
Vaccination with Adenovirus Type 5 Vector-Based COVID-19 Vaccine as the Primary Series in Adults: A Randomized, Double-Blind, Placebo-Controlled Phase 1/2 Clinical Trial


Abstract
1. Introduction
2. Methods
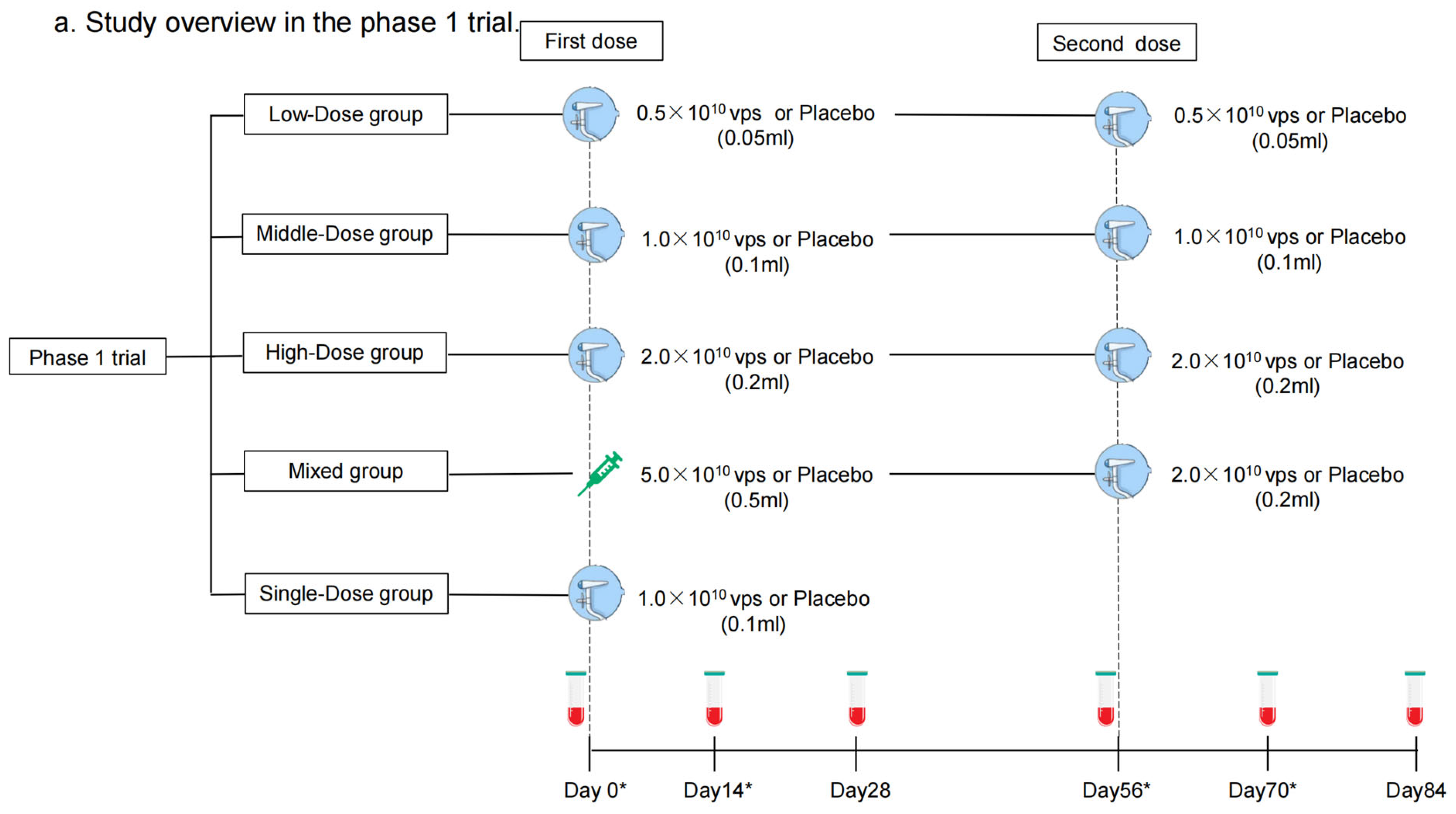
2.1. Study Design and Participants
2.2. Randomization and Masking
2.3. Procedures
2.4. Outcomes
2.5. Statistical Analysis
3. Results
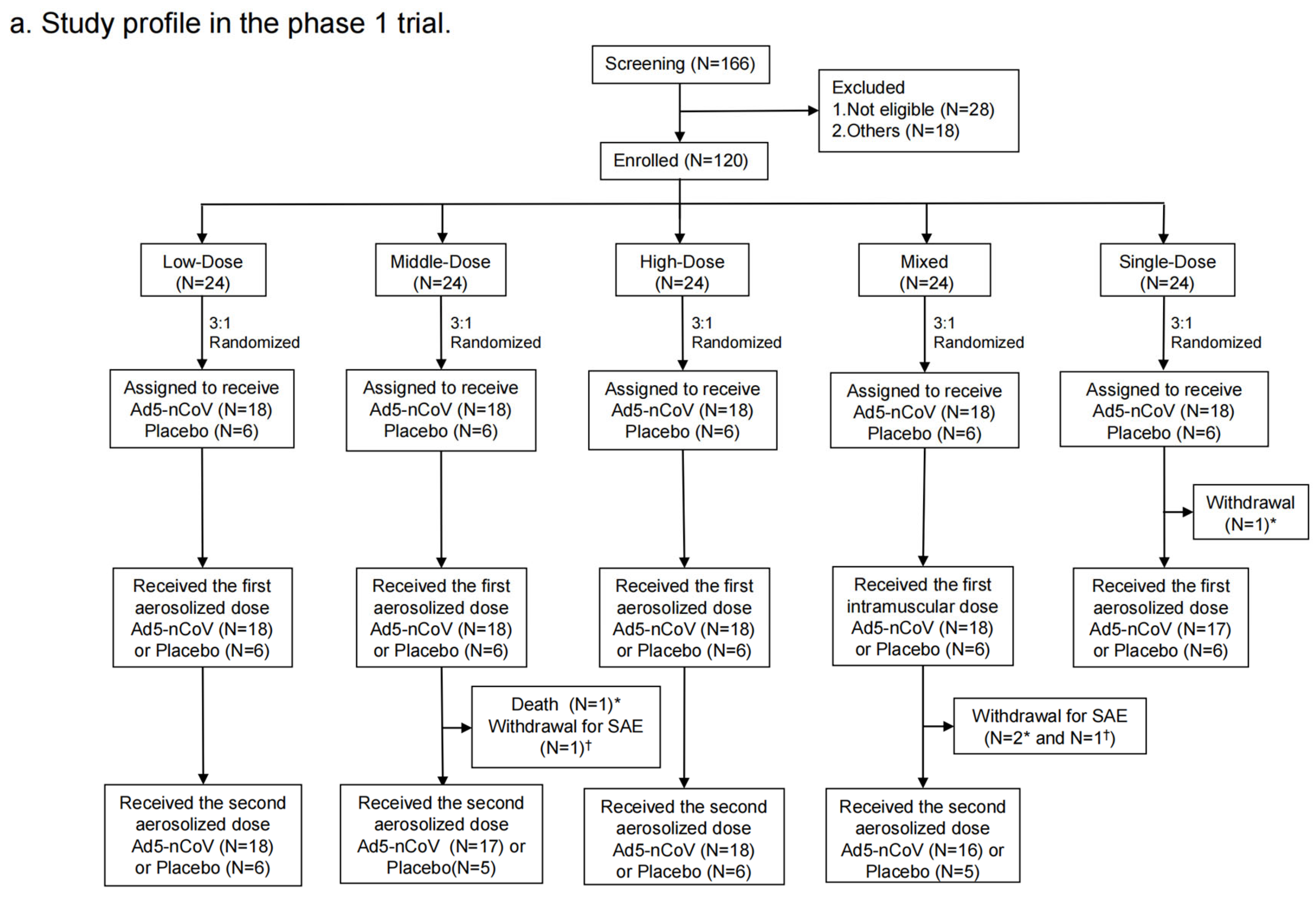
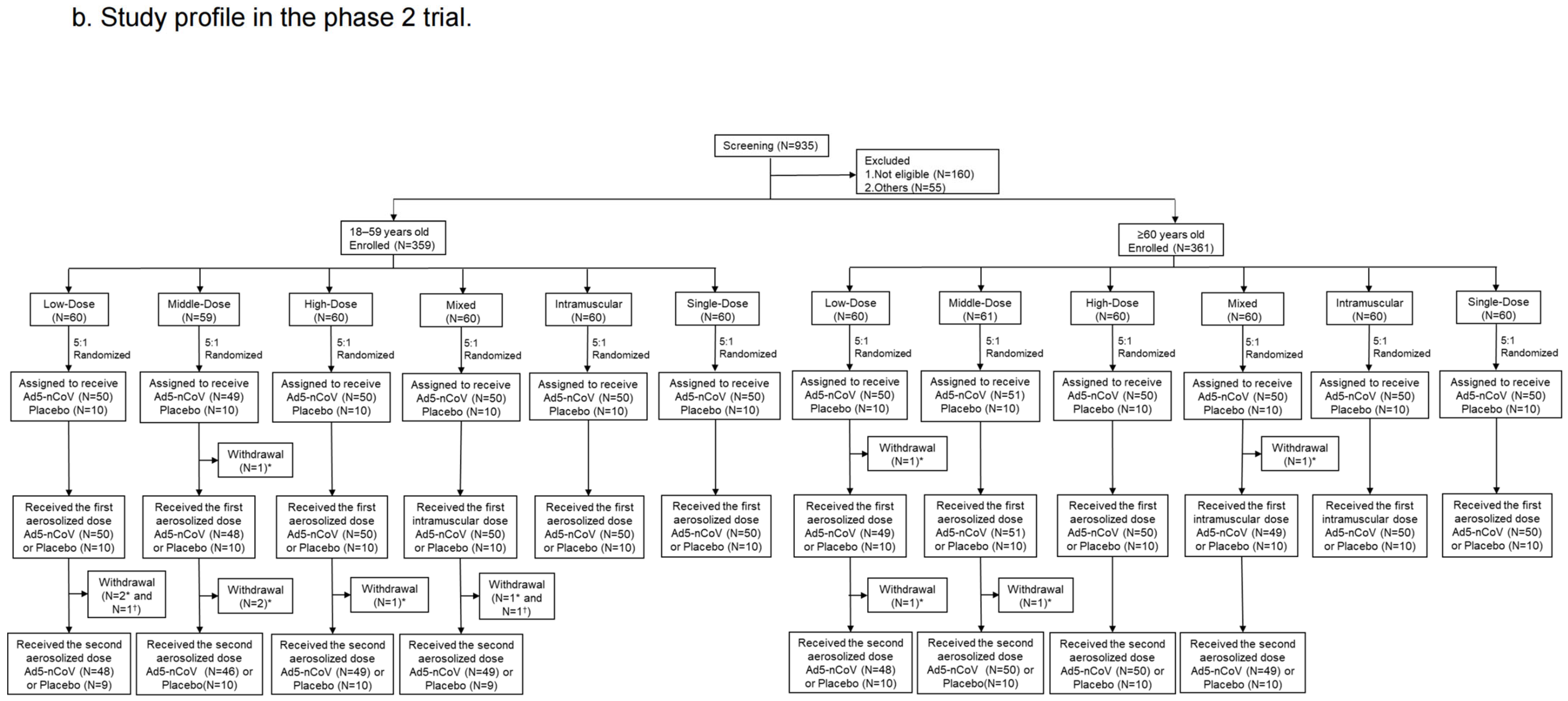
3.1. Study Participants
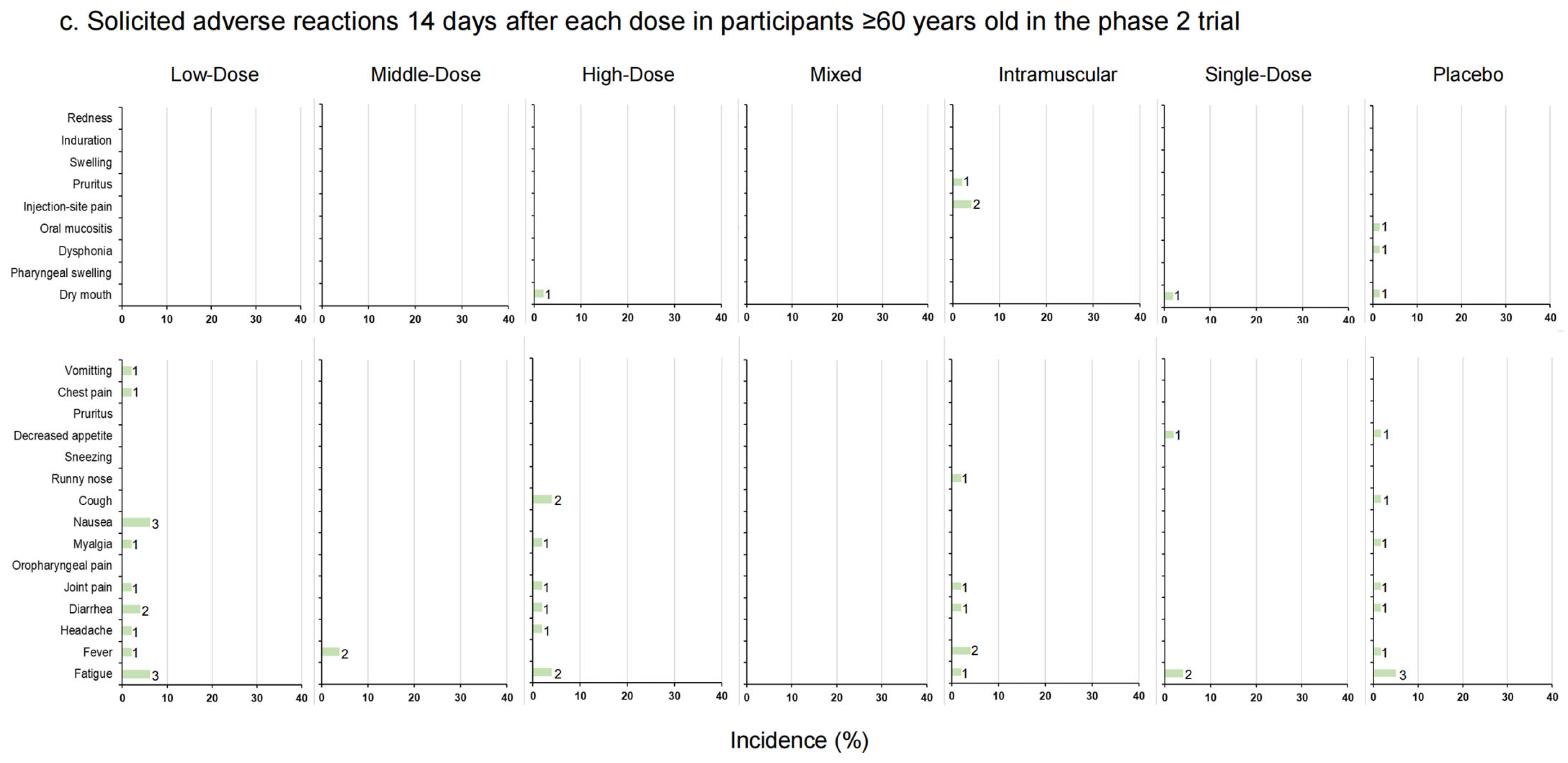
3.2. Safety
