
Sudden Sensorineural Hearing Loss after COVID-19 Vaccination: A Review of the Available Evidence through the Prism of Causality Assessment


Abstract
1. Available Epidemiological Data on Sudden Sensorineural Hearing Loss
2. What Do We Currently Know about SSNHL Observed after mRNA COVID-19 Vaccination?
3. Quantification of Sudden Sensorineural Hearing Loss after COVID-19 Vaccination
4. Evaluation of Hearing Recovery in SSNHL Post-COVID-19 Vaccination: Benefits of Active Audiogram-Based Surveillance
5. When an Adverse Event Becomes an Adverse Effect and Then a Signal
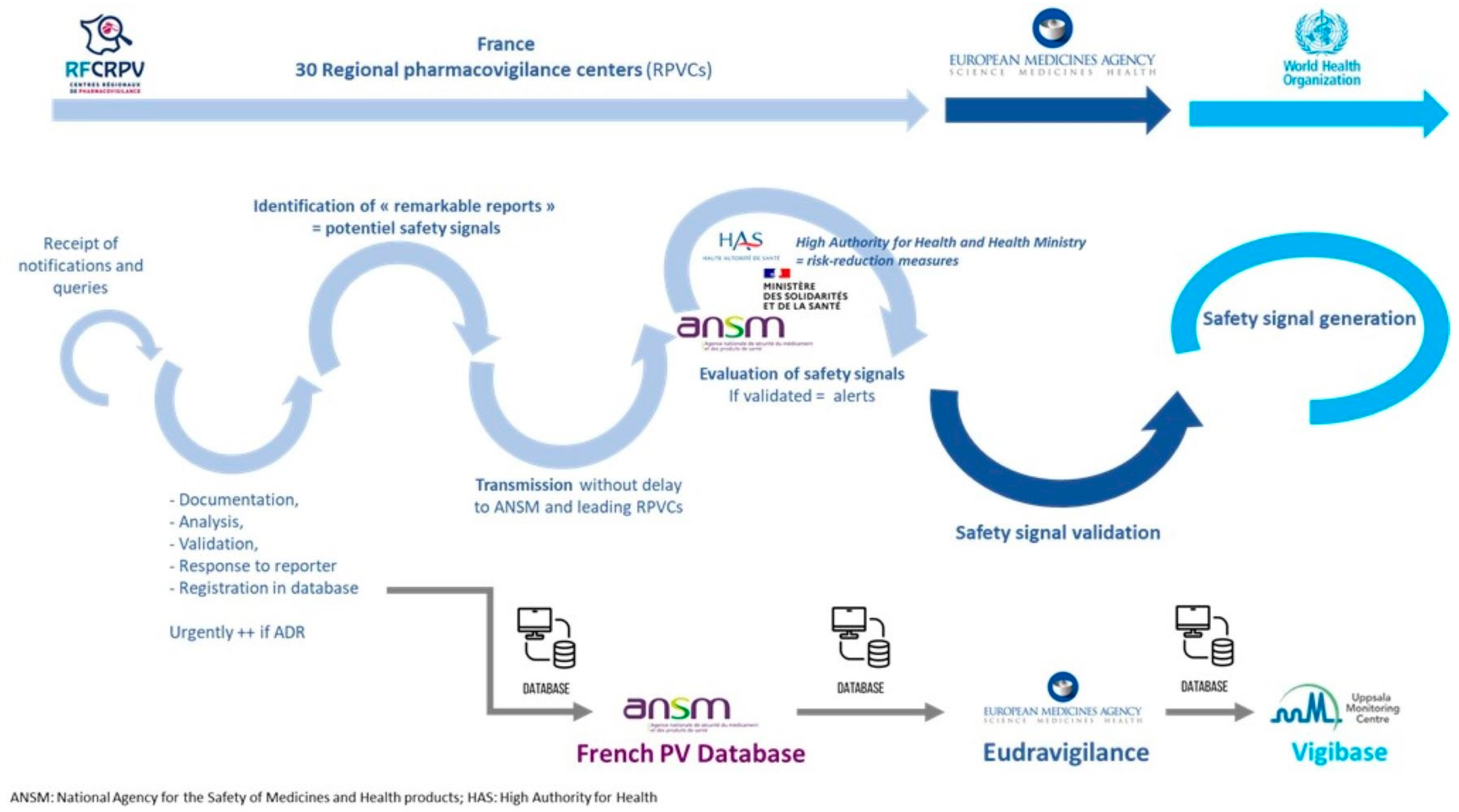
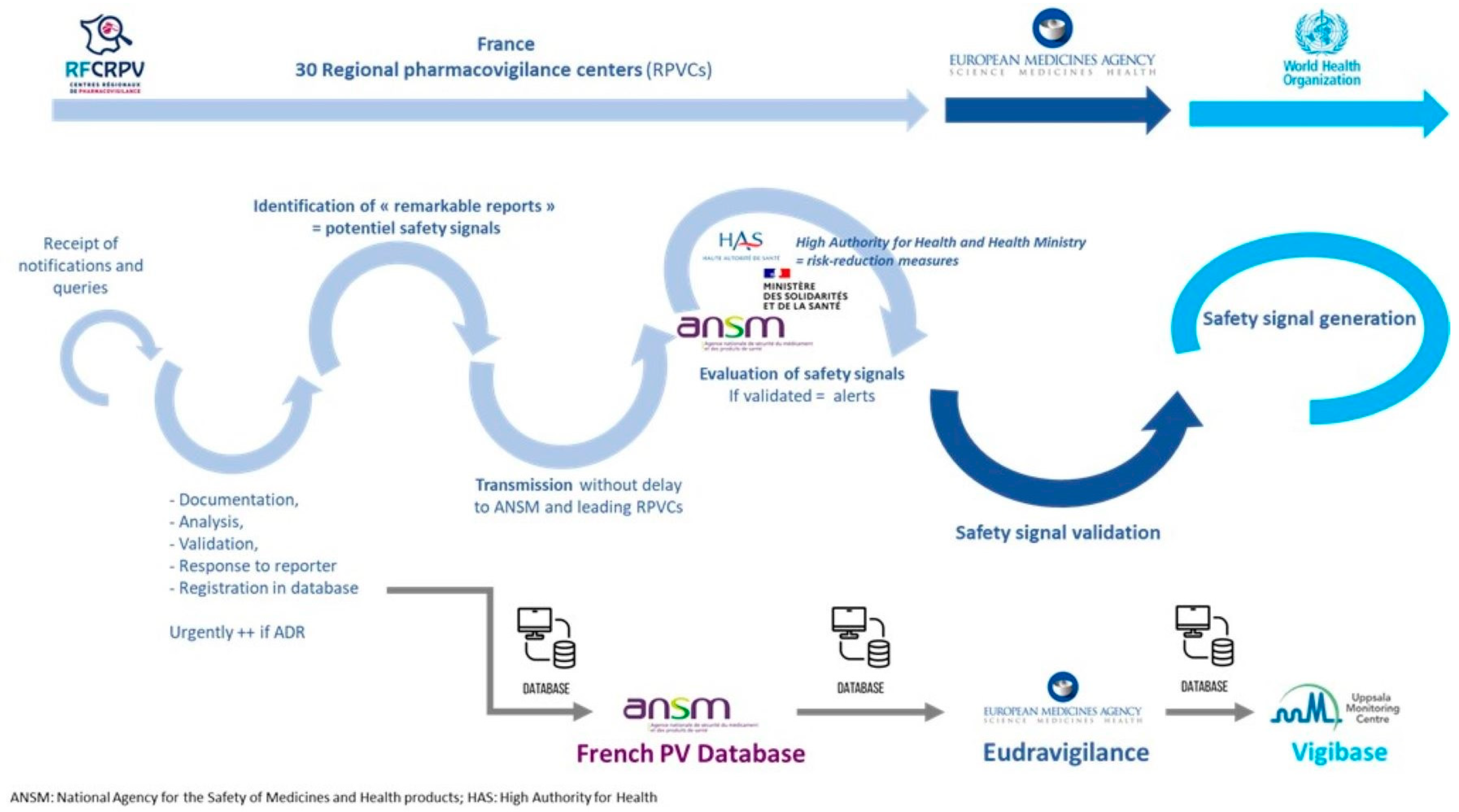
6. Two Different but Complementary Approaches to Safety Signal Evaluation
7. Rare Vaccine Adverse Events: Challenges and Perspectives
Author Contributions
Funding
Conflicts of Interest
References
- Hughes, G.B.; Freedman, M.A.; Haberkamp, T.J.; Guay, M.E. Sudden sensorineural hearing loss. Otolaryngol. Clin. N. Am. 1996, 29, 393–405. [Google Scholar] [CrossRef]
- Yin, J.; Mandrekar, S.J. High-Dose Glucocorticoids for Treating Sudden Hearing Loss: Cart before the Horse? NEJM Evid. 2024, 3, EVIDe2300296. [Google Scholar] [CrossRef] [PubMed]
- Chandrasekhar, S.S.; Tsai Do, B.S.; Schwartz, S.R.; Bontempo, L.J.; Faucett, E.A.; Finestone, S.A.; Hollingsworth, D.B.; Kelley, D.M.; Kmucha, S.T.; Moonis, G.; et al. Clinical Practice Guideline: Sudden Hearing Loss (Update). Otolaryngol. Head Neck Surg. 2019, 161, S1–S45. [Google Scholar] [CrossRef] [PubMed]
- Alexander, T.H.; Harris, J.P. Incidence of sudden sensorineural hearing loss. Otol. Neurotol. 2013, 34, 1586–1589. [Google Scholar] [CrossRef] [PubMed]
- Harris, J.P.; Sharp, P.A. Inner ear autoantibodies in patients with rapidly progressive sensorineural hearing loss. Laryngoscope 1990, 100, 516–524. [Google Scholar] [CrossRef]
- Lin, Y.T.; Young, Y.H. Retrocochlear mass lesion in mid-frequency sudden deafness. Otolaryngol. Head Neck Surg. 2008, 138, 13–17. [Google Scholar] [CrossRef]
- Jeong, K.H.; Choi, J.W.; Shin, J.E.; Kim, C.H. Abnormal Magnetic Resonance Imaging Findings in Patients with Sudden Sensorineural Hearing Loss: Vestibular Schwannoma as the Most Common Cause of MRI Abnormality. Medicine 2016, 95, e3557. [Google Scholar] [CrossRef]
- Cho, J.; Cheon, H.; Park, J.H.; Lee, H.J.; Kim, H.J.; Choi, H.G.; Koo, J.W.; Hong, S.K. Sudden sensorineural hearing loss associated with inner ear lesions detected by magnetic resonance imaging. PLoS ONE 2017, 12, e0186038. [Google Scholar] [CrossRef]
