Abstract
Background/Objectives: With declining vaccine coverage and rising concerns regarding vaccines, vaccine-preventable diseases are rising. Many research studies have examined approaches to enhance the acceptance of vaccines, but the integration of these approaches into practice has been limited. Thus, the objective was to identify recent evidence surrounding provider–patient communication tools and approaches related to vaccination confidence. Methods: A systematic review following PRISMA methodology was conducted. Using a pre-specified search strategy aligned with the research objective and performed in PubMed, CINAHL, and Web of Science, articles were evaluated by two researchers independently, with a third resolving discrepancies, at the title and abstract screening, full-text review, quality assessment, and data extraction phases. Extraction data were descriptively analyzed, including the impact on vaccine acceptance, and synthesized thematically. Results: From the 2291 studies which underwent screening, a total of, 143 articles were included. Most studies were conducted in the United States, in the outpatient setting, and utilized physicians and nurses to deliver the intervention. Many vaccines were covered, with the greatest number of studies focusing on influenza, HPV, and pneumococcal vaccines. The three predominant communication approaches and tools utilized were provider-focused training, direct patient education/materials, and provider–patient communication strategies. These strategies often focused on addressing knowledge gaps, health beliefs, and common concerns. Over two-thirds of studies increased vaccine acceptance following communication interventions. Conclusions: To address vaccine concerns, it is important to ensure providers have the education and training necessary as well as tools to address underlying causes of concerns. When equipped, providers are able to improve vaccine acceptance.
1. Introduction
Coverage of vaccines has faced challenges in recent years. Vaccine coverage, already below target levels, has continued to decline, especially among pediatric populations [1,2,3]. Many vaccinations have reduced infectious disease-related morbidity and mortality [4]; this requires substantial coverage of the population to prevent the spread of disease and protect those unable to be vaccinated [5]. Despite is, public confidence in vaccines has waned due to varying factors, including the recent COVID-19 pandemic and beliefs related to COVID vaccines [6,7,8,9]. Thus, many patients and caregivers of children may forgo or delay the receipt of a vaccine(s). Concerns about vaccines often stem from perceived safety and efficacy issues, weak social support, diminished perceptions of benefit, and misinformation [6,10,11,12,13,14,15,16]. Although vaccine confidence has declined, healthcare providers continue to increase vaccine acceptance [17] and are among the most trusted sources of vaccine information [18]. Leveraging this trust through effective communication is critical to addressing public confidence in vaccines.
Because declining vaccine confidence can contribute to increased global burden of disease, healthcare professionals must facilitate open dialogue to elicit underlying health beliefs, address misinformation, and provide evidence-based information regarding vaccine safety and efficacy. Prior work has demonstrated the effectiveness of interventions to enhancing provider–patient communication during vaccine confidence conversations, resulting in increased vaccine uptake [19,20,21,22,23]. For example, pediatric providers who utilized motivational interviewing, a patient-centered, collaborative approach to exploring perspectives and identifying reasons and desire for change, as well as communication tool were able to see a decline in documented vaccine refusals and an increase in seasonal influenza vaccine rates [19]. Expanding this approach into community pharmacies with patients who expressed initial hesitancy resulted in 35.4% of these patients receiving a vaccine [24]. Providers also have seen the benefits of these approaches in maternity patients [23,25].
Improving the implementation of evidence-based practices, such as vaccination confidence provider–patient communication tools and approaches, must include behavioral change by providers. Rather than being directive about the need to vaccinate and accepting the patient’s initial response to vaccinations, providers should facilitate open conversations, elicit patient perspectives, and collaborate with the patient to achieve health goals. However, despite growing evidence of effective communication-based interventions [26,27,28], there is limited integration into everyday practice. Providers often lack structured tools, adequate training, or organizational support to implement these approaches consistently. Thus, the objective of this systematic review was to identify recent evidence surrounding provider–patient communication tools and approaches related to vaccination confidence in order to provide the first steps for translating these findings into practice.
2. Materials and Methods
The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guideline was followed for this systematic review [29]. Prior to beginning the systematic review, the study protocol was registered in PROSPERO (CRD42024546568). Due to the heterogeneity of the study designs and outcomes that would be included, the planned analytical approach from the beginning was a qualitative synthesis rather than a meta-analysis.
Inclusion and exclusion criteria were identified. To be included, articles must be peer-reviewed, be primary literature research articles, be available in full-text, written in English, and include provider–patient communication tools/approaches related to vaccination confidence (description of the use of communication tools by a healthcare professional to talk about vaccines with patients or description of the use of communication approaches by a healthcare professional to talk about vaccines with patients). Articles that did not meet those criteria were excluded. Any review articles were excluded, and systematic reviews/meta-analyses were reviewed for any articles missed in the search and then excluded.
A comprehensive search strategy was created in collaboration with a research librarian. The core search strategy included the following terms, which were iterated appropriately depending on the database searched: (healthcare provider OR health personnel OR healthcare workers OR healthcare professional) AND (patient) AND (vaccine) AND (communication OR health communication OR patient education OR health education). PubMed, CINAHL, and Web of Science were utilized to perform the search from 1 January 2000, to date of search (14 May 2024). The search was piloted and refined until tests of the results indicated a comprehensive search. Results from the search were downloaded into Zotero (version 7), a reference management system, for cleaning before uploading into Covidence, a systematic review management system.
Prior to beginning the review process, the research team was trained on the protocol and the Covidence system. At each phase, two researchers performed the step independently, with a third researcher resolving any conflicts. In the first phase, titles and abstracts were reviewed for inclusion, and articles that received a “yes” or “maybe” moved on to full-text review. In the second phase, full-text copies of the articles were obtained and uploaded to Covidence. Full-text articles were reviewed against the inclusion and exclusion criteria. Articles that met these criteria advanced to data extraction. A pre-built template was created in Covidence to pull key article information. The following study characteristics were extracted: article characteristics (setting, study design, study aim, study length, type of provider(s), patient characteristics (pediatric, adolescent, adult, older adult), vaccine(s), type of intervention (communication approach, tool), description of intervention, and key findings. Then, the quality of the study was assessed using the Mixed-Methods Appraisal Tool (MMAT) [30], which allowed for the flexibility of quality assessment given the variety of study designs. Scores could range from 0 to 7, with higher scores indicating greater quality.
Findings from the data extraction were downloaded from Covidence and synthesized into tables. Key findings were thematically drawn from the data extraction tables. Where possible, the findings were categorized and summarized. Outcomes of the communication approach and tool interventions were categorized as: positive (improvement in vaccine acceptance), negative (decline in vaccine acceptance), neutral (limited or no change in vaccine acceptance), or mixed findings (could include positive, negative, and/or neutral in combination).
3. Results
In Figure 1, the PRISMA diagram shows the article identification process, screening, and inclusion.
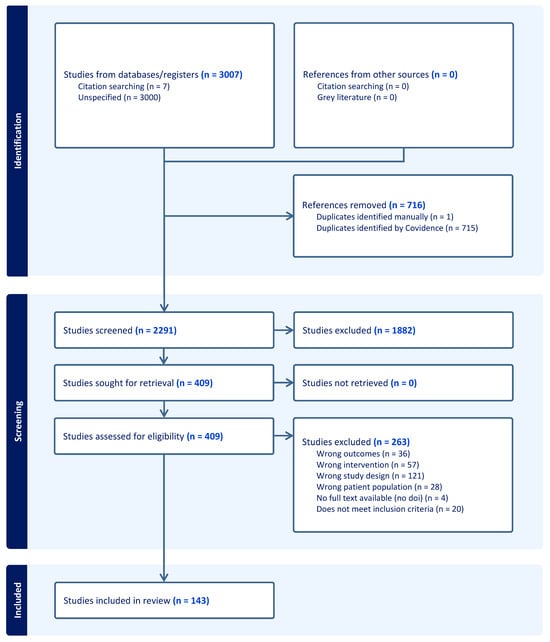
Figure 1.
PRISMA Diagram of Article Identification, Screening, and Inclusion.
From the 2291 studies which underwent screening, a total of 143 articles met inclusion criteria and underwent data extraction [19,22,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115,116,117,118,119,120,121,122,123,124,125,126,127,128,129,130,131,132,133,134,135,136,137,138,139,140,141,142,143,144,145,146,147,148,149,150,151,152,153,154,155,156,157,158,159,160,161,162,163,164,165,166,167,168,169,170,171]. Table 1 provides an overview of the studies included, overall and by age group. Most studies were conducted in the United States, in the outpatient setting, and were non-randomized controlled trial (RCT) designs or RCTs. Physicians and nurses most frequently delivered the interventions, which typically included both communication tools and approaches. Nine studies utilized community pharmacies and pharmacists for the intervention. Many vaccines were covered, with the greatest number of studies focusing on influenza, HPV, and pneumococcal vaccines.

Table 1.
Overview of Included Study Characteristics.
Communication approaches and tools utilized are summarized in Table 2. The three predominant approaches were provider-focused training and tools, patient education materials and communication, and provider–patient communication strategies. Many interventions trained providers in a variety of formats to provide information on vaccines as well as best practices in communicating and sharing decision-making about vaccines. These strategies often focused on addressing knowledge gaps, health beliefs, and common concerns. A small portion of the studies trained providers in behavior-related strategies, such as motivational interviewing (MI). Patient-focused education strategies were focused on sharing information with patients about vaccines to dispel myths, reframe perceptions, and summarize key information. Many of the materials were delivered in a written format, but some studies did include media-based interventions and information-based provider interventions. Provider–patient communication strategies included approaches to conducting vaccine conversations, such as “Ask, Acknowledge, Advise” or the presumptive versus participatory approaches of introducing vaccines. Some other strategies focused on behavioral approaches, such as MI or the 4C model of vaccine hesitancy. A few studies also included communication tools to help the providers in utilizing these approaches. System-level and structural supports commonly focused on integrating standing orders for vaccines and prompts in the electronic health record to ask about vaccines. Reminder and recall interventions focused on the use of technology or trained provider extenders (e.g., community health workers, patient navigators) to schedule and remind patients regarding vaccine appointments.
Table 2.
Core Themes Regarding Communication Tools and Approaches Utilized.
The impact of the tool or approach on vaccines, namely vaccine acceptance, is noted in Table 3.
Table 3.
Impact of Tool or Approach on Vaccinations.
Two-thirds of studies reported enhanced vaccine acceptance, with more benefits seen in adult studies. Pediatric studies had higher rates of mixed findings with positive and neutral results versus adult studies.
In the most common vaccines studied (HPV, influenza, and pneumococcal), intervention outcomes were overall positive. In HPV vaccination interventions, outcomes were predominantly positive or neutral. Reminder and recall interventions, patient education strategies, and provider–patient communication strategies were consistently used in the HPV interventions, particularly among adolescent patients and their parents. For example, clinics receiving announcement training had a 5.4% increase in HPV vaccine acceptance among 11- and 12-year-olds versus controls [38], while another text message reminder-based intervention improved HPV series completion from 30% to 49% and reduced time to completion by an average of 71 days [127]. A communication-based intervention saw an 17% increase in vaccine initiation and an 18% increase in vaccine completion, with an increase to 31% post-intervention [41].
