
Have Previous COVID-19 Vaccinations Shaped the Potential Enhancing Infection of Variant Strains?

 , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
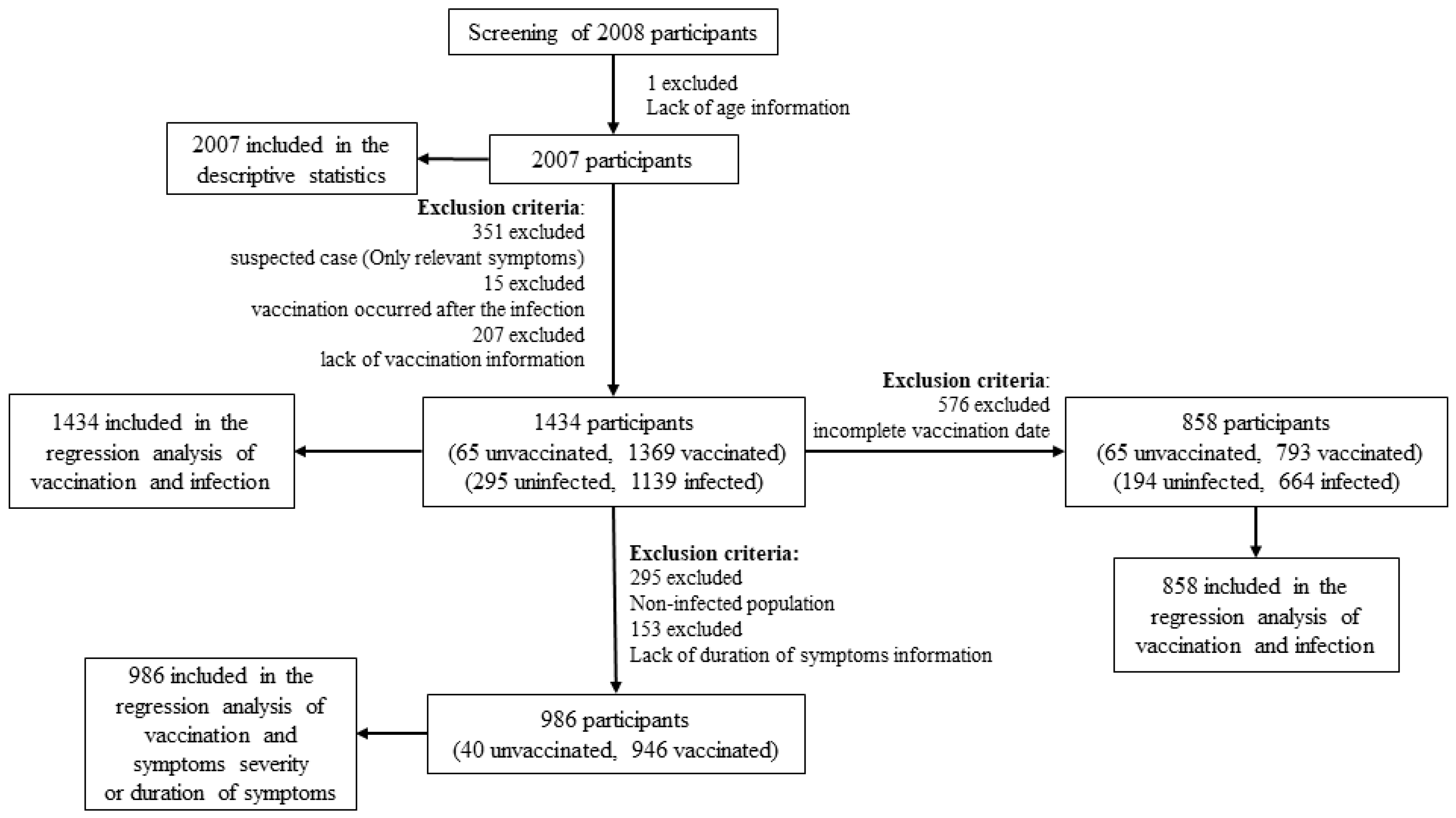
2.1. Study Design and Population
2.2. Questionnaires
2.3. Statistical Analysis
3. Results
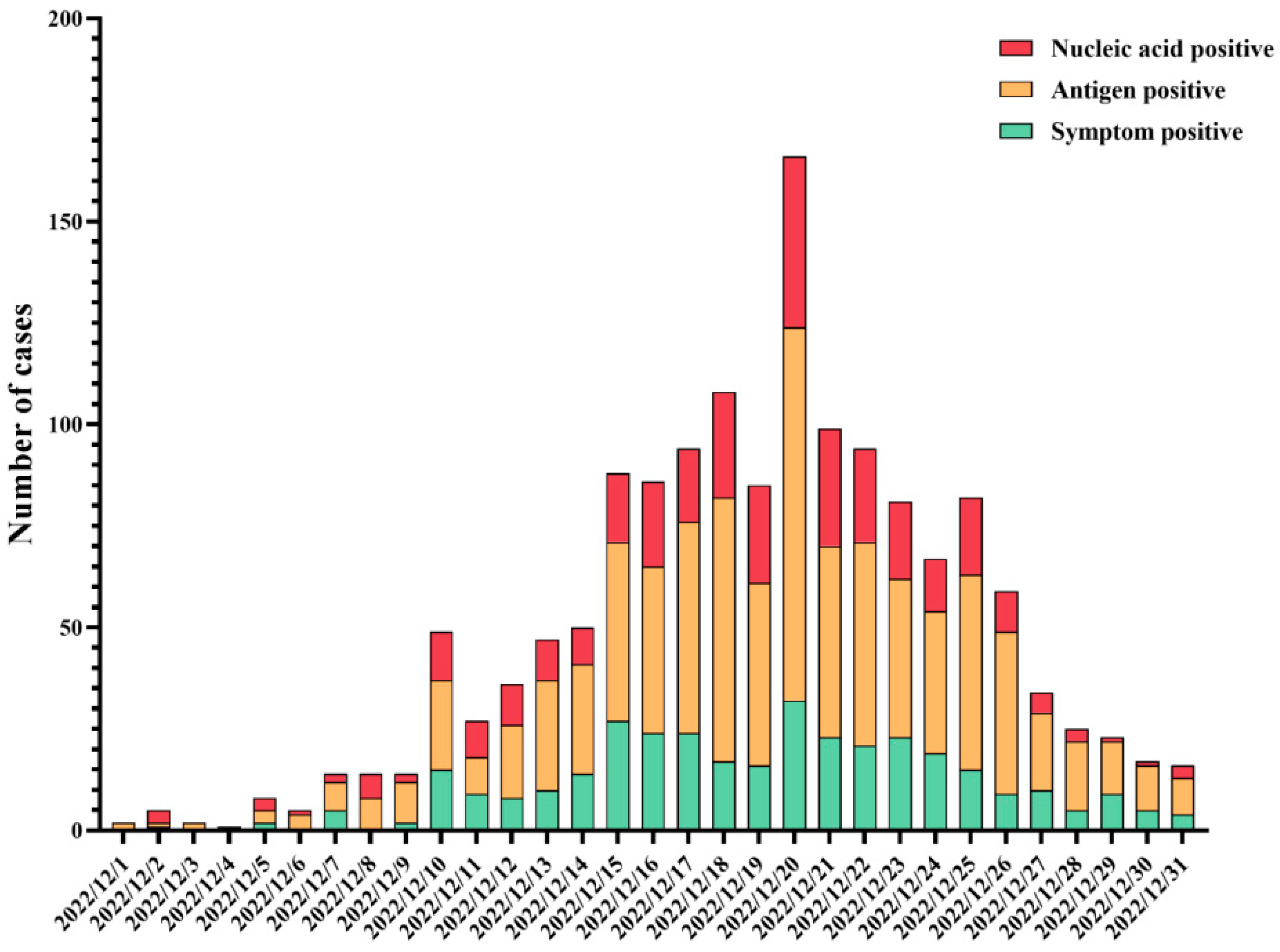
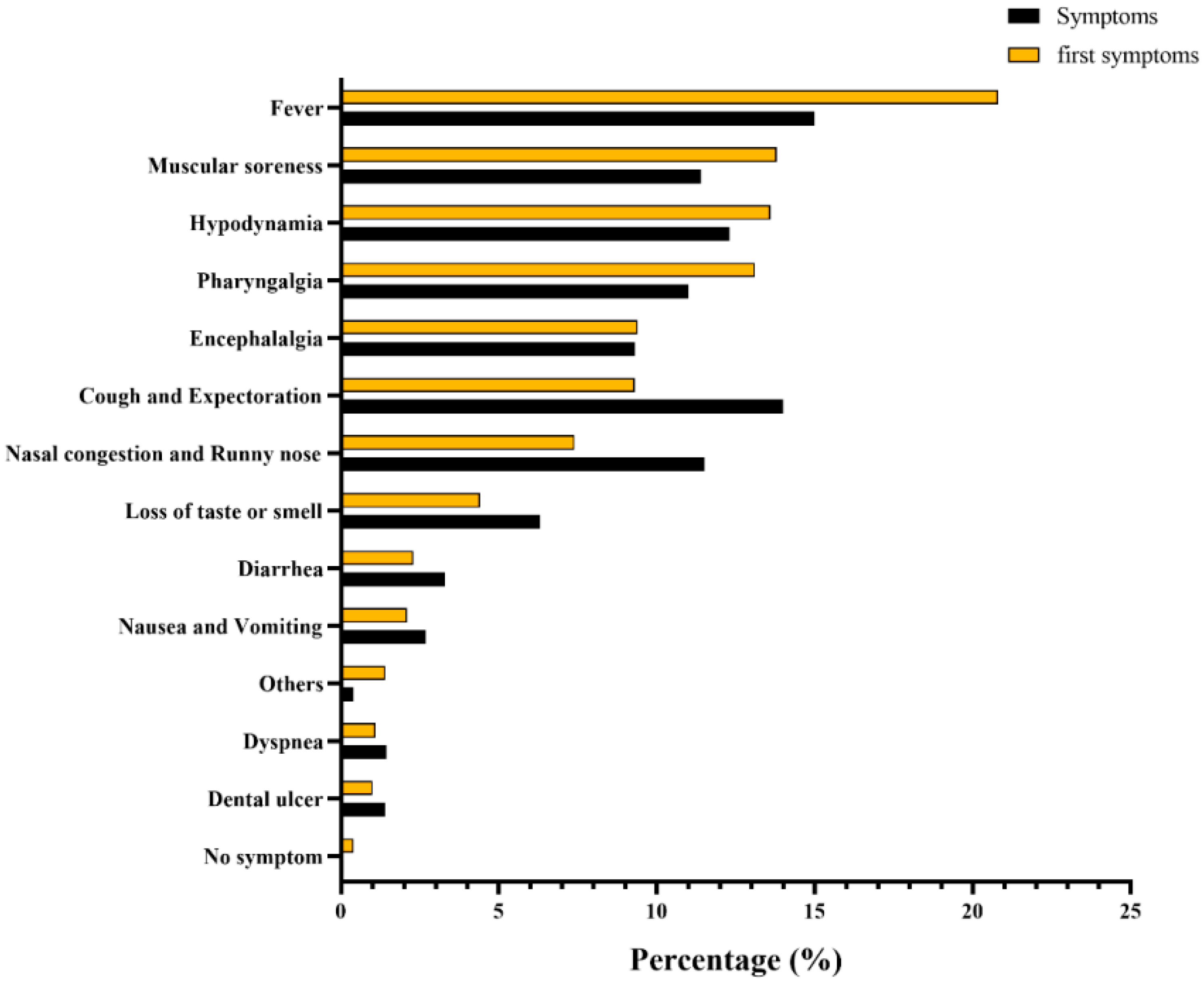
3.1. Descriptive Statistics for Infection with SARS-CoV-2
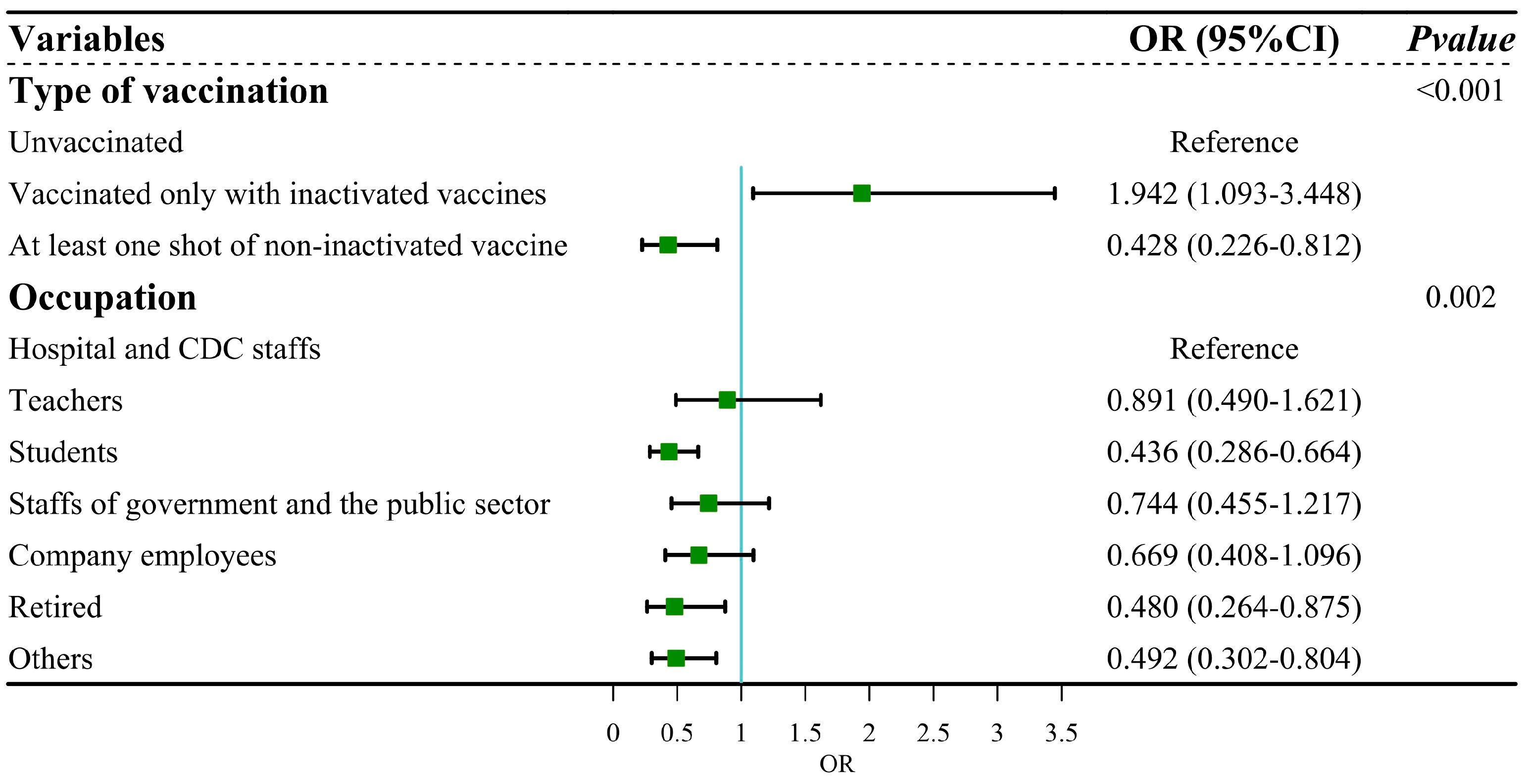
3.2. Binary Regression Analysis of COVID-19 Vaccination and Infection Outcomes
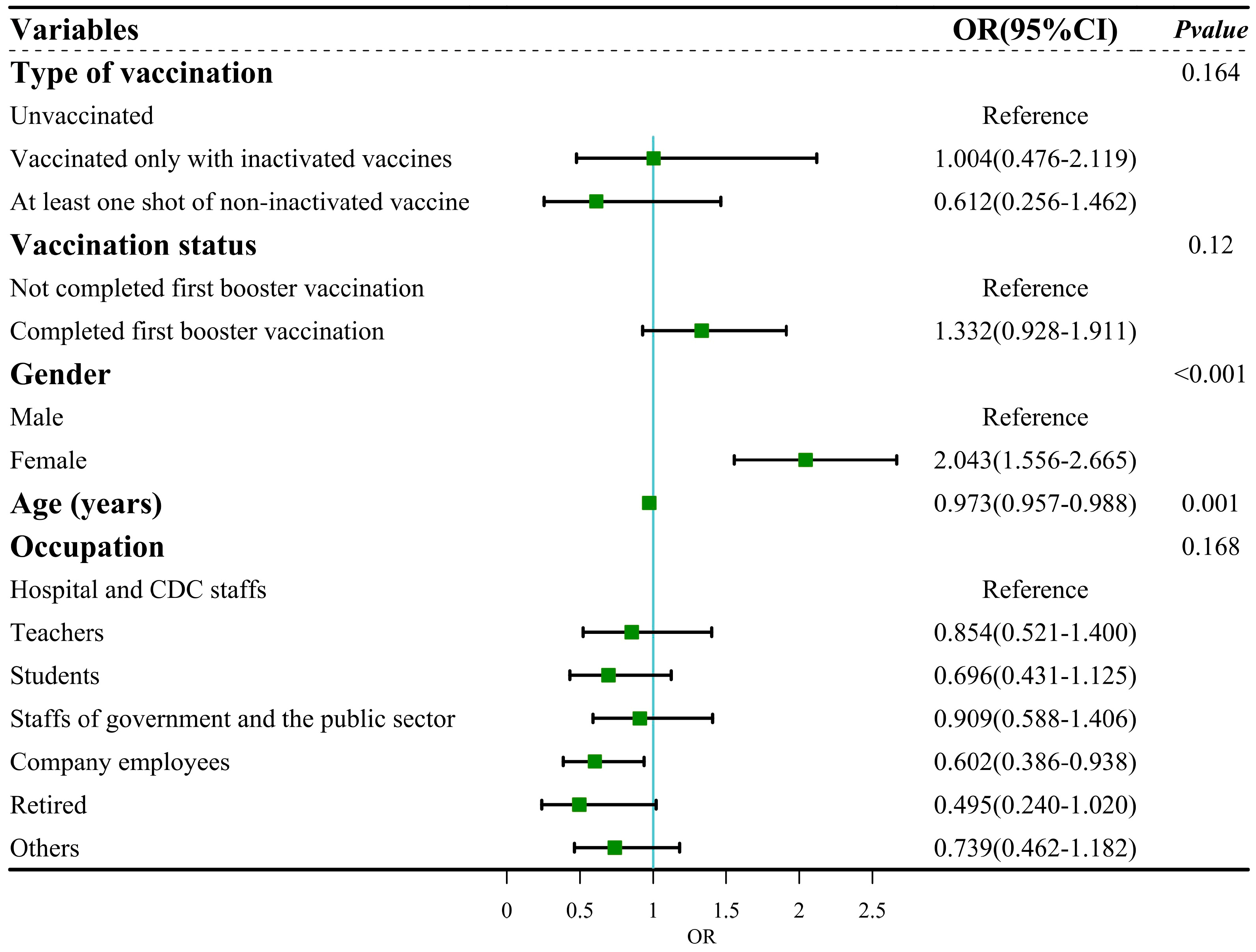
3.3. Regression Analysis of COVID-19 Vaccination and Symptom Severity or Duration of Symptoms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO. Statement on the Fifteenth Meeting of the IHR (2005) Emergency Committee on the COVID-19 Pandemic. Available online: https://www.who.int/news/item/05-05-2023-statement-on-the-fifteenth-meeting-of-the-international-health-regulations-(2005)-emergency-committee-regarding-the-coronavirus-disease-(covid-19)-pandemic (accessed on 4 December 2023).
- Halperin, S.A.; Ye, L.; MacKinnon-Cameron, D.; Smith, B.; Cahn, P.E.; Ruiz-Palacios, G.M.; Ikram, A.; Lanas, F.; Lourdes Guerrero, M.; Muñoz Navarro, S.R.; et al. Final Efficacy Analysis, Interim Safety Analysis, and Immunogenicity of a Single Dose of Recombinant Novel Coronavirus Vaccine (Adenovirus Type 5 Vector) in Adults 18 Years and Older: An International, Multicentre, Randomised, Double-Blinded, Placebo-Controlled Phase 3 Trial. Lancet 2022, 399, 237–248. [Google Scholar] [CrossRef] [PubMed]
- Dai, L.; Gao, L.; Tao, L.; Hadinegoro, S.R.; Erkin, M.; Ying, Z.; He, P.; Girsang, R.T.; Vergara, H.; Akram, J.; et al. Efficacy and Safety of the RBD-Dimer–Based COVID-19 Vaccine ZF2001 in Adults. N. Engl. J. Med. 2022, 386, 2097–2111. [Google Scholar] [CrossRef] [PubMed]
- Tanriover, M.D.; Doğanay, H.L.; Akova, M.; Güner, H.R.; Azap, A.; Akhan, S.; Köse, Ş.; Erdinç, F.Ş.; Akalın, E.H.; Tabak, Ö.F.; et al. Efficacy and Safety of an Inactivated Whole-Virion SARS-CoV-2 Vaccine (CoronaVac): Interim Results of a Double-Blind, Randomised, Placebo-Controlled, Phase 3 Trial in Turkey. Lancet 2021, 398, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Al Kaabi, N.; Zhang, Y.; Xia, S.; Yang, Y.; Al Qahtani, M.M.; Abdulrazzaq, N.; Al Nusair, M.; Hassany, M.; Jawad, J.S.; Abdalla, J.; et al. Effect of 2 Inactivated SARS-CoV-2 Vaccines on Symptomatic COVID-19 Infection in Adults. JAMA 2021, 326, 35–45. [Google Scholar] [CrossRef] [PubMed]