- Chau, J.K.; Lin, J.R.; Atashband, S.; Irvine, R.A.; Westerberg, B.D. Systematic review of the evidence for the etiology of adult sudden sensorineural hearing loss. Laryngoscope 2010, 120, 1011–1021. [Google Scholar] [CrossRef] [PubMed]
- Rowson, K.E.; Hinchcliffe, R. A virological and epidemiological study of patients with acute hearing loss. Lancet 1975, 1, 471–473. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Fu, Y.Y.; Zhang, T.Y. Role of viral infection in sudden hearing loss. J. Int. Med. Res. 2019, 47, 2865–2872. [Google Scholar] [CrossRef] [PubMed]
- Igarashi, M.; Alford, B.R.; Konishi, S. Functional and histopathological correlations after microembolism of the peripheral labyrinthite artery in the dog. Laryngoscope 1969, 79, 603–623. [Google Scholar] [CrossRef] [PubMed]
- Lin, R.J.; Krall, R.; Westerberg, B.D.; Chadha, N.K.; Chau, J.K. Systematic review and meta-analysis of the risk factors for sudden sensorineural hearing loss in adults. Laryngoscope 2012, 122, 624–635. [Google Scholar] [CrossRef] [PubMed]
- Gussen, R. Sudden hearing loss associated with cochlear membrane rupture. Two human temporal bone reports. Arch. Otolaryngol. 1981, 107, 598–600. [Google Scholar] [CrossRef] [PubMed]
- Okazaki, Y.; Yoshida, T.; Sugimoto, S.; Teranishi, M.; Kato, K.; Naganawa, S.; Sone, M. Significance of Endolymphatic Hydrops in Ears with Unilateral Sensorineural Hearing Loss. Otol. Neurotol. 2017, 38, 1076–1080. [Google Scholar] [CrossRef] [PubMed]
- Kang, K.T.; Young, Y.H. Sudden sensorineural hearing loss in a patient with primary antiphospholipid syndrome. J. Laryngol. Otol. 2009, 122, 204–206. [Google Scholar] [CrossRef]
- Di Stadio, A.; Dipietro, L.; Ralli, M.; Meneghello, F.; Minni, A.; Greco, A.; Stabile, M.R.; Bernitsas, E. Sudden hearing loss as an early detector of multiple sclerosis: A systematic review. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 4611–4624. [Google Scholar] [CrossRef]
- Oh, J.H.; Park, K.; Lee, S.J.; Shin, Y.R.; Choung, Y.H. Bilateral versus unilateral sudden sensorineural hearing loss. Otolaryngol. Head Neck Surg. 2007, 136, 87–91. [Google Scholar] [CrossRef]