Studies examining influenza vaccination interventions also revealed predominantly positive effects, with increased vaccine acceptance. Interventions focused on provider–patient communication and reminder/recall. For example, one study documented an increase in immunization rates from 8% to 39% following a free clinic-wide education and outreach initiative [61], while a transplant pharmacist-driven education and intervention initiative reported an increase from 36% to 74% after implementation [68]. Studies assessing interventions to improve pneumococcal vaccination rates consistently demonstrated positive effects and utilized provider–patient communication, system-level supports, and patient education. For example, a patient education initiative in primary care improved vaccine acceptance from 24% pre-intervention to 44% post-intervention [46]. Among liver-transplant recipients, annual pneumococcal vaccine acceptance rates increased from 46% to 58% during the intervention period (reminder/recall intervention and a provider communication tool) [54]. Similarly, 62% of intervention-group participants with inflammatory bowel disease accepted the pneumococcal vaccine compared with 23% in the control group. The intervention consisted of nurse-led communication (patient-provider communication) and patient educational materials [47].
The average quality assessment of the included studies was 6.03 ± 0.98. Of the 143 studies, 115 studies received a score of 6–8, with 16 studies receiving a 5, 9 receiving a 4, and 2 studies receiving a 3 or less. Average scores by study type are as follows: Cohort = 6.4, Cross-Sectional = 6.2, Mixed Methods = 5.4, Non-Randomized Experimental = 6.4; Qualitative = 6, RCT = 5.7; Other = 4. The quality assessment for each study can be found in Appendix A.
4. Discussion
This systematic review provided a summary of the current evidence surrounding communication tools and approaches used to improve vaccine acceptance. Because most studies (>66%) demonstrated increased vaccine acceptance, these findings support implementation of communication strategies across healthcare settings. Communication strategies clustered around a few key themes: (1) system-level supports (ex: electronic health record reminders, standing orders) and reminder/recall interventions (ex: sending text message notifications), (2) patient education materials (ex: reframing of rationale for being vaccinated), and (3) provider training and tools (ex: scripts, prompts, communication framework. These strategies were utilized individually as well as collectively to enhance vaccine acceptance.
The first strategy identified in this review was system-level supports and reminder/call interventions, which was utilized across many settings and often included small changes to address the reasons behind vaccine hesitancy. The 5C psychological antecedents by Betsch and colleagues (2018) also may be a helpful framework. In brief, much of the behaviors surrounding vaccination relate to 5 key elements: confidence (patient beliefs or attitudes with regard to vaccines), complacency (their perceived risk associated with the vaccine-related disease), constraints (barriers experienced with vaccinations), calculation (their evaluation of the vaccine and associated information-searching), and collective responsibility (their perceptions of their responsibility of protecting others through vaccination) [172]. This framework has proven useful in understanding patient choices, particularly during the COVID-19 pandemic [13]. Multiple studies integrated electronic health record (EHR) prompts, automated reminder systems for patients and for providers, text messages, and reminder phone calls which increased vaccine conversations and vaccine acceptance [86,127,146,161]. Indeed, Krantz (2018) posited that the integration of reminder interventions sustained the increased vaccine acceptance rates [86]. Several other studies utilized community health workers and patient navigators to reach patients in their home and enhance appointment scheduling [120,143], which is another approach to expand access to vaccines. Many of these approaches addressed elements such as constraints and calculation as well as other elements of the 5C antecedents. Approaches across settings, whether primary care, hospitals, community pharmacies, or other care settings could be enhanced through small changes; each community can determine which approach(es) (text messages, community health workers, provider reminders, etc.) best reaches their patient population. However, some disadvantaged settings may have limited resources to incorporate these interventions, patients may lack reliable cell phones and text message access to receive notifications, or cultural considerations may alter the receptiveness of patients and providers to these interventions. This should be explored further and adapted appropriately within resource and cultural contexts. Additionally, patient educational materials, the second key strategy, could be another low-resource option that is transferable. Educational materials were often centered around a disease and addressing misinformation or reframing the discussion surrounding the “why” of becoming vaccinated [46,135,148], However, these materials are language- and cultural context-dependent and would need adapted considerably outside of the specific language and cultural contexts that align with each study.
Many of the studies included in this review integrated provider training, whether on the tools, behavioral-based communication strategies, or how to prompt vaccine conversations, as a foundational element, which was the third key strategy. Traditional health professions education has focused on a more presumptive, directive approach to discussing vaccines. Best practices have shifted to a collaborative, patient-centered approach to elicit underlying concerns and health beliefs surrounding vaccines [26]. Interventions that trained providers in MI consistently improved vaccine acceptance [19,131,133,168]. However, concerns surrounding vaccines can be deeper than merely confidence in a vaccine. For example, the Health Belief Model [173] to explore patient beliefs about a vaccine-preventable disease and their evaluation of risk and benefits while considering cues to action (such as knowing someone who experienced consequences of the disease) [14]. The Health Belief Model also posits that individuals’ perceived benefits, barriers, and self-efficacy influence their health behaviors. Approaches like MI operationalize these constructs by eliciting patients’ beliefs, resolving ambivalence, and strengthening personal motivation to vaccinate (addressing the benefits). The consistent success of MI across vaccine types and settings suggests that interventions grounded in behavior change theory are particularly effective.
Generally, interventions focused on improving vaccine confidence and acceptance were more effective when addressing adult vaccines versus childhood vaccines. This may be influenced by a variety of factors [174,175]. First, parents typically have a strong and healthy desire to protect their children from what they might perceive as unnecessary danger or risk. For example, some parents express concerns regarding the number of vaccine doses given to children based on recommended immunization schedules. Parents also may want to avoid the child receiving injections due to a fear of needles or medical personnel. Secondly, social media influences, mainstream media reports of vaccine-related illnesses, and community or religious beliefs regarding vaccines specifically in children, have significant influence or parental decisions regarding vaccines. Also, parents typically can make decisions about vaccines for themselves, while parents serve as surrogate decision-makers for their children. Thus, the analysis of the risks and benefits may change when one is making decisions on behalf of another person, particularly children who are more vulnerable. These factors likely influence the results of vaccine confidence and should be considered when communicating with parents [174,175].
Research also was conducted primarily in the outpatient setting, such as primary care offices, and over 50% of studies focused on physicians and nurses for the intervention. Given the regularity with which patients see a primary care provider for wellness visits and chronic care visits, this setting can offer opportunities to intervene. With significant shortages in primary care access within the United States [176] and even greater ones globally [177], the primary care setting cannot be the only point of contact for vaccine conversations. Other settings where interventions occurred included hospital settings and community pharmacies [22,37,40,69,84,104,117,118,124], which are access points for older adults, patients with limited insurance, or those in medically underserved areas. Patients visit their pharmacies nearly twice as often as their primary care provider [178], and many of the pharmacy-based interventions were successful in enhancing vaccine acceptance. For example, one community pharmacy intervention for patients who had previously declined an influenza vaccine resulted in 23% of patients accepting the vaccine [124]. Similarly, a hospital-based intervention for influenza resulted in nearly 40% more patients being vaccinated [156].
It also is important to consider the context of the interventions, as briefly alluded to with patient educational materials. While over 75% of the studies were conducted in the United States, a substantial portion were completed elsewhere, namely in Europe and Asia. Concerns surrounding vaccines exist within the United States, with declining vaccine acceptance in the core pediatric vaccine series [2,3]. Global perspectives on vaccines also have shifted, with gains in vaccine confidence that occurred in the late 2010s moving to declines in the 2020s [179]. Initially indicated as one of the most significant public health threats [180], declines in vaccine confidence and vaccine acceptance raise further concerns. Thus, given that reasons for vaccine confidence may vary geographically and culturally, broadening research settings is important. Given that over two-thirds of included studies were U.S.-based, generalization to low- and middle-income countries (LMICs) also should be made cautiously for all interventions, where structural and cultural determinants of vaccine confidence may differ substantially. As underscored in theories behind health behavior change, such as the Health Belief Model [173], vaccine confidence is shaped by modifying factors (ex: cultural norms, socioeconomic factors, trust in healthcare systems and providers) that may differ by geographic region [179,181,182]. Future research should, therefore, prioritize low- and middle-income settings and evaluate whether interventions are equally effective among marginalized populations, where access and trust deficits are often greater. Studies also covered many different vaccines; with influenza, HPV, and pneumococcal vaccines being the most commonly addressed. These findings may not apply to all vaccines in all settings; further research should explore the utility of these interventions in other vaccines (ex: COVID-19 vaccines), patient populations (ex: routine pediatric immunizations), and contexts (ex: LMICs, underserved areas). However, these vaccines have some of the largest public concerns about efficacy and necessity as well as safety as well as low acceptance [183,184,185]; which should be considered when intervening. Lastly, bundling of interventions should be a focus of future research, as these could have additive impacts on vaccine acceptance within various populations.
5. Limitations
Although a research librarian was utilized to refine the search strategy, articles meeting the inclusion criteria may have been missed and not included in the review, leading to selection and reporting bias. Due to the limitation of published research, evidence emerging from or existing outside of research may have been missed. Additionally, publication bias is possible, as studies focusing on vaccine confidence that produce negative results are less likely to be published. Self-reported measures of confidence or intention also may not translate directly to vaccine acceptance or uptake. Intervention fidelity, i.e., how consistently providers and health systems implemented communication techniques and approaches, were rarely measured, limiting the ability to link interventions with outcomes. Further, the predominance of U.S. studies limits external validity related to other parts of the world.
At each stage of the systematic review process, two researchers independently completed the step, with a third reviewer resolving discrepancies. However, the review process itself may have introduced errors and incorrectly excluded relevant studies. Due to heterogeneity across studies, a thematic synthesis was conducted, which may limit precise estimations of intervention effect. The lack of quantitative analyses underscores the variability across outcomes. Although most studies were of high methodological quality, a minority exhibited weaker design rigor, reducing the interpretability of their findings.
6. Conclusions
In summary, this systematic review highlights that provider–patient communication tools and approaches, particularly those emphasizing patient-centered, collaborative strategies, consistently improve vaccine acceptance. Research should continue to evaluate these findings across global settings, particularly in diverse sociocultural and sociopolitical settings as well as in settings with differ. While most interventions were studied in outpatient primary care, evidence also demonstrates the value of expanding communication and vaccination opportunities into pharmacies, hospitals, and other community-based settings to address gaps in access. The integration of behavioral communication strategies, such as MI, combined with provider training and system-level reminders, shows particular promise in improving vaccine acceptance. Further, healthcare settings can start small by providing tools to have better conversations, integrating reminder prompts into EHR systems, and ensuring patient engagement in the decision-making process. As vaccine confidence continues to decline globally, translating these findings into routine practice is critical to avoid the burden of communicable disease.
Author Contributions
Conceptualization, A.M.H.C., J.W.C. and J.A.D.; Methodology, A.M.H.C.; Formal Analysis, A.M.H.C., S.M.T., J.A.D., M.E., A.P., T.Z., E.C., C.C. and N.G.; Investigation, A.M.H.C., J.W.C. and S.M.T.; Data Curation, A.M.H.C.; Writing—Original Draft Preparation, A.M.H.C. and T.Z.; Writing—Review and Editing, A.M.H.C., S.M.T., J.A.D., M.E., A.P., T.Z., E.C., C.C., J.W.C. and N.G.; Visualization, A.M.H.C.; Supervision, A.M.H.C.; Project Administration, A.M.H.C.; Funding Acquisition, A.M.H.C., J.W.C. and J.A.D. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported in part by a research grant from the Investigator-Initiated Studies Program of Merck Sharp & Dohme Corp [grant number 102205, 2024]. The opinions expressed in this paper are those of the authors and do not necessarily represent those of Merck Sharp & Dohme Corp.
Institutional Review Board Statement
Not applicable.
Informed Consent
Not applicable.
Data Availability Statement
The raw data supporting the conclusions of this article will be made available by the authors on request.
Conflicts of Interest
The authors declare no conflicts of interest, other than the research grant funding for the project.
Appendix A. Mixed Methods Assessment Tool (MMAT) Evaluation of Study Quality
Table A1.
