
Hybrid Immunity Improves the Immune Response after the Fourth COVID-19 Vaccine Dose in Individuals with Medical Conditions Predisposing to Severe COVID-19
 ,
,
Abstract
1. Introduction
2. Materials and Methods
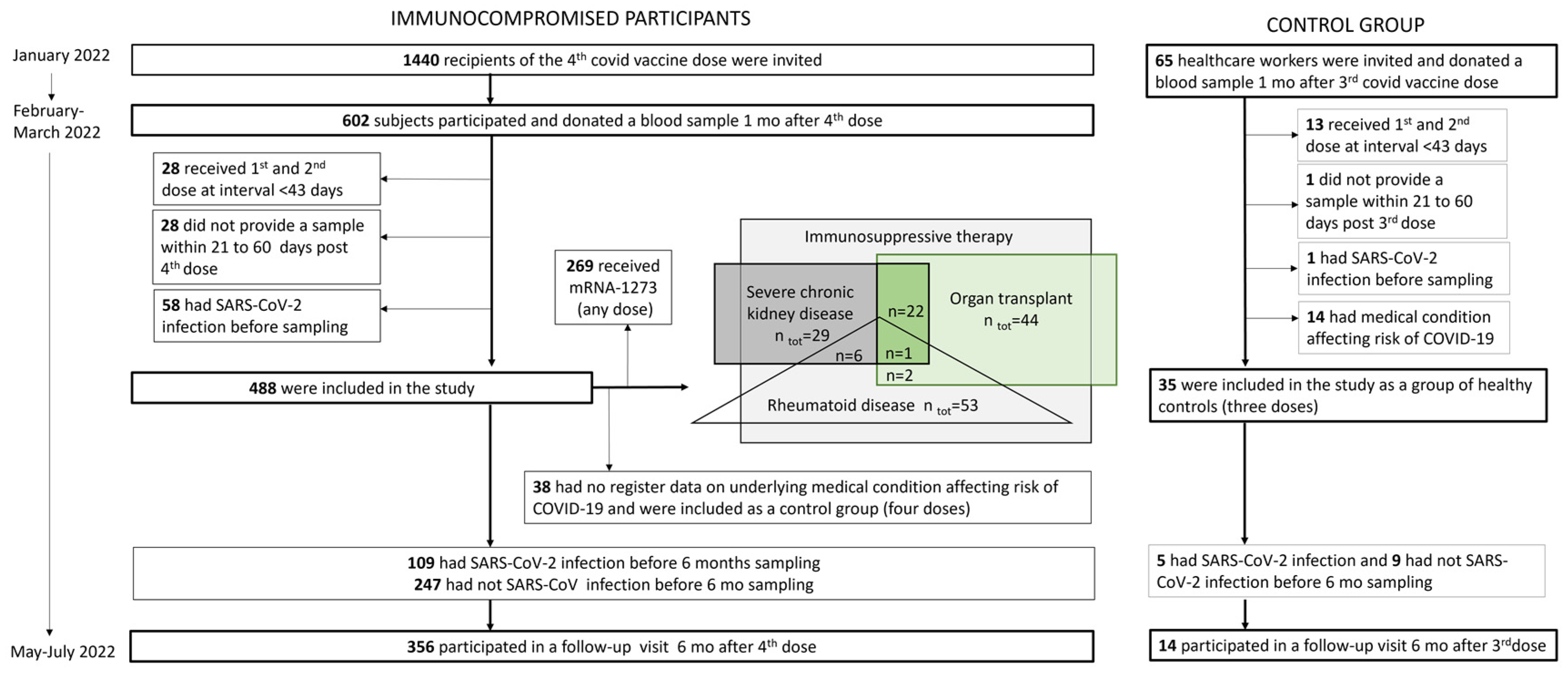
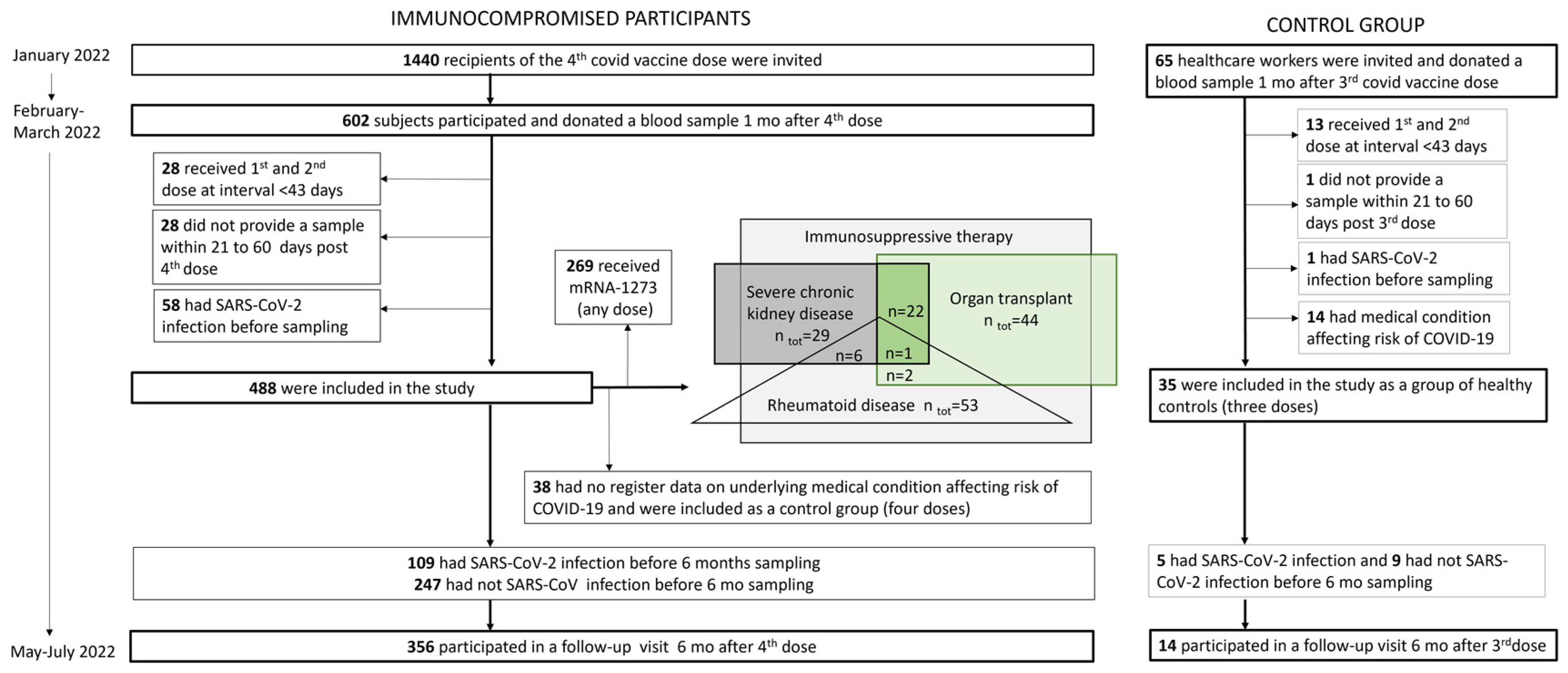
2.1. Study Design and Participants
2.2. Laboratory Analyses
2.2.1. SARS-CoV-2 Fluorescent Multiplex Immunoassay
2.2.2. Microneutralization Assay
2.3. Statistical Methods
3. Results
3.1. Characteristics of the Participants Who Received Four Vaccine Doses
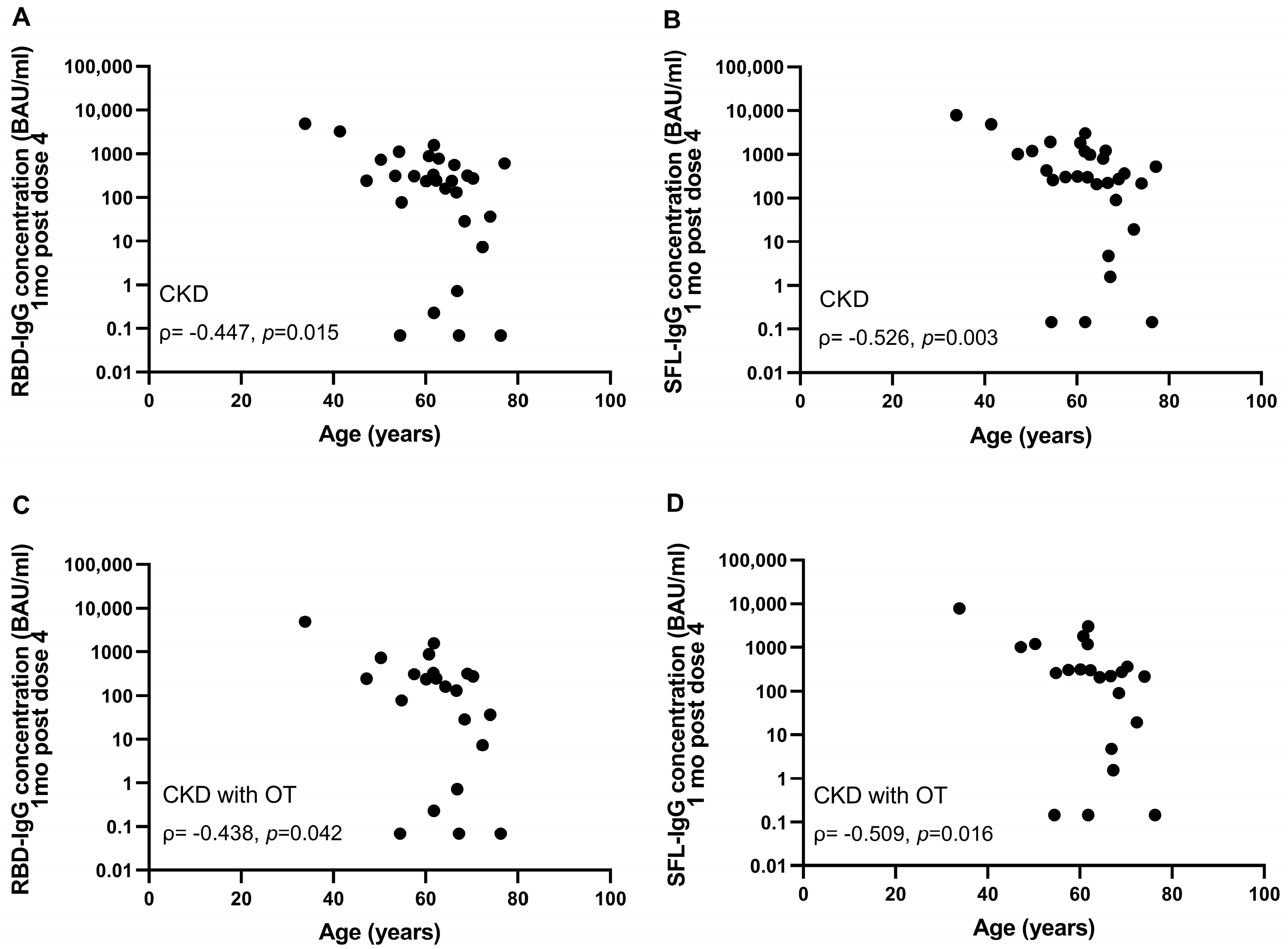
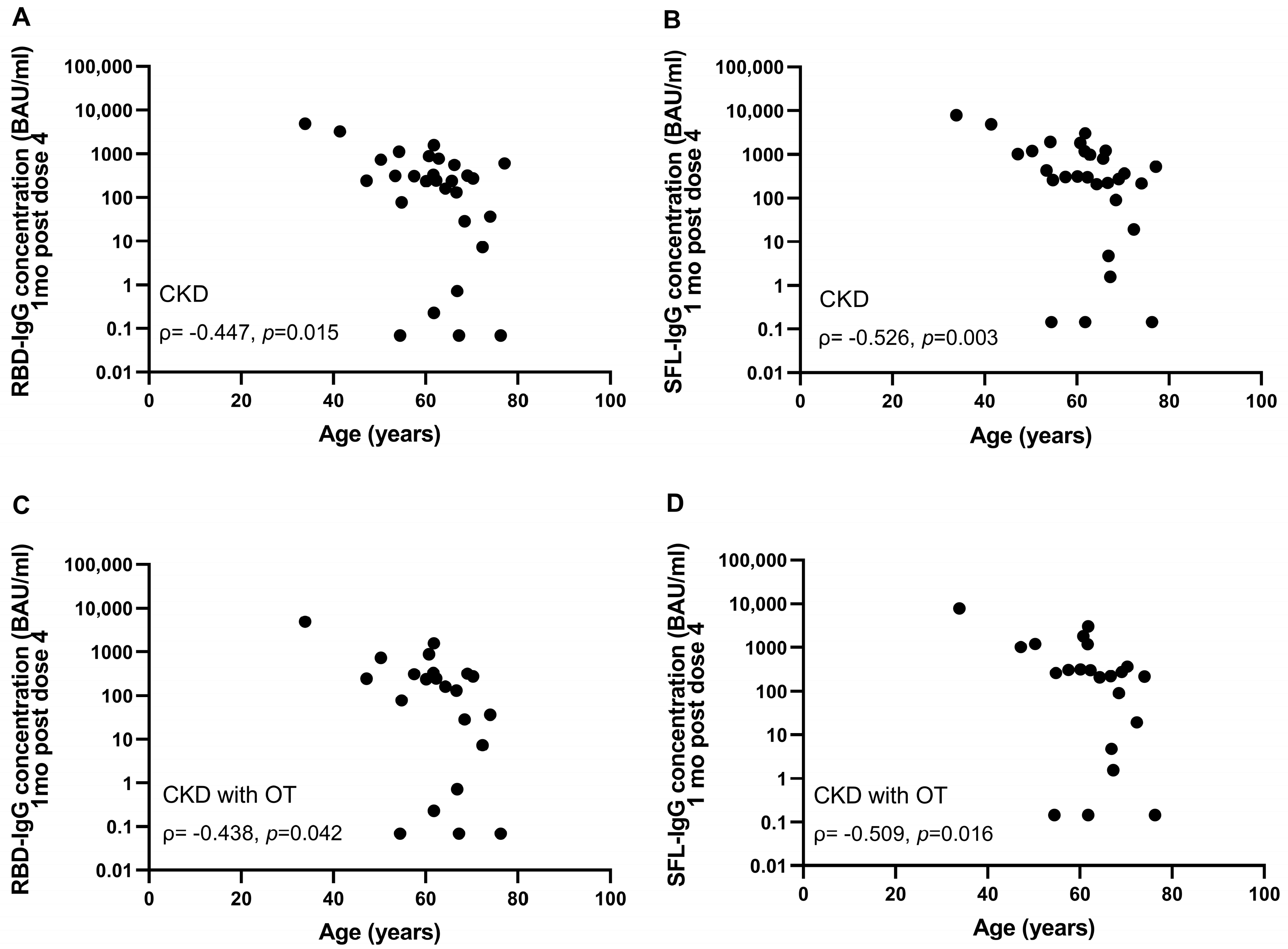
3.2. Impact of Different Factors on Antibody Levels after the Fourth Dose
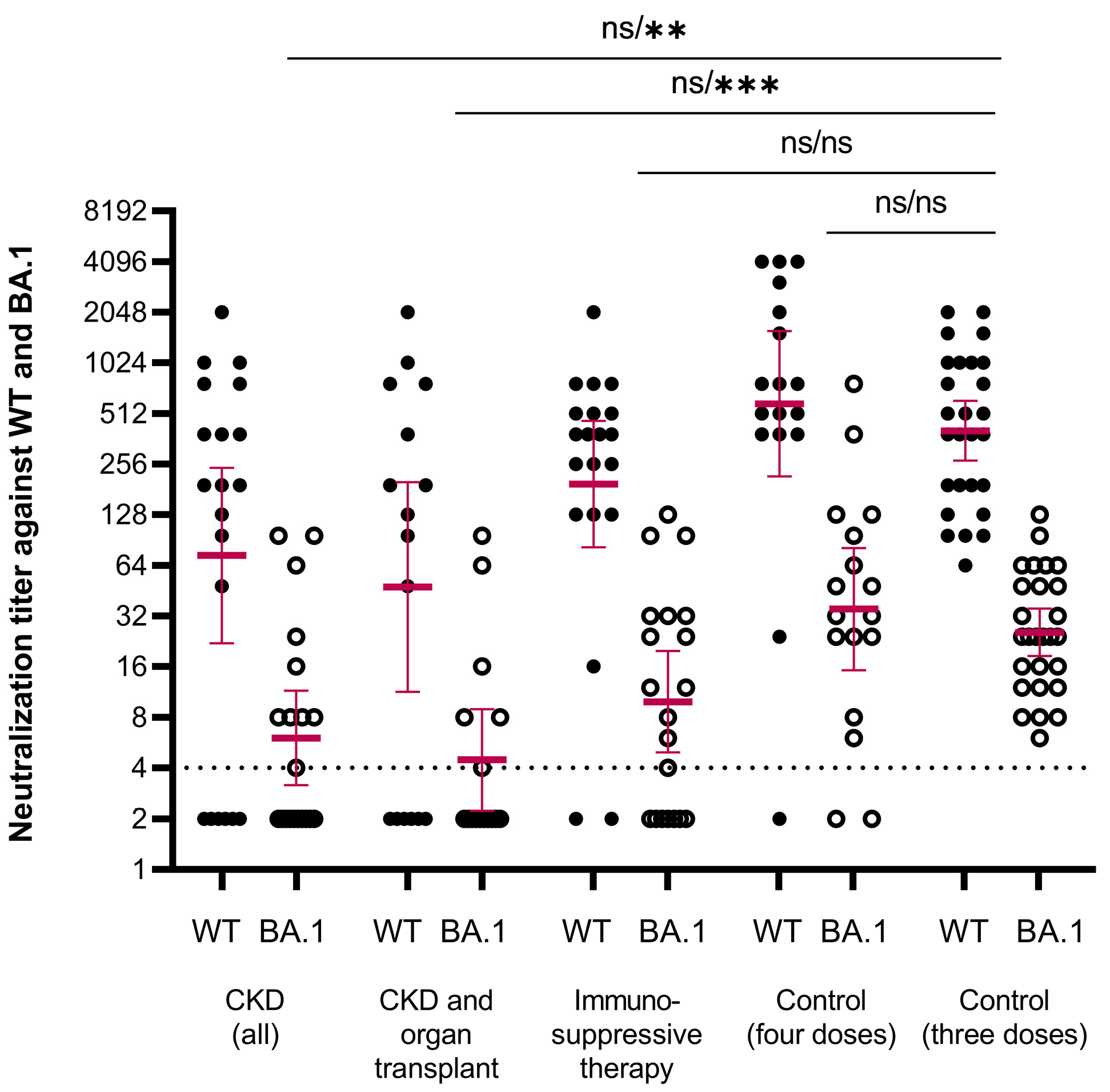
3.3. Antibody Levels and NAbs after Third Dose in Healthy Controls
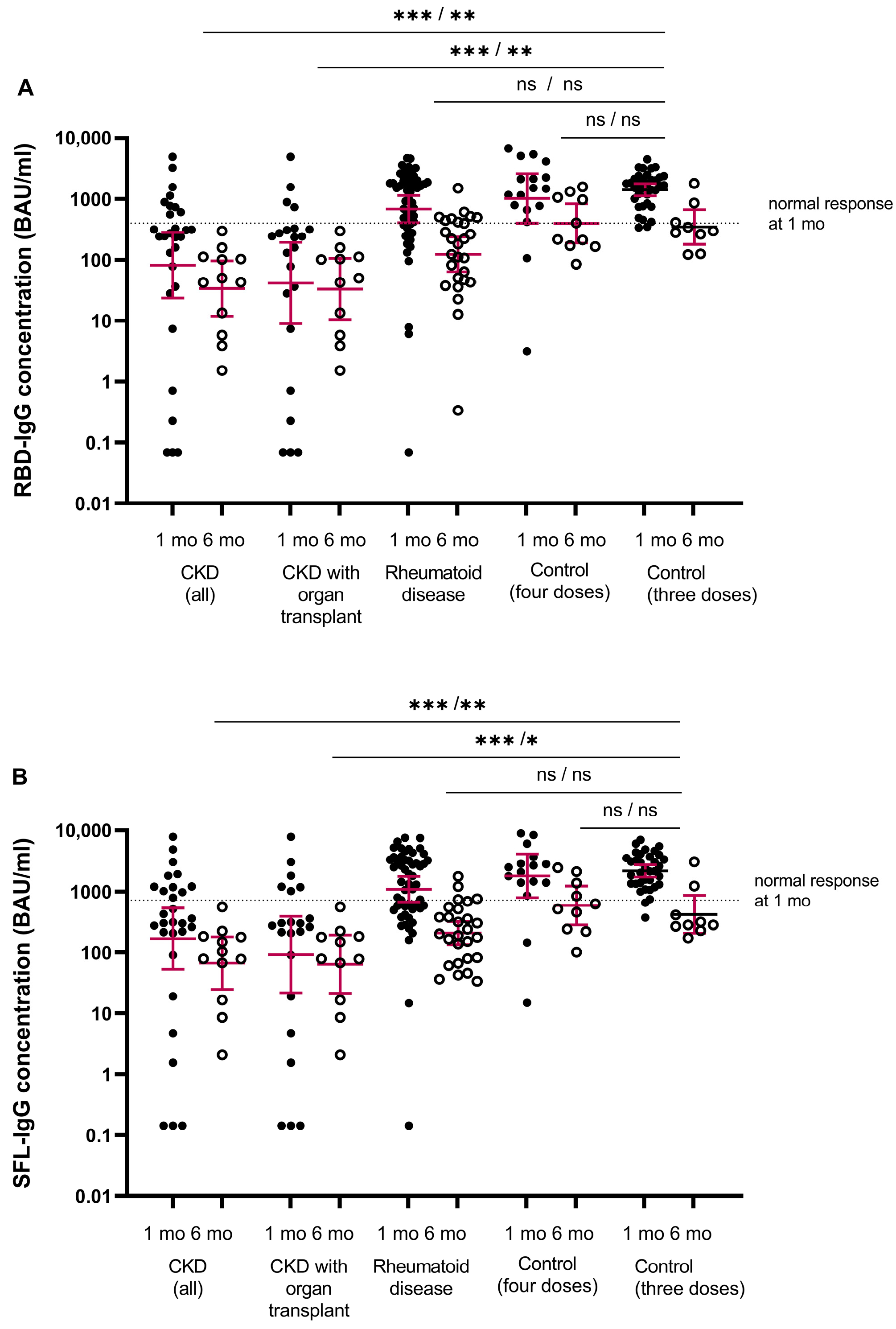
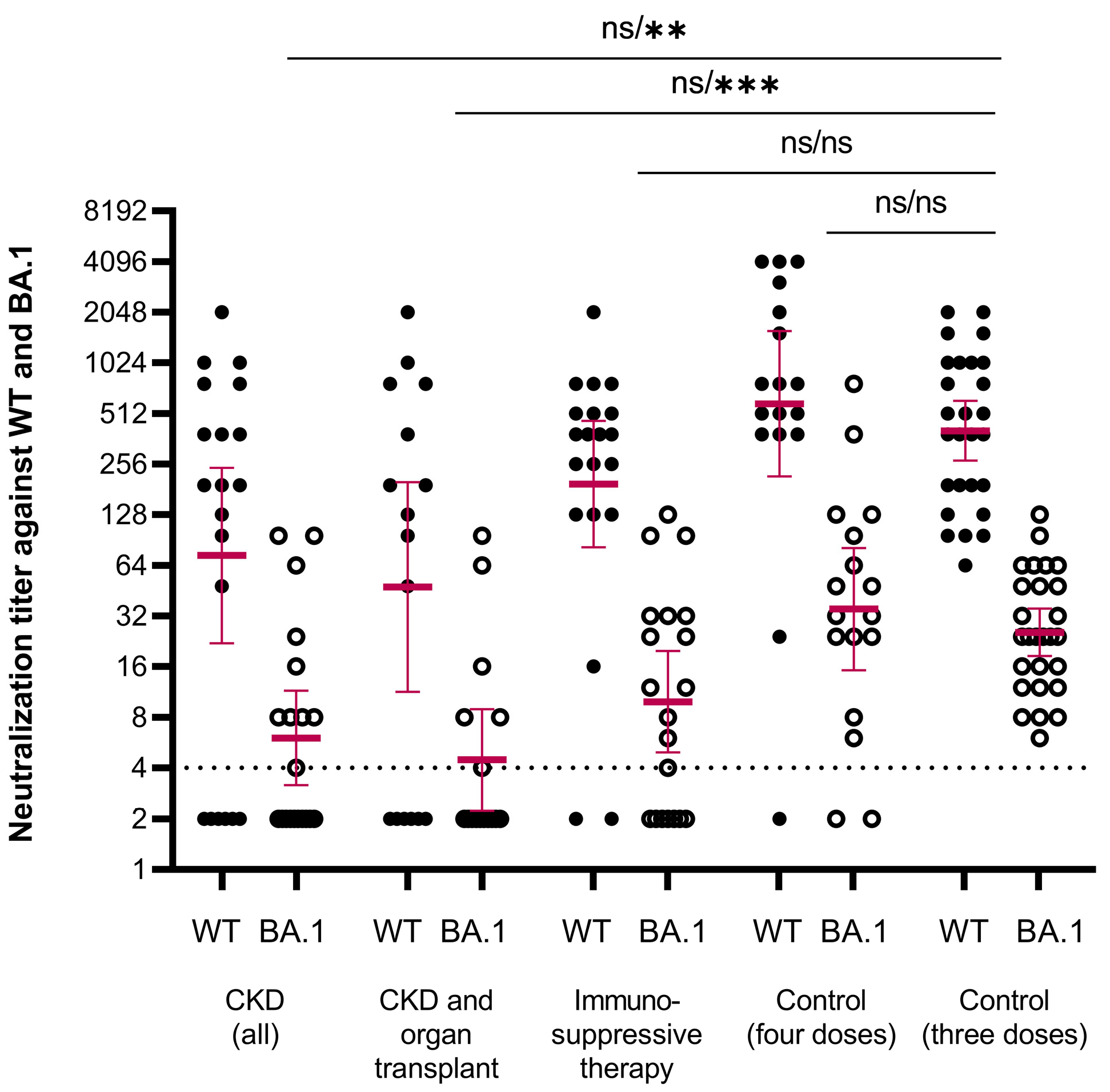
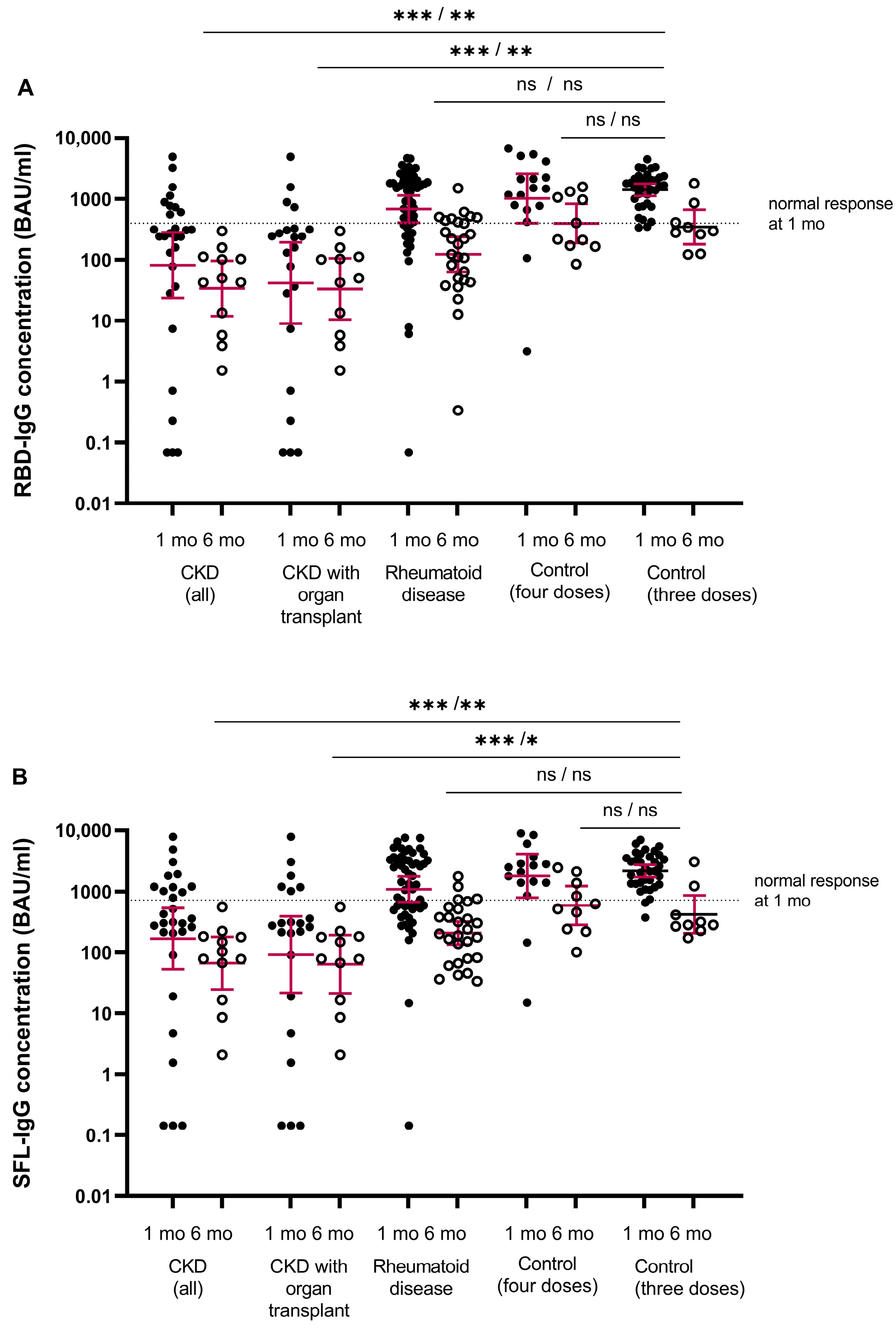
3.4. Antibody Levels and NAbs One Month after the Fourth Dose by Disease Groups
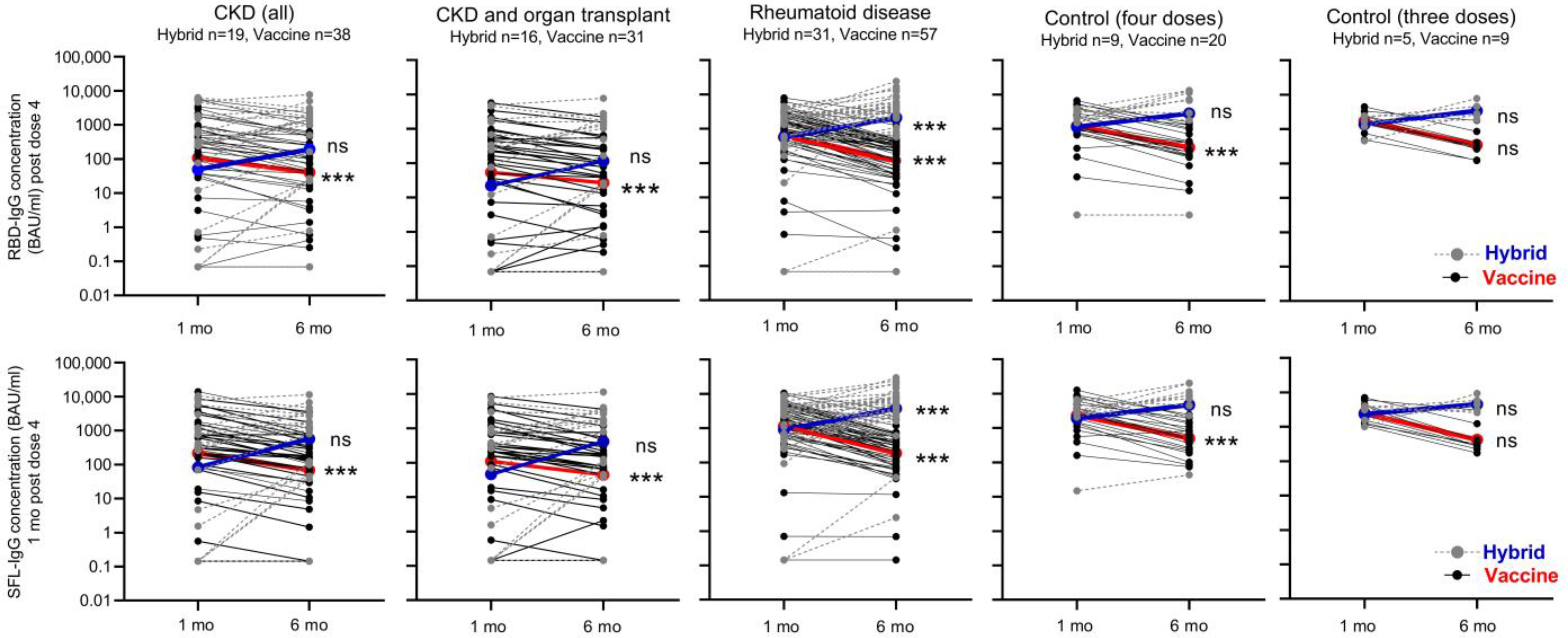
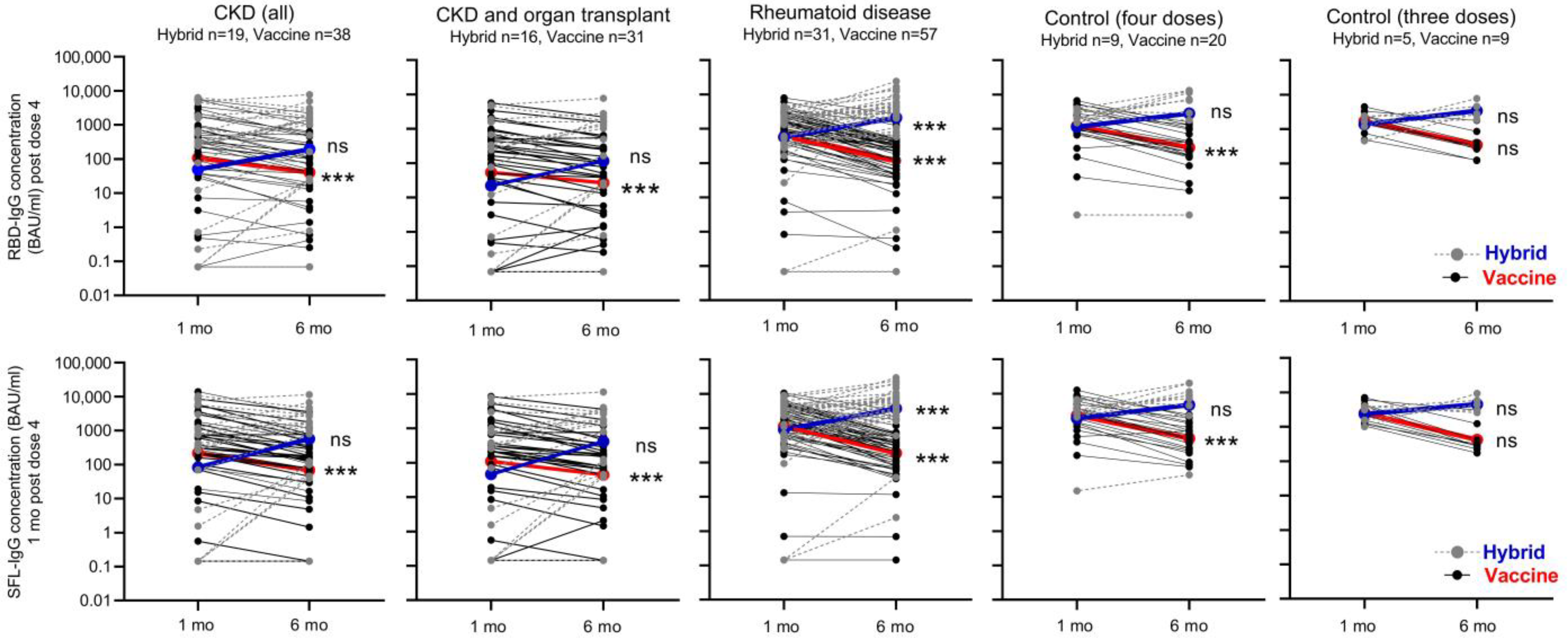
3.5. Antibody Levels Six Months after the Booster Dose in Participants with and without Infection
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Williamson, E.J.; Walker, A.J.; Bhaskaran, K.; Bacon, S.; Bates, C.; Morton, C.E.; Curtis, H.J.; Mehrkar, A.; Evans, D.; Inglesby, P.; et al. Factors associated with COVID-19-related death using OpenSAFELY. Nature 2020, 584, 430–436. [Google Scholar] [CrossRef] [PubMed]