- Araf, Y.; Akter, F.; Tang, Y.; Fatemi, R.; Parvez, M.S.A.; Zheng, C.; Hossain, M.G. Omicron Variant of SARS-CoV-2: Genomics, Transmissibility, and Responses to Current COVID-19 Vaccines. J. Med. Virol. 2022, 94, 1825–1832. [Google Scholar] [CrossRef] [PubMed]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Rickeard, T.; Gallagher, E.; Gower, C.; Kall, M.; Groves, N.; O’Connell, A.; et al. COVID-19 Vaccine Effectiveness against the Omicron (B.1.1.529) Variant. N. Engl. J. Med. 2022, 386, 1532–1546. [Google Scholar] [CrossRef] [PubMed]
- Khandia, R.; Munjal, A.; Dhama, K.; Karthik, K.; Tiwari, R.; Malik, Y.S.; Singh, R.K.; Chaicumpa, W. Modulation of Dengue/Zika Virus Pathogenicity by Antibody-Dependent Enhancement and Strategies to Protect Against Enhancement in Zika Virus Infection. Front. Immunol. 2018, 9, 597. [Google Scholar] [CrossRef] [PubMed]
- Eggink, D.; Andeweg, S.P.; Vennema, H.; van Maarseveen, N.; Vermaas, K.; Vlaemynck, B.; Schepers, R.; van Gageldonk-Lafeber, A.B.; van den Hof, S.; Reusken, C.B.; et al. Increased Risk of Infection with SARS-CoV-2 Omicron BA.1 Compared with Delta in Vaccinated and Previously Infected Individuals, the Netherlands, 22 November 2021 to 19 January 2022. Eurosurveillance 2022, 27, 2101196. [Google Scholar] [CrossRef]
- Wang, Z.; Deng, T.; Zhang, Y.; Niu, W.; Nie, Q.; Yang, S.; Liu, P.; Pei, P.; Chen, L.; Li, H.; et al. ACE2 Can Act as the Secondary Receptor in the FcγR-Dependent ADE of SARS-CoV-2 Infection. iScience 2022, 25, 103720. [Google Scholar] [CrossRef]
- Shimizu, J.; Sasaki, T.; Koketsu, R.; Morita, R.; Yoshimura, Y.; Murakami, A.; Saito, Y.; Kusunoki, T.; Samune, Y.; Nakayama, E.E.; et al. Reevaluation of Antibody-Dependent Enhancement of Infection in Anti-SARS-CoV-2 Therapeutic Antibodies and MRNA-Vaccine Antisera Using FcR- and ACE2-Positive Cells. Sci. Rep. 2022, 12, 15612. [Google Scholar] [CrossRef]