Mixed Methods Assessment Tool (MMAT) Study Quality.
Table A1.
Mixed Methods Assessment Tool (MMAT) Study Quality.
| Author (Year) | MMAT Part I Score 1 | MMAT Part II Score 2 | Total Score 3 |
|---|---|---|---|
| Cohort Studies | |||
| Brackett (2015) | 2 | 5 | 7 |
| Lim (2022) | 2 | 5 | 7 |
| Schirwani (2022) | 2 | 4 | 6 |
| Shafer (2021) | 2 | 4 | 6 |
| Villaverde Piñeiro (2024) | 2 | 4 | 6 |
| Cross-Sectional Studies | |||
| Fallucca (2023) | 2 | 5 | 7 |
| Omer (2018) | 2 | 5 | 7 |
| Suryadevara (2016) | 2 | 5 | 7 |
| Warner (2020) | 2 | 5 | 7 |
| Desai (2021) | 2 | 4 | 6 |
| Gilkey (2016) | 2 | 4 | 6 |
| Hofstetter (2017) | 2 | 4 | 6 |
| Ludwikowska (2020) | 2 | 4 | 6 |
| Margolis (2021) | 2 | 4 | 6 |
| Moss (2016) | 2 | 4 | 6 |
| Opel (2015) | 2 | 4 | 6 |
| Sato (2022) | 2 | 4 | 6 |
| Vu (2022) | 2 | 4 | 6 |
| Thompson (2021) | 2 | 3 | 5 |
| Mixed-Methods Studies | |||
| Berenson (2019) | 2 | 5 | 7 |
| Cox (2022) | 2 | 4 | 6 |
| Jain (2015) | 1 | 4 | 5 |
| Kempe (2014) | 2 | 3 | 5 |
| Tabana (2016) | 2 | 2 | 4 |
| Non-Randomized Experimental Studies | |||
| Baltes (2022) | 2 | 5 | 7 |
| Bar-Shain (2015) | 2 | 5 | 7 |
| Bechini (2019) | 2 | 5 | 7 |
| Bluml (2018) | 2 | 5 | 7 |
| Brewer (2021) | 2 | 5 | 7 |
| Caffrey (2018) | 2 | 5 | 7 |
| Cates (2018) | 2 | 5 | 7 |
| Cebollero (2020) | 2 | 5 | 7 |
| Chou (2014) | 2 | 5 | 7 |
| Clark (2015) | 2 | 5 | 7 |
| Cole (2022) | 2 | 5 | 7 |
| Davis (2022) | 2 | 5 | 7 |
| Dehlinger (2021) | 2 | 5 | 7 |
| Fenton (2021) | 2 | 5 | 7 |
| Foradori (2020) | 2 | 5 | 7 |
| Frew (2022) | 2 | 5 | 7 |
| Gattis (2019) | 2 | 5 | 7 |
| Kaufman (2020) | 2 | 5 | 7 |
| Krantz (2018) | 2 | 5 | 7 |
| Loskutova (2020) | 2 | 5 | 7 |
| Molokwu (2023) | 2 | 5 | 7 |
| Nowalk (2012) | 2 | 5 | 7 |
| Page (2020) | 2 | 5 | 7 |
| Pati (2015) | 2 | 5 | 7 |
| Perkins (2015) | 2 | 5 | 7 |
| Polonijo (2021) | 2 | 5 | 7 |
| Rand (2018) | 2 | 5 | 7 |
| Sanderson (2017) | 2 | 5 | 7 |
| Zhang (2023) | 2 | 5 | 7 |
| Adam (2015) | 2 | 4 | 6 |
| Connors (2018) | 2 | 4 | 6 |
| Cotugno (2017) | 2 | 4 | 6 |
| Dehnen (2019) | 2 | 4 | 6 |
| Freedman (2015) | 2 | 4 | 6 |
| Fu (2017) | 2 | 4 | 6 |
| Hirshberg (2021) | 2 | 4 | 6 |
| Kositzke (2023) | 2 | 4 | 6 |
| Lecce (2021) | 2 | 4 | 6 |
| Li (2019) | 2 | 4 | 6 |
| Mazzoni (2016) | 2 | 4 | 6 |
| McLean (2017) | 2 | 4 | 6 |
| Queeno (2017) | 2 | 4 | 6 |
| Rand (2018) | 2 | 4 | 6 |
| Rao (2018) | 2 | 4 | 6 |
| Rao (2020) | 2 | 4 | 6 |
| Salous (2020) | 2 | 4 | 6 |
| Sandokji (2022) | 2 | 4 | 6 |
| Sobota (2015) | 2 | 4 | 6 |
| Stetson (2019) | 2 | 4 | 6 |
| Stevenson (2000) | 2 | 4 | 6 |
| Strasel (2024) | 2 | 4 | 6 |
| Suryadevara (2019) | 2 | 4 | 6 |
| Townsend (2018) | 2 | 4 | 6 |
| Wedel (2016) | 2 | 4 | 6 |
| Wright (2019) | 2 | 4 | 6 |
| Zacharias (2015) | 2 | 4 | 6 |
| Falcone (2020) | 2 | 3 | 5 |
| McCarthy (2015) | 2 | 3 | 5 |
| Labbe (2022) | 2 | 2 | 4 |
| Suryadevara (2021) | 2 | 1 | 3 |
| Qualitative Studies | |||
| Lwembe (2016) | 2 | 5 | 7 |
| McGinnis (2021) | 2 | 5 | 7 |
| Shay (2016) | 2 | 4 | 6 |
| Todorova (2014) | 2 | 2 | 4 |
| Randomized Controlled Trials (Rcts) | |||
| Dempsey (2018) | 2 | 5 | 7 |
| Dudley (2022) | 2 | 5 | 7 |
| Goodman (2015) | 2 | 5 | 7 |
| Lau (2012) | 2 | 5 | 7 |
| Lockhart (2018) | 2 | 5 | 7 |
| Rand (2017) | 2 | 5 | 7 |
| Scott (2019) | 2 | 5 | 7 |
| Chan (2015) | 2 | 5 | 7 |
| Chamberlain (2015) | 2 | 4 | 6 |
| Debroy 2023 | 2 | 4 | 6 |
| Ekmez (2022) | 2 | 4 | 6 |
| Esposito (2009) | 2 | 4 | 6 |
| Fisher (2023) | 2 | 4 | 6 |
| Fisher-Borne (2018) | 2 | 4 | 6 |
| Gilkey (2022) | 2 | 4 | 6 |
| Gilkey (2023) | 2 | 4 | 6 |
| Ginson (2000) | 2 | 4 | 6 |
| Hanley (2023) | 2 | 4 | 6 |
| Henrikson (2015) | 2 | 4 | 6 |
| Kasting (2019) | 2 | 4 | 6 |
| Klassing (2018) | 2 | 4 | 6 |
| Kriss (2017) | 2 | 4 | 6 |
| Launay (2014) | 2 | 4 | 6 |
| Meharry (2014) | 2 | 4 | 6 |
| Milkman (2021) | 2 | 4 | 6 |
| Milkman (2022) | 2 | 4 | 6 |
| Muñoz-Miralles (2022) | 2 | 4 | 6 |
| Nowalk (2016) | 2 | 4 | 6 |
| Ozdemir (2023) | 2 | 4 | 6 |
| Patel (2023) | 2 | 4 | 6 |
| Perkins (2020) | 2 | 4 | 6 |
| Reno (2018) | 2 | 4 | 6 |
| Reno (2019) | 2 | 4 | 6 |
| Werk (2019) | 2 | 4 | 6 |
| Wong (2016) | 2 | 4 | 6 |
| Brewer (2017) | 2 | 3 | 5 |
| Coenen (2017) | 2 | 3 | 5 |
| Other | |||
| O’Donnell (2018) | 2 | 4 | 6 |
| Whelan (2014) | 2 | 3 | 5 |
| Wolynn (2023) | 0 | 1 | 1 |
1 MMAT Part I Scores are based on two items surrounding clear research questions and addressing the research questions. Higher scores indicate greater study quality, with scores ranging from 0–2. 2 MMAT Part II Scores are based on the methodology of the study, such as the approach; analysis; randomization, blinding, and adherence (RCTs); representativeness; measurements. Higher scores indicate greater study quality, with scores ranging from 0–5. 3 Higher scores indicate greater study quality, with scores ranging from 0 to 7.
References
- World Health Organization. Immunization Coverage. Available online: https://www.who.int/news-room/fact-sheets/detail/immunization-coverage (accessed on 5 September 2025).
- Williams, E.; Kates, J.; Michaud, J. Kindergarten Routine Vaccination Rates Continue to Decline. Available online: https://www.kff.org/medicaid/kindergarten-routine-vaccination-rates-continue-to-decline/ (accessed on 5 September 2025).
- Centers for Disease Control and Prevention. Vaccination Coverage and Exemptions Among Kindergartners. Available online: https://www.cdc.gov/schoolvaxview/data/index.html (accessed on 5 September 2025).
- Hsu, J.L. A brief history of vaccines: Smallpox to the present. S D Med. 2013, 33–37. Available online: https://openurl.ebsco.com/EPDB%3Agcd%3A9%3A19436233/detailv2?sid=ebsco%3Aplink%3Ascholar&id=ebsco%3Agcd%3A95624065&crl=c&link_origin=scholar.google.co.uk (accessed on 28 October 2025).
- Rashid, H.; Khandaker, G.; Booy, R. Vaccination and herd immunity: What more do we know? Curr. Opin. Infect. Dis. 2012, 25, 243–249. [Google Scholar] [CrossRef]
- MacDonald, N.E. Vaccine hesitancy: Definition, scope and determinants. Vaccine 2015, 33, 4161–4164. [Google Scholar] [CrossRef]
- Williams, G. Trust issues in vaccine uptake. J. Crit. Care 2022, 67, 198–199. [Google Scholar] [CrossRef]
- Lu, P.J.; Hung, M.C.; Srivastav, A.; Grohskopf, L.A.; Kobayashi, M.; Harris, A.M.; Dooling, K.L.; Markowitz, L.E.; Rodriguez-Lainz, A.; Williams, W.W. Surveillance of vaccination coverage among adult populations-United States, 2018. MMWR Surveill Summ. 2021, 70, 1–26. [Google Scholar] [CrossRef]
- Troiano, G.; Nardi, A. Vaccine hesitancy in the era of COVID-19. Public Health 2021, 194, 245–251. [Google Scholar] [CrossRef]
- Verger, P.; Fressard, L.; Collange, F.; Gautier, A.; Jestin, C.; Launay, O.; Raude, J.; Pulcini, C.; Peretti-Watel, P. Vaccine hesitancy among general practitioners and its determinants during controversies: A national cross-sectional survey in France. eBioMedicine 2015, 2, 891–897. [Google Scholar] [CrossRef] [PubMed]
- Collange, F.; Verger, P.; Launay, O.; Pulcini, C. Knowledge, attitudes, beliefs and behaviors of general practitioners/family physicians toward their own vaccination: A systematic review. Hum. Vaccin. Immunother. 2016, 12, 1282–1292. [Google Scholar] [CrossRef] [PubMed]
- Goin-Kochel, R.P.; Fombonne, E.; Mire, S.S.; Minard, C.G.; Sahni, L.C.; Cunningham, R.M.; Boom, J.A. Beliefs about causes of autism and vaccine hesitancy among parents of children with autism spectrum disorder. Vaccine 2020, 38, 6327–6333. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, A.R.; Chu, V.; Chen, A.M.H.; Wong, J.; Khare, M.M.; Law, A. COVID-19 behavioral questionnaire (CoBQ): Comparing the pandemic’s impact on health behavior in three US states. J. Am. Coll. Clin. Pharm. 2022, 5, 590–598. [Google Scholar] [CrossRef] [PubMed]
- Mercadante, A.R.; Law, A.V. Will they, or won’t they? Examining patients’ vaccine intention for flu and COVID-19 using the Health Belief Model. Res. Soc. Adm. Pharm. 2021, 17, 1596–1605. [Google Scholar] [CrossRef]
- Santibanez, T.A.; Nguyen, K.H.; Greby, S.M.; Fisher, A.; Scanlon, P.; Bhatt, A.; Srivastav, A.; Singleton, J.A. Parental vaccine hesitancy and childhood influenza vaccination. Pediatrics 2020, 146, e2020007609. [Google Scholar] [CrossRef]
- Solís Arce, J.S.; Warren, S.S.; Meriggi, N.F.; Scacco, A.; McMurry, N.; Voors, M.; Syunyaev, G.; Malik, A.A.; Aboutajdine, S.; Adeojo, O.; et al. COVID-19 vaccine acceptance and hesitancy in low- and middle-income countries. Nat. Med. 2021, 27, 1385–1394. [Google Scholar] [CrossRef]
- Arsenault, C.; Ravishankar, S.; Lewis, T.; Armeni, P.; Croke, K.; Doubova, S.V.; McKee, M.; Tarricone, R.; Kruk, M.E. The role of health systems in shaping vaccine decisions: Insights from Italy, Mexico, the United Kingdom, and the United States. Vaccine 2025, 54, 127134. [Google Scholar] [CrossRef]
- Montero, A.; Sparks, G.; Montalvo III, J.; Kirzinger, A.; Hamel, L. KFF Tracking Poll on Health Information and Trust: Vaccine Safety and Trust. Available online: https://www.kff.org/health-information-trust/kff-tracking-poll-on-health-information-and-trust-vaccine-safety-and-trust/ (accessed on 20 October 2025).
