
Knowledge, Attitudes, and Practices on COVID-19 Vaccination among General Adult Population in Malawi: A Countrywide Cross-Sectional Survey

 , , ,
, , , 
Abstract
1. Introduction
2. Methodology
2.1. Study Design
2.2. Study Setting and Period
2.3. Target Population
2.4. Sampling Technique and Tools
2.5. Sample Size Calculation
2.6. Data Quality Assurance
2.7. Data Analysis
2.8. Ethical Consideration
3. Results
3.1. Socio-Demographic Characteristics of Study Participants
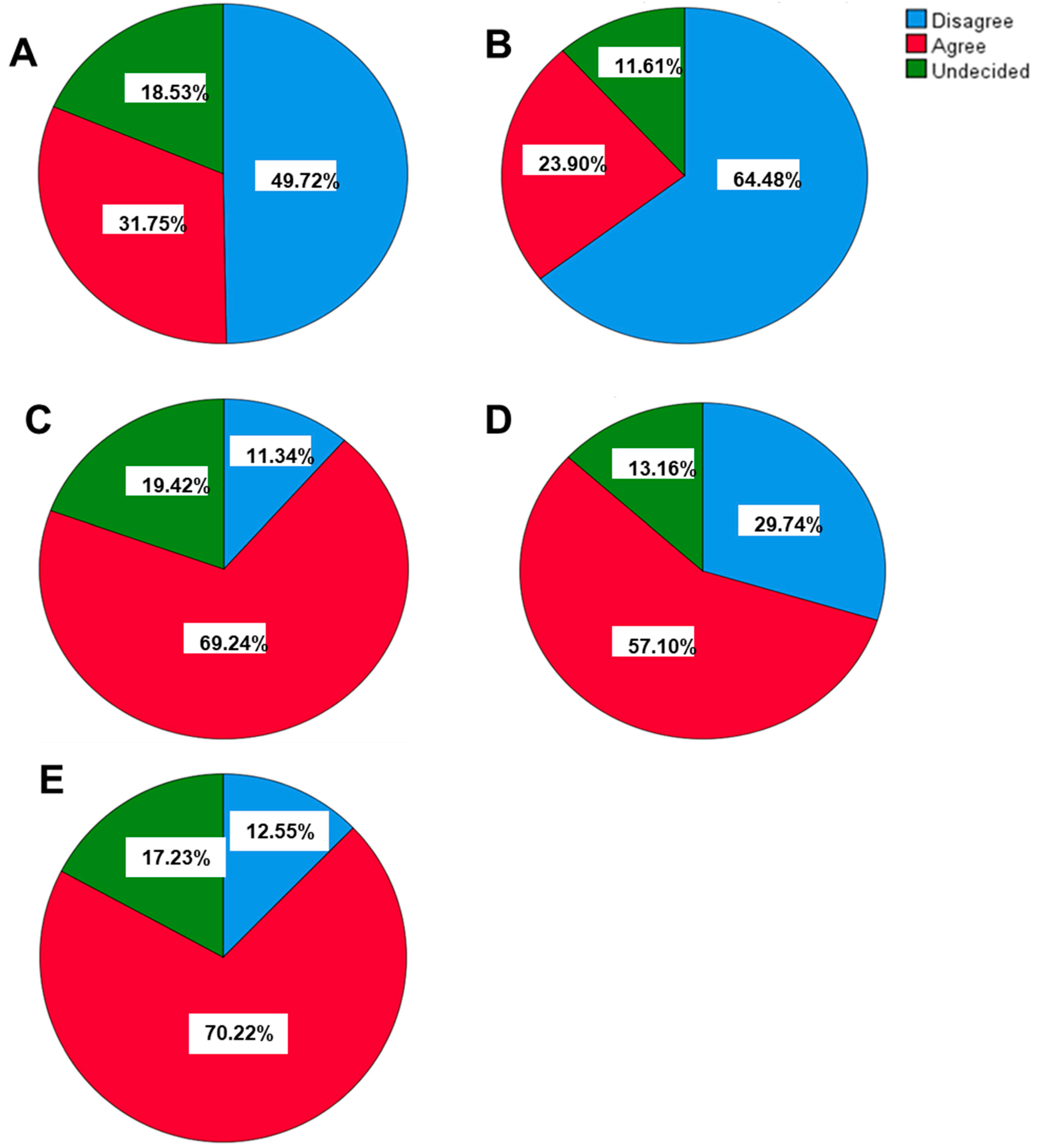
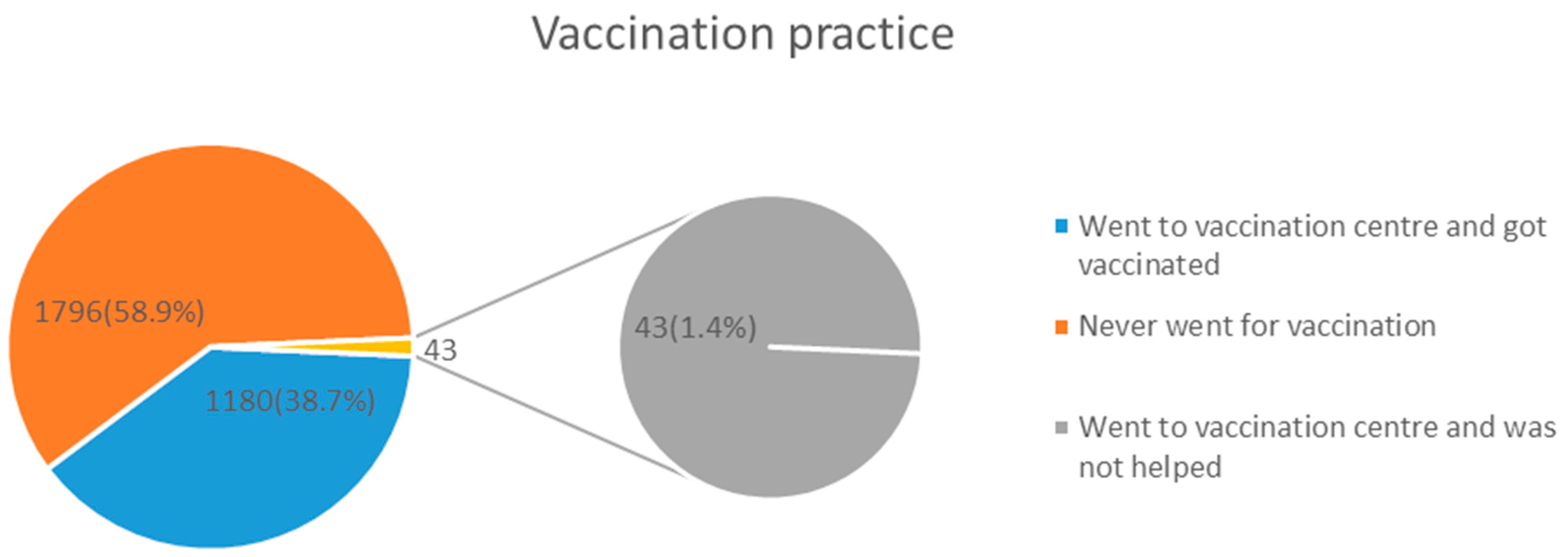
3.2. Knowledge, Attitudes, and Practices of COVID-19 Vaccination
3.3. Factors Influencing Knowledge, Attitudes, and Practices towards Coronavirus Disease 19 Vaccination
4. Discussion
5. Conclusions
6. Recommendations
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Stringhini, S.; Zaballa, M.-E.; Pullen, N.; Perez-Saez, J.; de Mestral, C.; Loizeau, A.J.; Lamour, J.; Pennacchio, F.; Wisniak, A.; Dumont, R.; et al. Seroprevalence of anti-SARS-CoV-2 antibodies 6 months into the vaccination campaign in Geneva, Switzerland, 1 June to 7 July 2021. Euro Surveill. 2021, 26, 1–8. [Google Scholar] [CrossRef]
- WHO. COVID-19 Vaccine Efficacy, Effectiveness and Protection. 2021. Available online: https://www.who.int/news-room/feature-stories/detail/vaccine-efficacy-effectiveness-and-protection (accessed on 1 November 2023).