- Wang, S.; Wang, J.; Yu, X.; Jiang, W.; Chen, S.; Wang, R.; Wang, M.; Jiao, S.; Yang, Y.; Wang, W.; et al. Antibody-Dependent Enhancement (ADE) of SARS-CoV-2 Pseudoviral Infection Requires FcγRIIB and Virus-Antibody Complex with Bivalent Interaction. Commun. Biol. 2022, 5, 262. [Google Scholar] [CrossRef]
- Zhang, K.; Chan, P.S.; Chen, S.; Fang, Y.; Cao, H.; Chen, H.; Hu, T.; Chen, Y.; Zhou, X.; Wang, Z. Factors Predicting COVID-19 Vaccination Uptake Among Men Who Have Sex with Men in China: An Observational Prospective Cohort Study. Front. Med. 2022, 9, 838973. [Google Scholar] [CrossRef]
- China CDC The Situation of the SARS-CoV-2 Infection in China. Available online: https://www.chinacdc.cn/jkzt/crb/zl/szkb_11803/jszl_13141/202304/t20230408_264979.html (accessed on 5 May 2024).
- Luo, M.; Gong, F.; Sun, J.; Gong, Z. For COVID-19, What Are the Priorities of Normalized Prevention and Control Strategies? BST 2023, 17, 63–67. [Google Scholar] [CrossRef]
- Zhao, J.; Zhao, S.; Ou, J.; Zhang, J.; Lan, W.; Guan, W.; Wu, X.; Yan, Y.; Zhao, W.; Wu, J.; et al. COVID-19: Coronavirus Vaccine Development Updates. Front. Immunol. 2020, 11, 602256. [Google Scholar] [CrossRef]
- Pérez-Then, E.; Lucas, C.; Monteiro, V.S.; Miric, M.; Brache, V.; Cochon, L.; Vogels, C.B.F.; Malik, A.A.; De la Cruz, E.; Jorge, A.; et al. Neutralizing Antibodies against the SARS-CoV-2 Delta and Omicron Variants Following Heterologous CoronaVac plus BNT162b2 Booster Vaccination. Nat. Med. 2022, 28, 481. [Google Scholar] [CrossRef]
- DiPiazza, A.T.; Graham, B.S.; Ruckwardt, T.J. T Cell Immunity to SARS-CoV-2 Following Natural Infection and Vaccination. Biochem. Biophys. Res. Commun. 2020, 538, 211–217. [Google Scholar] [CrossRef]
- Zhang, J.; He, Q.; An, C.; Mao, Q.; Gao, F.; Bian, L.; Wu, X.; Wang, Q.; Liu, P.; Song, L.; et al. Boosting with Heterologous Vaccines Effectively Improves Protective Immune Responses of the Inactivated SARS-CoV-2 Vaccine. Emerg. Microbes. Infect. 2021, 10, 1598–1608. [Google Scholar] [CrossRef]
- Karlsson, A.C.; Humbert, M.; Buggert, M. The Known Unknowns of T Cell Immunity to COVID-19. Sci. Immunol. 2020, 5, eabe8063. [Google Scholar] [CrossRef]
- McMahan, K.; Yu, J.; Mercado, N.B.; Loos, C.; Tostanoski, L.H.; Chandrashekar, A.; Liu, J.; Peter, L.; Atyeo, C.; Zhu, A.; et al. Correlates of Protection against SARS-CoV-2 in Rhesus Macaques. Nature 2020, 590, 630–634. [Google Scholar] [CrossRef] [PubMed]