- Cole, J.W.; A, M.H.C.; McGuire, K.; Berman, S.; Gardner, J.; Teegala, Y. Motivational interviewing and vaccine acceptance in children: The MOTIVE study. Vaccine 2022, 40, 1846–1854. [Google Scholar] [CrossRef] [PubMed]
- Gargano, L.M.; Herbert, N.L.; Painter, J.E.; Sales, J.M.; Morfaw, C.; Rask, K.; Murray, D.; DiClemente, R.J.; Hughes, J.M. Impact of a physician recommendation and parental immunization attitudes on receipt or intention to receive adolescent vaccines. Hum. Vaccin. Immunother. 2013, 9, 2627–2633. [Google Scholar] [CrossRef]
- Gagneur, A. Motivational interviewing: A powerful tool to address vaccine hesitancy. Can. Commun. Dis. Rep. 2020, 2, 93–97. [Google Scholar] [CrossRef] [PubMed]
- Brackett, A.; Butler, M.; Chapman, L. Using motivational interviewing in the community pharmacy to increase adult immunization readiness: A pilot evaluation. J. Am. Pharm. Assoc. JAPhA 2015, 55, 182–186. [Google Scholar] [CrossRef]
- Gagneur, A.; Battista, M.-C.; Boucher, F.D.; Tapiero, B.; Quach, C.; De Wals, P.; Lemaitre, T.; Farrands, A.; Boulianne, N.; Sauvageau, C.; et al. Promoting vaccination in maternity wards—Motivational interview technique reduces hesitancy and enhances intention to vaccinate, results from a multicentre non-controlled pre- and post-intervention RCT-nested study, Quebec, March 2014 to February 2015. Eurosurveillance 2019, 24, 1800641. [Google Scholar] [CrossRef] [PubMed]
- Chen, A.M.H.; Anthony, A.; Balogun, A.; Pereira, R.; Cole, J.W. The impact of motivational interviewing and MOTIVE tool use by pharmacists on vaccine acceptance. Pharmacy 2024, 12, 114. [Google Scholar] [CrossRef]
- Lemaitre, T.; Carrier, N.; Farrands, A.; Gosselin, V.; Petit, G.; Gagneur, A. Impact of a vaccination promotion intervention using motivational interview techniques on long-term vaccine coverage: The PromoVac strategy. Hum. Vaccin. Immunother. 2019, 15, 732–739. [Google Scholar] [CrossRef] [PubMed]
- Kaushik, A.; Fomicheva, J.; Boonstra, N.; Faber, E.; Gupta, S.; Kest, H. Pediatric vaccine hesitancy in the United States—The growing problem and strategies for management including motivational interviewing. Vaccines 2025, 13, 115. [Google Scholar] [CrossRef]
- Gagneur, A.; Gutnick, D.; Berthiaume, P.; Diana, A.; Rollnick, S.; Saha, P. From vaccine hesitancy to vaccine motivation: A motivational interviewing based approach to vaccine counselling. Hum. Vaccin. Immunother. 2024, 20, 2391625. [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services Office of Disease Prevention and Health Promotion. Healthy People 2030: Vaccination Programs: Community-Based Interventions Implemented in Combination. Available online: https://health.gov/healthypeople/tools-action/browse-evidence-based-resources/vaccination-programs-community-based-interventions-implemented-combination (accessed on 20 September 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- QN, H.; P, P.; S, F.; G, B.; F, B.; M, C.; P, D.; M-P, G.; F, G.; B, N.; et al. Mixed Methods Appraisal Tool (MMAT), Version 2018. Available online: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf (accessed on 5 September 2025).
- Adam, I.F.; Nakamura, K.; Kizuki, M.; Al Rifai, R.; Vanching, U. Relationship between implementing interpersonal communication and mass education campaigns in emergency settings and use of reproductive healthcare services: Evidence from Darfur, Sudan. BMJ Open 2015, 5, e008285. [Google Scholar] [CrossRef] [PubMed]
- Baltes, M.D.O.; Pronovost, E.; Kanuch, S.M.; Caron, A. Improving influenza vaccination rates in an underserved primary care clinic using a simple educational tool. Qual. Manag. Health Care 2022, 31, 80–84. [Google Scholar] [CrossRef]
- Bar-Shain, D.S.; Stager, M.M.; Runkle, A.P.; Leon, J.B.; Kaelber, D.C. Direct messaging to parents/guardians to improve adolescent immunizations. J. Adolesc. Health 2015, 56, S21–S26. [Google Scholar] [CrossRef]
- Bechini, A.; Moscadelli, A.; Pieralli, F.; Sartor, G.; Seravalli, V.; Panatto, D.; Amicizia, D.; Bonanni, P.; Boccalini, S. Impact assessment of an education course on vaccinations in a population of pregnant women: A pilot study. J. Prev. Med. Hyg. 2019, 60, E5–E11. [Google Scholar] [CrossRef]
- Berenson, A.B.; Rupp, R.; Dinehart, E.E.; Cofie, L.E.; Kuo, Y.F.; Hirth, J.M. Achieving high HPV vaccine completion rates in a pediatric clinic population. Hum. Vaccin. Immunother. 2019, 15, 1562–1569. [Google Scholar] [CrossRef]
- Birukila, G.; Babale, S.M.; Epstein, H.; Gugong, V.; Anger, R.; Corkum, M.; Jehoshaphat Nebanat, A.; Musoke, F.; Alabi, O. Reducing resistance to polio immunisation with free health camps and Bluetooth messaging: An update from Kaduna, Northern, Nigeria. Glob. Public Health 2017, 12, 19–30. [Google Scholar] [CrossRef]
- Bluml, B.M.; Brock, K.A.; Hamstra, S.; Tonrey, L. Evaluation of the impact of an innovative immunization practice model designed to improve population health: Results of the project IMPACT immunizations pilot. Popul. Health Manag. 2018, 21, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Brewer, N.T.; Hall, M.E.; Malo, T.L.; Gilkey, M.B.; Quinn, B.; Lathren, C. Announcements versus conversations to improve HPV vaccination coverage: A randomized trial. Pediatrics 2017, 139, e20161764. [Google Scholar] [CrossRef] [PubMed]
- Brewer, N.T.; Mitchell, C.G.; Alton Dailey, S.; Hora, L.; Fisher-Borne, M.; Tichy, K.; McCoy, T. HPV vaccine communication training in healthcare systems: Evaluating a train-the-trainer model. Vaccine 2021, 39, 3731–3736. [Google Scholar] [CrossRef]
- Caffrey, A.R.; DeAngelis, J.M.; Ward, K.E.; Orr, K.K.; Morrill, H.J.; Gosciminski, M.; LaPlante, K.L.; Rhode Island Pharmacy Pneumococcal Vaccination Education, G. A pharmacist-driven academic detailing program to increase adult pneumococcal vaccination. J. Am. Pharm. Assoc. JAPhA 2018, 58, 303–310. [Google Scholar] [CrossRef]
- Cates, J.R.; Crandell, J.L.; Diehl, S.J.; Coyne-Beasley, T. Immunization effects of a communication intervention to promote preteen HPV vaccination in primary care practices. Vaccine 2018, 36, 122–127. [Google Scholar] [CrossRef]
- Cebollero, J.; Walton, S.M.; Cavendish, L.; Quairoli, K.; Cwiak, C.; Kottke, M.J. Evaluation of Human Papillomavirus Vaccination after pharmacist-led intervention: A pilot project in an ambulatory clinic at a large academic urban medical center. Public Health Rep. 2020, 135, 313–321. [Google Scholar] [CrossRef]
- Chamberlain, A.T.; Seib, K.; Ault, K.A.; Rosenberg, E.S.; Frew, P.M.; Cortés, M.; Whitney, E.A.; Berkelman, R.L.; Orenstein, W.A.; Omer, S.B. Improving influenza and Tdap vaccination during pregnancy: A cluster-randomized trial of a multi-component antenatal vaccine promotion package in late influenza season. Vaccine 2015, 33, 3571–3579. [Google Scholar] [CrossRef]
- Chan, S.S.C.; Leung, D.Y.P.; Leung, A.Y.M.; Lam, C.; Hung, I.; Chu, D.; Chan, C.K.; Johnston, J.; Liu, S.H.; Liang, R.; et al. A nurse-delivered brief health education intervention to improve pneumococcal vaccination rate among older patients with chronic diseases: A cluster randomized controlled trial. Int. J. Nurs. Stud. 2015, 52, 317–324. [Google Scholar] [CrossRef]
- Chou, T.I.F.; Lash, D.B.; Malcolm, B.; Yousify, L.; Quach, J.Y.; Dong, S.; Yu, J. Effects of a student pharmacist consultation on patient knowledge and attitudes about vaccines. J. Am. Pharm. Assoc. JAPhA 2014, 54, 130–137. [Google Scholar] [CrossRef]
- Clark, R.C.; Jackson, J.; Hodges, D.; Gilliam, B.; Lane, J. Improving pneumococcal immunization rates in an ambulatory setting. J. Nurs. Care Qual. 2015, 30, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Coenen, S.; Weyts, E.; Jorissen, C.; De Munter, P.; Noman, M.; Ballet, V.; Vermeire, S.; Van Assche, G.; Ferrante, M. Effects of education and information on vaccination behavior in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2017, 23, 318–324. [Google Scholar] [CrossRef]
- Connors, J.T.; Hodges, E.A.; D’Auria, J.; Windham, L. Implementing vaccine hesitancy screening for targeted education. J. Am. Assoc. Nurse Pract. 2018, 30, 450–459. [Google Scholar] [CrossRef]
- Cotugno, S.; Morrow, G.; Cooper, C.; Cabie, M.; Cohn, S. Impact of pharmacist intervention on influenza vaccine assessment and documentation in hospitalized psychiatric patients. Am. J. Health Syst. Pharm. 2017, 74, S90–S94. [Google Scholar] [CrossRef]
- Cox, J.E.; Bogart, L.M.; Elliott, M.N.; Starmer, A.J.; Meleedy-Rey, P.; Goggin, K.; Banerjee, T.; Samuels, R.C.; Hahn, P.D.; Epee-Bounya, A.; et al. Improving HPV vaccination rates in a racially and ethnically diverse pediatric population. Pediatrics 2022, 150, e2021054186. [Google Scholar] [CrossRef] [PubMed]
- Davis, K.R.; Norman, S.L.; Olson, B.G.; Demirel, S.; Taha, A.A. A clinical educational intervention to increase HPV vaccination rates among pediatric patients through enhanced recommendations. J. Pediatr. Healthc. 2022, 36, 589–597. [Google Scholar] [CrossRef] [PubMed]