- Cashman, K.A.; Wilkinson, E.R.; Zeng, X.; Cardile, A.P.; Facemire, P.R.; Bell, T.M.; Bearss, J.J.; Shaia, C.I.; Schmaljohn, C.S. Immune-Mediated Systemic Vasculitis as the Proposed Cause of Sudden-Onset Sensorineural Hearing Loss following Lassa Virus Exposure in Cynomolgus Macaques. mBio 2018, 9, e01896-18. [Google Scholar] [CrossRef]
- Ciodaro, F.; Freni, F.; Alberti, G.; Forelli, M.; Gazia, F.; Bruno, R.; Sherdell, E.P.; Galletti, B.; Galletti, F. Application of Cervical Vestibular-Evoked Myogenic Potentials in Adults with Moderate to Profound Sensorineural Hearing Loss: A Preliminary Study. Int. Arch. Otorhinolaryngol. 2020, 24, e5–e10. [Google Scholar] [CrossRef]
- Lechien, J.R.; Chiesa-Estomba, C.M.; De Siati, D.R.; Horoi, M.; Le Bon, S.D.; Rodriguez, A. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): A multicenter European study. Eur. Arch. Otorhinolaryngol. 2020, 277, 2251–2261. [Google Scholar] [CrossRef]
- De Melo, G.D.; Lazarini, F.; Levallois, S.; Hautefort, C.; Michel, V.; Larrous, F.; Verillaud, B.; Aparicio, C.; Wagner, S.; Gheusi, G.; et al. COVID-19-related anosmia is associated with viral persistence and inflammation in human olfactory epithelium and brain infection in hamsters. Sci. Transl. Med. 2021, 13, eabf8396. [Google Scholar] [CrossRef] [PubMed]
- Koumpa, F.S.; Forde, C.T.; Manjaly, J.G. Sudden irreversible hearing loss post COVID-19. BMJ Case Rep. 2020, 13, e238419. [Google Scholar] [CrossRef]
- Sriwijitalai, W.; Wiwanitkit, V. Hearing loss and COVID-19: A note. Am. J. Otolaryngol. 2020, 41, 102473. [Google Scholar] [CrossRef]
- Cure, E.; Cumhur Cure, M. Comment on “Hearing loss and COVID-19: A note”. Am. J. Otolaryngol. 2020, 41, 102513. [Google Scholar] [CrossRef] [PubMed]
- Karimi-Galougahi, M.; Naeini, A.S.; Raad, N.; Mikaniki, N.; Ghorbani, J. Vertigo and hearing loss during the COVID-19 pandemic—Is there an association? Acta Otorhinolaryngol. Ital. 2020, 40, 463–465. [Google Scholar] [CrossRef]
- Lamounier, P.; Franco Gonçalves, V.; Ramos, H.V.L.; Gobbo, D.A.; Teixeira, R.P.; Dos Reis, P.C.; Bahmad, F., Jr.; Cândido Costa, C. A 67-Year-Old Woman with Sudden Hearing Loss Associated with SARS-CoV-2 Infection. Am. J. Case Rep. 2020, 21, e927519. [Google Scholar] [CrossRef] [PubMed]
- Kilic, O.; Kalcioglu, M.T.; Cag, Y.; Tuysuz, O.; Pektas, E.; Caskurlu, H.; Cetın, F. Could sudden sensorineural hearing loss be the sole manifestation of COVID-19? An investigation into SARS-CoV-2 in the etiology of sudden sensorineural hearing loss. Int. J. Infect. Dis. 2020, 97, 208–211. [Google Scholar] [CrossRef]
