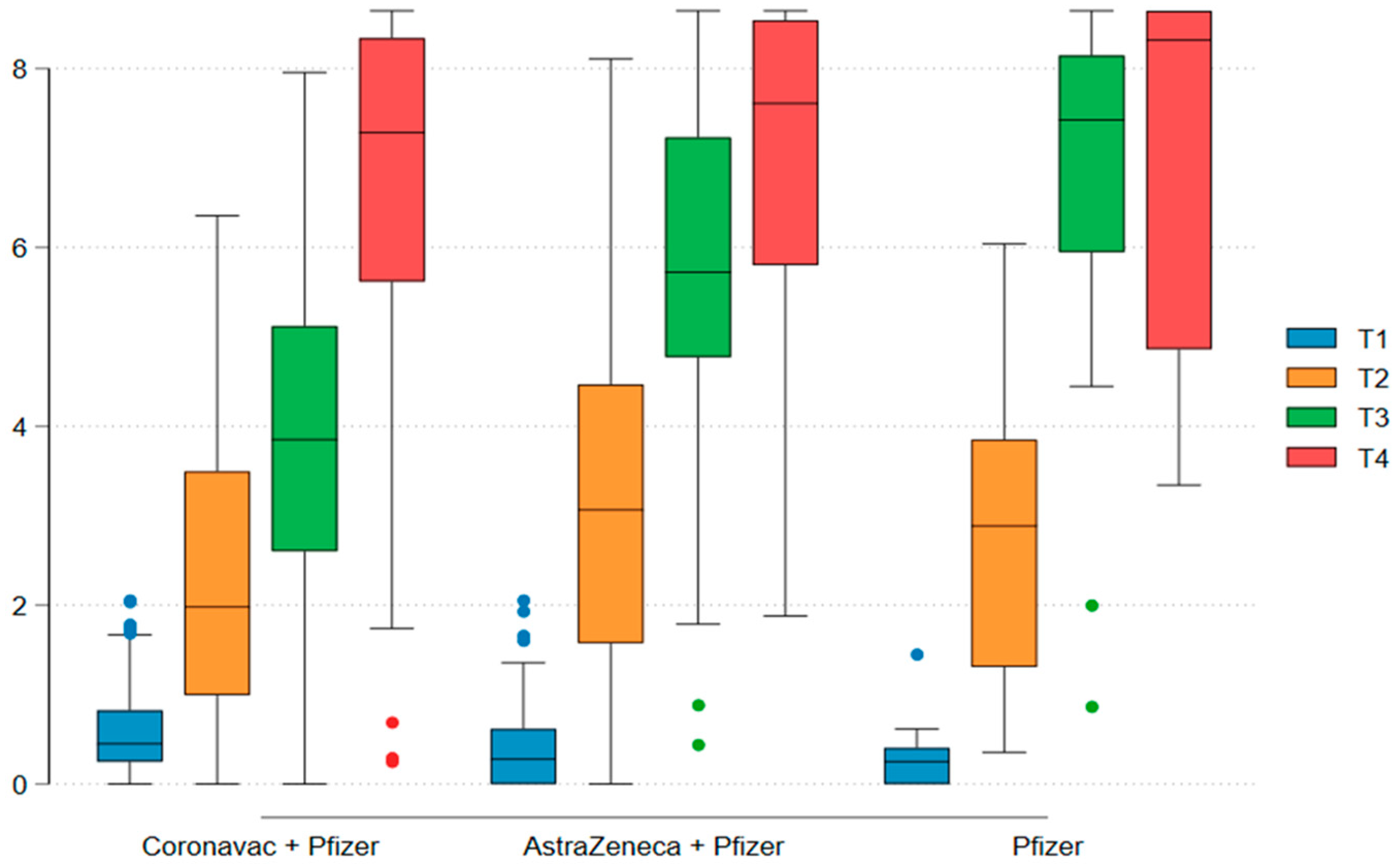
| IgG titer (Log10) | |||||
| Inclusion, mean (SD) | 1.86 (1.89) | 2.00 (1.88) | 1.70 (1.90) | 1.81 (1.94) | 0.540 |
| After 1st dose, mean (SD) | 4.10 (2.49) | 3.45 (2.04) | 4.72 (2.71) | 5.11 (2.82) | <0.001 |
| After 2nd dose, mean (SD) | 5.44 (2.17) | 4.37 (1.80) | 6.30 (1.98) | 7.09 (1.86) | <0.001 |
| After 3rd dose, mean (SD) | 7.06 (1.80) | 6.95 (1.95) | 7.17 (1.65) | 7.17 (1.59) | 0.680 |
| Multivariate Linear Regression | ||||
|---|---|---|---|---|
| Coefficient | CI [95%] | p | ||
| Disease activity | ||||
| Remission | - | - | - | - |
| Low activity | −0.503 | −1.624 | 0.617 | 0.373 |
| Moderate-to-high activity | −1.060 | −2.134 | 0.013 | 0.053 |
| Immunosuppression | ||||
| Without immunosuppression | - | - | - | - |
| Low degree of immunosuppression | −1.596 | −3.744 | 0.551 | 0.143 |
| High degree of immunosuppression | −0.692 | −1.650 | 0.266 | 0.154 |
| Serology after 1st | ||||
| Total N = 222 | Seronegative N = 61 | Seropositive N = 161 | p | |
| Mycophenolate | 48 (21.62) | 16 (16.23) | 32 (19.88) | 0.300 |
| Methotrexate | 31 (13.96) | 10 (16.39) | 21 (13.04) | 0.520 |
| Azathioprine | 51 (22..97) | 17 (27.87) | 34 (21.12) | 0.290 |
| Serology after 2nd | ||||
| Total N = 222 | Seronegative N = 21 | Seropositive N = 201 | p | |
| Mycophenolate | 51 (22.97) | 10 (47.62) | 41 (20.40) | 0.005 |
| Methotrexate | 28 (12.61) | 3 (14.29) | 25 (12.44) | 0.730 |
| Azathioprine | 49 (22.07) | 4 (19.05) | 45 (22.39) | 1.000 |
| Serology after 3rd | ||||
| Total N = 212 | Seronegative N = 5 | Seropositive N = 207 | p | |
| Mycophenolate | 49 (23.11) | 4 (80.00) | 45 (21.74) | 0.011 |
| Methotrexate | 29 (13.68) | 0 (0.00) | 29 (14.01) | 1.000 |
