
MV130 in the Prevention of Recurrent Respiratory Tract Infections: A Retrospective Real-World Study in Children and Adults

 ,
,  , and
, and
Abstract
1. Introduction
2. Materials and Methods
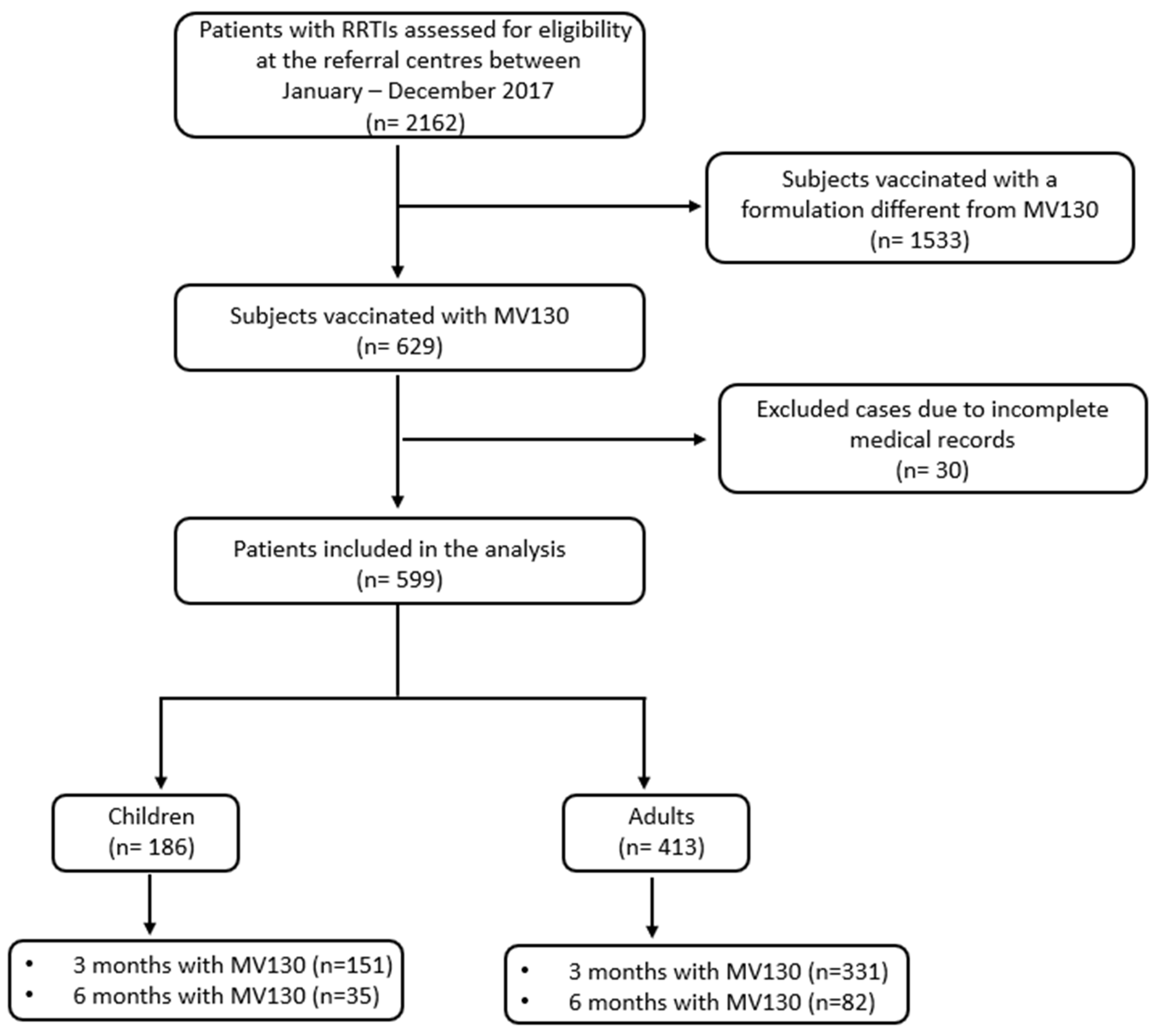
2.1. RWS Design and Data Collection
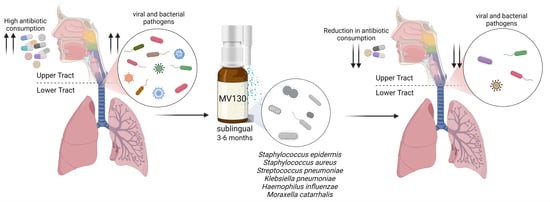
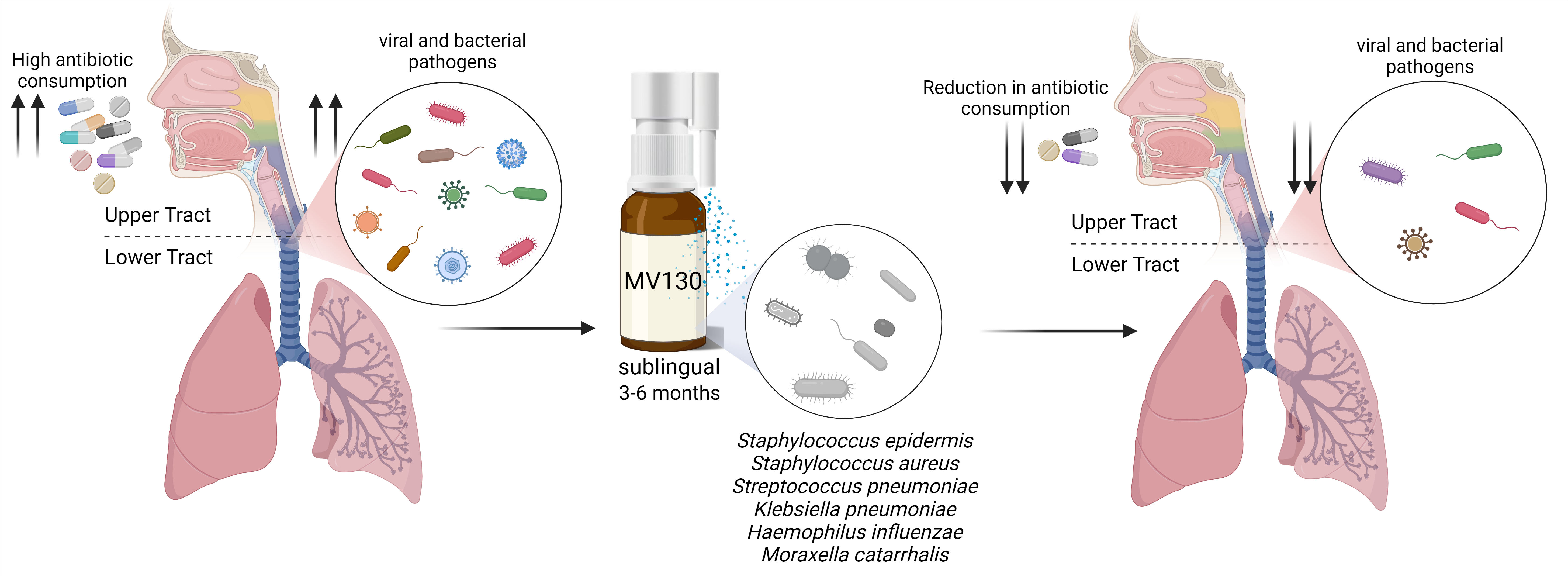
2.2. MV130 Prophylaxis
2.3. Statistical Analyses
3. Results
3.1. Patient Characteristics
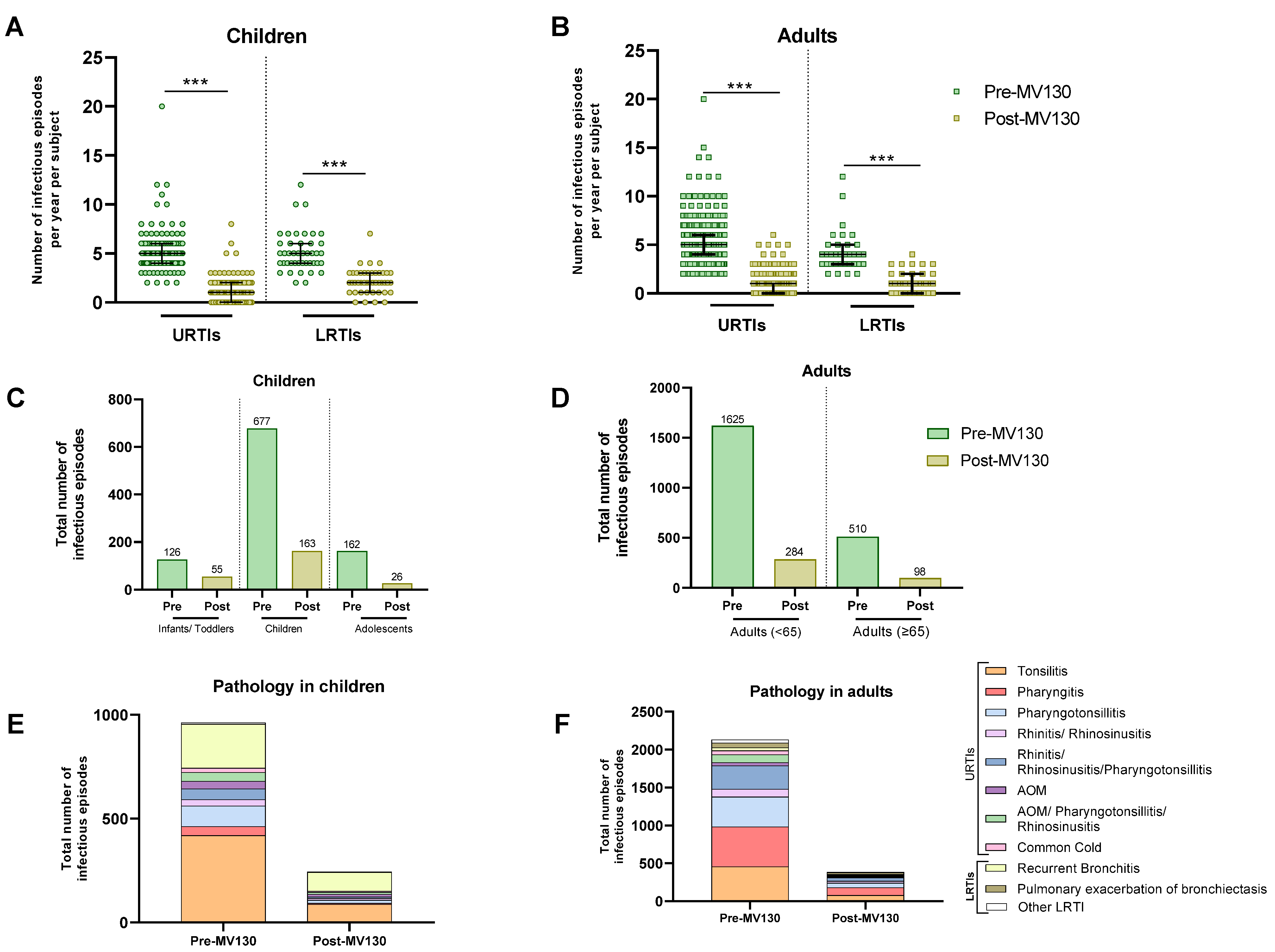
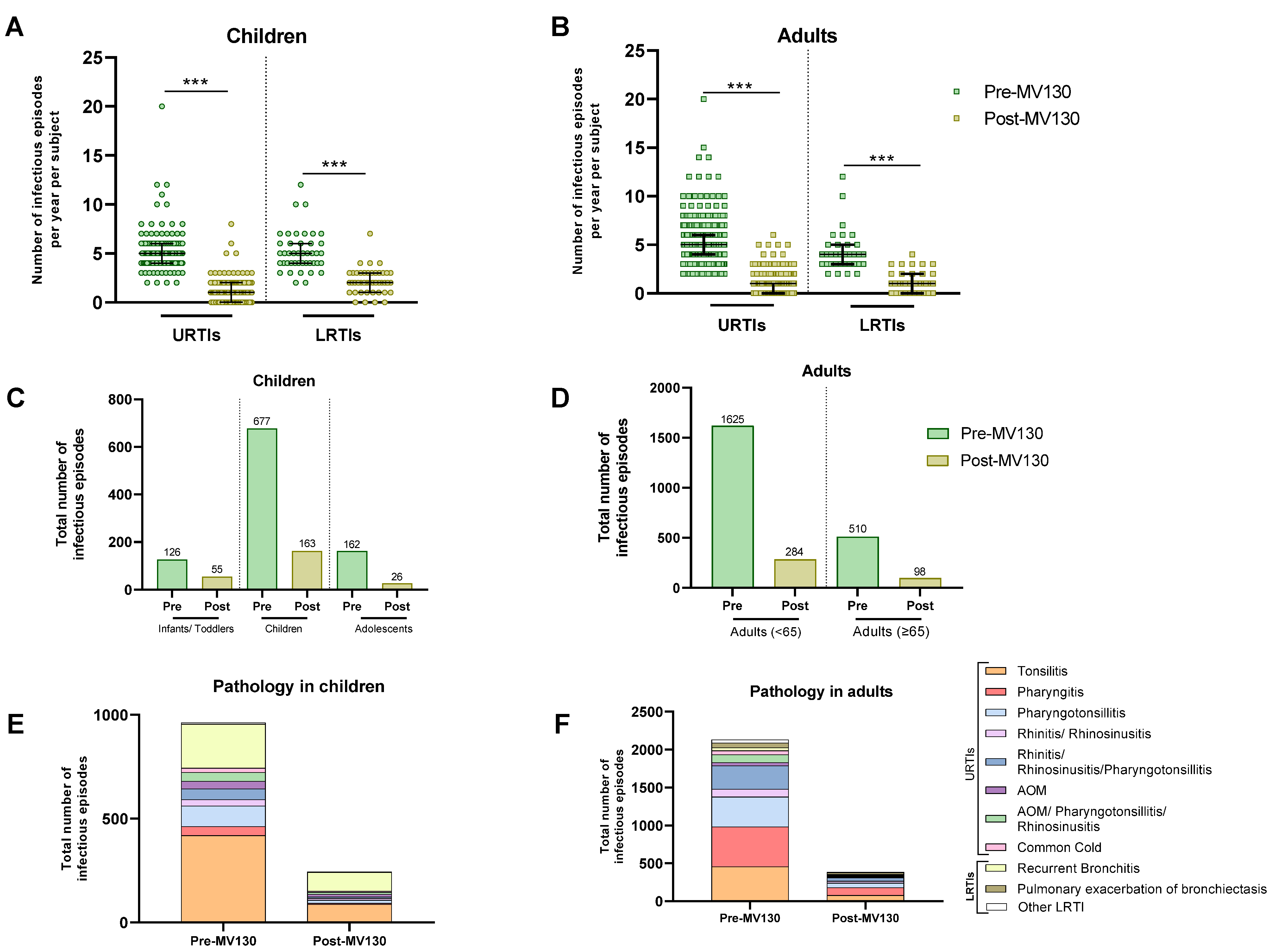
3.2. MV130 Prophylaxis Reduces the Number of RRTIs
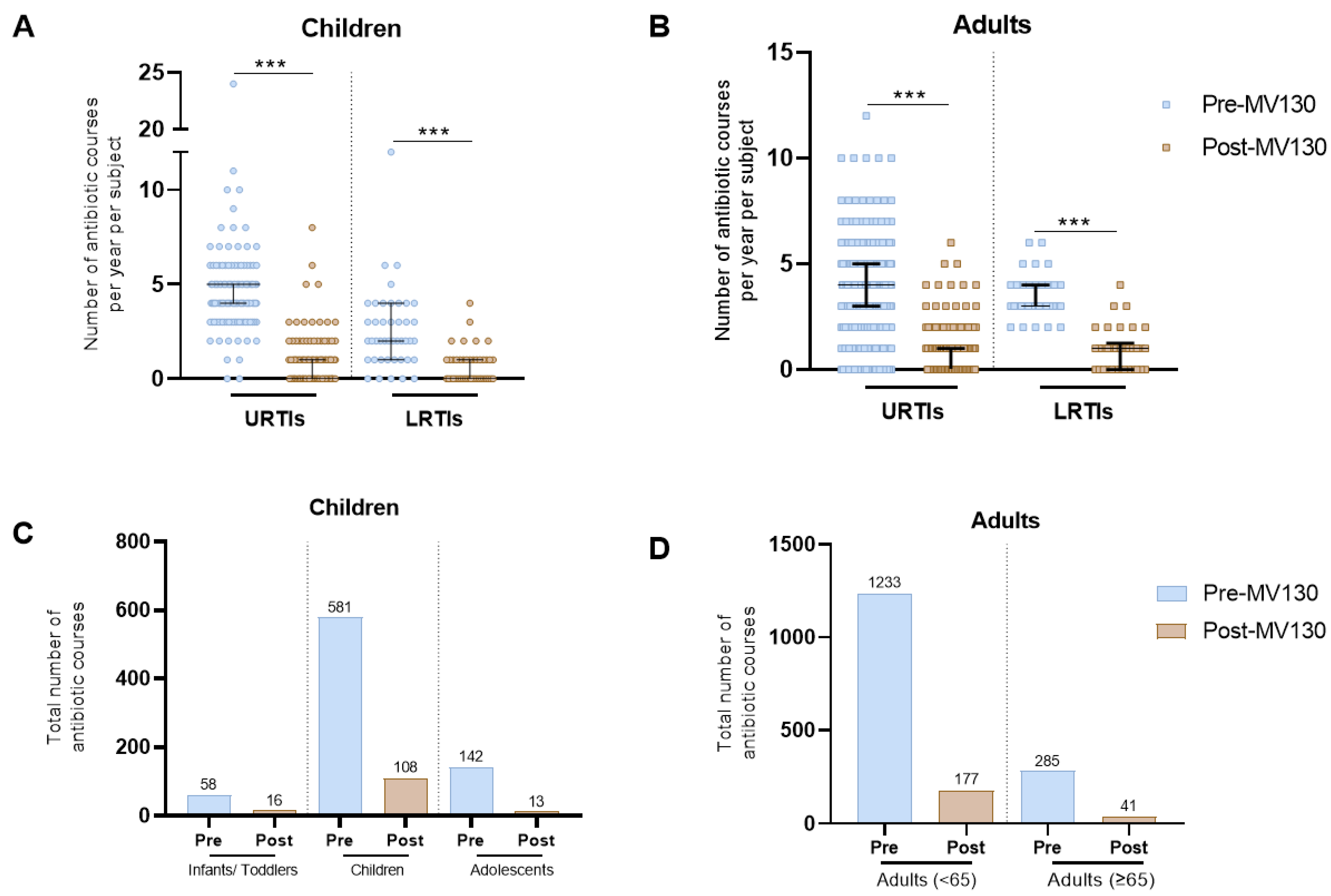
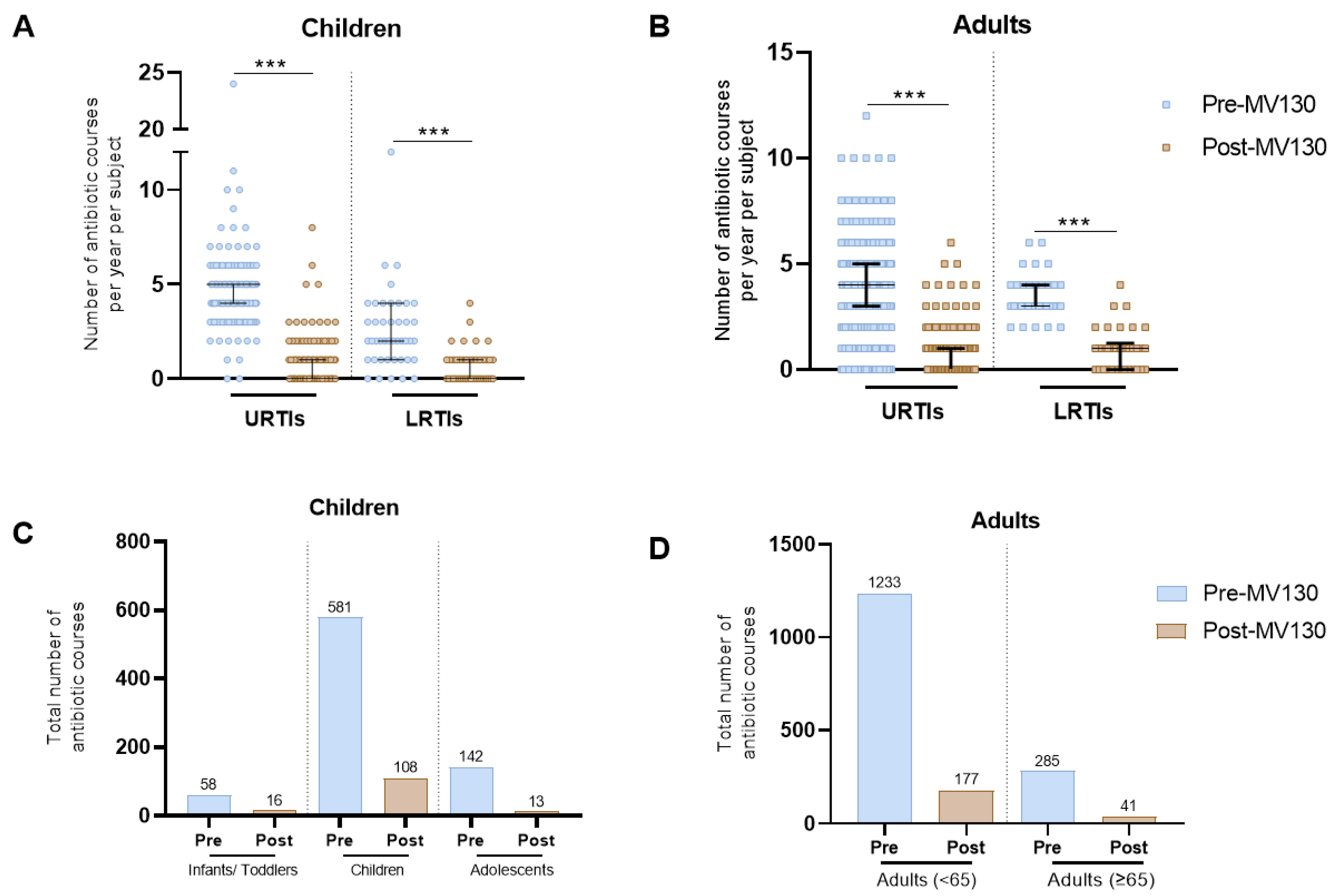
3.3. MV130 Prophylaxis Reduces Antibiotic Consumption
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ferkol, T.; Schraufnagel, D. The global burden of respiratory disease. Ann. Am. Thorac. Soc. 2014, 11, 404–406. [Google Scholar] [CrossRef] [PubMed]