- Lang, B.; Hintze, J.; Conlon, B. Coronavirus disease 2019 and sudden sensorineural hearing loss. J. Laryngol. Otol. 2020, 134, 1026–1028. [Google Scholar] [CrossRef]
- Umashankar, A.; Prakash, P.; Prabhu, P. Sudden Sensorineural Hearing Loss Post Coronavirus Disease: A Systematic Review of Case Reports. Indian J. Otolaryngol. Head Neck Surg. 2022, 74 (Suppl. S2), 3028–3035. [Google Scholar] [CrossRef]
- Beckers, E.; Chouvel, P.; Cassetto, V.; Mustin, V. Sudden sensorineural hearing loss in COVID-19: A case report and literature review. Clin. Case Rep. 2021, 9, 2300–2304. [Google Scholar] [CrossRef] [PubMed]
- Ricciardiello, F.; Pisani, D.; Viola, P.; Cristiano, E.; Scarpa, A.; Giannone, A.; Longo, G.; Russo, G.; Bocchetti, M.; Coppola, C.; et al. Sudden Sensorineural Hearing Loss in Mild COVID-19: Case Series and Analysis of the Literature. Audiol. Res. 2021, 11, 313–326. [Google Scholar] [CrossRef] [PubMed]
- Saniasiaya, J. Hearing Loss in SARS-CoV-2: What Do We Know? Ear Nose Throat J. 2021, 100, 152S–154S. [Google Scholar] [CrossRef]
- Lorenzo-Villalba, N.; Pierre, L.; Guerrero-Niño, J.; Jannot, X.; Andrès, E. Hearing Loss and Sixth Cranial Nerve Paresis after COVID-19. Eur. J. Case Rep. Intern. Med. 2022, 9, 003221. [Google Scholar] [CrossRef]
- Chern, A.; Famuyide, A.O.; Moonis, G.; Lalwani, A.K. Bilateral Sudden Sensorineural Hearing Loss and Intralabyrinthine Hemorrhage in a Patient with COVID-19. Otol. Neurotol. 2021, 42, e10–e14. [Google Scholar] [CrossRef]
- Li, W.; Moore, M.J.; Vasilieva, N.; Sui, J.; Wong, S.K.; Berne, M.A.; Somasundaran, M.; Sullivan, J.L.; Luzuriaga, K.; Greenough, T.C.; et al. Angiotensin-converting enzyme 2 is a functional receptor for the SARS coronavirus. Nature 2003, 426, 450–454. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef] [PubMed]
- Umashankar, A.; Prakash, P.; Prabhu, P. Delta Variant of COVID-19 and Hearing Loss. Indian J. Otolaryngol. Head Neck Surg. 2023, 75, 2634–2636. [Google Scholar] [CrossRef]
- Wang, Q.; Gu, H.; Ren, J.; Zhao, Y.; Meng, Z. Analysis of characteristics of and risk factors for otological symptoms after COVID-19 infection. PLoS ONE 2024, 19, e0297100. [Google Scholar] [CrossRef]
- Rausch, C.; Qun-Ying, Y. COVID-19 vaccines and hearing loss and tinnitus. WHO Pharm. Newsl. 2022, 1, 18–22. Available online: https://apps.who.int/iris/rest/bitstreams/1407437/retrieve (accessed on 5 April 2022).