- Zhang, D.; Zhong, J.; Xiong, H.; Li, Y.; Guo, T.; Peng, B.; Fang, C.; Kang, Y.; Tan, J.; Ma, Y. Protective Effect of Inactivated COVID-19 Vaccines against Omicron BA.2 Infection in Guangzhou: A Test-Negative Case-Control Real-World Study. Vaccines 2023, 11, 566. [Google Scholar] [CrossRef]
- Remelli, F.; Volpato, S.; Trevisan, C. Clinical Features of SARS-CoV-2 Infection in Older Adults. Clin. Geriatr. Med. 2022, 38, 483–500. [Google Scholar] [CrossRef]
- Scully, E.P.; Haverfield, J.; Ursin, R.L.; Tannenbaum, C.; Klein, S.L. Considering how biological sex impacts immune responses and COVID-19 outcomes. Nat. Rev. Immunol. 2020, 20, 442–447. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total Participants | Infection Outcome | p Value (χ2 Test of Fisher’s Exact Test) | OR (95% CI) (Univariable Regression Analysis) | p Value (Univariable Regression Analysis) | |
|---|---|---|---|---|---|---|
| (n/%) (n = 2007) | Infected (n/%) (n = 1663) | Uninfected (n/%) (n = 344) | ||||
| Gender | 0.732 | 0.732 | ||||
| Male | 841 (41.9) | 694 (41.7) | 147 (42.7) | 0.96 (0.759–1.214) | ||
| Female | 1166 (58.1) | 969 (58.3) | 197 (57.3) | Reference | ||
| Age (years) | 0.001 | 0.002 | ||||
| Less than 18 | 23 (1.1) | 16 (1.0) | 7 (2.0) | 1.000 (0.370–2.699) | ||
| 18–39 | 1076 (53.6) | 896 (53.9) | 180 (52.3) | 2.178 (1.358–3.492) | ||
| 40–59 | 816 (40.7) | 687 (41.3) | 129 (37.5) | 2.330 (1.438–3.774) | ||
| 60 and older | 92 (4.6) | 64 (3.8) | 28 (8.1) | Reference | ||
| Occupation | 0.001 | 0.001 | ||||
| Hospital and CDC staffs | 369 (18.4) | 318 (19.1) | 51 (14.8) | Reference | ||
| Teachers | 205 (10.2) | 184 (11.1) | 21 (6.1) | 1.405 (0.819–2.410) | ||
| Students | 475 (23.7) | 376 (22.6) | 99 (28.8) | 0.609 (0.421–0.881) | ||
| Staffs of government and the public sector | 245 (12.2) | 204 (12.3) | 41 (11.9) | 0.798 (0.510–1.248) | ||
| Company employees | 282 (14.1) | 242 (14.6) | 40 (11.6) | 0.970 (0.621–1.516) | ||
| Retired | 131 (6.5) | 99 (6.0) | 32 (9.3) | 0.496 (0.302–0.815) | ||
| Others | 300 (14.9) | 240 (14.4) | 60 (17.4) | 0.642 (0.426–0.966) | ||
| History of underlying disease | 0.786 | 0.787 | ||||
| No prior medical history | 1716 (85.5) | 1421 (85.4) | 295 (85.8) | Reference | ||