- Jain, S. Epidemiology of viral pneumonia. Clin. Chest Med. 2017, 38, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Feleszko, W.; Marengo, R.; Vieira, A.S.; Ratajczak, K.; Mayorga Butron, J.L. Immunity-targeted approaches to the management of chronic and recurrent upper respiratory tract disorders in children. Clin. Otolaryngol. 2019, 44, 502–510. [Google Scholar] [CrossRef] [PubMed]
- Chiappini, E.; Santamaria, F.; Marseglia, G.L.; Marchisio, P.; Galli, L.; Cutrera, R.; De Martino, M.; Antonini, S.; Becherucci, P.; Biasci, P.; et al. Prevention of recurrent respiratory infections. Ital. J. Pediatr. 2021, 47, 211. [Google Scholar] [CrossRef]
- Connors, T.J.; Ravindranath, T.M.; Bickham, K.L.; Gordon, C.L.; Zhang, F.; Levin, B.; Baird, J.S.; Farber, D.L. Airway CD8+ T cells are associated with lung injury during infant viral respiratory tract infection. Am. J. Respir. Cell Mol. Biol. 2016, 54, 822–830. [Google Scholar] [CrossRef] [PubMed]
- Barr, R.; Green, C.A.; Sande, C.J.; Drysdale, S.B. Respiratory syncytial virus: Diagnosis, prevention and management. Ther. Adv. Infect. Dis. 2019, 6, 2049936119865798. [Google Scholar] [CrossRef]