- Semenzato, L.; Botton, J.; Drouin, J.; Baricault, B.; Bertrand, M.; Jabagi, M.-J.; Cuenot, F.; Vu, S.L.; Dray-Spira, R.; Weill, A.; et al. Characteristics associated with the residual risk of severe COVID-19 after a complete vaccination schedule: A cohort study of 28 million people in France. Lancet Reg. Health Eur. 2022, 19, 100441. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.A.; Dube, S.; Lu, Y.; Yates, M.; Arnetorp, S.; Barnes, E.; Bell, S.; Carty, L.; Evans, K.; Graham, S.; et al. Impact of COVID-19 on immunocompromised populations during the Omicron era: Insights from the observational population-based INFORM study. Lancet Reg. Health Eur. 2023, 35, 100747. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.R.Y.B.; Wong, S.Y.; Chai, L.Y.A.; Lee, S.C.; Lee, M.X.; Muthiah, M.D.; Tay, S.H.; Teo, C.B.; Tan, B.K.J.; Chan, Y.H.; et al. Efficacy of COVID-19 vaccines in immunocompromised patients: Systematic review and meta-analysis. BMJ 2022, 376, e068632. [Google Scholar] [CrossRef] [PubMed]
- Widhani, A.; Hasibuan, A.S.; Rismawati, R.; Maria, S.; Koesnoe, S.; Hermanadi, M.I.; Ophinni, Y.; Yamada, C.; Harimurti, K.; Sari, A.N.L.; et al. Efficacy, Immunogenicity, and Safety of COVID-19 Vaccines in Patients with Autoimmune Diseases: A Systematic Review and Meta-Analysis. Vaccines 2023, 11, 1456. [Google Scholar] [CrossRef] [PubMed]