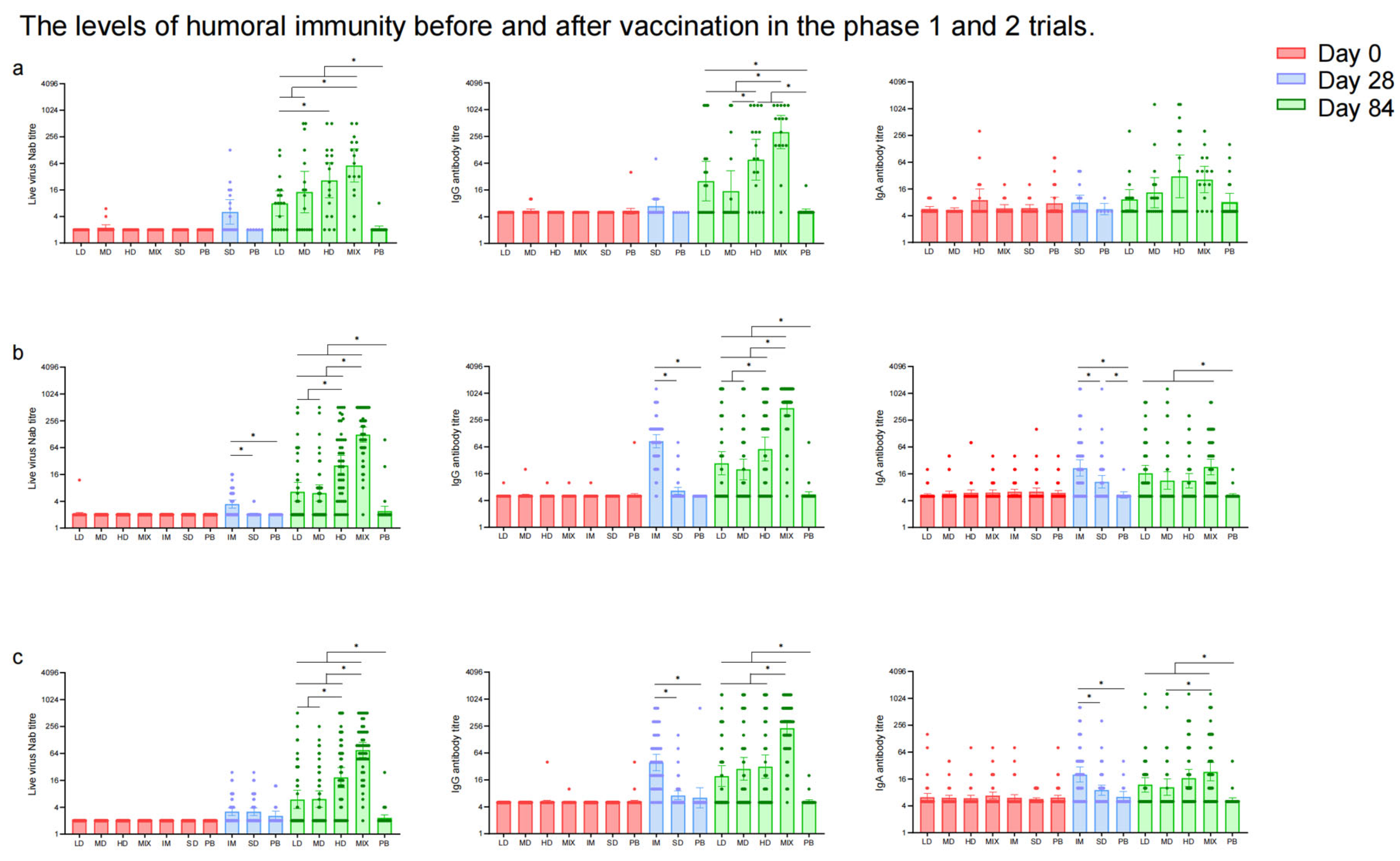
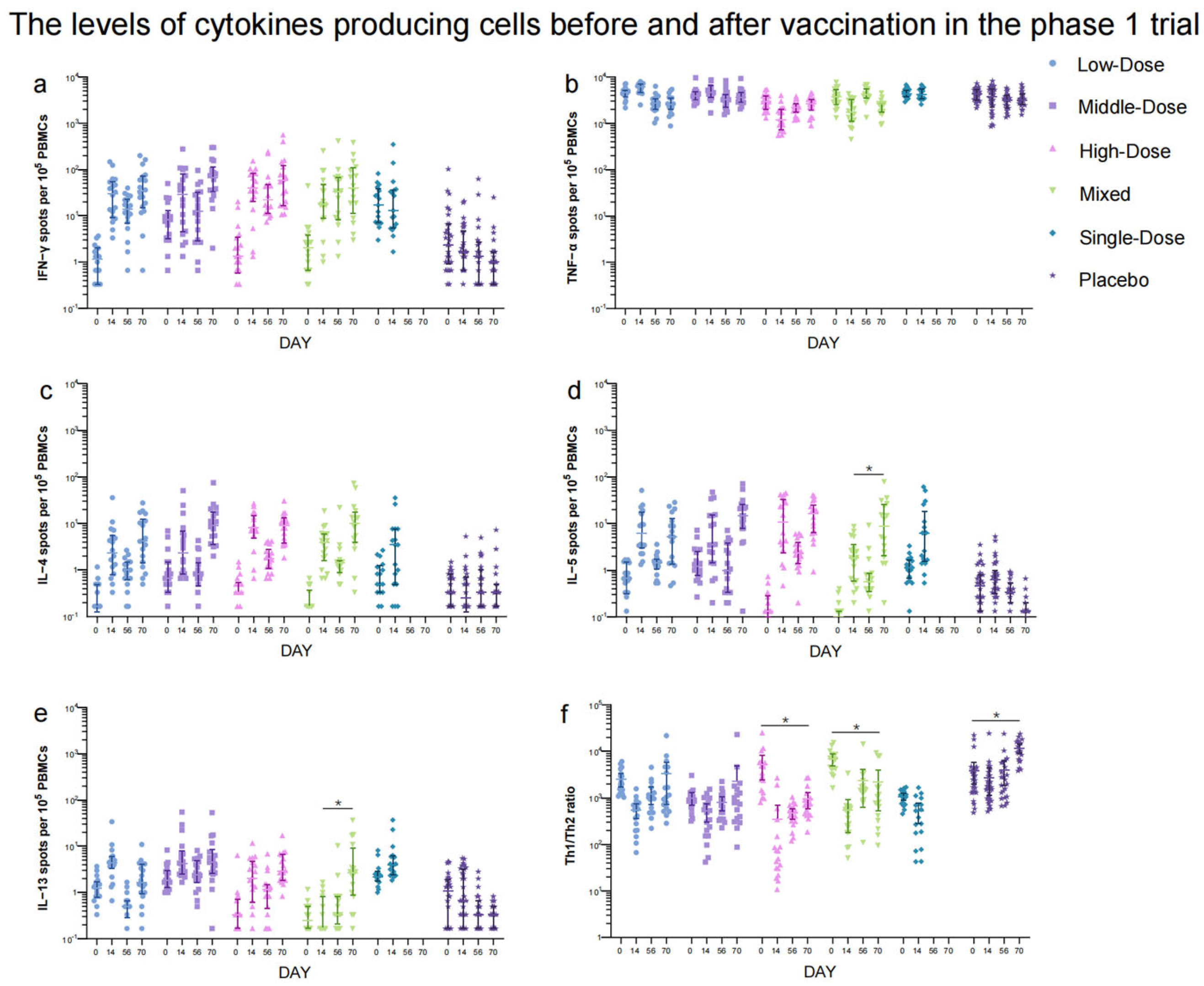
3.3. Immunogenicity
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Halperin, S.A.; Ye, L.; MacKinnon-Cameron, D.; Smith, B.; Cahn, P.E.; Ruiz-Palacios, G.M.; Ikram, A.; Lanas, F.; Lourdes Guerrero, M.; Muñoz Navarro, S.R.; et al. Final efficacy analysis, interim safety analysis, and immunogenicity of a single dose of recombinant novel coronavirus vaccine (adenovirus type 5 vector) in adults 18 years and older: An international, multicentre, randomised, double-blinded, placebo-controlled phase 3 trial. Lancet 2022, 399, 237–248. [Google Scholar] [CrossRef] [PubMed]