| Cerebral-cardiovascular diseases | 146 (7.3) | 124 (7.5) | 22 (6.4) | 1.170 (0.731–1.873) | ||
| Pulmonary disease | 39 (1.9) | 33 (2.0) | 6 (1.7) | 1.142 (0.474–2.750) | ||
| Others | 106 (5.3) | 85 (5.1) | 21 (6.1) | 0.840 (0.513–1.377) | ||
| History of vaccination | 0.047 | 0.050 | ||||
| Unvaccinated | 74 (3.7) | 55 (3.3) | 19 (5.5) | Reference | ||
| Vaccinated | 1933 (96.3) | 1608 (96.7) | 325 (94.5) | 1.709 (1.001–2.918) | ||
| Variables | Dependent Variable | β | Odds Ratio | 95% CI | p Value | |
|---|---|---|---|---|---|---|
| Infected (n/%) | Uninfected (n/%) | |||||
| Type of vaccination | <0.001 | |||||
| Unvaccinated | 46 (4.0) | 19 (6.4) | — | Reference | ||
| Vaccinated only with inactivated vaccines | 1007 (88.4) | 203 (68.8) | 0.717 | 2.049 | 1.176–3.570 | |
| At least one shot of non-inactivated vaccine | 86 (7.6) | 73 (24.7) | −0.720 | 0.487 | 0.262–0.904 | |
| Vaccination status | 0.553 | |||||
| Not completed first booster vaccination | 222 (19.5) | 53 (18.0) | — | Reference | ||
| Completed first booster vaccination | 917 (80.5) | 242 (82.0) | −0.100 | 0.905 | 0.649–1.260 | |
| Gender | 0.997 | |||||
| Male | 470 (41.3) | 122 (41.4) | — | Reference | ||
| Female | 669 (58.7) | 173 (58.6) | 0.004 | 1.004 | 0.774–1.302 | |
| Age (years) | — | — | −0.001 | 0.999 | 0.989–1.009 | 0.871 |
| Occupation | 0.004 | |||||
| Hospital and CDC staffs | 241 (21.2) | 45 (15.3) | — | Reference | ||
| Teachers | 116 (10.2) | 19 (6.4) | 0.131 | 1.140 | 0.638–2.036 | |
| Students | 251 (22.0) | 87 (29.5) | −0.619 | 0.539 | 0.361–0.804 | |
| Staffs of government and the public sector | 170 (14.9) | 38 (12.9) | −0.180 | 0.835 | 0.520–1.342 | |
| Company employees | 168 (14.7) | 38 (12.9) | −0.192 | 0.826 | 0.514–1.327 | |
| Retired | 61 (5.4) | 24 (8.1) | −0.745 | 0.475 | 0.269–0.839 | |
| Others | 132 (11.6) | 44 (3.1) | −0.580 | 0.560 | 0.351–0.893 | |
| History of underlying disease | 0.591 | |||||
| No prior medical history | 966 (84.8) | 256 (86.8) | — | Reference | ||
| Cerebral-cardiovascular diseases | 86 (7.6) | 16 (5.4) | 0.354 | 1.424 | 0.821–2.472 | |
| Pulmonary disease | 24 (2.1) | 5 (1.7) | 0.241 | 1.272 | 0.481–3.367 | |
| Others | 63 (5.5) | 18 (6.1) | −0.75 | 0.928 | 0.540–1.594 | |
| Variables | Dependent Variable | β | Odds Ratio | 95% CI | p Value | |