- Mustafa, M.W.M. Audiological profile of asymptomatic COVID-19 PCR-positive cases. Am. J. Otolaryngol. 2020, 41, 102483. [Google Scholar] [CrossRef] [PubMed]
- Jeong, J.; Choi, H.S. Sudden sensorineural hearing loss after COVID-19 vaccination. Int. J. Infect. Dis. 2021, 113, 341–343. [Google Scholar] [CrossRef] [PubMed]
- Wichova, H.; Miller, M.E.; Derebery, M.J. Otologic Manifestations after COVID-19 Vaccination: The House Ear Clinic Experience. Otol. Neurotol. 2021, 42, e1213–e1218. [Google Scholar] [CrossRef] [PubMed]
- Ekobena, P.; Rothuizen, L.E.; Bedussi, F.; Guilcher, P.; Meylan, S.; Ceschi, A.; Dao, K. Four cases of audio-vestibular disorders related to immunisation with SARS-CoV-2 mRNA vaccines. Int. J. Audiol. 2022, 5, 587–591. [Google Scholar] [CrossRef] [PubMed]
- Liew, X.W.; Tang, Z.H.M.; Ong, Y.Q.C.; See, K.C. Hearing Loss after COVID-19 and Non-COVID-19 Vaccination: A Systematic Review. Vaccines 2023, 11, 1834. [Google Scholar] [CrossRef] [PubMed]
- Formeister, E.J.; Wu, M.J.; Chari, D.A.; Meek, R., 3rd; Rauch, S.D.; Remenschneider, A.K.; Quesnel, A.M.; de Venecia, R.; Lee, D.J.; Chien, W.; et al. Assessment of Sudden Sensorineural Hearing Loss after COVID-19 Vaccination. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 307–315. [Google Scholar] [CrossRef] [PubMed]
- Formeister, E.J.; Chien, W.; Agrawal, Y.; Carey, J.P.; Stewart, C.M.; Sun, D.Q. Preliminary Analysis of Association between COVID-19 Vaccination and Sudden Hearing Loss Using US Centers for Disease Control and Prevention Vaccine Adverse Events Reporting System Data. JAMA Otolaryngol. Head Neck Surg. 2021, 147, 674–676. [Google Scholar] [CrossRef]
- Nieminen, T.A.; Kivekâs, I.; Artama, M.; Nohynek, H.; Kujansivu, J.; Hovi, P. Sudden hearing loss following vaccination against COVID-19. JAMA Otolaryngol. Head Neck Surg. 2023, 149, 133–140. [Google Scholar] [CrossRef]
- Yanir, Y.; Doweck, I.; Shibli, R.; Najjar-Debbiny, R.; Saliba, W. Association between the BNT162b2 Messenger RNA COVID-19 Vaccine and the Risk of Sudden Sensorineural Hearing Loss. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 299–306. [Google Scholar] [CrossRef]
- Chen, C.; Fu, F.; Ding, L.; Xiao, J. Hearing disorder following COVID-19 vaccination: A pharmacovigilance analysis using the Vaccine Adverse Event Reporting System. J. Clin. Pharm. Ther. 2022, 47, 1789–1795. [Google Scholar] [CrossRef]
- Thai-Van, H.; Valnet-Rabier, M.B.; Anciaux, M.; Lambert, A.; Maurier, A.; Cottin, J.; Pietri, T.; Destère, A.; Damin-Pernik, M.; Perrouin, F.; et al. Safety Signal Generation for Sudden Sensorineural Hearing Loss Following Messenger RNA COVID-19 Vaccination: Postmarketing Surveillance Using the French Pharmacovigilance Spontaneous Reporting Database. JMIR Public Health Surveill. 2023, 9, e45263. [Google Scholar] [CrossRef] [PubMed]
- Damkier, P.; Cleary, B.; Hallas, J.; Schmidt, J.H.; Ladebo, L.; Jensen, P.B.; Lund, L.C. Sudden Sensorineural Hearing Loss Following immunization with BNT162b2 or mRNA-1273: A danish population-based cohort study. Otolaryngol. Head Neck Surg. 2023, 169, 1472–1480. [Google Scholar] [CrossRef] [PubMed]
- Cohen, M.O.; Tamir, S.O.; O’ Rourke, N.; Marom, T. Audiometry-confirmed Sudden Sensorineural Hearing Loss incidence among COVID-19 patients and BNT162b2 vaccine recipiens. Otol. Neurotol. 2023, 44, e68–e72. [Google Scholar] [CrossRef] [PubMed]
- Fisher, R.; Tarnovsky, Y.; Hirshoren, N.; Kaufman, M.; Stern, S.S. The association between COVID-19 vaccination and idiopathic Sudden Sensorineural Hearing Loss, clinical manifestation and outcomes. Eur. Arch. Otorhinolaryngol. 2023, 280, 3609–3613. [Google Scholar] [CrossRef] [PubMed]
- Pisani, D.; Leopardi, G.; Viola, P.; Scarpa, A.; Ricciardiello, F.; Cerchiai, N.; Astorina, A.; Chiarella, G. Sudden sensorineural hearing loss after COVID-19 vaccine; A possible adverse reaction? Otolaryngol. Case Rep. 2021, 21, 100384. [Google Scholar] [CrossRef] [PubMed]
