
Use of the PRECEDE-PROCEED Model in Piloting Vaccine Promotion and Infection Self-Protection: Intervention Development and Effectiveness Examination

 ,
,  , , ,
, , ,  ,
,  ,
,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Study Design
2.2. Part I: Development of the Intervention Package
2.3. Part II: Implementation and Evaluation of the Intervention Package
2.3.1. Study Subjects and Sample Size Calculation
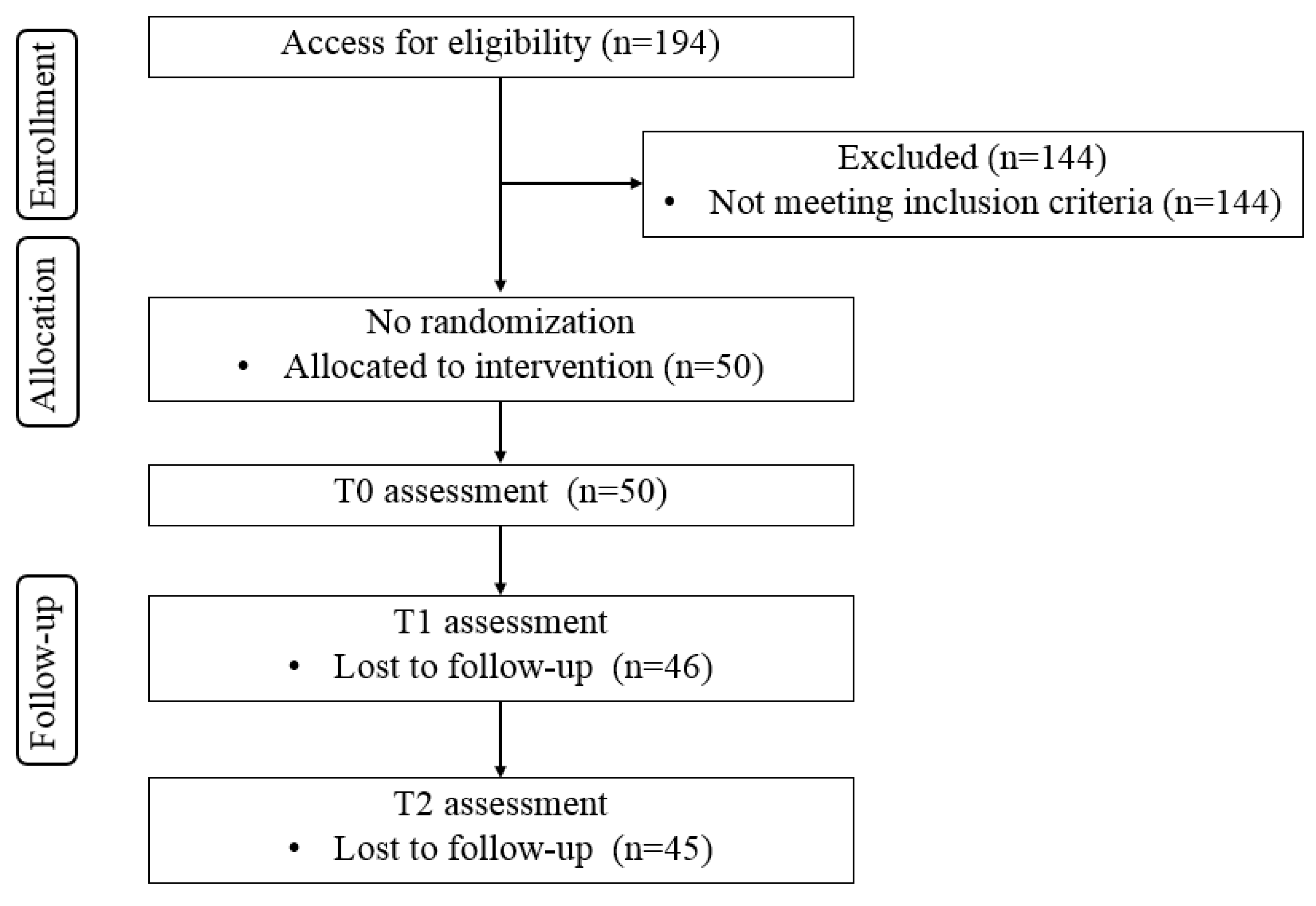
2.3.2. Recruitment
2.3.3. Intervention Implementation
2.3.4. Outcome Measures
2.3.5. Statistical Analysis
3. Results
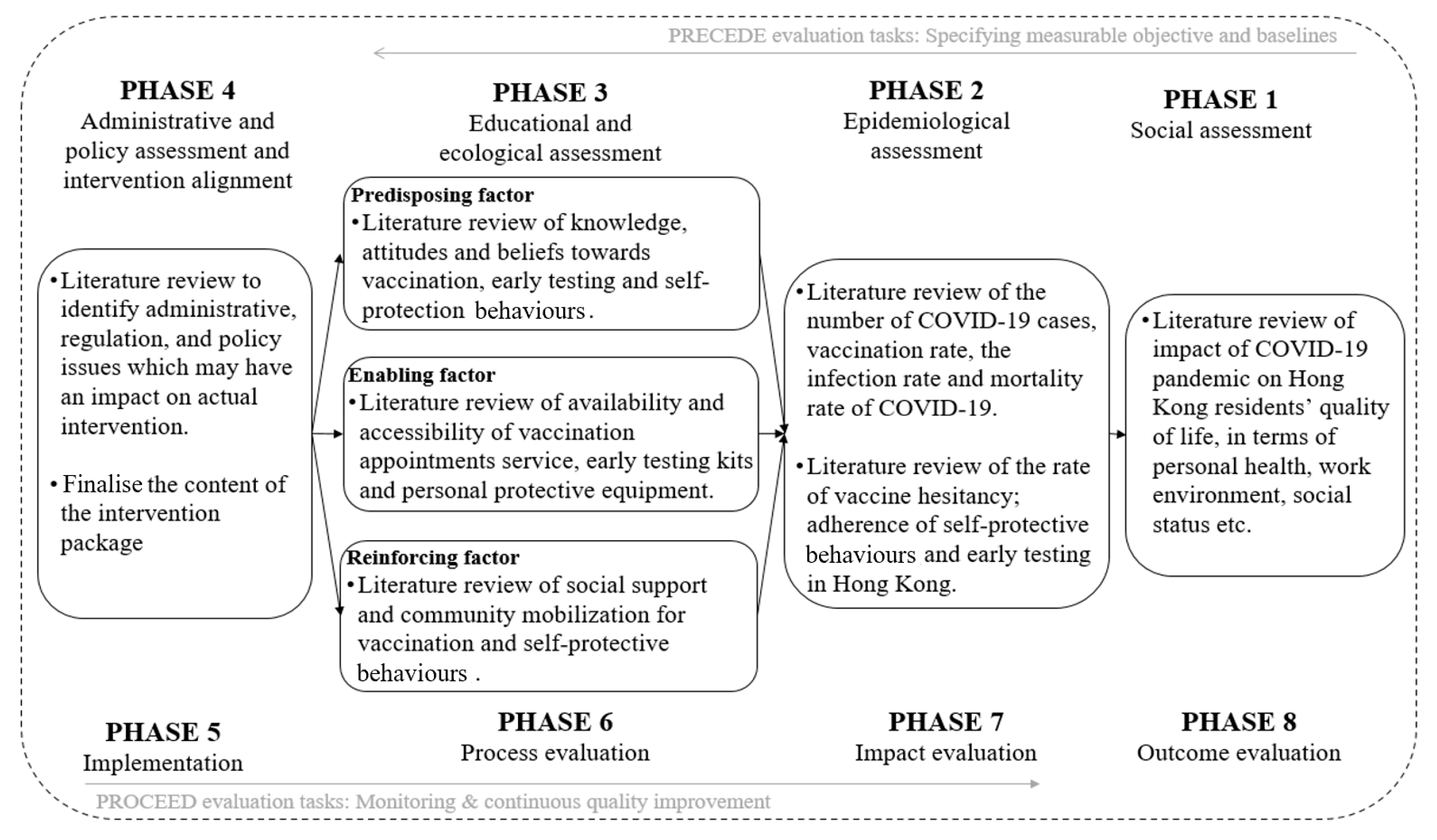
3.1. Assessment Results Based on Phases 1–4 of the PRECEDE-PROCEED Model
3.2. Structure and Contents of the Intervention Package
3.3. Effectiveness of the Intervention Package on Vaccination Promotion and Self-Protective Behaviors
3.3.1. Baseline Characteristics of the Participants
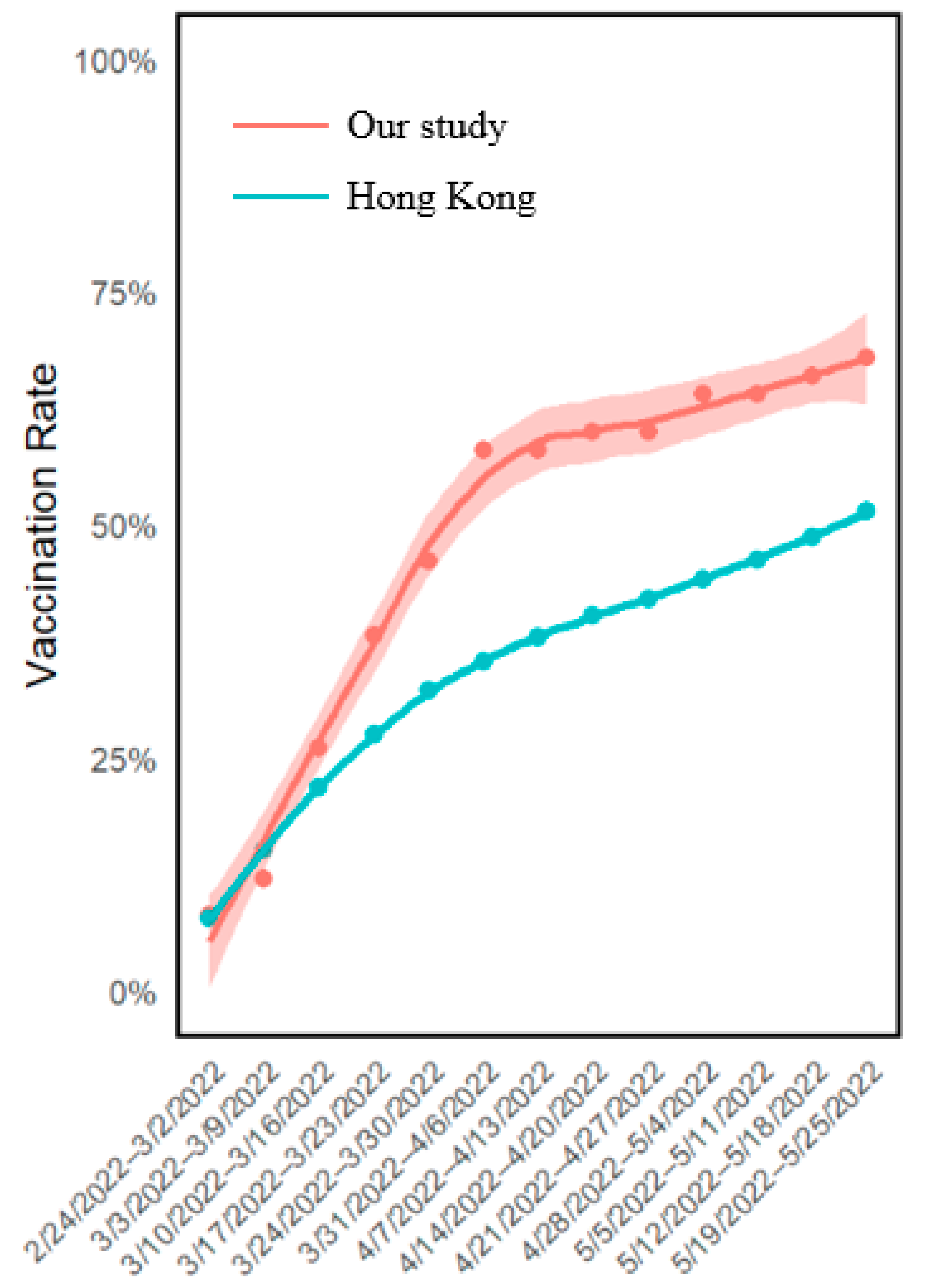
3.3.2. Vaccination Rate after Intervention
3.3.3. Early Testing and Self-Protection Behavior
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Muturi, N. The Influence of Information Source on COVID-19 Vaccine Efficacy and Motivation for Self-Protective Behavior. J. Health Commun. 2022, 27, 241–249. [Google Scholar] [CrossRef]
- Fang, F.; Chen, S.; Geng, X.; Kiprop, E. Survey on public awareness, attitudes and self-protective behavior adoption in different periods of COVID-19. Front. Public Health 2022, 10, 1063384. [Google Scholar] [CrossRef]
- Ezati Rad, R.; Mohseni, S.; Kamalzadeh Takhti, H.; Azad, M.H.; Shahabi, N.; Aghamolaei, T.; Norozian, F. Application of the protection motivation theory for predicting COVID-19 preventive behaviors in Hormozgan, Iran: A cross-sectional study. BMC Public Health 2021, 21, 466. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Rolling Updates on Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 21 September 2023).
- World Health Organization (WHO). Advice for the Public: Coronavirus Disease (COVID-19). Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/advice-for-public (accessed on 22 May 2024).
- Bo, Y.; Guo, C.; Lin, C.; Zeng, Y.; Li, H.B.; Zhang, Y.; Hossain, S.; Chan, J.W.; Yeung, D.W.; Kwok, K.O.; et al. Effectiveness of non-pharmaceutical interventions on COVID-19 transmission in 190 countries from 23 January to 13 April 2020. Int. J. Infect. Dis. 2021, 102, 247–253. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Wyka, K.; White, T.M.; Picchio, C.A.; Gostin, L.O.; Larson, H.J.; Rabin, K.; Ratzan, S.C.; Kamarulzaman, A.; El-Mohandes, A. A survey of COVID-19 vaccine acceptance across 23 countries in 2022. Nat. Med. 2023, 29, 366–375. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; Wong, E.L.; Ho, K.F.; Cheung, A.W.-L.; Yau, P.S.-Y.; Dong, D.; Wong, S.Y.-S.; Yeoh, E.-K. Change of Willingness to Accept COVID-19 Vaccine and Reasons of Vaccine Hesitancy of Working People at Different Waves of Local Epidemic in Hong Kong, China: Repeated Cross-Sectional Surveys. Vaccines 2021, 9, 62. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.M.; Vostok, J.; Johnson, H.; Burns, M.; Gharpure, R.; Sami, S.; Sabo, R.T.; Foreman, A.; Schubert, P.L.; Gallagher, G.R.; et al. Outbreak of SARS-CoV-2 Infections, Including COVID-19 Vaccine Breakthrough Infections, Associated with Large Public Gatherings—Barnstable County, Massachusetts, July 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1059–1062. [Google Scholar] [CrossRef] [PubMed]
- Kaim, A.; Jaffe, E.; Siman-Tov, M.; Khairish, E.; Adini, B. Impact of a Brief Educational Intervention on Knowledge, Perceived Knowledge, Perceived Safety, and Resilience of the Public During COVID-19 Crisis. Int. J. Environ. Res. Public Health 2020, 17, 5971. [Google Scholar] [CrossRef] [PubMed]
- Sayed, S.H.; Al-Mohaithef, M.; Elgzar, W.T. Effect of Digital-Based Self-Learned Educational Intervention about COVID-19 Using Protection Motivation Theory on Non-Health Students’ Knowledge and Self-Protective Behaviors at Saudi Electronic University. Int. J. Environ. Res. Public Health 2022, 19, 14626. [Google Scholar] [CrossRef]
- Tramm, R.; McCarthy, A.; Yates, P. Using the Precede-Proceed Model of Health Program Planning in breast cancer nursing research. J. Adv. Nurs. 2012, 68, 1870–1880. [Google Scholar] [CrossRef]
- Kim, J.; Jang, J.; Kim, B.; Lee, K.H. Effect of the PRECEDE-PROCEED model on health programs: A systematic review and meta-analysis. Syst. Rev. 2022, 11, 213. [Google Scholar] [CrossRef] [PubMed]
- Saulle, R.; Sinopoli, A.; De Paula Baer, A.; Mannocci, A.; Marino, M.; de Belvis, A.G.; Federici, A.; La Torre, G. The PRECEDE-PROCEED model as a tool in Public Health screening: A systematic review. Clin. Ter. 2020, 171, e167–e177. [Google Scholar] [CrossRef] [PubMed]
- Handyside, L.; Warren, R.; Devine, S.; Drovandi, A. Utilisation of the PRECEDE-PROCEED model in community pharmacy for health needs assessment: A narrative review. Res. Soc. Adm. Pharm. 2021, 17, 292–299. [Google Scholar] [CrossRef]