|---|---|---|---|---|---|---|
| Infected (n/%) | Uninfected (n/%) | |||||
| Type of vaccination | <0.001 | |||||
| Unvaccinated | 46 (6.9) | 19 (9.8) | — | Reference | ||
| Vaccinated only with inactivated vaccines | 558 (84.0) | 122 (62.9) | 0.639 | 1.889 | 1.069–3.338 | |
| At least one shot of non-inactivated vaccine | 60 (9.0) | 53 (27.3) | −0.760 | 0.468 | 0.244–0.895 | |
| Vaccination status | 0.619 | |||||
| Not completed first booster vaccination | 141 (21.2) | 38 (19.6) | — | Reference | ||
| Completed first booster vaccination | 523 (78.8) | 156 (80.4) | −0.101 | 0.904 | 0.605–1.348 | |
| Time interval | 0.352 | |||||
| Unvaccinated | 46 (6.9) | 19 (9.8) | Reference | |||
| <1 years | 344 (51.8) | 93 (47.9) | 0.424 | 1.528 | 0.854–2.733 | |
| >1 years | 274 (41.3) | 82 (23.0) | 0.322 | 1.380 | 0.766–2.487 | |
| Gender | 0.634 | |||||
| Male | 251 (37.8) | 77 (39.7) | — | Reference | ||
| Female | 413 (77.9) | 117 (60.3) | 0.080 | 1.083 | 0.780–1.503 | |
| Age (years) | — | — | −0.005 | 0.995 | 0.983–1.007 | 0.422 |
| Occupation | 0.339 | |||||
| Hospital and CDC staffs | 132 (19.9) | 35 (18.0) | — | Reference | ||
| Teachers | 67 (10.1) | 12 (6.2) | 0.392 | 1.480 | 0.722–3.037 | |
| Students | 142 (21.4) | 48 (24.7) | −0.243 | 0.784 | 0.478–1.288 | |
| Staffs of government and the public sector | 104 (15.1) | 27 (13.9) | 0.021 | 1.021 | 0.581–1.795 | |
| Company employees | 100 (15.1) | 26 (13.4) | 0.020 | 1.020 | 0.577–1.803 | |
| Retired | 50 (7.5) | 21 (10.8) | −0.460 | 0.631 | 0.366–1.187 | |
| Others | 69 (10.4) | 25 (12.9) | −0.312 | 0.732 | 0.406–1.320 | |
| History of underlying disease | 0.366 | |||||
| No prior medical history | 545 (76.4) | 168 (86.6) | — | Reference | ||
| Cerebral-cardiovascular diseases | 59 (8.9) | 12 (6.2) | 0.416 | 1.516 | 0.796–2.887 | |
| Pulmonary disease | 17 (2.6) | 2 (1.0) | 0.963 | 2.620 | 0.599–11.457 | |
| Others | 43 (6.5) | 12 (6.2) | 0.099 | 1.105 | 0.569–2.143 | |
| Variables | Dependent Variable | β | Odds Ratio | 95% CI | p Value | |
|---|---|---|---|---|---|---|
| Mild (n/%) | Severe (n/%) | |||||
| Type of vaccination | 0.044 | |||||
| Unvaccinated | 25 (5.2) | 15 (3.0) | — | Reference | ||
| Vaccinated only with inactivated vaccines | 418 (86.2) | 457 (91.2) | 0.600 | 1.822 | 0.948–3.503 | |