- WHO. WHO Validates 11th Vaccine for COVID-19. 19 May 2022. Available online: https://www.who.int/news/item/19-05-2022-who-validates-11th-vaccine-for-covid-19 (accessed on 9 December 2023).
- WHO. WHO Lists Two Additional COVID-19 Vaccines for Emergency Use and COVAX Roll-Out. 15 February 2021. Available online: https://www.who.int/news/item/15-02-2021-who-lists-two-additional-covid-19-vaccines-for-emergency-use-and-covax-roll-out (accessed on 9 December 2023).
- WHO. The Janssen Ad26.COV2.S COVID-19 Vaccine: What you Need to Know. 6 June 2022. Available online: https://www.who.int/news-room/feature-stories/detail/the-j-j-covid-19-vaccine-what-you-need-to-know (accessed on 9 December 2023).
- Morens, D.M.; Taubenberger, J.K.; Fauci, A.S. Rethinking next-generation vaccines for coronaviruses, influenzaviruses, and other respiratory viruses. Cell Host Microbe 2023, 31, 146–157. [Google Scholar] [CrossRef] [PubMed]
- Knisely, J.M.; Buyon, L.E.; Mandt, R.; Farkas, R.; Balasingam, S.; Bok, K.; Buchholz, U.J.; D’Souza, M.P.; Gordon, J.L.; King, D.F.L.; et