- Bammann, K.; Recke, C.; Albrecht, B.M.; Stalling, I.; Doerwald, F. Promoting Physical Activity Among Older Adults Using Community-Based Participatory Research With an Adapted PRECEDE-PROCEED Model Approach: The AEQUIPA/OUTDOOR ACTIVE Project. Am. J. Health Promot. 2021, 35, 409–420. [Google Scholar] [CrossRef]
- Green, L.; Kreuter, M. Health Program Planning: An Educational and Ecological Approach; McGraw-Hill Education: New York, NY, USA, 2005. [Google Scholar]
- Kan, W.; Yang, R.; Tang, M. Application research of chronic disease health management in an urban community based on the PRECEDE-PROCEED model in the long-term management of diabetes mellitus. Am. J. Transl. Res. 2021, 13, 8142–8149. [Google Scholar]
- Bahadori, F.; Ghofranipour, F.; Zarei, F.; Ziaei, R.; Ghaffarifar, S. Application of the PRECEDE -PROCEED model in prevention of brucellosis focused on livestock vaccination process. BMC Vet. Res. 2021, 17, 384. [Google Scholar] [CrossRef]
- Lake, P.; Kasting, M.L.; Malo, T.; Giuliano, A.R.; Vadaparampil, S.T. An environmental scan to examine stakeholder perspectives on human papillomavirus vaccination: A mixed methods study. Vaccine 2019, 37, 187–194. [Google Scholar] [CrossRef]
- Vamos, C.A.; Kline, N.; Vázquez-Otero, C.; Lockhart, E.A.; Lake, P.W.; Wells, K.J.; Proctor, S.; Meade, C.D.; Daley, E.M. Stakeholders’ perspectives on system-level barriers to and facilitators of HPV vaccination among Hispanic migrant farmworkers. Ethn. Health 2022, 27, 1442–1464. [Google Scholar] [CrossRef]
- Vamos, C.A.; Vázquez-Otero, C.; Kline, N.; Lockhart, E.A.; Wells, K.J.; Proctor, S.; Meade, C.D.; Daley, E.M. Multi-level determinants to HPV vaccination among Hispanic farmworker families in Florida. Ethn. Health 2021, 26, 319–336. [Google Scholar] [CrossRef] [PubMed]
- Zimmerman, R.K.; Nowalk, M.P.; Bardella, I.J.; Fine, M.J.; Janosky, J.E.; Santibanez, T.A.; Wilson, S.A.; Raymund, M. Physician and practice factors related to influenza vaccination among the elderly. Am. J. Prev. Med. 2004, 26, 1–10. [Google Scholar] [CrossRef]
- Choi, E.P.H.; Hui, B.P.H.; Wan, E.Y.F.; Kwok, J.Y.Y.; Tam, T.H.L.; Wu, C. COVID-19 and Health-Related Quality of Life: A Community-Based Online Survey in Hong Kong. Int. J. Environ. Res. Public Health 2021, 18, 3228. [Google Scholar] [CrossRef]
- Xiao, J.; Cheung, J.K.; Wu, P.; Ni, M.Y.; Cowling, B.J.; Liao, Q. Temporal changes in factors associated with COVID-19 vaccine hesitancy and uptake among adults in Hong Kong: Serial cross-sectional surveys. Lancet Reg. Health West. Pac. 2022, 23, 100441. [Google Scholar] [CrossRef] [PubMed]