- Zoccali, F.; Cambria, F.; Colizza, A.; Ralli, M.; Greco, A.; de Vincentiis, M.; Petrella, C.; Fiore, M.; Minni, A.; Barbato, C. Sudden Sensorineural Hearing Loss after third booster of COVID-19 vaccine administration. Diagnostics 2022, 12, 2039. [Google Scholar] [CrossRef]
- Andrade, J.; Sessa, L.; Ephrat, M.; Truong, J.; Di Gregorio, R. A Case Report of Sudden Sensorineural Hearing Loss (SSNHL) after administration of the COVID-19 Vaccine. J. Pharm. Pract. 2022, 19, 8971900221147584. [Google Scholar] [CrossRef]
- Kuhn, M.; Heman-Ackah, S.E.; Shaikh, J.A.; Roehm, P.C. Sudden sensorineural hearing loss: A review of diagnosis, treatment, and prognosis. Trends Amplif. 2011, 15, 91–105. [Google Scholar] [CrossRef]
- Byl, F.M., Jr. Sudden hearing loss: Eight years’ experience and suggested prognostic table. Laryngoscope 1984, 94, 647–661. [Google Scholar] [CrossRef]
- Fetterman, B.L.; Saunders, J.E.; Luxford, W.M. Prognosis and treatment of sudden sensorineural hearing loss. Am. J. Otol. 1996, 17, 529–536. [Google Scholar]
- Tran Ba Huy, P.; Sauvaget, E. Idiopathic sudden sensorineural hearing loss is not an otologic emergency. Otol. Neurotol. 2005, 26, 896–902. [Google Scholar] [CrossRef]
- Cheng, Y.F.; Chu, Y.C.; Tu, T.Y.; Shiao, A.S.; Wu, S.L.; Liao, W.H. Modified Siegel’s criteria for sudden sensorineural hearing loss: Reporting recovery outcomes with matched pretreatment hearing grades. J. Chin. Med. Assoc. 2018, 81, 1008–1012. [Google Scholar] [CrossRef]
- Kandakure, V.T.; Kunjumon, R.; Dube, Y.; More, M.S.; Garje, S. A Prospective Study on Post Covid Sudden Onset Sensory Neural Hearing Loss and its Recovery. Indian J. Otolaryngol. Head Neck Surg. 2023, 75 (Suppl. S1), 451–457. [Google Scholar] [CrossRef] [PubMed]
- Siegel, L.G. The treatment of idiopathic sudden sensorineural hearing loss. Otolaryngol. Clin. N. Am. 1975, 8, 467–473. [Google Scholar] [CrossRef]
- Ulrich, A.K.; Sundaram, M.E.; Osterholm, M.T. Rare Sudden Sensorineural Hearing Loss Potentially Associated with COVID-19 Vaccination Does Not Outweigh the Benefit of COVID-19 Vaccines. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 315–316. [Google Scholar] [CrossRef] [PubMed]
- Briggs, S.E.; Brenner, M.J.; Chandrasekhar, S.S. Sudden Sensorineural Hearing Loss and COVID-19 Vaccination. JAMA Otolaryngol. Head Neck Surg. 2022, 148, 196–197. [Google Scholar] [CrossRef] [PubMed]
- Law, B.; Villaescusa, M.J. Safety Platform for Emergency Vaccines (SPEAC). Sensorineural Hearing Loss. V1.0. 28-2-23. Available online: http://zenodo.org/record/7705371#.ZCFZXPbP270 (accessed on 14 April 2023).
- Pradhan, P.; Lavallee, M.; Akinola, S.; Escobar Gimenes, F.R.; Berard, A.; Methot, J.; Piché, M.-E.; Gonella, J.M.; Cloutier, L.; Leclerc, J. Causality assessment of adverse drug reaction: A narrative review to find the most exhaustive and easy-to-use tool in post-authorization settings. J. Appl. Biomed. 2023, 21, 59–66. [Google Scholar] [CrossRef] [PubMed]
- Cercle de Réflexion sur l’Imputabilité (CRI); Arimone, Y.; Bidault, I.; Dutertre, J.P.; Gérardin, M.; Guy, C.; Haramburu, F.; Hillaire-Buys, D.; Meglio, C.; Penfornis, C.; et al. Update of the French drug reaction assessment method. Therapie 2011, 66, 517–525. [Google Scholar] [CrossRef] [PubMed]
- Sassolas, B.; Haddad, C.; Mockenhaupt, M.; Dunant, A.; Liss, Y.; Bork, K.; Haustein, U.F.; Vieluf, D.; Roujeau, J.C.; Le Louet, H. ALDEN, an algorithm for assessment of drug causality in Stevens-Johnson Syndrome and toxic epidermal necrolysis: Comparison with case-control analysis. Clin. Pharmacol. Ther. 2010, 88, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Causality Assessment of an Adverse Event Following Immunization (AEFI): User Manual Fir the Revised WHO Classification. Available online: https://www.who.int/publications/i/item/9789241516990 (accessed on 29 December 2023).
- Report of CIOMS/WHO Working Group on Vaccine Pharmacovigilance; Council for International Organizations of Medical Sciences: Geneva, Switzerland. 2012. Available online: http://www.who.int/vaccine_safety/initiative/tools/CIOMS_report_WG_vaccine.pdf (accessed on 29 December 2023).