al. Mucosal vaccines for SARS-CoV-2: Scientific gaps and opportunities-workshop report. NPJ Vaccines 2023, 8, 53. [Google Scholar] [CrossRef] [PubMed]
- Freeman, D.; Lambe, S.; Yu, L.M.; Freeman, J.; Chadwick, A.; Vaccari, C.; Waite, F.; Rosebrock, L.; Petit, A.; Vanderslott, S.; et al. Injection fears and COVID-19 vaccine hesitancy. Psychol. Med. 2023, 53, 1185–1195. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Huang, J.; Zhang, Z.; Wu, J.; Zhang, J.; Hu, H.; Zhu, T.; Zhang, J.; Luo, L.; Fan, P.; et al. Safety, tolerability, and immunogenicity of an aerosolised adenovirus type-5 vector-based COVID-19 vaccine (Ad5-nCoV) in adults: Preliminary report of an open-label and randomised phase 1 clinical trial. Lancet Infect. Dis. 2021, 21, 1654–1664. [Google Scholar] [CrossRef]
- China National Medical Products of Administration. Guidelines for Grading Standards of Adverse Events in Clinical Studies of Prophylactic Vaccines (No. 102, 2019). 26 December 2019. Available online: https://www.nmpa.gov.cn/xxgk/ggtg/ypggtg/ypqtggtg/20191231111901460.html (accessed on 29 January 2024).