- Ehmsen, S.; Asmussen, A.; Jeppesen, S.S.; Nilsson, A.C.; Østerlev, S.; Vestergaard, H.; Justesen, U.S.; Johansen, I.S.; Frederiksen, H.; Ditzel, H.J. Antibody and T cell immune responses following mRNA COVID-19 vaccination in patients with cancer. Cancer Cell 2021, 39, 1034–1036. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.-S.F.; Messchendorp, A.L.; de Vries, R.D.; Baan, C.C.; van Baarle, D.; van Binnendijk, R.; Diavatopoulos, D.A.; Geers, D.; Schmitz, K.S.; GeurtsvanKessel, C.H.; et al. Antibody and T-Cell Responses 6 Months After Coronavirus Disease 2019 Messenger RNA-1273 Vaccination in Patients with Chronic Kidney Disease, on Dialysis, or Living with a Kidney Transplant. Clin. Infect. Dis. 2023, 76, e188–e199. [Google Scholar] [CrossRef]
- Andrews, N.; Stowe, J.; Kirsebom, F.; Toffa, S.; Sachdeva, R.; Gower, C.; Ramsay, M.; Lopez Bernal, J. Effectiveness of COVID-19 booster vaccines against COVID-19-related symptoms, hospitalization and death in England. Nat. Med. 2022, 28, 831–837. [Google Scholar] [CrossRef]
- Andrews, N.; Tessier, E.; Stowe, J.; Gower, C.; Kirsebom, F.; Simmons, R.; Gallagher, E.; Thelwall, S.; Groves, N.; Dabrera, G.; et al. Duration of Protection against Mild and Severe Disease by COVID-19 Vaccines. N. Engl. J. Med. 2022, 386, 340–350. [Google Scholar] [CrossRef]