- Chisale, M.R.O.; Nyambalo, B.W.; Mitambo, C.; Kumwenda, P.; Mwale, S.E.; Mbakaya, B.C. Comparative characterisation of COVID-19 patients with hypertension comorbidity in Malawi: A 1:2 matched retrospective case-control study. IJID Reg. 2022, 2, 25–29. [Google Scholar] [CrossRef]
- Ministry of Health Malawi. COVID-19 Malawi Dashboard. 2022. Available online: https://covid19.health.gov.mw/ (accessed on 31 March 2022).
- World Health Organization. COVID-19 Vaccinations. 2023. Available online: https://covid19.who.int/?mapFilter=vaccinations (accessed on 2 January 2023).
- Reuters. COVID-19 Vaccine Tracker. 2023. Available online: https://www.reuters.com/graphics/world-coronavirus-tracker-and-maps/vaccination-rollout-and-access/ (accessed on 2 January 2023).
- Johns Hopkins University. COVID-19 Mortality Analyses. 2023. Available online: https://coronavirus.jhu.edu/data/mortality (accessed on 22 January 2024).
- Reuben, R.C.; Danladi, M.M.A.; Saleh, D.A.; Ejembi, P.E. Knowledge, Attitudes and Practices Towards COVID-19: An Epidemiological Survey in North-Central Nigeria. J. Community Health 2021, 46, 457–470. [Google Scholar] [CrossRef]
- Lee, S.K.; Sun, J.; Jang, S.; Connelly, S. Misinformation of COVID-19 vaccines and vaccine hesitancy. Sci. Rep. 2022, 12, 13681. [Google Scholar] [CrossRef]
- Acharya, S.R.; Moon, D.H.; Shin, Y.C. Assessing Attitude Toward COVID-19 Vaccination in South Korea. Front. Psychol. 2021, 12, 1–6. [Google Scholar] [CrossRef]
- Graham, M.S.; May, A.; Varsavsky, T.; Sudre, C.; Murray, B.; Klaser, K.; Antonelli, M.; Canas, L.; Molteni, E.; Modat, M.; et al. Knowledge barriers in the symptomatic-COVID-19 testing programme in the UK: An observational study. medRxiv 2021. [Google Scholar] [CrossRef]
- Li, Y.; Liu, G.; Egolet, R.O.; Yang, R.; Huang, Y.; Zheng, Z. Knowledge, attitudes, and practices related to COVID-19 among Malawi adults: A community-based survey. Int. J. Environ. Res. Public Health 2021, 18, 4090. [Google Scholar] [CrossRef]
- Chirwa, G.C. ‘Who knows more, and why?’ Explaining socioeconomic-related inequality in knowledge about HIV in Malawi. Sci. Afr. 2020, 7, e00213. [Google Scholar] [CrossRef]
- Islam, S.; Siddique, A.B.; Akter, R.; Tasnim, R.; Sujan, S.H.; Ward, P.R.; Sikder, T. Knowledge, attitudes and perceptions towards COVID-19 vaccinations: A cross-sectional community survey in Bangladesh. BMC Public Health 2021, 21, 1851. [Google Scholar] [CrossRef]
- Sengupta, M.; Dutta, S.; Roy, A.; Chakrabarti, S.; Mukhopadhyay, I. Knowledge, attitude and practice survey towards COVID-19 vaccination: A mediation analysis. Int. J. Health Plan. Manag. 2022, 37, 2063–2080. [Google Scholar] [CrossRef]