- de Steenhuijsen Piters, W.A.; Watson, R.L.; de Koff, E.M.; Hasrat, R.; Arp, K.; Chu, M.L.J.; de Groot, P.C.; van Houten, M.A.; Sanders, E.A.; Bogaert, D. Early-life viral infections are associated with disadvantageous immune and microbiota profiles and recurrent respiratory infections. Nat. Microbiol. 2022, 7, 224–237. [Google Scholar] [CrossRef] [PubMed]
- Hendaus, M.A.; Jomha, F.A.; Alhammadi, A.H. Virus-induced secondary bacterial infection: A concise review. Ther. Clin. Risk Manag. 2015, 11, 1265–1271. [Google Scholar] [CrossRef]
- Schaad, U.B.; Esposito, S.; Razi, C.H. Diagnosis and management of recurrent respiratory tract infections in children: A practical guide. Arch. Pediatr. Infect. Dis. 2016, 4, e31039. [Google Scholar] [CrossRef]
- Manohar, P.; Loh, B.; Athira, S.; Nachimuthu, R.; Hua, X.; Welburn, S.C.; Leptihn, S. Secondary bacterial infections during pulmonary viral disease: Phage therapeutics as alternatives to antibiotics? Front. Microbiol. 2020, 11, 1434. [Google Scholar] [CrossRef]