- Hill, A.B. The Environment and Disease: Association or Causation? Proc. R. Soc. Med. 1965, 58, 295–300. [Google Scholar] [CrossRef]
- Jonville-Bera, A.P.; Gautier, S.; Micallef, J.; Massy, N.; Atzenhoffer, M.; Grandvuillemin, A.; Drici, M.D.; The French Network of Regional Pharmacovigilance Centres. Monitoring the safety of drugs and COVID-19 vaccines by the French Pharmacovigilance Centers during the pandemic: A win-win bet with Health Authorities! Therapies 2023, 78, 467–475. [Google Scholar] [CrossRef] [PubMed]
- Massy, N.; Atzenhoffer, M.; Boulay, C.; Pecquet, P.E.; Ledys, F.; Cracowski, J.L.; Masmoudi, K.; Lepelley, M.; Gras-Champel, V. COVID-19 et vaccins à adénovirus: Expérience française de suivi renforcé de pharmacovigilance. Therapies 2023, 78, 489–498. [Google Scholar] [CrossRef] [PubMed]
- Valnet-Rabier, M.B.; Tebacher, M.; Gautier, S.; Micallef, J.; Salvo, F.; Pariente, A.; Bagheri, H. Pharmacovigilance signals from active surveillance of mRNA platform vaccines (tozinameran and elasomeran). Therapies 2023, 78, 499–507. [Google Scholar] [CrossRef] [PubMed]
- Salvo, F.; Pariente, A.; Valnet-Rabier, M.B.; Drici, M.D.; Cholle, C.; Mathieu, C.; Singier, A.; Bagheri, H.; Tebacher, M.; Micallef, J.; et al. Role of spontaneous reporting in investigating the relationship between mRNA COVID-19 vaccines and myocarditis: The French perspective. Therapies 2023, 78, 509–515. [Google Scholar] [CrossRef]
- Abu Mouch, S.; Roguin, A.; Hellou, E.; Ishai, A.; Shoshan, U.; Mahamid, L.; Zoabi, M.; Aisman, M.; Goldschmid, N.; Yanay, N.B. Myocarditis following COVID-19 mRNA vaccination. Vaccine 2021, 39, 3790–3793. [Google Scholar] [CrossRef]
- Sexson Tejtel, S.K.; Munoz, F.M.; Al-Ammouri, I.; Savorgnan, F.; Guggilla, R.K.; Khuri-Bulos, N.; Phillips, L.; Engler, R.J. Myocarditis and pericarditis: Case definition and guidelines for data collection, analysis, and presentation of immunization safety data. Vaccine 2022, 40, 1499–1511. [Google Scholar] [CrossRef]
- Le Vu, S.; Bertrand, M.; Jabagi, M.J.; Botton, J.; Drouin, J.; Baricault, B.; Weill, A.; Dray-Spira, R.; Zureik, M. Age and sex-specific risks of myocarditis and pericarditis following COVID-19 messenger RNA vaccines. Nat. Commun. 2022, 13, 3633. [Google Scholar] [CrossRef]
- Chouchana, L.; Blet, A.; Al-Khalaf, M.; Kafil, T.S.; Nair, G.; Robblee, J.; Drici, M.; Valnet-Rabier, M.; Micallef, J.; Salvo, F.; et al. Features of Inflammatory Heart Reactions Following mRNA COVID-19 Vaccination at a Global Level. Clin. Pharmacol. Ther. 2022, 111, 605–613. [Google Scholar] [CrossRef]
- Pariente, A.; Bezin, J. Evaluation of COVID-19 vaccines: Pharmacoepidemiological aspects. Therapies 2021, 76, 305–309. [Google Scholar] [CrossRef] [PubMed]
- Dhodapkar, M.M.; Ross, J.S.; Ramachandran, R. Spontaneous reporting of post-market safety signals: What evidence should support regulatory action? BMJ 2022, 379, o2409. [Google Scholar] [CrossRef] [PubMed]
- Dhodapkar, M.M.; Shi, X.; Ramachandran, R.; Chen, E.M.; Wallach, J.D.; Ross, J.S. Characterization and corroboration of safety signals identified from the US Food and Drug Administration Adverse Event Reporting System, 2008–2019: Cross sectional study. BMJ 2022, 379, e071752. [Google Scholar] [CrossRef] [PubMed]
- Tyagi, S. Global research output in ‘pharmacovigilance’ during 2010–2020. Therapies 2022, 77, 273–290. [Google Scholar] [CrossRef] [PubMed]
- Lasser, K.E.; Allen, P.D.; Woolhandler, S.J.; Himmelstein, D.U.; Wolfe, S.M.; Bor, D.H. Timing of new black box warnings and withdrawals for precription medications. JAMA 2002, 287, 2215–2220. [Google Scholar] [CrossRef] [PubMed]
- Olivier, P.; Montastruc, J.L. The nature of the scientific evidence leading to drug withdrawals for pharmacovigilance reasons in France. Pharmacoepidemiol. Drug Saf. 2006, 15, 808–812. [Google Scholar] [CrossRef] [PubMed]
- Craveiro, N.S.; Lopes, B.S.; Tomás, L.; Almeida, S.F. Drug withdrawal due to safety: A review of the data supporting withdrawal decision. Curr. Drug Saf. 2020, 15, 4–12. [Google Scholar] [CrossRef] [PubMed]
- Khouri, C.; Petit, C.; Tod, M.; Lepelley, M.; Revol, B.; Roustit, M.; Cracowski, J.-L. Adverse drug reaction risks obtained from meta-analyses and pharmacovigilance disproportionality analyses are correlated in most cases. J. Clin. Epidemiol. 2021, 134, 14–21. [Google Scholar] [CrossRef]