- Marra, A.R.; Kobayashi, T.; Suzuki, H.; Alsuhaibani, M.; Hasegawa, S.; Tholany, J.; Perencevich, E.; Maezato, A.M.; Ricardo, V.C.V.; Salinas, J.L.; et al. The effectiveness of coronavirus disease 2019 (COVID-19) vaccine in the prevention of post-COVID-19 conditions: A systematic literature review and meta-analysis. Antimicrob. Steward. Healthc. Epidemiol. 2022, 2, e192. [Google Scholar] [CrossRef]
- Tan, T.T.; Ng, H.J.; Young, B.; Khan, B.A.; Shetty, V.; Azmi, N.; Clissold, S. Effectiveness of vaccination against SARS-CoV-2 and the need for alternative preventative approaches in immunocompromised individuals: A narrative review of systematic reviews. Expert Rev. Vaccines 2023, 22, 341–365. [Google Scholar] [CrossRef] [PubMed]
- Boyarsky, B.J.; Werbel, W.A.; Avery, R.K.; Tobian, A.A.R.; Massie, A.B.; Segev, D.L.; Garonzik-Wang, J.M. Antibody Response to 2-Dose SARS-CoV-2 mRNA Vaccine Series in Solid Organ Transplant Recipients. JAMA 2021, 325, 2204–2206. [Google Scholar] [CrossRef] [PubMed]
- Interim Recommendations for an Extended Primary Series with an Additional Vaccine Dose for COVID-19 Vaccination in Immunocompromised Persons. Available online: https://www.who.int/publications/i/item/WHO-2019-nCoV-vaccines-SAGE_recommendation-immunocompromised-persons (accessed on 21 December 2023).
- Salo, H.; Lehtonen, T.; Auranen, K.; Baum, U.; Leino, T. Predictors of hospitalisation and death due to SARS-CoV-2 infection in Finland: A population-based register study with implications to vaccinations. Vaccine 2022, 40, 3345–3355. [Google Scholar] [CrossRef]