- Brynildsrud, O. COVID-19 prevalence estimation by random sampling in population—Optimal sample pooling under varying assumptions about true prevalence. BMC Med. Res. Methodol. 2020, 20, 196. [Google Scholar] [CrossRef]
- Wiegand, R.P. An Analysis of Cooperative Coevolutionary Algorithms; George Mason University: Fairfax, VA, USA, 2003; pp. 1–115. [Google Scholar]
- Wiegand, H. Kish, L.: Survey Sampling; John Wiley & Sons, Inc.: New York, London 1965, IX + 643 S., 31 Abb., 56 Tab., Preis 83 s. Biom. J. 1968, 10, 88–89. [Google Scholar] [CrossRef]
- Azene, Z.N.; Merid, M.W.; Muluneh, A.G.; Geberu, D.M.; Kassa, G.M.; Yenit, M.K.; Tilahun, S.Y.; Gelaye, K.A.; Mekonnen, H.S.; Azagew, A.W.; et al. Adherence towards COVID-19 mitigation measures and its associated factors among Gondar City residents: A community-based cross-sectional study in Northwest Ethiopia. PLoS ONE 2020, 15, e0244265. [Google Scholar] [CrossRef]
- Khamis, F.; Badahdah, A.; Al, N.; Furqan, M.; Lawati, A.; Al, J. Attitudes Towards COVID-19 Vaccine: A Survey of Health Care Workers in Oman. J. Epidemiol. Glob. Health 2022, 12, 1–6. [Google Scholar] [CrossRef]
- Al-Marshoudi, S.; Al-Balushi, H.; Al-Wahaibi, A.; Al-Khalili, S.; Al-Maani, A.; Al-Farsi, N.; Al-Jahwari, A.; Al-Habsi, Z.; Al-Shaibi, M.; Al-Msharfi, M.; et al. Knowledge, attitudes, and practices (Kap) toward the COVID-19 vaccine in Oman: A pre-campaign cross-sectional study. Vaccines 2021, 9, 602. [Google Scholar] [CrossRef]
- Cheng, J.Y.J.; Loong, S.S.E.; Ho, C.E.S.M.; Ng, K.J.; Ng, M.M.Q.; Chee, R.C.H.; Chin, T.X.L.; Fong, F.J.Y.; Goh, S.L.G.; Venkatesh, K.N.S.; et al. Knowledge, Attitudes, and Practices of COVID-19 Vaccination among Adults in Singapore: A Cross-Sectional Study. Am. J. Trop. Med. Hyg. 2022, 107, 540–550. [Google Scholar] [CrossRef]
- Sinuraya, R.K.; Kusuma, A.S.W.; Pardoel, Z.E.; Postma, M.J.; Suwantika, A.A. Parents’ Knowledge, Attitude, and Practice on Childhood Vaccination During the COVID-19 Pandemic in Indonesia. Patient Prefer. Adherence 2022, 16, 105–112. [Google Scholar] [CrossRef]
- Hossain, M.A.; Jahid, I.K.; Hossain, K.M.A.; Walton, L.M.; Uddin, Z.; Haque, O.; Kabir, F.; Arafat, S.M.Y.; Sakel, M.; Faruqui, R.; et al. Knowledge Attitudes and fear of COVID-19 during the Rapid Rise Period in Bangladesh. PLoS ONE 2020, 15, e0239646. [Google Scholar] [CrossRef]
- Banik, R.; Rahman, M.; Sikder, M.T.; Rahman, Q.M.; Pranta, M.U.R. Knowledge, attitudes, and practices related to the COVID-19 pandemic among Bangladeshi youth: A web-based cross-sectional analysis. J. Public Health 2023, 31, 9–19. [Google Scholar] [CrossRef]