- Debroy, P.; Balu, R.; Burnett, R.; Johnson, R.A.; Kappes, H.B.; Wallace, J.M.; Marconi, V.C. A cluster randomized controlled trial of a modified vaccination clinical reminder for primary care providers. Health Psychol. 2023, 42, 195–204. [Google Scholar] [CrossRef]
- Dehlinger, C.; Nypaver, C.; Whiteside, J. Use of an evidence-based approach to improve influenza vaccination uptake in pregnancy. J. Midwifery Womens Health 2021, 66, 360–365. [Google Scholar] [CrossRef]
- Dehnen, D.; Herwig, A.; Herzer, K.; Weltermann, B. Improving the vaccination status of liver transplant patients: Effectiveness of personally addressing patients and written recommendations to family physicians after 3 years. Transpl. Infect. Dis. 2019, 21, e13140. [Google Scholar] [CrossRef] [PubMed]
- Dempsey, A.F.; Maertens, J.; Sevick, C.; Jimenez-Zambrano, A.; Juarez-Colunga, E. A randomized, controlled, pragmatic trial of an iPad-based, tailored messaging intervention to increase human papillomavirus vaccination among Latinos. Hum. Vaccin. Immunother. 2019, 15, 1577–1584. [Google Scholar] [CrossRef]
- Dempsey, A.F.; Pyrznawoski, J.; Lockhart, S.; Barnard, J.; Campagna, E.J.; Garrett, K.; Fisher, A.; Dickinson, L.M.; O’Leary, S.T. Effect of a health care professional communication training intervention on adolescent Human Papillomavirus Vaccination: A cluster randomized clinical trial. JAMA Pediatr. 2018, 172, e180016. [Google Scholar] [CrossRef]
- Desai, P.; Kaur, G.; Fanglong, D.; Rodriguez, M.H. COVID-19 vaccine acceptance in pregnancy. Neonatol. Today 2021, 16, 11–15. [Google Scholar] [CrossRef]
- Dudley, M.Z.; Omer, S.B.; O’Leary, S.T.; Limaye, R.J.; Ellingson, M.K.; Spina, C.I.; Brewer, S.E.; Bednarczyk, R.A.; Chamberlain, A.T.; Malik, F.; et al. MomsTalkShots, tailored educational app, improves vaccine attitudes: A randomized controlled trial. BMC Public Health 2022, 22, 2134. [Google Scholar] [CrossRef]
- Ekmez, F.; Ekmez, M. Effects of information sources in HPV vaccine acceptance: Prospective randomized trial. Postgrad. Med. 2022, 134, 829–833. [Google Scholar] [CrossRef]
- Esposito, S.; Pelucchi, C.; Tel, F.; Chiarelli, G.; Sabatini, C.; Semino, M.; Marseglia, G.L.; De Mattia, D.; Principi, N. Factors conditioning effectiveness of a reminder/recall system to improve influenza vaccination in asthmatic children. Vaccine 2009, 27, 633–635. [Google Scholar] [CrossRef]
- Falcone, A.L.; Vess, J.; Johnson, E. Evidence-based interventions cause multifold increase of influenza immunization rates in a free clinic. J. Am. Assoc. Nurse Pract. 2020, 32, 817–823. [Google Scholar] [CrossRef]
- Fisher, K.A.; Nguyen, N.; Fouayzi, H.; Singh, S.; Crawford, S.; Mazor, K.M. Impact of a physician recommendation on COVID-19 vaccination intent among vaccine hesitant individuals. Patient Educ. Couns. 2023, 106, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Fisher-Borne, M.; Preiss, A.J.; Black, M.; Roberts, K.; Saslow, D. Early outcomes of a multilevel Human Papillomavirus Vaccination pilot intervention in Federally Qualified Health Centers. Acad. Pediatr. 2018, 18, S79–S84. [Google Scholar] [CrossRef]
- Foradori, D.M.; Sampayo, E.M.; Fanny, S.A.; Namireddy, M.K.; Kumar, A.M.; Huay-ying, L. Improving influenza vaccination in hospitalized children with asthma. Pediatrics 2020, 145, e20191735. [Google Scholar] [CrossRef] [PubMed]
- Freedman, J.L.; Reilly, A.F.; Powell, S.C.; Bailey, L.C. Quality improvement initiative to increase influenza vaccination in pediatric cancer patients. Pediatrics 2015, 135, e540–e546. [Google Scholar] [CrossRef] [PubMed]
- Frew, P.M.; Gonzalez-Casanova, I.; Otieno, N.A.; Malik, F.A.; Fenimore, V.L.; Owino, D.; Adero, M.O.; Atito, R.O.; Bigogod, G.; Chaves, S.S.; et al. Development of effective messages to promote maternal immunization in Kenya. Vaccine 2022, 40, 3761–3770. [Google Scholar] [CrossRef]
- Fu, L.Y.; Zimet, G.D.; Latkin, C.A.; Joseph, J.G. Associations of trust and healthcare provider advice with HPV vaccine acceptance among African American parents. Vaccine 2017, 35, 802–807. [Google Scholar] [CrossRef]
- Gattis, S.; Yildirim, I.; Shane, A.L.; Serluco, S.; McCracken, C.; Liverman, R. Impact of pharmacy-initiated interventions on influenza vaccination rates in pediatric solid organ transplant recipients. J. Pediatr. Infect. Dis. Soc. 2019, 8, 525–530. [Google Scholar] [CrossRef]
- Gatwood, J.; Renfro, C.; Hagemann, T.; Chiu, C.-Y.; Kapan, S.; Frederick, K.; Hohmeier, K.C. Facilitating pneumococcal vaccination among high-risk adults: Impact of an assertive communication training program for community pharmacists. J. Am. Pharm. Assoc. JAPhA 2021, 61, 572–580.e571. [Google Scholar] [CrossRef]
- Gilkey, M.B.; Calo, W.A.; Moss, J.L.; Shah, P.D.; Marciniak, M.W.; Brewer, N.T. Provider communication and HPV vaccination: The impact of recommendation quality. Vaccine 2016, 34, 1187–1192. [Google Scholar] [CrossRef]
- Gilkey, M.B.; Grabert, B.K.; Heisler-MacKinnon, J.; Bjork, A.; Boynton, M.H.; Kim, K.; Alton Dailey, S.; Liu, A.; Todd, K.G.; Schauer, S.L.; et al. Coaching and communication training for HPV vaccination: A cluster randomized trial. Pediatrics 2022, 150, e2021052351. [Google Scholar] [CrossRef] [PubMed]
- Gilkey, M.B.; Heisler-MacKinnon, J.; Boynton, M.H.; Calo, W.A.; Moss, J.L.; Brewer, N.T. Impact of brief quality improvement coaching on adolescent HPV vaccination coverage: A pragmatic cluster randomized trial. Cancer Epidemiol. Biomark. Prev. 2023, 32, 957–962. [Google Scholar] [CrossRef]
- Ginson, S.H.; Malmberg, C.; French, D.J. Impact on vaccination rates of a pharmacist-initiated influenza and pneumococcal vaccination program. Can. J. Hosp. Pharm. 2000, 53, 1163–1172. [Google Scholar] [CrossRef]
- Goodman, K.; Mossad, S.B.; Taksler, G.B.; Emery, J.; Schramm, S.; Rothberg, M.B. Impact of video education on influenza vaccination in pregnancy. J. Reprod. Med. 2015, 60, 471–479. [Google Scholar] [PubMed]
- Hanley, K.; Chung, T.H.; Nguyen, L.K.; Amadi, T.; Stansberry, S.; Yetman, R.J.; Foxhall, L.E.; Bello, R.; Diallo, T.; Le, Y.C.L. Using electronic reminders to improve Human Papillomavirus (HPV) vaccinations among primary care patients. Vaccines 2023, 11, 872. [Google Scholar] [CrossRef]
- Henrikson, N.B.; Opel, D.J.; Grothaus, L.; Nelson, J.; Scrol, A.; Dunn, J.; Faubion, T.; Roberts, M.; Marcuse, E.K.; Grossman, D.C. Physician communication training and parental vaccine hesitancy: A randomized trial. Pediatrics 2015, 136, 70–79. [Google Scholar] [CrossRef]
- Hirshberg, J.S.; Huysman, B.C.; Oakes, M.C.; Cater, E.B.; Odibo, A.O.; Raghuraman, N.; Kelly, J.C. Offering onsite COVID-19 vaccination to high-risk obstetrical patients: Initial findings. Am. J. Obs. Gynecol. MFM 2021, 3, 100478. [Google Scholar] [CrossRef] [PubMed]
- Ho, H.J.; Tan, Y.-R.; Cook, A.R.; Koh, G.; Tham, T.Y.; Anwar, E.; Hui Chiang, G.S.; Lwin, M.O.; Chen, M.I. Increasing influenza and pneumococcal vaccination uptake in seniors using point-of-care informational interventions in primary care in Singapore: A pragmatic, cluster-randomized crossover trial. Am. J. Public Health 2019, 109, 1776–1783. [Google Scholar] [CrossRef] [PubMed]
- Hofstetter, A.M.; Robinson, J.D.; Lepere, K.; Cunningham, M.; Etsekson, N.; Opel, D.J. Clinician-parent discussions about influenza vaccination of children and their association with vaccine acceptance. Vaccine 2017, 35, 2709–2715. [Google Scholar] [CrossRef]
- Jain, M.; Taneja, G.; Amin, R.; Steinglass, R.; Favin, M. Engaging communities with a simple tool to help increase immunization coverage. Glob. Health Sci. Pract. 2015, 3, 117–125. [Google Scholar] [CrossRef]
- Kasting, M.L.; Head, K.J.; Cox, D.; Cox, A.D.; Zimet, G.D. The effects of message framing and healthcare provider recommendation on adult hepatitis B vaccination: A randomized controlled trial. Prev. Med. 2019, 127, 105798. [Google Scholar] [CrossRef]
- Kaufman, J.; Attwell, K.; Tuckerman, J.; O’Sullivan, J.; Omer, S.B.; Leask, J.; Regan, A.; Marshall, H.; Lee, K.J.; Snelling, T.; et al. Feasibility and acceptability of the multi-component P3-MumBubVax antenatal intervention to promote maternal and childhood vaccination: A pilot study. Vaccine 2020, 38, 4024–4031. [Google Scholar] [CrossRef]
- Kempe, A.; Albright, K.; O’Leary, S.; Kolasa, M.; Barnard, J.; Kile, D.; Lockhart, S.; Dickinson, L.M.; Shmueli, D.; Babbel, C. Effectiveness of primary care–public health collaborations in the delivery of influenza vaccine: A cluster-randomized pragmatic trial. Prev. Med. 2014, 69, 110–116. [Google Scholar] [CrossRef]
- Klassing, H.M.; Ruisinger, J.F.; Prohaska, E.S.; Melton, B.L. Evaluation of pharmacist-initiated interventions on vaccination rates in patients with Asthma or COPD. J. Community Health 2018, 43, 297–303. [Google Scholar] [CrossRef] [PubMed]
- Kositzke, C.; Linscheid, L.; Sheehan, A. Improving pediatric influenza vaccination rates in the primary care setting. Pediatr. Nurs. 2023, 49, 247–253. [Google Scholar] [CrossRef]
- Krantz, L.; Ollberding, N.J.; Beck, A.F.; Carol Burkhardt, M. Increasing HPV vaccination coverage through provider-based interventions. Clin. Pediatr. 2018, 57, 319–326. [Google Scholar] [CrossRef]