- Yang, B.; Lin, Y.; Xiong, W.; Liu, C.; Gao, H.; Ho, F.; Zhou, J.; Zhang, R.; Wong, J.Y.; Cheung, J.K.; et al. Comparison of control and transmission of COVID-19 across epidemic waves in Hong Kong: An observational study. Lancet Reg. Health West. Pac. 2024, 43, 100969. [Google Scholar] [CrossRef] [PubMed]
- Tam, V.C.W.; Tam, S.Y.; Khaw, M.L.; Law, H.K.W.; Chan, C.P.L.; Lee, S.W.Y. Behavioural insights and attitudes on community masking during the initial spread of COVID-19 in Hong Kong. Hong Kong Med. J. 2021, 27, 106–112. [Google Scholar] [CrossRef]
- Wong, E.L.; Qiu, H.; Wang, K.; Sun, K.-S.; Yam, C.H.-K.; Cheung, A.W.-L.; Yeoh, E.-K. Screening Hesitancy of a Universal Voluntary-based Rapid Antigen Test for coronavirus disease 2019 (COVID-19) During Omicron Wave in Hong Kong. J. Infect. Public Health 2023, 16, 1306–1312. [Google Scholar] [CrossRef]
- Molassiotis, A.; Xie, Y.J.; Leung, A.Y.M.; Ho, G.W.K.; Li, Y.; Leung, P.H.-M.; Wang, H.L.; Chen, C.X.R.; Tong, D.W.K.; Siu, J.Y.-M.; et al. A Community-Based Participatory Research Approach to Developing and Testing Social and Behavioural Interventions to Reduce the Spread of SARS-CoV-2: A Protocol for the ‘COPAR for COVID’ Programme of Research with Five Interconnected Studies in the Hong Kong Context. Int. J. Environ. Res. Public Health 2022, 19, 13392. [Google Scholar] [CrossRef]
- Perkins, J.R.; Jaqua, E.E.; Nguyen, V.T.; Franz, D.A.; Elkins, J.; Morton, K.R. Optimizing Education to Improve COVID-19 Vaccination Rates in a Federally Qualified Health Center. Perm. J. 2023, 27, 143–150. [Google Scholar] [CrossRef] [PubMed]
- Centre for Health Protection TGotHKSAR. Proper Hand Hygiene. Available online: https://www.chp.gov.hk/en/healthtopics/content/460/19728.html (accessed on 21 September 2023).
- Centre for Health Protection TGotHKSAR. Proper Use of Mask. Available online: https://www.chp.gov.hk/en/healthtopics/content/460/19731.html (accessed on 21 September 2023).
- Centre for Health Protection TGotHKSAR. How Many Doses of COVID-19 Vaccine Are Recommended for Me. Available online: https://www.chp.gov.hk/en/features/106951.html (accessed on 21 September 2023).
- Data.gov.hk. Daily Count of Vaccination by Age Groups. Available online: https://data.gov.hk/en-data/dataset/hk-hhb-hhbcovid19-vaccination-rates-over-time-by-age (accessed on 21 September 2023).
- Census and Statistics Department TGotHKSAR. Population by Sex and Age Group. Available online: https://www.censtatd.gov.hk/en/web_table.html?id=110-01001 (accessed on 21 September 2023).