| Azathioprine | 46 (21.70) | 1 (20.00) | 45 (21.74) | 1.000 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sartori, N.S.; Machado, K.L.L.L.; Miyamoto, S.T.; Pretti, F.Z.; Gouveia, M.d.P.G.; de Oliveira, Y.G.P.; da Silva, V.G.; Faé, F.; Burian, A.P.N.; Tapia, K.R.L.; et al. Immunogenicity of SARS-CoV-2 Vaccination Schedules Including a Booster Dose in Patients with Systemic Lupus Erythematosus: Data from a Prospective Multicenter Study. Vaccines 2025, 13, 127. https://doi.org/10.3390/vaccines13020127
Sartori NS, Machado KLLL, Miyamoto ST, Pretti FZ, Gouveia MdPG, de Oliveira YGP, da Silva VG, Faé F, Burian APN, Tapia KRL, et al. Immunogenicity of SARS-CoV-2 Vaccination Schedules Including a Booster Dose in Patients with Systemic Lupus Erythematosus: Data from a Prospective Multicenter Study. Vaccines. 2025; 13(2):127. https://doi.org/10.3390/vaccines13020127
Chicago/Turabian StyleSartori, Natália Sarzi, Ketty Lysie Libardi Lira Machado, Samira Tatiyama Miyamoto, Flávia Zon Pretti, Maria da Penha Gomes Gouveia, Yasmin Gurtler Pinheiro de Oliveira, Vanezia Gonçalves da Silva, Filipe Faé, Ana Paula Neves Burian, Karina Rosemarie Lallemand Tapia, and et al. 2025. "Immunogenicity of SARS-CoV-2 Vaccination Schedules Including a Booster Dose in Patients with Systemic Lupus Erythematosus: Data from a Prospective Multicenter Study" Vaccines 13, no. 2: 127. https://doi.org/10.3390/vaccines13020127
APA StyleSartori, N. S., Machado, K. L. L. L., Miyamoto, S. T., Pretti, F. Z., Gouveia, M. d. P. G., de Oliveira, Y. G. P., da Silva, V. G., Faé, F., Burian, A. P. N., Tapia, K. R. L., Moulin, A. C. S., Grillo, L. L., Athayde, P. d. S., Corona, H. d. S., Ramos, S. d. S., Peixoto, F. M. M. M. C., Ribeiro, P. D. C., Magalhães, V. d. O., de Aguiar, M. F., ... Monticielo, O. A., on behalf of the SAFER-Study Group Task Force. (2025). Immunogenicity of SARS-CoV-2 Vaccination Schedules Including a Booster Dose in Patients with Systemic Lupus Erythematosus: Data from a Prospective Multicenter Study. Vaccines, 13(2), 127. https://doi.org/10.3390/vaccines13020127