- Rahman, S.M.M.; Akter, A.; Mostary, K.F.; Ferdousi, S.; Ummon, I.J.; Mubdi-Un-Naafi, S.; Rahman, M.M.; Uddin, M.G.M.N.; Tasmin, S.; Uddin, M.A.; et al. Assessment of knowledge, attitudes and practices towards prevention of coronavirus disease (COVID-19) among Bangladeshi population. Bangladesh Med. Res. Counc. Bull. 2020, 46, 73–82. [Google Scholar] [CrossRef]
- Adane, M.; Ademas, A.; Kloos, H. Knowledge, attitudes, and perceptions of COVID-19 vaccine and refusal to receive COVID-19 vaccine among healthcare workers in Northeastern Ethiopia. BMC Public Health 2022, 22, 128. [Google Scholar] [CrossRef] [PubMed]
- Lazarus, J.V.; Romero, D.; Kopka, C.J.; Karim, S.A.; Abu-Raddad, L.J.; Almeida, G.; Baptista-Leite, R.; Barocas, J.A.; Barreto, M.L.; Bar-Yam, Y.; et al. A multinational Delphi consensus to end the COVID-19 public health threat. Nature 2022, 611, 332–345. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Category | Number | Percentage |
|---|---|---|
| Gender | ||
| Male | 1116 | 36.4 |
| Female | 1947 | 63.6 |
| Age | ||
| 18–60 | 2788 | 92.0 |
| 61–100 | 242 | 8.0 |
| Education | ||
| No education | 326 | 10.7 |
| Primary incomplete | 1039 | 34.1 |
| Primary complete | 359 | 11.8 |
| Secondary incomplete | 626 | 20.6 |
| Secondary complete | 527 | 17.3 |
| College and above | 169 | 5.5 |
| Region | ||
| Southern | 1528 | 49.8 |
| Central | 737 | 24.0 |
| Northern | 803 | 26.2 |
| Location | ||
| Urban | 2046 | 66.7 |
| Rural | 1022 | 33.3 |
| Denomination | ||
| Christian | 2755 | 90.7 |
| Muslim | 263 | 8.7 |
| Others | 18 | 0.6 |
| Occupation | ||
| Unemployed | 1498 | 49.9 |
| Business | 1322 | 43.9 |
| Employed | 185 | 6.2 |
| Marital status | ||
| Married | 2086 | 69.3 |
| Not married | 566 | 18.8 |
| Widowed | 212 | 7.0 |
| Divorced | 145 | 4.8 |
| Family size | ||
| <four members | 1162 | 39.9 |
| >four members | 1746 | 60.0 |
| Monthly income of the household | ||
| Less than MK 35,000 | 1816 | 60.3 |
| MK 35,000 to MK 50,000 | 534 | 17.7 |
| MK 51,000 to MK100,000 | 370 | 12.3 |
| MK100,000 to MK500,000 | 267 | 8.9 |
| Greater than MK500,000 | 24 | 0.8 |
| Chronic illness | ||
| Yes | 432 | 14.1 |
| No | 2636 | 85.9 |
| Type of chronic illness? | ||
| Respiratory and lung disease | 52 | 1.7 |
| Cardiovascular disease | 186 | 6.1 |
| Diabetes Mellitus | 42 | 1.4 |
| HIV/AIDS | 152 | 5 |
| Factor | Frequency (%) |
|---|---|
| Do you know about the COVID-19 vaccine? (n = 3068) | |
| Yes | 2936 (95.7) |
| No | 132 (4.3) |
| Do you know about the effectiveness of COVID-19 vaccine? (n = 3018) | |
| Yes | 2063 (68.4) |
| No | 955 (31.6) |
| Which COVID-19 vaccines are currently being administered in Malawi (n =3068) | |