- THL Recommends That Third Doses of the Corona Vaccine Start to be Offered to All 18-Year-Olds 5-6 Months after the Second Dose. Available online: https://thl.fi/-/thl-suosittelee-etta-kolmansia-koronarokoteannoksia-aletaan-tarjota-kaikille-18-vuotta-tayttaneille-5-6-kuukautta-toisesta-annoksesta (accessed on 20 December 2023).
- Solastie, A.; Nieminen, T.; Ekström, N.; Nohynek, H.; Lehtonen, L.; Palmu, A.A.; Melin, M. Changes in SARS-CoV-2 seroprevalence and population immunity in Finland, 2020–2022. Emerg. Microbes Infect. 2023, 12, 2222849. [Google Scholar] [CrossRef] [PubMed]
- Kurhade, C.; Zou, J.; Xia, H.; Liu, M.; Chang, H.C.; Ren, P.; Xie, X.; Shi, P.-Y. Low neutralization of SARS-CoV-2 Omicron BA.2.75.2, BQ.1.1 and XBB.1 by parental mRNA vaccine or a BA.5 bivalent booster. Nat. Med. 2023, 29, 344–347. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Iketani, S.; Li, Z.; Liu, L.; Guo, Y.; Huang, Y.; Bowen, A.D.; Liu, M.; Wang, M.; Yu, J.; et al. Alarming antibody evasion properties of rising SARS-CoV-2 BQ and XBB subvariants. Cell 2023, 186, 279–286.e8. [Google Scholar] [CrossRef]
- THL Instructs Municipalities to Offer Third Vaccine Doses to People with Severe Immune Deficiency. Available online: https://thl.fi/-/thl-ohjeistaa-kuntia-tarjoamaan-kolmansia-rokoteannoksia-voimakkaasti-immuunipuutteisille (accessed on 21 December 2023).