- Claassen-Weitz, S.; Lim, K.Y.; Mullally, C.; Zar, H.J.; Nicol, M.P. The association between bacteria colonizing the upper respiratory tract and lower respiratory tract infection in young children: A systematic review and meta-analysis. Clin. Microbiol. Infect. 2021, 27, 1262–1270. [Google Scholar] [CrossRef] [PubMed]
- Prestinaci, F.; Pezzotti, P.; Pantosti, A. Antimicrobial resistance: A global multifaceted phenomenon. Pathog. Glob. Health 2015, 109, 309–318. [Google Scholar] [CrossRef] [PubMed]
- Aslam, B.; Wang, W.; Arshad, M.I.; Khurshid, M.; Muzammil, S.; Rasool, M.H.; Nisar, M.A.; Alvi, R.F.; Aslam, M.A.; Qamar, M.U. Antibiotic resistance: A rundown of a global crisis. Infect. Drug Resist. 2018, 11, 1645. [Google Scholar] [CrossRef] [PubMed]
- Day, M.J.; Jacobsson, S.; Spiteri, G.; Kulishev, C.; Sajedi, N.; Woodford, N.; Blumel, B.; van der Werf, M.J.; Amato-Gauci, A.J.; Unemo, M. Significant increase in azithromycin “resistance” and susceptibility to ceftriaxone and cefixime in Neisseria gonorrhoeae isolates in 26 European countries, 2019. BMC Infect. Dis. 2022, 22, 524. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Sanchez, F.; Gomez-Gomez, B. Antibiotic Management of Patients with Hematologic Malignancies: From Prophylaxis to Unusual Infections. Curr. Oncol. Rep. 2022, 24, 835–842. [Google Scholar] [CrossRef] [PubMed]
- Roca, I.; Akova, M.; Baquero, F.; Carlet, J.; Cavaleri, M.; Coenen, S.; Cohen, J.; Findlay, D.; Gyssens, I.; Heure, O. The global threat of antimicrobial resistance: Science for intervention. New Microbes New Infect. 2015, 6, 22–29. [Google Scholar] [CrossRef]
- Murray, C.J.; Ikuta, K.S.; Sharara, F.; Swetschinski, L.; Aguilar, G.R.; Gray, A.; Han, C.; Bisignano, C.; Rao, P.; Wool, E. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef]
- Pacios, O.; Blasco, L.; Bleriot, I.; Fernandez-Garcia, L.; González Bardanca, M.; Ambroa, A.; López, M.; Bou, G.; Tomás, M. Strategies to combat multidrug-resistant and persistent infectious diseases. Antibiotics 2020, 9, 65. [Google Scholar] [CrossRef]
- Lavelle, E.C.; Ward, R.W. Mucosal vaccines—Fortifying the frontiers. Nat. Rev. Immunol. 2022, 22, 236–250. [Google Scholar] [CrossRef]
- Sanchez-Ramon, S.; Conejero, L.; Netea, M.G.; Sancho, D.; Palomares, O.; Subiza, J.L. Trained Immunity-Based Vaccines: A New Paradigm for the Development of Broad-Spectrum Anti-infectious Formulations. Front. Immunol. 2018, 9, 2936. [Google Scholar] [CrossRef]
- Del Fresno, C.; Garcia-Arriaza, J.; Martinez-Cano, S.; Heras-Murillo, I.; Jarit-Cabanillas, A.; Amores-Iniesta, J.; Brandi, P.; Dunphy, G.; Suay-Corredera, C.; Pricolo, M.R.; et al. The Bacterial Mucosal Immunotherapy MV130 Protects Against SARS-CoV-2 Infection and Improves COVID-19 Vaccines Immunogenicity. Front. Immunol. 2021, 12, 748103. [Google Scholar] [CrossRef] [PubMed]
- Brandi, P.; Conejero, L.; Cueto, F.J.; Martinez-Cano, S.; Dunphy, G.; Gomez, M.J.; Relano, C.; Saz-Leal, P.; Enamorado, M.; Quintas, A.; et al. Trained immunity induction by the inactivated mucosal vaccine MV130 protects against experimental viral respiratory infections. Cell Rep. 2022, 38, 110184. [Google Scholar] [CrossRef] [PubMed]