- Hung, M.S.Y.; Lam, S.K.K.; Chan, L.C.K.; Liu, S.P.S.; Chow, M.C.M. The Psychological and Quality of Life Impacts on Women in Hong Kong during the COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 6734. [Google Scholar] [CrossRef] [PubMed]
- Yan, E.; Lai, D.W.L.; Lee, V.W.P.; Ng, H.K.L. Predicting Public Adherence to COVID-19 Preventive Measures: A Cross-Sectional Study in Hong Kong. Int. J. Environ. Res. Public Health 2021, 18, 12403. [Google Scholar] [CrossRef]
- Cowling, B.J.; Ali, S.T.; Ng, T.W.Y.; Tsang, T.K.; Li, J.C.M.; Fong, M.W.; Liao, Q.; Kwan, M.Y.; Lee, S.L.; Chiu, S.S.; et al. Impact assessment of non-pharmaceutical interventions against coronavirus disease 2019 and influenza in Hong Kong: An observational study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Chan, E.Y.Y.; Huang, Z.; Lo, E.S.K.; Hung, K.K.C.; Wong, E.L.Y.; Wong, S.Y.S. Sociodemographic Predictors of Health Risk Perception, Attitude and Behavior Practices Associated with Health-Emergency Disaster Risk Management for Biological Hazards: The Case of COVID-19 Pandemic in Hong Kong, SAR China. Int. J. Environ. Res. Public Health 2020, 17, 3869. [Google Scholar] [CrossRef]
- Hsing, J.C.; Ma, J.; Barrero-Castillero, A.; Jani, S.G.; Pulendran, U.P.; Lin, B.-J.; Thomas-Uribe, M.; Wang, C.J. Influence of Health Beliefs on Adherence to COVID-19 Preventative Practices: International, Social Media-Based Survey Study. J. Med. Internet Res. 2021, 23, e23720. [Google Scholar] [CrossRef] [PubMed]
- Chan, E.Y.Y.; Kim, J.H.; Kwok, K.O.; Huang, Z.; Hung, K.K.C.; Wong, E.L.Y.; Lee, E.K.P.; Wong, S.Y.S. Population Adherence to Infection Control Behaviors during Hong Kong’s First and Third COVID-19 Waves: A Serial Cross-Sectional Study. Int. J. Environ. Res. Public Health 2021, 18, 11176. [Google Scholar] [CrossRef] [PubMed]
- Kwan, W.M.; Mok, C.K.; Kwok, Y.T.; Lam, H.-W.; Chan, K.-H.; Law, T.-H.S.; Leung, P.-M.; Mak, M.-Y.; Que, T.-L.; Tang, Y.-H. Bundled interventions for consumption management and monitoring of personal protective equipment in COVID-19 pandemic in Hong Kong local hospitals. BMJ Open Qual. 2020, 9, e000990. [Google Scholar] [CrossRef] [PubMed]
- Health Promotion Branch Centre for Health Protection Department of Health. Risk Communication for COVID-19. Available online: https://icidportal.ha.org.hk/Home/File?path=/Training%20Calendar/161/Risk%20communication%20for%20COVID-19_preparation%20for%20the%20next%20battle.pdf (accessed on 2 July 2024).