- Kriss, J.L.; Frew, P.M.; Cortes, M.; Malik, F.A.; Chamberlain, A.T.; Seib, K.; Flowers, L.; Ault, K.A.; Howards, P.P.; Orenstein, W.A.; et al. Evaluation of two vaccine education interventions to improve pertussis vaccination among pregnant African American women: A randomized controlled trial. Vaccine 2017, 35, 1551–1558. [Google Scholar] [CrossRef]
- Labbe, S.; Colmegna, I.; Valerio, V.; Boucher, V.G.; Pelaez, S.; Dragomir, A.I.; Laurin, C.; Hazel, E.M.; Bacon, S.L.; Lavoie, K.L. Training physicians in motivational communication to address influenza vaccine hesitation: A proof-of-concept study. Vaccines 2022, 10, 143. [Google Scholar] [CrossRef]
- Lau, A.Y.; Sintchenko, V.; Crimmins, J.; Magrabi, F.; Gallego, B.; Coiera, E. Impact of a web-based personally controlled health management system on influenza vaccination and health services utilization rates: A randomized controlled trial. J. Am. Med. Inf. Assoc. 2012, 19, 719–727. [Google Scholar] [CrossRef]
- Launay, O.; Le Strat, Y.; Tosini, W.; Kara, L.; Quelet, S.; Lévy, S.; Danan, J.; Réveillon, J.; Houdayer, J.; Bouvet, E.; et al. Impact of free on-site vaccine and/or healthcare workers training on hepatitis B vaccination acceptability in high-risk subjects: A pre-post cluster randomized study. Clin. Microbiol. Infect. 2014, 20, 1033–1039. [Google Scholar] [CrossRef] [PubMed]
- Lecce, M.; Perrone, P.M.; Bonalumi, F.; Castaldi, S.; Cremonesi, M. 2020-21 Influenza vaccination campaign strategy as a model for the third COVID-19 vaccine dose? Acta Biomed 2021, 92, e2021447. [Google Scholar] [CrossRef]
- Li, A.; Chan, Y.-H.; Liew, M.F.; Pandey, R.; Phua, J. Improving influenza vaccination coverage among patients with COPD: A pilot project. Int. J. Chron. Obs. Pulmon Dis. 2019, 14, 2527–2533. [Google Scholar] [CrossRef] [PubMed]
- Lim, C.; Van Alphen, M.U.; Maclaurin, S.; Mulligan, C.; Macri, B.; Cather, C.; Freudenreich, O. Increasing COVID-19 vaccination rates among patients with serious mental illness: A pilot intervention study. Psychiatr. Serv. 2022, 73, 1274–1277. [Google Scholar] [CrossRef]
- Lockhart, S.; Dempsey, A.F.; Pyrzanowski, J.; O’Leary, S.T.; Barnard, J.G. Provider and parent perspectives on enhanced communication tools for Human Papillomavirus Vaccine-hesitant parents. Acad. Pediatr. 2018, 18, 776–782. [Google Scholar] [CrossRef]
- Loskutova, N.Y.; Smail, C.; Callen, E.; Staton, E.W.; Nazir, N.; Webster, B.; Pace, W.D. Effects of multicomponent primary care-based intervention on immunization rates and missed opportunities to vaccinate adults. BMC Fam. Pract. 2020, 21, 46. [Google Scholar] [CrossRef]
- Ludwikowska, K.M.; Biela, M.; Szenborn, L. HPV vaccine acceptance and hesitancy—Lessons learned during 8 years of regional HPV prophylaxis program in Wroclaw, Poland. Eur. J. Cancer Prev. 2020, 29, 346–349. [Google Scholar] [CrossRef]
- Lwembe, S.; Green, S.A.; Tanna, N.; Connor, J.; Valler, C.; Barnes, R. A qualitative evaluation to explore the suitability, feasibility and acceptability of using a ‘celebration card’ intervention in primary care to improve the uptake of childhood vaccinations. BMC Fam. Pract. 2016, 17, 101. [Google Scholar] [CrossRef] [PubMed]
- Margolis, M.A.; Brewer, N.T.; Boynton, M.H.; Lafata, J.E.; Southwell, B.G.; Gilkey, M.B. Provider response and follow-up to parental declination of HPV vaccination. Vaccine 2022, 40, 344–350. [Google Scholar] [CrossRef]
- Mazzoni, S.E.; Brewer, S.E.; Pyrzanowski, J.L.; Durfee, M.J.; Dickinson, L.M.; Barnard, J.G.; Dempsey, A.F.; O’Leary, S.T. Effect of a multi-modal intervention on immunization rates in obstetrics and gynecology clinics. Am. J. Obs. Gynecol. 2016, 214, e611–e617. [Google Scholar] [CrossRef]
- McCarthy, E.A.; Pollock, W.E.; Tapper, L.; Sommerville, M.; McDonald, S. Increasing uptake of influenza vaccine by pregnant women post H1N1 pandemic: A longitudinal study in Melbourne, Australia, 2010 to 2014. BMC Pregnancy Childbirth 2015, 15, 53. [Google Scholar] [CrossRef][Green Version]
- McGinnis, J.M.; Jones, R.; Hillis, C.; Kokus, H.; Thomas, H.; Thomas, J.; Alyafi, M.; Bernard, L.; Eiriksson, L.R.; Elit, L.M.; et al. A pneumococcal pneumonia and influenza vaccination quality improvement program for women receiving chemotherapy for gynecologic cancers at a major tertiary cancer Centre. Gynecol. Oncol. 2021, 161, 236–243. [Google Scholar] [CrossRef]
- McLean, H.Q.; VanWormer, J.J.; Chow, B.D.W.; Birchmeier, B.; Vickers, E.; DeVries, E.; Meyer, J.; Moore, J.; McNeil, M.M.; Stokley, S.; et al. Improving Human Papillomavirus Vaccine use in an integrated health system: Impact of a provider and staff intervention. J. Adolesc. Health 2017, 61, 252–258. [Google Scholar] [CrossRef]
- Meharry, P.M.; Cusson, R.M.; Stiller, R.; Vázquez, M. Maternal influenza vaccination: Evaluation of a patient-centered pamphlet designed to increase uptake in pregnancy. Matern. Child. Health J. 2014, 18, 1205–1214. [Google Scholar] [CrossRef]
- Milkman, K.L.; Gandhi, L.; Patel, M.S.; Graci, H.N.; Gromet, D.M.; Ho, H.; Kay, J.S.; Lee, T.W.; Rothschild, J.; Bogard, J.E.; et al. A 680,000-person megastudy of nudges to encourage vaccination in pharmacies. Proc. Natl. Acad. Sci. USA 2022, 119, e2115126119. [Google Scholar] [CrossRef] [PubMed]
- Milkman, K.L.; Patel, M.S.; Gandhi, L.; Graci, H.N.; Gromet, D.M.; Ho, H.; Kay, J.S.; Lee, T.W.; Akinola, M.; Beshears, J.; et al. A megastudy of text-based nudges encouraging patients to get vaccinated at an upcoming doctor’s appointment. Proc. Natl. Acad. Sci. USA 2021, 118, e2101165118. [Google Scholar] [CrossRef] [PubMed]
- Molokwu, J.; Mendez, M.; Bracamontes, C. The effect of clinical decision prompts in improving Human Papillomavirus Vaccination rates in a multispecialty practice in a predominantly Hispanic population: Quasi-experimental study. JMIR Cancer 2023, 9, e42890. [Google Scholar] [CrossRef]
- Moss, J.L.; Reiter, P.L.; Rimer, B.K.; Brewer, N.T. Collaborative patient-provider communication and uptake of adolescent vaccines. Soc. Sci. Med. 2016, 159, 100–107. [Google Scholar] [CrossRef]
- Muñoz-Miralles, R.; Nadeu, S.B.; Masoliver, C.S.; Gallego, A.M.; del Canto, J.G.; Peña, J.M.; Esteve, A.M.B. Original effectiveness of a brief intervention for acceptance of influenza vaccine in reluctant primary care patients. Gac. Sanit. 2022, 36, 446–451. [Google Scholar] [CrossRef]
- Nowalk, M.P.; Lin, C.J.; Pavlik, V.N.; Brown, A.E.; Zhang, S.; Moehling, K.K.; Raviotta, J.M.; South-Paul, J.E.; Hawk, M.; Ricci, E.M.; et al. Using the 4 Pillars™ Practice Transformation Program to increase adult Tdap immunization in a randomized controlled cluster trial. Vaccine 2016, 34, 5026–5033. [Google Scholar] [CrossRef]
- Nowalk, M.P.; Nutini, J.; Raymund, M.; Ahmed, F.; Albert, S.M.; Zimmerman, R.K. Evaluation of a toolkit to introduce standing orders for influenza and pneumococcal vaccination in adults: A multimodal pilot project. Vaccine 2012, 30, 5978–5982. [Google Scholar] [CrossRef]
- O’Donnell, M.; Shurpin, K.; Janotha, B. Improving herpes zoster vaccine rates: The impact of a targeted educational program. J. Am. Acad. Nurse Pract. 2018, 30, 435–442. [Google Scholar] [CrossRef] [PubMed]
- O’Leary, S.T.; Pyrzanowski, J.; Brewer, S.E.; Sevick, C.; Miriam Dickinson, L.; Dempsey, A.F. Effectiveness of a multimodal intervention to increase vaccination in obstetrics/gynecology settings. Vaccine 2019, 37, 3409–3418. [Google Scholar] [CrossRef] [PubMed]
- Okuhara, T.; Okada, H.; Goto, E.; Tsunezumi, A.; Kagawa, Y.; Kiuchi, T. Encouraging COVID-19 vaccination via an evolutionary theoretical approach: A randomized controlled study in Japan. Patient Educ. Couns. 2022, 105, 2248–2255. [Google Scholar] [CrossRef]
- Omer, S.B.; Allen, K.; Chang, D.H.; Guterman, L.B.; Bednarczyk, R.A.; Jordan, A.; Buttenheim, A.; Jones, M.; Hannan, C.; deHart, M.P.; et al. Exemptions from mandatory immunization after legally mandated parental counseling. Pediatrics 2018, 141, e20172364. [Google Scholar] [CrossRef]
- Omer, S.B.; O’Leary, S.T.; Bednarczyk, R.A.; Ellingson, M.K.; Spina, C.I.; Dudley, M.Z.; Chamberlain, A.T.; Limaye, R.J.; Brewer, S.E.; Frew, P.M.; et al. Multi-tiered intervention to increase maternal immunization coverage: A randomized, controlled trial. Vaccine 2022, 40, 4955–4963. [Google Scholar] [CrossRef] [PubMed]
- Opel, D.J.; Mangione-Smith, R.; Robinson, J.D.; Heritage, J.; DeVere, V.; Salas, H.S.; Zhou, C.; Taylor, J.A. The influence of provider communication behaviors on parental vaccine acceptance and visit experience. Am. J. Public Health 2015, 105, 1998–2004. [Google Scholar] [CrossRef]
- Ozdemir, N.; Aktas, B.Y.; Gulmez, A.; Inkaya, A.C.; Bayraktar-Ekincioglu, A.; Kilickap, S.; Unal, S. Impact of pharmacist-led educational intervention on pneumococcal vaccination rates in cancer patients: A randomized controlled study. Support. Care Cancer Off. J. Multinatl. Assoc. Support. Care Cancer 2023, 31, 194. [Google Scholar] [CrossRef]