- Cirauqui, C.; Benito-Villalvilla, C.; Sanchez-Ramon, S.; Sirvent, S.; Diez-Rivero, C.M.; Conejero, L.; Brandi, P.; Hernandez-Cillero, L.; Ochoa, J.L.; Perez-Villamil, B.; et al. Human dendritic cells activated with MV130 induce Th1, Th17 and IL-10 responses via RIPK2 and MyD88 signalling pathways. Eur. J. Immunol. 2018, 48, 180–193. [Google Scholar] [CrossRef] [PubMed]
- Netea, M.G.; Dominguez-Andres, J.; Barreiro, L.B.; Chavakis, T.; Divangahi, M.; Fuchs, E.; Joosten, L.A.B.; van der Meer, J.W.M.; Mhlanga, M.M.; Mulder, W.J.M.; et al. Defining trained immunity and its role in health and disease. Nat. Rev. Immunol. 2020, 20, 375–388. [Google Scholar] [CrossRef] [PubMed]
- Netea, M.G.; Joosten, L.A.; Latz, E.; Mills, K.H.; Natoli, G.; Stunnenberg, H.G.; O’Neill, L.A.; Xavier, R.J. Trained immunity: A program of innate immune memory in health and disease. Science 2016, 352, aaf1098. [Google Scholar] [CrossRef] [PubMed]