| At least one shot of non-inactivated vaccine | 42 (8.7) | 29 (5.8) | 0.140 | 1.151 | 0.519–2.551 | |
| Vaccination status | 0.037 | |||||
| Not completed first booster vaccination | 110 (22.7) | 87 (17.4) | — | Reference | ||
| Completed first booster vaccination | 375 (77.3) | 414 (82.6) | 0.334 | 1.396 | 1.020–1.911 | |
| Gender | <0.001 | |||||
| Male | 246 (50.7) | 173 (34.5) | — | Reference | ||
| Female | 239 (49.3) | 328 (65.5) | 0.669 | 1.951 | 1.511–2.521 | |
| Age (years) | — | — | −0.027 | 0.973 | 0.963–0.984 | <0.001 |
| Occupation | 0.002 | |||||
| Hospital and CDC staffs | 91 (18.8) | 115 (23.0) | — | Reference | — | |
| Teachers | 51 (10.5) | 51 (10.2) | −0.234 | 0.791 | 0.492–1.273 | |
| Students | 85 (17.5) | 122 (24.4) | 0.127 | 1.136 | 0.769–1.678 | |
| Staffs of government and the public sector | 73 (15.1) | 77 (15.4) | −0.181 | 0.835 | 0.547–1.273 | |
| Company employees | 83 (17.1) | 63 (12.6) | −0.510 | 0.601 | 0.392–0.921 | |
| Retired | 39 (8.0) | 17 (3.4) | −1.064 | 0.345 | 0.183–0.649 | |
| Others | 63 (13.0) | 56 (11.2) | −0.352 | 0.703 | 0.447–1.106 | |
| History of underlying disease | 0.123 | |||||
| No prior medical history | 404 (83.3) | 433 (86.4) | — | Reference | — | |
| Cerebral-cardiovascular diseases | 48 (9.9) | 31 (6.2) | −0.507 | 0.603 | 0.376–0.966 | |
| Pulmonary disease | 6 (1.2) | 11 (2.2) | 0.537 | 1.711 | 0.627–4.668 | |
| Others | 27 (5.6) | 26 (5.2) | −0.107 | 0.898 | 0.516–1.566 | |
| Variables | Dependent Variable (Days) | β | Odds Ratio | 95% CI | p Value | ||
|---|---|---|---|---|---|---|---|
| Less than 3 (n/%) | 4–6 (n/%) | 7 and More (n/%) | |||||
| Type of vaccination | |||||||
| Unvaccinated | 11 (6.9) | 11 (2.7) | 18 (4.2) | — | Reference | — | — |
| Vaccinated only with inactivated vaccines | 135 (84.9) | 358 (89.3) | 382 (89.7) | 0.222 | 1.249 | 0.691–2.259 | 0.462 |
| At least one shot of non-inactivated vaccine | 13 (8.2) | 32 (8.0) | 26 (6.1) | −0.039 | 0.962 | 0.466–1.984 | 0.915 |
| Vaccination status | |||||||
| Not completed first booster vaccination | 30 (18.9) | 80 (20.0) | 87 (20.4) | — | Reference | — | — |
| Completed first booster vaccination | 129 (81.1) | 321 (80.0) | 339 (79.6) | −0.058 | 0.944 | 0.703–1.266 | 0.699 |