- THL Recommends Fourth Vaccine Doses to People with Severe Immune Deficiency. Available online: https://thl.fi/fi/-/thl-suosittelee-vakavasti-immuunipuutteisille-neljatta-koronarokoteannosta (accessed on 21 December 2023).
- THL Has Instructed Municipalities on the 3rd Corona Vaccine Doses for Those Vaccinated with a Short Dose Interval—The Third Dose Not Yet for Men under 30. Available online: https://thl.fi/-/thl-ohjeistanut-kuntia-lyhyella-annosvalilla-rokotettujen-3.-koronarokoteannoksista-kolmatta-annosta-ei-viela-alle-30-vuotiaille-miehille (accessed on 21 December 2023).
- THL Recommends Third Doses of COVID-19 Vaccine for Those Treating Corona Patients and Other Critical Care Staff. Available online: https://thl.fi/-/thl-suosittelee-kolmansia-koronarokoteannoksia-koronapotilaita-hoitaville-seka-muulle-kriittisen-hoidon-henkilokunnalle (accessed on 20 December 2023).
- Solastie, A.; Virta, C.; Haveri, A.; Ekström, N.; Kantele, A.; Miettinen, S.; Lempainen, J.; Jalkanen, P.; Kakkola, L.; Dub, T.; et al. A Highly Sensitive and Specific SARS-CoV-2 Spike- and Nucleoprotein-Based Fluorescent Multiplex Immunoassay (FMIA) to Measure IgG, IgA, and IgM Class Antibodies. Microbiol. Spectr. 2021, 9, e0113121. [Google Scholar] [CrossRef]
- Establishment of the WHO International Standard and Reference Panel for Anti-SARS-CoV-2 Antibody. WHO/BS/20202402. Available online: https://www.who.int/publications/m/item/WHO-BS-2020.2403 (accessed on 21 December 2023).
- Haveri, A.; Smura, T.; Kuivanen, S.; Österlund, P.; Hepojoki, J.; Ikonen, N.; Pitkäpaasi, M.; Blomqvist, S.; Rönkkö, E.; Kantele, A.; et al. Serological and molecular findings during SARS-CoV-2 infection: The first case study in Finland, January to February 2020. Eurosurveillance 2020, 25, 2000266. [Google Scholar] [CrossRef]
- Haveri, A.; Ekström, N.; Solastie, A.; Virta, C.; Österlund, P.; Isosaari, E.; Nohynek, H.; Palmu, A.A.; Melin, M. Persistence of neutralizing antibodies a year after SARS-CoV-2 infection in humans. Eur. J. Immunol. 2021, 51, 3202–3213. [Google Scholar] [CrossRef]
- Haveri, A.; Solastie, A.; Ekström, N.; Österlund, P.; Nohynek, H.; Nieminen, T.; Palmu, A.A.; Melin, M. Neutralizing antibodies to SARS-CoV-2 Omicron variant after third mRNA vaccination in health care workers and elderly subjects. Eur. J. Immunol. 2022, 52, 816–824. [Google Scholar] [CrossRef]
- Genomic Surveillance of SARS-CoV-2. Available online: https://thl.fi/en/web/infectious-diseases-and-vaccinations/what-s-new/coronavirus-covid-19-latest-updates/coronavirus-variants/genomic-surveillance-of-sars-cov-2 (accessed on 21 December 2023).
- Rusanen, J.; Kareinen, L.; Szirovicza, L.; Uğurlu, H.; Levanov, L.; Jääskeläinen, A.; Ahava, M.; Kurkela, S.; Saksela, K.; Hedman, K.; et al. A Generic, Scalable, and Rapid Time-Resolved Förster Resonance Energy Transfer-Based Assay for Antigen Detection-SARS-CoV-2 as a Proof of Concept. mBio 2021, 12, e00902-21. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, C.M.; Polson, N.G.; Scott, J.G. Handling Sparsity via the Horseshoe. In Proceedings of the 12th International Conference on Artificial Intelligence and Statistics (AISTATS) 2009, Clearwater Beach, FL, USA, 16–18 April 2009; Volume 5. [Google Scholar]
- THL Recommends Offering the Third Dose of the Corona Vaccine to People over 60 and Medical Risk Groups. Available online: https://thl.fi/-/thl-suosittelee-kolmannen-koronarokoteannoksen-tarjoamista-60-vuotta-tayttaneille-ja-laaketieteellisille-riskiryhmille (accessed on 21 December 2023).
- Bobrovitz, N.; Ware, H.; Ma, X.; Li, Z.; Hosseini, R.; Cao, C.; Selemon, A.; Whelan, M.; Premji, Z.; Issa, H.; et al. Protective effectiveness of previous SARS-CoV-2 infection and hybrid immunity against the omicron variant and severe disease: A systematic review and meta-regression. Lancet Infect. Dis. 2023, 23, 556–567. [Google Scholar] [CrossRef]
- Abebe, E.C.; Dejenie, T.A. Protective roles and protective mechanisms of neutralizing antibodies against SARS-CoV-2 infection and their potential clinical implications. Front. Immunol. 2023, 14, 1055457. [Google Scholar] [CrossRef] [PubMed]
- Sanders, J.-S.F.; Bemelman, F.J.; Messchendorp, A.L.; Baan, C.C.; van Baarle, D.; van Binnendijk, R.; Diavatopoulos, D.A.; Frölke, S.C.; Geers, D.; GeurtsvanKessel, C.H.; et al. The RECOVAC Immune-response Study: The Immunogenicity, Tolerability, and Safety of COVID-19 Vaccination in Patients with Chronic Kidney Disease, on Dialysis, or Living with a Kidney Transplant. Transplantation 2022, 106, 821–834. [Google Scholar] [CrossRef] [PubMed]
- Bouwmans, P.; Messchendorp, A.L.; Imhof, C.; Sanders, J.-S.F.; Hilbrands, L.B.; Reinders, M.E.J.; Vart, P.; Bemelman, F.J.; Abrahams, A.C.; van den Dorpel, R.M.A.; et al. Impact of immunosuppressive treatment and type of SARS-CoV-2 vaccine on antibody levels after three vaccinations in patients with chronic kidney disease or kidney replacement therapy. Clin. Kidney J. 2022, 16, 528–540. [Google Scholar] [CrossRef]
- Simader, E.; Tobudic, S.; Mandl, P.; Haslacher, H.; Perkmann, T.; Nothnagl, T.; Sautner, J.; Radner, H.; Winkler, F.; Burgmann, H.; et al. Importance of the second SARS-CoV-2 vaccination dose for achieving serological response in patients with rheumatoid arthritis and seronegative spondyloarthritis. Ann. Rheum. Dis. 2022, 81, 416–421. [Google Scholar] [CrossRef]
- Mandl, P.; Tobudic, S.; Haslacher, H.; Karonitsch, T.; Mrak, D.; Nothnagl, T.; Perkmann, T.; Radner, H.; Sautner, J.; Simader, E.; et al. Response to SARS-CoV-2 vaccination in systemic autoimmune rheumatic disease depends on immunosuppressive regimen: A matched, prospective cohort study. Ann. Rheum. Dis. 2022, 81, 1017–1022. [Google Scholar] [CrossRef]
- Corradini, P.; Agrati, C.; Apolone, G.; Mantovani, A.; Giannarelli, D.; Marasco, V.; Bordoni, V.; Sacchi, A.; Matusali, G.; Salvarani, C.; et al. Humoral and T-Cell Immune Response After 3 Doses of Messenger RNA Severe Acute Respiratory Syndrome Coronavirus 2 Vaccines in Fragile Patients: The Italian VAX4FRAIL Study. Clin. Infect. Dis. 2023, 76, e426–e438. [Google Scholar] [CrossRef]
- Tobudic, S.; Simader, E.; Deimel, T.; Straub, J.; Kartnig, F.; Heinz, L.X.; Mandl, P.; Haslacher, H.; Perkmann, T.; Schneider, L.; et al. The accelerated waning of immunity and reduced effect of booster in patients treated with bDMARD and tsDMARD after SARS-CoV-2 mRNA vaccination. Front. Med. 2023, 10, 1049157. [Google Scholar] [CrossRef]