- Tang, R.; Zheng, H.; Wang, B.S.; Gou, J.B.; Guo, X.L.; Chen, X.Q.; Chen, Y.; Wu, S.P.; Zhong, J.; Pan, H.X.; et al. Safety and immunogenicity of aerosolised Ad5-nCoV, intramuscular Ad5-nCoV, or inactivated COVID-19 vaccine CoronaVac given as the second booster following three doses of CoronaVac: A multicentre, open-label, phase 4, randomised trial. Lancet Respir. Med. 2023, 11, 613–623. [Google Scholar] [CrossRef] [PubMed]
- Sprangers, M.C.; Lakhai, W.; Koudstaal, W.; Verhoeven, M.; Koel, B.F.; Vogels, R.; Goudsmit, J.; Havenga, M.J.; Kostense, S. Quantifying adenovirus-neutralizing antibodies by luciferase transgene detection: Addressing preexisting immunity to vaccine and gene therapy vectors. J. Clin. Microbiol. 2003, 41, 5046–5052. [Google Scholar] [CrossRef]
- Cines, D.B.; Bussel, J.B. SARS-CoV-2 Vaccine-Induced Immune Thrombotic Thrombocytopenia. N. Engl. J. Med. 2021, 384, 2254–2256. [Google Scholar] [CrossRef] [PubMed]
- Walker, J.A.; McKenzie, A.N.J. TH2 cell development and function. Nat. Rev. Immunol. 2018, 18, 121–133. [Google Scholar] [CrossRef] [PubMed]
- CanSinoBio. The first Aerosolized COVID-19 Vaccine around the World Has Been Approved for Emergency Use in China. September 2022. Available online: https://www.cansinotech.com.cn/html/1///179/180/1750.html (accessed on 9 December 2023).
- Zhang, H.; Xu, N.; Xu, Y.; Qin, P.; Dai, R.; Xu, B.; Wang, S.; Ding, L.; Fu, J.; Zhang, S.; et al. Safety and immunogenicity of Ad5-nCoV immunization after three-dose priming with inactivated SARS-CoV-2 vaccine in Chinese adults. Nat. Commun. 2023, 14, 4757. [Google Scholar] [CrossRef] [PubMed]
- Deng, J.; Ma, Y.; Liu, Q.; Du, M.; Liu, M.; Liu, J. Comparison of the Effectiveness and Safety of Heterologous Booster Doses with Homologous Booster Doses for SARS-CoV-2 Vaccines: A Systematic Review and Meta-Analysis. Int. J. Environ. Res. Public Health 2022, 19, 10752. [Google Scholar] [CrossRef] [PubMed]
- Wang, F.; Huang, B.; Deng, Y.; Zhang, S.; Liu, X.; Wang, L.; Liu, Q.; Zhao, L.; Tang, L.; Wang, W.; et al. Neutralizing antibody levels associated with injectable and aerosolized Ad5-nCoV boosters and BA.2 infection. BMC Med. 2023, 21, 233. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Phase 1 | Low-Dose | Middle-Dose | High-Dose | Mixed | Single-Dose | Placebo | |
|---|---|---|---|---|---|---|---|
| N | 18 | 18 | 18 | 18 | 17 | 30 | |
| Age (SD), years | 45.4 (17.4) | 51.1 (14.4) | 50.9 (15.5) | 57.4 (14.2) | 50.3 (15.5) | 56.5 (13.9) | |
| 18–59 | 12 (66.67) | 13 (72.22) | 12 (66.67) | 11 (61.11) | 10 (58.82) | 14 (46.67) | |
| ≥60 | 6 (33.33) | 5 (27.78) | 6 (33.33) | 7 (38.89) | 7 (41.18) | 16 (53.33) | |
| Sex (%) | |||||||
| Male | 9 (50.0) | 4 (22.2) | 7 (38.9) | 12 (66.7) | 5 (29.4) | 17 (56.7) | |
| Female | 9 (50.0) | 14 (77.8) | 11 (61.1) | 6 (33.3) | 12 (70.6) | 13 (43.3) | |