- Khouri, C.; Fusaroli, M.; Salvo, F.; Raschi, E. Interpretation of Pharmacovigilance Disproportionality Analyses. Clin. Pharmacol. Ther. 2023, 114, 745–746. [Google Scholar] [CrossRef]
- Arnaud, M.; Bégaud, B.; Thurin, N.; Moore, N.; Pariente, A.; Salvo, F. Methods for safety signal detection in healthcare databases: A literature review. Expert Opin. Drug Saf. 2017, 16, 721–732. [Google Scholar] [CrossRef]
- Zureik, M.; Cuenot, F.; Bégaud, B. Pharmacoepidemiology and public decision. Therapies 2023, 78, 549–551. [Google Scholar] [CrossRef]
- Aronson, J.K.; Hauben, M. Anecdotes that provide definitive evidence. BMJ 2006, 333, 1267–1269. [Google Scholar] [CrossRef]
- Orhon, P.; Robert, M.; Morand, T.; Cracowski, J.L.; Khouri, C. Investigating the link between drug consumption and adverse events reporting in France. Fundam. Clin. Pharmacol. 2023, 37, 879–882. [Google Scholar] [CrossRef]
- Boulefaa, D.; Bagheri, H.; Salvo, F.; Rabier, M.B.; Geniaux, H.; Lepelley, M.; Rocher, F.; Mahe, J.; Grandvillemuin, A.; Hung, T.V. Sudden sensorineural hearing loss after mRNA COVID-19 vaccination: Early safety signal generation using disproportionality analysis on a nationwide pharmacovigilance database. Drug Saf. 2023; submitted. [Google Scholar]
- Faillie, J.L.; Montastruc, F.; Montastruc, J.L.; Pariente, A. Pharmacoepidemiology and its input to pharmacovigilance. Therapie 2016, 71, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Patadia, V.K.; Schuemie, M.J.; Coloma, P.; Herings, R.; Van Der Lei, J.; Straus, S.; Sturkenboom, M.; Trifiro, G. Evaluating performance of electronic healthcare records and spontaneous reporting data in drug safety signal detection. Int. J. Clin. Pharm. 2015, 37, 94–104. [Google Scholar] [CrossRef] [PubMed]
- Harenberg, J.; Jonas, J.B.; Trecca, E.M. A liaison between sudden sensorineural hearing loss and SARS-CoV-2 infection. Thromb. Haemost. 2020, 120, 1237–1239. [Google Scholar] [CrossRef] [PubMed]
- Degen, C.; Lenarz, T.; Willenborg, K. Acute profound sensorineural hearing loss after COVID-19 pneumonia. Mayo Clin. Proc. 2020, 95, 1801–1803. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
| Siegel’s Grade of Hearing Loss | Hearing Loss Degree (dB HL) |
|---|---|
| Grade 1 | ≤25 |
| Grade 2 | 26–40 |
| Grade 3 | 41–70 |
| Grade 4 | 71–90 |
| Grade 5 | >90 |
| Number of SSNHL Cases after mRNA COVID-19 Vaccination = 171 (From January 2021 to February 2022, in France) | ||||||
|---|---|---|---|---|---|---|
| Hearing Outcome Hearing loss N (%) | Complete Recovery | Partial Recovery | Slight Improvement | No Improvement | Non-Serviceable Ear | Total Number of Cases/Hearing Loss Grade |
| Grade 1 | 16 (10) | 0 | 0 | 15 (9) | 0 | 31 (18) |
| Grade 2 | 11 (6.5) | 6 (3) | 0 | 25 (15) | 0 | 42 (24.5) |
| Grade 3 | 11 (6.5) | 8 (5) | 1 (0.5) | 33 (19.5) | 0 | 53 (31) |
| Grade 4 | 1 (0.5) | 4 (2) | 3 (1.5) | 14 (8) | 0 | 22 (13) |
| Grade 5 | 0 | 2 (1) | 4 (2) | 0 | 17 (10) | 23 (13.5) |
| Total number of cases/outcome | 39 (23) | 20 (12) | 8 (4) | 87 (51) | 17 (10) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Thai-Van, H.; Bagheri, H.; Valnet-Rabier, M.-B. Sudden Sensorineural Hearing Loss after COVID-19 Vaccination: A Review of the Available Evidence through the Prism of Causality Assessment. Vaccines 2024, 12, 181. https://doi.org/10.3390/vaccines12020181
Thai-Van H, Bagheri H, Valnet-Rabier M-B. Sudden Sensorineural Hearing Loss after COVID-19 Vaccination: A Review of the Available Evidence through the Prism of Causality Assessment. Vaccines. 2024; 12(2):181. https://doi.org/10.3390/vaccines12020181
Chicago/Turabian StyleThai-Van, Hung, Haleh Bagheri, and Marie-Blanche Valnet-Rabier. 2024. "Sudden Sensorineural Hearing Loss after COVID-19 Vaccination: A Review of the Available Evidence through the Prism of Causality Assessment" Vaccines 12, no. 2: 181. https://doi.org/10.3390/vaccines12020181
APA StyleThai-Van, H., Bagheri, H., & Valnet-Rabier, M.-B. (2024). Sudden Sensorineural Hearing Loss after COVID-19 Vaccination: A Review of the Available Evidence through the Prism of Causality Assessment. Vaccines, 12(2), 181. https://doi.org/10.3390/vaccines12020181