- Kartnig, F.; Mrak, D.; Simader, E.; Tobudic, S.; Radner, H.; Mandl, P.; Göschl, L.; Hommer, N.; Mayer, M.; Hofer, P.; et al. Safety and immunogenicity of a third COVID-19 vaccination in patients with immune-mediated inflammatory diseases compared with healthy controls. Ann. Rheum. Dis. 2023, 82, 292–300. [Google Scholar] [CrossRef]
- Tillmann, F.-P.; Figiel, L.; Ricken, J.; Still, H.; Korte, C.; Plaßmann, G.; Harth, A.; Jörres, A.; von Landenberg, P. Effect of Third and Fourth mRNA-Based Booster Vaccinations on SARS-CoV-2 Neutralizing Antibody Titer Formation, Risk Factors for Non-Response, and Outcome after SARS-CoV-2 Omicron Breakthrough Infections in Patients on Chronic Hemodialysis: A Prospective Multicenter Cohort Study. J. Clin. Med. 2022, 11, 3187. [Google Scholar] [CrossRef] [PubMed]
- Poli, M.C.; Vial, C.; Rey-Jurado, E.; González, N.; Cortés, L.J.; Hormazabal, J.; Ramírez-Riffo, C.; de la Cruz, J.; Ulloa, C. A Third Dose of SARS-CoV-2 mRNA Vaccine Improves Immune Response in Chronic Kidney Disease Patients. Vaccines 2023, 11, 1012. [Google Scholar] [CrossRef] [PubMed]
- Westhoff, T.H.; Seibert, F.S.; Anft, M.; Blazquez-Navarro, A.; Skrzypczyk, S.; Zgoura, P.; Meister, T.L.; Pfaender, S.; Stumpf, J.; Hugo, C.; et al. A third vaccine dose substantially improves humoral and cellular SARS-CoV-2 immunity in renal transplant recipients with primary humoral nonresponse. Kidney Int. 2021, 100, 1135–1136. [Google Scholar] [CrossRef] [PubMed]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Orero, E.; Tejedor, S.; Mantecón, C.J.J.; Gómez Pérez, V.O.; Marín Franco, A.J.; Alfaro Sánchez, C.; Puerta Carretero, M.; et al. Humoral Response to Third Dose of SARS-CoV-2 Vaccines in the CKD Spectrum. Clin. J. Am. Soc. Nephrol. 2022, 17, 872–876. [Google Scholar] [CrossRef] [PubMed]
- Quiroga, B.; Soler, M.J.; Ortiz, A.; Jarava Mantecón, C.J.; Gomes Pérez, V.O.; Bordils, A.; Lacueva, J.; Marin Franco, A.J.; Delgado Conde, P.; Muñoz Ramos, P.; et al. Humoral response after the fourth dose of the SARS-CoV-2 vaccine in the CKD spectrum: A prespecified analysis of the SENCOVAC study. Nephrol. Dial. Transplant. 2023, 38, 969–981. [Google Scholar] [CrossRef] [PubMed]
- Bertrand, D.; Lemée, V.; Laurent, C.; Lemoine, M.; Hanoy, M.; Le Roy, F.; Nezam, D.; Pruteanu, D.; Lebourg, L.; Grange, S.; et al. Waning antibody response and cellular immunity 6 months after third dose SARS-Cov-2 mRNA BNT162b2 vaccine in kidney transplant recipients. Am. J. Transplant. 2022, 22, 1498–1500. [Google Scholar] [CrossRef]
- ECDC and EMA Update Recommendations on Additional Booster Doses of COVID-19 Vaccines. Available online: https://www.ecdc.europa.eu/en/news-events/ecdc-and-ema-update-recommendations-additional-booster-doses-covid-19-vaccines (accessed on 21 December 2023).
- Martinelli, S.; Pascucci, D.; Laurenti, P. Humoral response after a fourth dose of SARS-CoV-2 vaccine in immunocompromised patients. Results of a systematic review. Front. Public Health 2023, 11, 1108546. [Google Scholar] [CrossRef]
- Bjørlykke, K.H.; Ørbo, H.S.; Tveter, A.T.; Jyssum, I.; Sexton, J.; Tran, T.T.; Christensen, I.E.; Kro, G.B.; Kvien, T.K.; Jahnsen, J.; et al. Four SARS-CoV-2 vaccine doses or hybrid immunity in patients on immunosuppressive therapies: A Norwegian cohort study. Lancet Rheumatol. 2023, 5, e36–e46. [Google Scholar] [CrossRef]
- Rescigno, M.; Agrati, C.; Salvarani, C.; Giannarelli, D.; Costantini, M.; Mantovani, A.; Massafra, R.; Zinzani, P.L.; Morrone, A.; Notari, S.; et al. Neutralizing antibodies to Omicron after the fourth SARS-CoV-2 mRNA vaccine dose in immunocompromised patients highlight the need of additional boosters. Front. Immunol. 2023, 14, 1104124. [Google Scholar] [CrossRef]
- Nazaruk, P.; Tkaczyk, I.; Monticolo, M.; Jędrzejczak, A.M.; Krata, N.; Pączek, L.; Foroncewicz, B.; Mucha, K. Hybrid Immunity Provides the Best COVID-19 Humoral Response in Immunocompromised Patients with or without SARS-CoV-2 Infection History. Vaccines 2023, 11, 1380. [Google Scholar] [CrossRef]
- Gilbert, P.B.; Montefiori, D.C.; McDermott, A.B.; Fong, Y.; Benkeser, D.; Deng, W.; Zhou, H.; Houchens, C.R.; Martins, K.; Jayashankar, L.; et al. Immune correlates analysis of the mRNA-1273 COVID-19 vaccine efficacy clinical trial. Science 2022, 375, 43–50. [Google Scholar] [CrossRef] [PubMed]
- Khoury, D.S.; Cromer, D.; Reynaldi, A.; Schlub, T.E.; Wheatley, A.K.; Juno, J.A.; Subbarao, K.; Kent, S.J.; Triccas, J.A.; Davenport, M.P.; et al. Neutralizing antibody levels are highly predictive of immune protection from symptomatic SARS-CoV-2 infection. Nat. Med. 2021, 27, 1205–1211. [Google Scholar] [CrossRef] [PubMed]
- Hurme, A.; Jalkanen, P.; Marttila-Vaara, M.; Heroum, J.; Jokinen, H.; Vara, S.; Liedes, O.; Lempainen, J.; Melin, M.; Julkunen, I.; et al. T cell immunity following COVID-19 vaccination in adult patients with primary antibody deficiency–A 22-month follow-up. Front. Immunol. 2023, 14, 1146500. [Google Scholar] [CrossRef] [PubMed]
- van Leeuwen, L.P.M.; Grobben, M.; GeurtsvanKessel, C.H.; Ellerbroek, P.M.; de Bree, G.J.; Potjewijd, J.; Rutgers, A.; Jolink, H.; van de Veerdonk, F.L.; van Gils, M.J.; et al. Immune Responses 6 Months After mRNA-1273 COVID-19 Vaccination and the Effect of a Third Vaccination in Patients with Inborn Errors of Immunity. J. Clin. Immunol. 2023, 43, 1104–1117. [Google Scholar] [CrossRef]
- Azzolini, E.; Pozzi, C.; Germagnoli, L.; Oresta, B.; Carriglio, N.; Calleri, M.; Selmi, C.; De Santis, M.; Finazzi, S.; Carlo-Stella, C.; et al. mRNA COVID-19 vaccine booster fosters B- and T-cell responses in immunocompromised patients. Life Sci. Alliance 2022, 5, e202201381. [Google Scholar] [CrossRef]
- Regev-Yochay, G.; Gonen, T.; Gilboa, M.; Mandelboim, M.; Indenbaum, V.; Amit, S.; Meltzer, L.; Asraf, K.; Cohen, C.; Fluss, R.; et al. Efficacy of a Fourth Dose of COVID-19 mRNA Vaccine against Omicron. N. Engl. J. Med. 2022, 386, 1377–1380. [Google Scholar] [CrossRef]
- Parry, H.; Bruton, R.; Stephens, C.; Bentley, C.; Brown, K.; Amirthalingam, G.; Hallis, B.; Otter, A.; Zuo, J.; Moss, P.; et al. Extended interval BNT162b2 vaccination enhances peak antibody generation. NPJ Vaccines 2022, 7, 14. [Google Scholar] [CrossRef]
- Bates, T.A.; Leier, H.C.; McBride, S.K.; Schoen, D.; Lyski, Z.L.; Lee, D.X.; Messer, W.B.; Curlin, M.E.; Tafesse, F.G. An extended interval between vaccination and infection enhances hybrid immunity against SARS-CoV-2 variants. JCI Insight 2023, 8, e165265. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Demographics, Vaccination, and Infection Status | All Immunocompromised Participants | Chronic Kidney Disease, All | Chronic Kidney Disease and Organ Transplantation | Rheumatoid Disease | Controls (Four Vaccine Doses) | Controls (Three Vaccine Doses) | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Any COVID-19 vaccines n | 488 | 85 | 66 | 122 | 38 | 35 | ||||||