| Age (years) | — | — | — | 0.018 | 1.018 | 1.008–1.028 | <0.001 |
| Occupation | |||||||
| Hospital and CDC staffs | 17 (10.7) | 92 (22.9) | 97 (22.8) | — | Reference | — | — |
| Teachers | 14 (8.8) | 39 (9.7) | 49 (11.5) | −0.070 | 0.932 | 0.593–1.465 | 0.761 |
| Students | 39 (24.5) | 96 (23.9) | 72 (16.9) | −0.564 | 0.569 | 0.395–0.820 | 0.002 |
| Staffs of government and the public sector | 19 (11.9) | 64 (16.0) | 67 (15.7) | −0.154 | 0.857 | 0.575–1.279 | 0.451 |
| Company employees | 31 (19.5) | 63 (15.7) | 52 (12.2) | −0.594 | 0.552 | 0.370–0.824 | 0.004 |
| Retired | 10 (6.3) | 11 (2.7) | 35 (8.2) | 0.360 | 1.433 | 0.803–2.563 | 0.224 |
| Others | 29 (18.2) | 36 (9.0) | 54 (12.7) | −0.376 | 0.687 | 0.448–1.051 | 0.084 |
| History of underlying disease | |||||||
| No prior medical history | 135 (84.9) | 355 (88.5) | 347 (81.5) | — | Reference | — | — |
| Cerebral-cardiovascular diseases | 13 (8.2) | 26 (6.5) | 40 (9.4) | 0.276 | 1.318 | 0.850–2.044 | 0.217 |
| Pulmonary disease | 3 (1.9) | 4 (1.0) | 10 (2.3) | 0.538 | 1.713 | 0.672–4.362 | 0.260 |
| Others | 8 (5.0) | 16 (4.0) | 29 (6.8) | 0.439 | 1.551 | 0.908–2.649 | 0.108 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Xiong, H.; Meng, X.; Song, Y.; Zhong, J.; Liu, S.; Zhu, X.; Ye, X.; Zhong, Y.; Zhang, D. Have Previous COVID-19 Vaccinations Shaped the Potential Enhancing Infection of Variant Strains? Vaccines 2024, 12, 567. https://doi.org/10.3390/vaccines12060567
Xiong H, Meng X, Song Y, Zhong J, Liu S, Zhu X, Ye X, Zhong Y, Zhang D. Have Previous COVID-19 Vaccinations Shaped the Potential Enhancing Infection of Variant Strains? Vaccines. 2024; 12(6):567. https://doi.org/10.3390/vaccines12060567
Chicago/Turabian StyleXiong, Husheng, Xiang Meng, Yanqin Song, Jiayi Zhong, Shuang Liu, Xun Zhu, Xin Ye, Yonghui Zhong, and Dingmei Zhang. 2024. "Have Previous COVID-19 Vaccinations Shaped the Potential Enhancing Infection of Variant Strains?" Vaccines 12, no. 6: 567. https://doi.org/10.3390/vaccines12060567
APA StyleXiong, H., Meng, X., Song, Y., Zhong, J., Liu, S., Zhu, X., Ye, X., Zhong, Y., & Zhang, D. (2024). Have Previous COVID-19 Vaccinations Shaped the Potential Enhancing Infection of Variant Strains? Vaccines, 12(6), 567. https://doi.org/10.3390/vaccines12060567