- Page, A.; Harrison, A.; Nadpara, P.; Goode, J.-V.R. Pharmacist impact on pneumococcal polysaccharide vaccination rates in patients with diabetes in a national grocery chain pharmacy. J. Am. Pharm. Assoc. JAPhA 2020, 60, S51–S55.e51. [Google Scholar] [CrossRef] [PubMed]
- Patel, M.S.; Milkman, K.L.; Gandhi, L.; Graci, H.N.; Gromet, D.; Ho, H.; Kay, J.S.; Lee, T.W.; Rothschild, J.; Akinola, M.; et al. A randomized trial of behavioral nudges delivered through text messages to increase influenza vaccination among patients with an upcoming primary care visit. Am. J. Health Promot. 2023, 37, 324–332. [Google Scholar] [CrossRef] [PubMed]
- Pati, S.; Ladowski, K.L.; Wong, A.T.; Huang, J.; Yang, J. An enriched medical home intervention using community health workers improves adherence to immunization schedules. Vaccine 2015, 33, 6257–6263. [Google Scholar] [CrossRef] [PubMed]
- Perkins, R.B.; Legler, A.; Jansen, E.; Bernstein, J.; Pierre-Joseph, N.; Eun, T.J.; Biancarelli, D.L.; Schuch, T.J.; Leschly, K.; Fenton, A.T.H.R.; et al. Improving HPV vaccination rates: A stepped-wedge randomized trial. Pediatrics 2020, 146, e20192737. [Google Scholar] [CrossRef]
- Perkins, R.B.; Zisblatt, L.; Legler, A.; Trucks, E.; Hanchate, A.; Gorin, S.S. Effectiveness of a provider-focused intervention to improve HPV vaccination rates in boys and girls. Vaccine 2015, 33, 1223–1229. [Google Scholar] [CrossRef]
- Polonijo, A.N.; Lee, S.S.; Nagpal, N.; Barros, R.; Hopfer, S.; Brown, B.; Pellman, H.; Singh, J. How do patient-provider relationship continuity, gender, and language affect pediatric HPV vaccine acceptance? Hum. Vaccin. Immunother. 2021, 17, 4467–4469. [Google Scholar] [CrossRef]
- Queeno, B.V. Evaluation of inpatient influenza and pneumococcal vaccination acceptance rates with pharmacist education. J. Pharm. Pract. 2017, 30, 202–208. [Google Scholar] [CrossRef]
- Rand, C.M.; Schaffer, S.J.; Dhepyasuwan, N.; Blumkin, A.; Albertin, C.; Serwint, J.R.; Darden, P.M.; Humiston, S.G.; Mann, K.J.; Stratbucker, W.; et al. Provider communication, prompts, and feedback to improve HPV vaccination rates in resident clinics. Pediatrics 2018, 141, e20170498. [Google Scholar] [CrossRef]
- Rand, C.M.; Tyrrell, H.; Wallace-Brodeur, R.; Goldstein, N.P.N.; Darden, P.M.; Humiston, S.G.; Albertin, C.S.; Stratbucker, W.; Schaffer, S.J.; Davis, W.; et al. A learning collaborative model to improve Human Papillomavirus Vaccination rates in primary care. Acad. Pediatr. 2018, 18, S46–S52. [Google Scholar] [CrossRef]
- Rand, C.M.; Vincelli, P.; Goldstein, N.P.N.; Blumkin, A.; Szilagyi, P.G. Effects of phone and text message reminders on completion of the Human Papillomavirus Vaccine series. J. Adolesc. Health 2017, 60, 113–119. [Google Scholar] [CrossRef]
- Rao, S.; Fischman, V.; Kaplan, D.W.; Wilson, K.M.; Hyman, D. Evaluating interventions to increase influenza vaccination rates among pediatric inpatients. Pediatr. Qual. Saf. 2018, 3, e102. [Google Scholar] [CrossRef]
- Rao, S.; Ziniel, S.I.; Khan, I.a.; Dempsey, A. Be inFLUential: Evaluation of a multifaceted intervention to increase influenza vaccination rates among pediatric inpatients. Vaccine 2020, 38, 1370–1377. [Google Scholar] [CrossRef] [PubMed]
- Real, F.J.; DeBlasio, D.; Beck, A.F.; Ollberding, N.J.; Davis, D.; Cruse, B.; Samaan, Z.; McLinden, D.; Klein, M.D. A virtual reality curriculum for pediatric residents decreases rates of influenza vaccine refusal. Acad. Pediatr. 2017, 17, 431–435. [Google Scholar] [CrossRef] [PubMed]
- Reno, J.E.; O’Leary, S.; Garrett, K.; Pyrzanowski, J.; Lockhart, S.; Campagna, E.; Barnard, J.; Dempsey, A.F. Improving provider communication about HPV vaccines for vaccine-hesitant parents through the use of motivational interviewing. J. Health Commun. 2018, 23, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Reno, J.E.; O’Leary, S.T.; Pyrzanowski, J.; Lockhart, S.; Thomas, J.; Dempsey, A.F. Evaluation of the implementation of a multicomponent intervention to improve health care provider communication about Human Papillomavirus Vaccination. Acad. Pediatr. 2018, 18, 882–888. [Google Scholar] [CrossRef]
- Reno, J.E.; Thomas, J.; Pyrzanowski, J.; Lockhart, S.; O’Leary, S.T.; Campagna, E.J.; Dempsey, A.F. Examining strategies for improving healthcare providers’ communication about adolescent HPV vaccination: Evaluation of secondary outcomes in a randomized controlled trial. Hum. Vaccin. Immunother. 2019, 15, 1592–1598. [Google Scholar] [CrossRef]
- Salous, M.H.; Bind, M.A.; Granger, L.; Johnson, L.B.; Welch, K.; Villa, A. An educational intervention on HPV knowledge and comfortability discussing vaccination among oral health care professionals of the American Indian and Alaskan Native population. Hum. Vaccin. Immunother. 2020, 16, 3131–3137. [Google Scholar] [CrossRef]
- Sanderson, M.; Canedo, J.R.; Khabele, D.; Fadden, M.K.; Harris, C.; Beard, K.; Burress, M.; Pinkerton, H.; Jackson, C.; Mayo-Gamble, T.; et al. Pragmatic trial of an intervention to increase human papillomavirus vaccination in safety-net clinics. BMC Public Health 2017, 17, 158. [Google Scholar] [CrossRef]
- Sandokji, I.; Anderson, L.S.; Warejko, J.K.; Emerson, B.L.; Greenberg, J.H. An initiative to improve pneumococcal immunization counseling in children with nephrotic syndrome. Pediatr. Nephrol. 2022, 37, 1333–1338. [Google Scholar] [CrossRef]
- Sato, K.; Kondo, N.; Murata, C.; Shobugawa, Y.; Saito, K.; Kondo, K. Association of pneumococcal and influenza vaccination with patient-physician communication in older adults: A nationwide cross-sectional study From the JAGES 2016. J. Epidemiol. 2022, 32, 401–407. [Google Scholar] [CrossRef]
- Schirwani, N.; Pateisky, P.; Koren, T.; Farr, A.; Kiss, H.; Bancher-Todesca, D. Written briefing and oral counseling increase the willingness to receive the SARS-CoV-2 vaccination among women in puerperium: A qualitative prospective cohort study. Vaccines 2022, 10, 1505. [Google Scholar] [CrossRef] [PubMed]
- Scott, V.P.; Opel, D.J.; Reifler, J.; Rikin, S.; Pethe, K.; Barrett, A.; Stockwell, M.S. Office-based educational handout for influenza vaccination: A randomized controlled trial. Pediatrics 2019, 144, e20182580. [Google Scholar] [CrossRef]
- Shafer, R.; Kearns, C.; Carney, M.; Sagar, A. Leveraging interdisciplinary teams for pre-visit planning to improve pneumococcal immunization rates among internal medicine subspecialty practices. J. Prim. Care Community Health 2021, 12, 21501319211060986. [Google Scholar] [CrossRef]
- Shay, L.A.; Street, R.L.; Baldwin, A.S.; Marks, E.G.; Lee, S.C.; Higashi, R.T.; Skinner, C.S.; Fuller, S.; Persaud, D.; Tiro, J.A. Characterizing safety-net providers’ HPV vaccine recommendations to undecided parents: A pilot study. Patient Educ. Couns. 2016, 99, 1452–1460. [Google Scholar] [CrossRef]
- Shegog, R.; Savas, L.S.; Healy, C.M.; Frost, E.L.; Coan, S.P.; Gabay, E.K.; Preston, S.M.; Spinner, S.W.; Wilbur, M.; Becker, E.; et al. AVPCancerFree: Impact of a digital behavior change intervention on parental HPV vaccine-related perceptions and behaviors. Hum. Vaccin. Immunother. 2022, 18, 2087430. [Google Scholar] [CrossRef]
- Sobota, A.E.; Kavanagh, P.L.; Adams, W.G.; McClure, E.; Farrell, D.; Sprinz, P.G. Improvement in influenza vaccination rates in a pediatric sickle cell disease clinic. Pediatr. Blood Cancer 2015, 62, 654–657. [Google Scholar] [CrossRef][Green Version]
- Stetson, R.C.; Fang, J.L.; Colby, C.E.; Jacobson, R.M. Improving infant vaccination status in a level IV neonatal intensive care unit. Pediatrics 2019, 144, e20190337. [Google Scholar] [CrossRef]
- Stevenson, K.B.; McMahon, J.W.; Harris, J.; Hillman, J.R.; Helgerson, S.D. Increasing pneumococcal vaccination rates among residents of long-term-care facilities: Provider-based improvement strategies implemented by peer-review organizations in four western states. Infect. Control Hosp. Epidemiol. 2000, 21, 705–710. [Google Scholar] [CrossRef]
- Strasel, M.; VanLangen, K.M.; Benzer, J.; Geyer, A.; Jameson, A.P.; Dumkow, L.E. HPV vaccination rates in 9- and 10-year-olds following a pharmacist-led intervention. J. Am. Pharm. Assoc. JAPhA 2024, 64, 278–282. [Google Scholar] [CrossRef]
- Suryadevara, M.; Bonville, C.A.; Cibula, D.A.; Domachowske, J.B. Cancer prevention education for providers, staff, parents, and teens improves adolescent Human Papillomavirus Immunization rates. J. Pediatr. 2019, 205, 145–152.e142. [Google Scholar] [CrossRef]
- Suryadevara, M.; Bonville, C.A.; Cibula, D.A.; Domachowske, J.B. Multi-component cancer prevention awareness program to improve adolescent HPV vaccine uptake. Hum. Vaccin. Immunother. 2021, 17, 1052–1058. [Google Scholar] [CrossRef]
- Suryadevara, M.; Bonville, J.R.; Kline, R.M.; Magowan, C.; Domachowske, E.; Cibula, D.A.; Domachowske, J.B. Student HPV vaccine attitudes and vaccine completion by education level. Hum. Vaccin. Immunother. 2016, 12, 1491–1497. [Google Scholar] [CrossRef]
- Szilagyi, P.G.; Serwint, J.R.; Humiston, S.G.; Rand, C.M.; Schaffer, S.; Vincelli, P.; Dhepyasuwan, N.; Blumkin, A.; Albertin, C.; Curtis, C.R. Effect of provider prompts on adolescent immunization rates: A randomized trial. Acad. Pediatr. 2015, 15, 149–157. [Google Scholar] [CrossRef]