- Wu, Y.; Yan, X.; Zhao, S.; Wang, J.; Ran, J.; Dong, D.; Wang, M.; Fung, H.; Yeoh, E.-K.; Chung, R.Y.-N. Association of time to diagnosis with socioeconomic position and geographical accessibility to healthcare among symptomatic COVID-19 patients: A retrospective study in Hong Kong. Health Place 2020, 66, 102465. [Google Scholar] [CrossRef]
- Zhang, X. Examining COVID-19 Vaccination Misinformation and Clarification by the Public Sector in Hong Kong: A Study of Cantonese COVID-19 Fake News Detection on Social Media. 2021. Available online: https://research.hkbu.edu.hk/f/page/20923/22993/Combating2022_HKGDebunk_HKBU_Xinzhi_Eng.pdf (accessed on 2 July 2024).
- Wang, Z.; Zhao, M.; Chen, Y.; Song, Y.; Lan, L. A Study of Cantonese COVID-19 Fake News Detection on Social Media. In Proceedings of the IEEE International Conference on Big Data 2021, Orlando, FL, USA, 15–18 December 2021. [Google Scholar] [CrossRef]
- Dermody, T.S.; DiMaio, D.; Enquist, L.W. Vaccine Safety, Efficacy, and Trust Take Time. Annu. Rev. Virol. 2021, 8, 3–4. [Google Scholar] [CrossRef]
- Drokow, E.K.; Effah, C.Y.; Agboyibor, C.; Sasu, E.; Amponsem-Boateng, C.; Akpabla, G.S.; Ahmed, H.A.W.; Sun, K. The Impact of Video-Based Educational Interventions on Cervical Cancer, Pap Smear and HPV Vaccines. Front. Public Health 2021, 9, 681319. [Google Scholar] [CrossRef]
- Xie, Y.J.; Liao, X.; Lin, M.; Cheung, K.; Zhang, Q.; Li, Y.; Hao, C.; Wang, H.H.; Gao, Y.; Zhang, D.D.; et al. Community Engagement in Vaccination Promotion: Systematic Review and Meta-Analysis. JMIR Public Health Surveill. 2024, 10, e49695. [Google Scholar] [CrossRef]
- Noar, S.M.; Palmgreen, P.; Chabot, M.; Dobransky, N.; Zimmerman, R.S. A 10-year systematic review of HIV/AIDS mass communication campaigns: Have we made progress? J. Health Commun. 2009, 14, 15–42. [Google Scholar] [CrossRef]
- Sachs, J.D.; Karim, S.S.A.; Aknin, L.; Allen, J.; Brosbøl, K.; Colombo, F.; Barron, G.C.; Espinosa, M.F.; Gaspar, V.; Gaviria, A.; et al. The Lancet Commission on lessons for the future from the COVID-19 pandemic. Lancet 2022, 400, 1224–1280. [Google Scholar] [CrossRef]
- Torres, C.; Ogbu-Nwobodo, L.; Alsan, M.; Stanford, F.C.; Banerjee, A.; Breza, E.; Chandrasekhar, A.G.; Eichmeyer, S.; Karnani, M.; Loisel, T.; et al. Effect of Physician-Delivered COVID-19 Public Health Messages and Messages Acknowledging Racial Inequity on Black and White Adults’ Knowledge, Beliefs, and Practices Related to COVID-19: A Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2117115. [Google Scholar] [CrossRef] [PubMed]
- Gao, H.; Du, Z.; Tsang, T.K.; Xiao, J.; Shan, S.; Liao, Q.; Wu, P.; Leung, G.M.; Cowling, B.J. Pandemic fatigue and attenuated impact of avoidance behaviours against COVID-19 transmission in Hong Kong by cross-sectional telephone surveys. BMJ Open 2021, 11, e055909. [Google Scholar] [CrossRef]
- Marquez, C.; Kerkhoff, A.D.; Naso, J.; Contreras, M.G.; Castellanos Diaz, E.; Rojas, S.; Peng, J.; Rubio, L.; Jones, D.; Jacobo, J.; et al. A multi-component, community-based strategy to facilitate COVID-19 vaccine uptake among Latinx populations: From theory to practice. PLoS ONE 2021, 16, e0257111. [Google Scholar] [CrossRef] [PubMed]
- Gielen, A.C.; McDonald, E.M.; Gary, T.L.; Bone, L.R. Using the precede-proceed model to apply health behavior theories. Health Behav. Health Educ. Theory Res. Pract. 2008, 4, 407–429. [Google Scholar]
- U.S. Department of Health and Human Services. Theory at a Glance: A Guide for Health Promotion Practice; Lulu Press: Morrisville, NC, USA, 2018.