| Age, years, median (IQR) | 64.3 | (52.1–69.4) | 66.7 | (60.2–71.0) | 66.9 | (61.6–70.6) | 59.4 | (45.4–67.0) | 61.0 | (47.9–67.6) | 45.0 | (36.5–55.6) |
| Female n (%) | 285 | (58.4) | 42 | (49.4) | 31 | (47.0) | 89 | (73.6) | 27 | (71.1) | 30 | (85.7) |
| Male n (%) | 203 | (41.6) | 43 | (50.6) | 35 | (53.0) | 32 | (26.4) | 11 | (28.9) | 5 | (14.3) |
| No mRNA-1273 vaccine n (%) * | 198 | (40.6) | 29 | (34.1) | 22 | (33.3) | 53 | (43.4) | 17 | (44.7) | 35 | (100) |
| Age, years, median (IQR) | 62.8 | (50.9–67.7) | 62.3 | (54.8–67.2) | 62.1 | (58.2–68.2) | 55.3 | (43.4–66.2) | 63.5 | (50.8–67.7) | 45.0 | (36.5–55.6) |
| Female n (%) | 119 | (60.1) | 16 | (55.2) | 12 | (54.5) | 38 | (71.1) | 12 | (70.6) | 30 | (85.7) |
| Male n (%) | 79 | (39.9) | 13 | (44.8) | 10 | (45.5) | 15 | (28.3) | 5 | (29.4) | 5 | (14.3) |
| No. of risk group classifications (median, IQR) | 3 | (2–4) | 5 | (4–6) | 5 | (4–6) | 1 | (1–2) | 0 | (0) | 0 | (0) |
| First vaccine n (%) | ||||||||||||
| BNT162B2 | 221 | (45.3) | 20 | (23.5) | 12 | (33.3) | 82 | (67.8) | 20 | (52.6) | 17 | (48.6) |
| ChAdOx1 nCoV-19 | 245 | (50.2) | 61 | (71.8) | 51 | (77.3) | 32 | (26.4) | 16 | (42.1) | 18 | (51.4) |
| mRNA-1273 | 22 | (4.5) | 4 | (4.7) | 3 | (4.5) | 7 | (5.8) | 2 | (5.3) | 0 | (0) |
| Second vaccine n (%) | ||||||||||||
| BNT162B2 | 323 | (66.2) | 45 | (52.9) | 31 | (47.0) | 94 | (77.7) | 27 | (71.1) | 35 | (100) |
| ChAdOx1 nCoV-19 | 123 | (25.2) | 29 | (34.1) | 26 | (39.4) | 18 | (14.9) | 8 | (21.1) | 0 | (0) |
| mRNA-1273 | 42 | (8.6) | 11 | (12.9) | 9 | (13.6) | 9 | (7.4) | 3 | (7.9) | 0 | (0) |
| Third vaccine n (%) | ||||||||||||
| BNT162B2 | 322 | (66.0) | 46 | (54.1) | 33 | (50.0) | 81 | (66.9) | 27 | (71.1) | 35 | (100) |
| ChAdOx1 nCoV-19 | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) |
| mRNA-1273 | 166 | (34.0) | 39 | (45.9) | 33 | (50.0) | 40 | (33.1) | 11 | (28.9) | 0 | (0) |
| Fourth vaccine n (%) | ||||||||||||
| BNT162B2 | 264 | (54.1) | 43 | (50.6) | 34 | (51.5) | 69 | (57.0) | 21 | (55.3) | 0 | (0) |
| ChAdOx1 nCoV-19 | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) |
| mRNA-1273 | 224 | (45.9) | 42 | (49.4) | 32 | (48.5) | 52 | (43.0) | 17 | (44.7) | 0 | (0) |
| COVID-19 # (hybrid immunity) n/n § (%) | 109/356 | (30.6) | 19/57 | (33.3) | 16/47 | (34.0) | 31/88 | (34.9) | 9/29 | (31.0) | 5/14 | (36) |
| Variable | N | Estimate (SFL-IgG) | 95% CI (SFL-IgG) | Estimate (RBD-IgG) | 95% CI (RBD-IgG) |
|---|---|---|---|---|---|
| Age (in years) | 0.995 | (0.985–1.003) | 0.995 | (0.984–1.003) | |
| Sex—female | 1.001 | (0.874–1.169) | 1.001 | (0.876–1.159) | |
| Vaccine—mRNA-1273 (fourth dose) | 224 | 1.568 | (1.161–2.018) | 1.510 | (1.092–1.968) |
| Cancer under treatment | 149 | 1.088 | (0.954–1.534) | 1.098 | (0.963–1.606) |
| Autoimmune diseases * | 203 | 0.997 | (0.808–1.129) | 0.999 | (0.833–1.149) |
| Organ or stem cell transplant | 113 | 0.993 | (0.764–1.124) | 0.994 | (0.768–1.142) |
| Neurological disease or condition that interferes with breathing | 27 | 1.009 | (0.859–1.463) | 1.013 | (0.879–1.614) |
| Immunosuppressive therapy | 340 | 0.612 | (0.455–0.845) | 0.652 | (0.482–0.940) |
| Type 2 diabetes with drug therapy | 79 | 1.004 | (0.877–1.293) | 1.002 | (0.856–1.264) |
| Type 1 diabetes or adrenal insufficiency | 46 | 0.895 | (0.491–1.059) | 0.878 | (0.474–1.064) |
| Sleep apnea | 68 | 1.032 | (0.926–1.541) | 1.021 | (0.923–1.435) |
| Severe chronic pulmonary disease | 63 | 1.000 | (0.829–1.185) | 0.999 | (0.817–1.196) |
| Severe chronic liver disease | 19 | 1.001 | (0.798–1.393) | 1.006 | (0.838–1.498) |
| Severe chronic kidney disease | 85 | 0.479 | (0.339–0.741) | 0.490 | (0.342–0.787) |
| Severe disorders of the immune system | 21 | 0.991 | (0.631–1.177) | 0.994 | (0.633–1.222) |
| Severe heart diseases e.g heart failure | 166 | 0.990 | (0.771–1.127) | 0.989 | (0.754–1.108) |
| S-IgG % Seropositive (n/n) at 1 mo | S-IgG % with Normal Response (n/n) at 1 mo | NAb % Positive (n/n) WT at 1 mo | NAb % Positive (n/n) BA.1 at 1 mo | RBD-IgG >200 BAU/mL % (n/n) at 1 mo | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| CKD (all) | 83 | (24/29) | 31 *** | (9/29) | 70 * | (14/20) | 45 *** | (9/20) | 45 *** | (13/29) |
| CKD with organ transplant | 77 | (17/22) | 18 *** | (4/22) | 63 * | (10/16) | 38 *** | (6/16) | 50 *** | (11/22) |
| Immunosuppressive therapy/ rheumatoid disease # | 98 | (52/53) | 64 ** | (34/53) | 90 | (18/20) | 60 ** | (12/20) | ||
| 100 | (10/10) | 50 ** | (5/10) | 87 | (46/53) | |||||
| Control (four doses) | 100 | (17/17) | 88 | (15/17) | 94 | (16/17) | 88 | (15/17) | 88 | (15/17) |
| Control (three doses) | 100 | (35/35) | 94 | (33/35) | 100 | (27/27) | 100 | (27/27) | 100 | (35/35) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ekström, N.; Leino, T.M.; Juutinen, A.; Lehtonen, T.; Haveri, A.; Liedes, O.; Vara, S.; Salo, H.; Palmu, A.A.; Nohynek, H.; et al. Hybrid Immunity Improves the Immune Response after the Fourth COVID-19 Vaccine Dose in Individuals with Medical Conditions Predisposing to Severe COVID-19. Vaccines 2024, 12, 247. https://doi.org/10.3390/vaccines12030247
Ekström N, Leino TM, Juutinen A, Lehtonen T, Haveri A, Liedes O, Vara S, Salo H, Palmu AA, Nohynek H, et al. Hybrid Immunity Improves the Immune Response after the Fourth COVID-19 Vaccine Dose in Individuals with Medical Conditions Predisposing to Severe COVID-19. Vaccines. 2024; 12(3):247. https://doi.org/10.3390/vaccines12030247
Chicago/Turabian StyleEkström, Nina, Tuija M. Leino, Aapo Juutinen, Toni Lehtonen, Anu Haveri, Oona Liedes, Saimi Vara, Heini Salo, Arto A. Palmu, Hanna Nohynek, and et al. 2024. "Hybrid Immunity Improves the Immune Response after the Fourth COVID-19 Vaccine Dose in Individuals with Medical Conditions Predisposing to Severe COVID-19" Vaccines 12, no. 3: 247. https://doi.org/10.3390/vaccines12030247
APA StyleEkström, N., Leino, T. M., Juutinen, A., Lehtonen, T., Haveri, A., Liedes, O., Vara, S., Salo, H., Palmu, A. A., Nohynek, H., Martelius, T., & Melin, M. (2024). Hybrid Immunity Improves the Immune Response after the Fourth COVID-19 Vaccine Dose in Individuals with Medical Conditions Predisposing to Severe COVID-19. Vaccines, 12(3), 247. https://doi.org/10.3390/vaccines12030247