| AstraZeneca | 1639 (53.4) |
| Johnson & Johnson | 1840 (60.0) |
| Pfizer | 817 (26.6) |
| Not sure | 807 (26.3) |
| Does vaccination increase allergic reactions? (n = 3003) | |
| Yes | 1006 (33.5) |
| No | 1255 (41.8) |
| I don’t know | 742 (24.7) |
| Does vaccination increase autoimmune diseases? (n = 2894) | |
| Yes | 765 (26.4) |
| No | 1271 (43.9) |
| I don’t know | 858 (29.6) |
| Children do not require to get COVID-19 vaccination (n = 2962) | |
| Yes | 1228 (41.5) |
| No | 1340 (45.2) |
| I don’t know | 394 (13.3) |
| Vaccine against COVID-19 is available free of cost (n = 2998) | |
| Yes | 2736 (91.3) |
| No | 123 (4.1) |
| I don’t know | 139 (4.6) |
| Variables | Vaccination Knowledge | p-Value | Attitude | p-Value | Vaccination Practice | p-Value | |||
|---|---|---|---|---|---|---|---|---|---|
| Good | Poor | Favorable | Unfavorable | Went for Vaccination | Did Not Go for Vaccination | ||||
| Gender | |||||||||
| Male | 882 (87.3) | 130 (12.8) | 0.20 | 912 (92.3) | 76 (7.7) | 0.02 | 480 (43.8) | 615 (51.2) | 0.005 |
| Female | 1491 (85.5) | 253 (14.5) | 1522 (89.6) | 177 (11.4) | 742 (38.6) | 1178 (61.4) | |||
| Age | |||||||||
| 18–60 | 2166 (86.2) | 346 (13.8) | 0.50 | 2216 (90.6) | 230 (9.4) | 0.71 | 1089 (39.7) | 1655 (60.3) | 0.000 |
| 61–100 | 186 (84.5) | 34 (15.5) | 194 (89.8) | 22 (10.2) | 122 (51.3) | 116 (49.3) | |||
| Education | |||||||||
| No education | 247 (83.2) | 50 (16.8) | 258 (88.7) | 33 (11.3) | 134 (41.4) | 190 (58.6) | |||
| Primary incomplete | 741 (81.1) | 173 (18.9) | 809 (89.6) | 94 (10.4) | 368 (36.3) | 646 (63.7) | |||
| Primary complete | 282 (85.5) | 48 (14.5) | 0.000 | 294 (92.2) | 25 (7.8) | 0.21 | 146 (40.9) | 211 (59.1) | 0.000 |
| Secondary incomplete | 498 (88.3) | 66 (11.7) | 509 (92.7) | 40 (7.3) | 247 (40.1) | 369 (59.9) | |||
| Secondary complete | 443 (93.1) | 33 (6.9) | 415 (91.0) | 41 (9.0) | 216 (41.4) | 305 (58.4) | |||
| College and above | 150 (93.8) | 10 (6.2) | 137 (88.4) | 18 (11.6) | 101 (60.8) | 65 (39.2) | |||
| Region | |||||||||
| Southern | 1128 (87.1) | 167 (12.9) | 1130 (98.9) | 122 (1.1) | 0.52 | 493 (32.8) | 1010 (67.2) | ||
| Central | 583 (86.4) | 92 (13.6) | 0.20 | 601 (90.0) | 67 (10.0) | 358 (49.7) | 363 (50.3) | 0.000 | |
| Northern | 665 (84.3) | 124 (15.7) | 705 (91.6) | 65 (8.4) | 372 (46.8) | 423 (53.2) | |||
| Location | |||||||||
| Urban | 1594 (87.6) | 225 (12.4) | 0.001 | 1598 (90.3) | 172 (9.7) | 0.50 | 845 (41.9) | 1174 (58.1) | 0.03 |
| Rural | 782 (83.2) | 158 (16.8) | 838 (91.1) | 82 (8.9) | 378 (37.8) | 622 (62.2) | |||
| Denomination | |||||||||