- Crosby, R.; Noar, S.M. What is a planning model? An introduction to PRECEDE-PROCEED. J. Public Health Dent. 2011, 71 (Suppl. S1), S7–S15. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Time | Core Intervention Package | |||
|---|---|---|---|---|
| Strategies to Address Predisposing Factors | Strategies to Address Reinforcing Factors | Strategies to Address Enabling Factors | ||
| Week 1 | Health education video 1: Introduction to the project. Health education video 2: Etiology, symptoms, and transmission of COVID-19. Health education video 3: Epidemiology of COVID-19. | Health tips * Tips 1–3 | Individual consultant | Delivering anti-epidemic package |
| Week 2 | Health education video 4: Reasons for taking COVID-19 vaccines and two types of COVID-19. vaccines in Hong Kong. Health education video 5: Effectiveness and safety of Comirnaty and Sinovac. Health education video 6: Safety and side effects of COVID-19 vaccine. | Tips 4–6 | Reminder of vaccination | Vaccine booking service |
| Week 3 | Health education video 7: COVID-19 vaccination program in Hong Kong. Health education video 8: Vaccine hesitation. Health education video 9: Breaking vaccine prejudice. | Tips 7–9 | Individual consultant | |
| Week 4 | Health education video 10: Arrangement on COVID-19 vaccinations for persons who have recovered from previous COVID-19 infection. Health education video 11: Importance of early testing. Health education video 12: Arrangement for early testing. | Tips 10–12 | Reminder of vaccination | |
| Week 5 | Health education video 13: Self-protection behaviors. Health education video 14: How to perform handwashing properly. | Tips 13–15 | Individual consultant | |
| Week 6 | Health education video 15: How to wear masks properly. Health education video 16: QUIZ: test your COVID-19 knowledge. | Tips 16–18 | Reminder of vaccination | |
| Week 7–8 (Booster session) | Review health education videos 1–6 | Tips 19–24 | Individual consultant and Reminder of vaccination | |
| Week 9–10 (Booster session) | Review health education videos 7–12 | Tips 25–30 | Individual consultant and Reminder of vaccination | |
| Week 11–12 (Booster session) | Review health education videos 13–16 | Tips 31–36 | Individual consultant and Reminder of vaccination | Delivering anti-epidemic package |
| Variables a | All Participants (n = 50) | Participants with Comirnaty (n = 30) | Participants with Sinovac (n = 18) | p b |
|---|---|---|---|---|
| Sex | 0.614 | |||
| Male | 2 (4.0) | 1 (3.3) | 1 (5.6) | |
| Female | 48 (96.0) | 29 (96.7) | 17 (94.4) | |
| Age (years) | 57.1 (9.3) | 56.93 (9.34) | 58.11 (8.34) | 0.663 |
| <60 | 25 (50.0) | 15 (50.0) | 9 (50.0) | 0.617 |
| ≥60 | 25 (50.0) | 15 (50.0) | 9 (50.0) | |
| Chronic diseases | 0.762 | |||
| No | 19 (32.0) | 11 (36.7) | 8 (44.4) | |
| Yes | 31 (68.0) | 19 (63.3) | 10 (55.6) | |
| Smoking | 0.924 | |||
| Never | 43 (86.0) | 27 (90.0) | 16 (88.9) | |
| Ever smoking | 4 (8.0) | 1 (3.3) | 1 (5.6) | |
| Current smoking | 3 (6.0) | 2 (6.7) | 1 (5.6) | |
| Drinking | 0.592 | |||
| No | 29 (58.0) | 18 (60.0) | 11 (61.1) | |
| Yes | 21 (42.0) | 12 (40.0) | 7 (38.9) | |
| Exercise habit | 0.301 | |||
| No | 24 (48.0) | 13 (43.3) | 10 (55.6) | |
| Yes | 26 (52.0) | 17 (56.7) | 8 (44.4) | |
| Employment | 0.772 | |||
| Employed | 24 (48.0) | 15 (50.0) | 8 (44.4) | |
| Not employed/Retired | 26 (52.0) | 15 (50.0) | 10 (55.6) | |
| Occupation | 0.894 | |||
| Managers, administrative staff, and professionals | 5 (20.8) | 3 (20.0) | 1 (12.5) | |
| Clerk | 16 (66.7) | 10 (66.7) | 6 (75.0) | |
| Service workers, sales and others | 3 (12.5) | 2 (13.3) | 1 (12.5) | |
| Education | 0.744 | |||
| Primary or below | 3 (6.0) | 2 (6.7) | 1 (5.6) | |