- Tabana, H.; Dudley, L.D.; Knight, S.; Cameron, N.; Mahomed, H.; Goliath, C.; Eggers, R.; Wiysonge, C.S. The acceptability of three vaccine injections given to infants during a single clinic visit in South Africa. BMC Public Health 2016, 16, 749. [Google Scholar] [CrossRef]
- Thompson, E.L.; Garg, A.; Galvin, A.M.; Moore, J.D.; Kasting, M.L.; Wheldon, C.W. Correlates of HPV vaccination intentions among adults ages 27–45 years old in the U.S. J. Community Health 2021, 46, 893–902. [Google Scholar] [CrossRef]
- Todorova, I.; Alexandrova-Karamanova, A.; Panayotova, Y.; Dimitrova, E.; Kotzeva, T. Managing uncertainty: Healthcare professionals’ meanings regarding the HPV vaccine. Int. J. Behav. Med. 2014, 21, 29–36. [Google Scholar] [CrossRef]
- Townsend, J.S.; Puckett, M.; Gelb, C.A.; Whiteside, M.; Thorsness, J.; Stewart, S.L. Improving knowledge and awareness of Human Papillomavirus-associated gynecologic cancers: Results from the National Comprehensive Cancer Control Program/Inside Knowledge Collaboration. J. Womens Health 2018, 27, 955–964. [Google Scholar] [CrossRef]
- Usami, T.; Hashiguchi, M.; Kouhara, T.; Ishii, A.; Nagata, T.; Mochizuki, M. Impact of community pharmacists advocating immunization on influenza vaccination rates among the elderly. Yakugaku Zasshi 2009, 129, 1063–1068. [Google Scholar] [CrossRef]
- Villaverde Piñeiro, L.; Cachafeiro Pin, A.I.; Tajes González, Y.M.; Neira Blanco, P.; Arias Fernández, L.; Vázquez López, M.; Blanco Hortas, A.; Castro Rubiños, C.; Aparici Bolufer, J.V. Impact of a pharmaceutical intervention on influenza vaccination in patients receiving treatment with biological medicines. Eur. J. Hosp. Pharm. 2024, 31, 36–39. [Google Scholar] [CrossRef]
- Vu, M.; Bednarczyk, R.A.; Escoffery, C.; Ta, D.; Huynh, V.N.; Berg, C.J.U.S. Vietnamese parents’ HPV vaccine decision-making for their adolescents: An exploration of practice-, provider-, and patient-level influences. J. Behav. Med. 2022, 45, 197–210. [Google Scholar] [CrossRef]
- Warner, E.L.; Vaca Lopez, P.L.; Kepka, D.; Mann, K.; Kaddas, H.K.; Fair, D.; Fluchel, M.; Knackstedt, E.D.; Pannier, S.T.; Martel, L.; et al. Influence of provider recommendations to restart vaccines after childhood cancer on caregiver intention to vaccinate. J. Cancer Surviv. 2020, 14, 757–767. [Google Scholar] [CrossRef]
- Wedel, S.; Navarrete, R.; Burkard, J.F.; Clark, M.J. Improving Human Papillomavirus Vaccinations in military women. Mil. Med. 2016, 181, 1224–1227. [Google Scholar] [CrossRef][Green Version]
- Werk, L.N.; Diaz, M.C.; Cadilla, A.; Franciosi, J.P.; Hossain, M.J. Promoting adherence to influenza vaccination recommendations in pediatric practice. J. Prim. Care Community Health 2019, 10, 2150132719853061. [Google Scholar] [CrossRef]
- Whelan, N.W.; Steenbeek, A.; Martin-Misener, R.; Scott, J.; Smith, B.; D’Angelo-Scott, H. Engaging parents and schools improves uptake of the human papillomavirus (HPV) vaccine: Examining the role of the public health nurse. Vaccine 2014, 32, 4665–4671. [Google Scholar] [CrossRef]
- Wijesundara, J.G.; Ito Fukunaga, M.; Ogarek, J.; Barton, B.; Fisher, L.; Preusse, P.; Sundaresan, D.; Garber, L.; Mazor, K.M.; Cutrona, S.L. Electronic health record portal messages and interactive voice response calls to improve rates of early season influenza vaccination: Randomized controlled trial. J. Med. Internet Res. 2020, 22, e16373. [Google Scholar] [CrossRef]
- Williams, S.E.; Adams, L.E.; Sommer, E.C. Improving vaccination for young children (IVY): A stepped-wedge cluster randomized trial. Acad. Pediatr. 2021, 21, 1151–1160. [Google Scholar] [CrossRef]
- Wolynn, T.; Hermann, C.; Hoffman, B.L. Social media and vaccine hesitancy help us move the needle. Pediatr. Clin. N. Am. 2023, 70, 329–341. [Google Scholar] [CrossRef]
- Wong, V.W.Y.; Fong, D.Y.T.; Lok, K.Y.W.; Wong, J.Y.H.; Sing, C.; Choi, A.Y.-Y.; Yuen, C.Y.S.; Tarrant, M. Brief education to promote maternal influenza vaccine uptake: A randomized controlled trial. Vaccine 2016, 34, 5243–5250. [Google Scholar] [CrossRef]
- Wright, W.L.; Bruns, D.P.; Feeney, A.S.; Strowman, S.R. Improving vaccination rates in older adults: A quality improvement project. Nurse Pract. 2019, 44, 40–49. [Google Scholar] [CrossRef]
- Zacharias, T.; Wang, W.; Dao, D.; Wojciechowski, H.; Lee, W.M.; Do, S.; Singal, A.G. HBV outreach programs significantly increase knowledge and vaccination rates among Asian Pacific Islanders. J. Community Health 2015, 40, 619–624. [Google Scholar] [CrossRef]
- Zhang, C.; Greengold, J.; Tackett, S.; Lentz, C.; Bennett, W.; McGuire, M. Evaluation of online educational curriculum on HPV vaccination practices among adult primary care providers. BMC Med. Educ. 2023, 23, 923. [Google Scholar] [CrossRef] [PubMed]
- Zimet, G.; Dixon, B.E.; Xiao, S.; Tu, W.; Kulkarni, A.; Dugan, T.; Sheley, M.; Downs, S.M. Simple and elaborated clinician reminder prompts for Human Papillomavirus Vaccination: A randomized clinical trial. Acad. Pediatr. 2018, 18, S66–S71. [Google Scholar] [CrossRef]
- Zimmerman, R.K.; Brown, A.E.; Pavlik, V.N.; Moehling, K.K.; Raviotta, J.M.; Lin, C.J.; Zhang, S.; Hawk, M.; Kyle, S.; Patel, S.; et al. Using the 4 pillars practice transformation program to increase pneumococcal immunizations for older adults: A cluster-randomized trial. J. Am. Geriatr. Soc. 2017, 65, 114–122. [Google Scholar] [CrossRef]
- Fallucca, A.; Ferro, P.; Mazzeo, L.; Zagra, L.; Cocciola, E.; Oliveri, R.; Tuttolomondo, A.; Benfante, A.; Battaglia, S.; Scichilone, N.; et al. Impact of actively offering influenza vaccination to frail people during hospitalisation: A pilot study in Italy. Vaccines 2023, 11, 1829. [Google Scholar] [CrossRef] [PubMed]
- Betsch, C.; Schmid, P.; Heinemeier, D.; Korn, L.; Holtmann, C.; Böhm, R. Beyond confidence: Development of a measure assessing the 5C psychological antecedents of vaccination. PLoS ONE 2018, 13, e0208601. [Google Scholar] [CrossRef] [PubMed]
- Janz, N.K.; Becker, M.H. The Health Belief Model: A decade later. Health Educ. Behav. 1984, 11, 1–47. [Google Scholar] [CrossRef]
- McKee, C.; Bohannon, K. Exploring the reasons behind parental refusal of vaccines. J. Pediatr. Pharmacol. Ther. 2016, 21, 104–109. [Google Scholar] [CrossRef]
- O’Leary, S.T.; Opel, D.J.; Cataldi, J.R.; Hackell, J.M.; Committee on Infectious Diseases; Committee on Practice and Ambulatory Medicine; Committee on Bioethics. Strategies for improving vaccine communication and uptake. Pediatrics 2024, 153, e2023065483. [Google Scholar] [CrossRef]
- Health Resources and Services Administration National Center for Health Workforce Analysis. State of the Primary Care Workforce. 2024. Available online: https://bhw.hrsa.gov/sites/default/files/bureau-health-workforce/state-of-the-primary-care-workforce-report-2024.pdf (accessed on 13 September 2025).
- Lawson, E. The global primary care crisis. Br. J. Gen. Pract. 2023, 73, 3. [Google Scholar] [CrossRef]
- Valliant, S.N.; Burbage, S.C.; Pathak, S.; Urick, B.Y. Pharmacists as accessible health care providers: Quantifying the opportunity. J. Manag. Care Spec. Pharm. 2022, 28, 85–90. [Google Scholar] [CrossRef]
- Liu, B.; Zhang, X.; Lai, Y.; Sun, T.; Wang, C.; Zhao, T.; Zhang, S.; Shi, B.; Li, Y.; Cui, F. Global vaccine confidence trends among adults above and below age 65. NPJ Vaccines 2025, 10, 160. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Ten Threats to Global Health in 2019. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 16 May 2021).
- Matas, J.L.; Landry, L.G.; Lee, L.; Hansel, S.; Coudray, M.S.; Mata-McMurry, L.V.; Chalasani, N.; Xu, L.; Stair, T.; Edwards, C.; et al. Demographic determinants and geographical variability of COVID-19 vaccine hesitancy in underserved communities: Cross-sectional study. JMIR Public Health Surveill. 2023, 9, e34163. [Google Scholar] [CrossRef]
- Soorapanth, S.; Cheung, R.; Zhang, X.; Mokdad, A.H.; Mensah, G.A. Rural-urban differences in vaccination and hesitancy rates and trust: US COVID-19 trends and impact survey on a social media platform, May 2021–April 2022. Am. J. Public Health 2023, 113, 680–688. [Google Scholar] [CrossRef] [PubMed]
- Welch, V.L.; Metcalf, T.; Macey, R.; Markus, K.; Sears, A.J.; Enstone, A.; Langer, J.; Srivastava, A.; Cane, A.; Wiemken, T.L. Understanding the barriers and attitudes toward influenza vaccine uptake in the adult general population: A rapid review. Vaccines 2023, 11, 180. [Google Scholar] [CrossRef] [PubMed]
- Adjei Boakye, E.; Nair, M.; Abouelella, D.K.; Joseph, C.L.M.; Gerend, M.A.; Subramaniam, D.S.; Osazuwa-Peters, N. Trends in reasons for Human Papillomavirus Vaccine hesitancy: 2010–2020. Pediatrics 2023, 151, e2022060410. [Google Scholar] [CrossRef]
- Gatwood, J.; McKnight, M.; Frederick, K.; Hohmeier, K.; Kapan, S.; Chiu, C.-Y.; Renfro, C.; Hagemann, T. Extent of and reasons for vaccine hesitancy in adults at high-risk for pneumococcal disease. Am. J. Health Promot. 2021, 35, 908–916. [Google Scholar] [CrossRef]

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).