| Christian | 2141 (86.5) | 335 (13.5) | 2193 (91.0) | 217 (9.0) | 0.02 | 1115 (41.1) | 1597 (58.9) | 0.20 | |
| Muslim | 201 (82.7) | 42 (17.3) | 0.08 | 208 (87.0) | 31 (13.0) | 95 (36.5) | 165 (63.5) | ||
| Others | 10 (71.4) | 4 (28.6) | 13 (76.5) | 4 (23.5) | 5 (29.4) | 12 (70.6) | |||
| Occupation | |||||||||
| Unemployed | 1124 (83.9) | 215 (16.1) | 1181 (90.3) | 127 (9.7) | 563 (38.2) | 910 (61.8) | |||
| Business | 1036 (86.4) | 163 (13.6) | 0.000 | 1059 (90.8) | 107 (9.2) | 0.31 | 531 (40.8) | 772 (59.2) | 0.000 |
| Employed | 166 (98.2) | 3 (1.8) | 155 (93.9) | 10 (6.1) | 106 (58.0) | 77 (42.0) | |||
| Marital status | |||||||||
| Married | 1599 (85.8) | 264 (14.2) | 1642 (90.4) | 174 (9.6) | 831 (40.5) | 1221 (59.5) | |||
| Not married | 464 (89.4) | 55 (10.6) | 0.009 | 461 (91.5) | 43 (8.5) | 0.85 | 207 (37.2) | 349 (62.8) | 0.007 |
| Widowed | 153 (79.7) | 39 (20.3) | 167 (90.3) | 19 (9.7) | 108 (50.9) | 104 (49.1) | |||
| Divorced | 116 (87.2) | 17 (12.8) | 121 (89.6) | 14 (10.4) | 60 (41.4) | 85 (58.6) | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chisale, M.R.O.; Kambalame, D.; Mwale, S.E.; Mbakaya, B.C.; Mankhamba, R.; Kumwenda, P.; Chilima, B.; Mitambo, C.; Chiwaula, M.; Nyambalo, B.; et al. Knowledge, Attitudes, and Practices on COVID-19 Vaccination among General Adult Population in Malawi: A Countrywide Cross-Sectional Survey. Vaccines 2024, 12, 221. https://doi.org/10.3390/vaccines12030221
Chisale MRO, Kambalame D, Mwale SE, Mbakaya BC, Mankhamba R, Kumwenda P, Chilima B, Mitambo C, Chiwaula M, Nyambalo B, et al. Knowledge, Attitudes, and Practices on COVID-19 Vaccination among General Adult Population in Malawi: A Countrywide Cross-Sectional Survey. Vaccines. 2024; 12(3):221. https://doi.org/10.3390/vaccines12030221
Chicago/Turabian StyleChisale, Master R. O., Dzinkambani Kambalame, Saul Eric Mwale, Balwani Chingatichifwe Mbakaya, Regina Mankhamba, Pizga Kumwenda, Ben Chilima, Collins Mitambo, Mavuto Chiwaula, Billy Nyambalo, and et al. 2024. "Knowledge, Attitudes, and Practices on COVID-19 Vaccination among General Adult Population in Malawi: A Countrywide Cross-Sectional Survey" Vaccines 12, no. 3: 221. https://doi.org/10.3390/vaccines12030221
APA StyleChisale, M. R. O., Kambalame, D., Mwale, S. E., Mbakaya, B. C., Mankhamba, R., Kumwenda, P., Chilima, B., Mitambo, C., Chiwaula, M., Nyambalo, B., Sambani, C., Gondwe, J., Muwalo, C., Dembo, A., Chinyamunyamu, L., Thomas, M., Kagoli, M., & Banda, E. C. (2024). Knowledge, Attitudes, and Practices on COVID-19 Vaccination among General Adult Population in Malawi: A Countrywide Cross-Sectional Survey. Vaccines, 12(3), 221. https://doi.org/10.3390/vaccines12030221