| Secondary or matriculation | 28 (56.0) | 18 (60.0) | 9 (50.0) | |
| Tertiary or above | 19 (38.0) | 10 (33.3) | 8 (44.4) | |
| Marital status | 0.680 | |||
| Single | 12 (24.0) | 6 (20.0) | 5 (27.8) | |
| Married/Cohabiting | 30 (60.0) | 19 (63.3) | 10 (55.6) | |
| Divorced/Separated/Widowed | 8 (16.0) | 5 (16.7) | 3 (16.7) | |
| Living | 0.451 | |||
| With family | 42 (84.0) | 26 (86.7) | 14 (77.8) | |
| Alone | 8 (16.0) | 4 (13.3) | 4 (13.3) | |
| Residential area | 0.140 | |||
| Hong Kong Island | 7 (14.0) | 5 (16.7) | 2 (11.1) | |
| Kowloon | 16 (32.0) | 12 (40.0) | 3 (16.7) | |
| New Territories | 27 (54.0) | 13 (43.3) | 13 (72.2) | |
| Income (per month) | 0.453 | |||
| ≤10,000 HKD | 7 (14.0) | 4 (13.3) | 3 (16.7) | |
| 10,000–29,999 HKD | 14 (28.0) | 8 (26.7) | 5 (27.8) | |
| 30,000–49,999 HKD | 10 (20.0) | 8 (26.7) | 2 (11.1) | |
| ≥50,000 HKD | 6 (12.0) | 2 (6.7) | 4 (22.2) | |
| Prefer not to disclose | 13 (26.0) | 8 (26.7) | 4 (22.2) | |
| Ever taken influenza vaccine | 12 (24.0) | 5 (16.7) | 7 (38.9) | 0.101 |
| Took influenza vaccine in the past year | 8 (16.0) | 4 (13.3) | 4 (22.2) | 0.451 |
| Participants Receiving New Dose | Raw Vaccination Rate | Modified Vaccination Rate a | ||||
|---|---|---|---|---|---|---|
| n | Rate | 95% CI | Rate | 95% CI | ||
| 1.5th month (n = 46) | New vaccine (anyone) | 28 | 60.9% | 45.4–74.9% | 73.3% | 58.1–85.4% |
| New 3rd dose | 25 | 62.5% | 45.8–77.3% | 76.9% | 60.7–88.9% | |
| New 2nd dose | 3 | 75.0% | 19.4–99.4% | 75.0% | 19.4–99.4% | |
| 3rd month (n = 45) | New vaccine (anyone) | 33 | 73.3% | 58.1–85.4% | 94.3% | 80.8–99.3% |
| New 3rd dose | 30 | 76.9% | 60.7–88.9% | 93.8% | 79.2–99.2% | |
| New 2nd dose | 3 | 75.0% | 19.4–99.4% | 100.0% | 29.2–100.0% b | |
| Behavior | Baseline | 1.5 Months | p b | 3 Months | p b |
|---|---|---|---|---|---|
| Early testing—oneself | 59.2% (44.2–73.0%) | 78.3% (63.7–89.1%) | 0.018 * | 86.7% (73.2–95.0%) | 0.021 * |
| Early testing—family | 57.1% (42.2–71.2%) | 78.3% (63.7–89.1%) | 0.021 * | 84.4% (70.1–93.5%) | 0.004 ** |
| Hand washing | 9.1 (1.6) | 9.4 (1.3) | 0.088 | 9.5 (1.0) | 0.037 * |
| Mask wearing | 4.9 (1.3) | 5.2 (1.0) | 0.042 * | 5.3 (1.2) | 0.048 * |
| Social distancing | 7.6 (1.3) | 8.0 (1.1) | 0.017 * | 7.5 (1.1) | 0.901 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xie, Y.J.; Tian, L.; Deng, Y.; Yang, L.; Cheung, K.; Li, Y.; Wang, H.H.; Hao, C.; Siu, G.K.H.; Zhang, Q.; et al. Use of the PRECEDE-PROCEED Model in Piloting Vaccine Promotion and Infection Self-Protection: Intervention Development and Effectiveness Examination. Vaccines 2024, 12, 979. https://doi.org/10.3390/vaccines12090979
Xie YJ, Tian L, Deng Y, Yang L, Cheung K, Li Y, Wang HH, Hao C, Siu GKH, Zhang Q, et al. Use of the PRECEDE-PROCEED Model in Piloting Vaccine Promotion and Infection Self-Protection: Intervention Development and Effectiveness Examination. Vaccines. 2024; 12(9):979. https://doi.org/10.3390/vaccines12090979
Chicago/Turabian StyleXie, Yao Jie, Longben Tian, Yunyang Deng, Lin Yang, Kin Cheung, Yan Li, Harry Haoxiang Wang, Chun Hao, Gilman Kit Hang Siu, Qingpeng Zhang, and et al. 2024. "Use of the PRECEDE-PROCEED Model in Piloting Vaccine Promotion and Infection Self-Protection: Intervention Development and Effectiveness Examination" Vaccines 12, no. 9: 979. https://doi.org/10.3390/vaccines12090979
APA StyleXie, Y. J., Tian, L., Deng, Y., Yang, L., Cheung, K., Li, Y., Wang, H. H., Hao, C., Siu, G. K. H., Zhang, Q., Molassiotis, A., & Leung, A. Y. M. (2024). Use of the PRECEDE-PROCEED Model in Piloting Vaccine Promotion and Infection Self-Protection: Intervention Development and Effectiveness Examination. Vaccines, 12(9), 979. https://doi.org/10.3390/vaccines12090979