| Body-mass index (SD), kg/m2 | 25.4 (3.8) | 25.0 (2.5) | 25.3 (3.9) | 25.5 (2.6) | 26.3 (3.4) | 24.9 (3.5) | |
| Pre-existing adenovirus type 5 neutralizing antibody | |||||||
| ≤1:200, titer | 5 (27.8) | 6 (33.3) | 7 (38.9) | 6 (33.3) | 6 (35.3) | 12 (40.0) | |
| >1:200, titer | 13 (72.2) | 12 (66.7) | 11 (61.1) | 12 (66.7) | 11 (64.7) | 18 (60.0) | |
| Phase 2 | Low-Dose | Middle-Dose | High-Dose | Mixed | Intramuscular | Single-Dose | Placebo |
| N | 99 | 99 | 100 | 99 | 100 | 99 | 120 |
| Age (SD), years | 56.8 (12.9) | 57.5 (12.3) | 58.8 (13.4) | 56.7 (14.0) | 58.9 (12.7) | 57.7 (11.8) | 55.8 (13.8) |
| 18–59 | 50 (50.5) | 48 (48.5) | 50 (50.0) | 50 (50.5) | 50 (50.0) | 50 (50.5) | 60 (50.0) |
| ≥60 | 49 (49.5) | 51 (51.5) | 50 (50.0) | 49 (49.5) | 50 (50.0) | 49 (49.5) | 60 (50.0) |
| Sex | |||||||
| Male | 42 (42.4) | 50 (50.5) | 56 (56.0) | 54 (54.5) | 45 (45.0) | 48 (48.0) | 50 (41.7) |
| Female | 57 (57.6) | 49 (49.5) | 44 (44.0) | 45 (45.5) | 55 (55.0) | 52 (52.0) | 70 (58.3) |
| Body-mass index (SD), kg/m2 | 26.7 (3.2) | 25.7 (3.2) | 26.0 (3.8) | 25.3 (3.6) | 25.5 (4.2) | 25.8 (3.7) | 25.4 (3.5) |
| Pre-existing adenovirus type 5 neutralizing antibody | |||||||
| ≤1:200, titer | 29 (29.3) | 24 (24.2) | 37 (37.0) | 37 (37.4) | 27 (27.0) | 38 (38.4) | 36 (30.0) |
| >1:200, titer | 70 (70.7) | 75 (75.8) | 63 (63.0) | 62 (62.6) | 73 (73.0) | 62 (61.6) | 84 (70.0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhu, Y.; Tang, R.; Li, X.; Chen, X.; Wang, X.; Wang, Y.; Wang, R.; Zhu, F.; Li, J. Vaccination with Adenovirus Type 5 Vector-Based COVID-19 Vaccine as the Primary Series in Adults: A Randomized, Double-Blind, Placebo-Controlled Phase 1/2 Clinical Trial. Vaccines 2024, 12, 292. https://doi.org/10.3390/vaccines12030292
Zhu Y, Tang R, Li X, Chen X, Wang X, Wang Y, Wang R, Zhu F, Li J. Vaccination with Adenovirus Type 5 Vector-Based COVID-19 Vaccine as the Primary Series in Adults: A Randomized, Double-Blind, Placebo-Controlled Phase 1/2 Clinical Trial. Vaccines. 2024; 12(3):292. https://doi.org/10.3390/vaccines12030292
Chicago/Turabian StyleZhu, Yawen, Rong Tang, Xiaolong Li, Xiaoqin Chen, Xue Wang, Ying Wang, Ruijie Wang, Fengcai Zhu, and Jingxin Li. 2024. "Vaccination with Adenovirus Type 5 Vector-Based COVID-19 Vaccine as the Primary Series in Adults: A Randomized, Double-Blind, Placebo-Controlled Phase 1/2 Clinical Trial" Vaccines 12, no. 3: 292. https://doi.org/10.3390/vaccines12030292
APA StyleZhu, Y., Tang, R., Li, X., Chen, X., Wang, X., Wang, Y., Wang, R., Zhu, F., & Li, J. (2024). Vaccination with Adenovirus Type 5 Vector-Based COVID-19 Vaccine as the Primary Series in Adults: A Randomized, Double-Blind, Placebo-Controlled Phase 1/2 Clinical Trial. Vaccines, 12(3), 292. https://doi.org/10.3390/vaccines12030292