- Yan, J.; Nielsen, T.B.; Lu, P.; Talyansky, Y.; Slarve, M.; Reza, H.; Novakovic, B.; Netea, M.G.; Keller, A.E.; Warren, T. A protein-free vaccine stimulates innate immunity and protects against nosocomial pathogens. Sci. Transl. Med. 2023, 15, eadf9556. [Google Scholar] [CrossRef]
- Dotiwala, F.; Upadhyay, A.K. Next Generation Mucosal Vaccine Strategy for Respiratory Pathogens. Vaccines 2023, 11, 1585. [Google Scholar] [CrossRef]
- Alecsandru, D.; Valor, L.; Sanchez-Ramon, S.; Gil, J.; Carbone, J.; Navarro, J.; Rodriguez, J.; Rodriguez-Sainz, C.; Fernandez-Cruz, E. Sublingual therapeutic immunization with a polyvalent bacterial preparation in patients with recurrent respiratory infections: Immunomodulatory effect on antigen-specific memory CD4+ T cells and impact on clinical outcome. Clin. Exp. Immunol. 2011, 164, 100–107. [Google Scholar] [CrossRef]
- Garcia Gonzalez, L.A.; Arrutia, F. Mucosal bacterial immunotherapy with MV130 highly reduces the need of tonsillectomy in adults with recurrent tonsillitis. Hum. Vaccin. Immunother. 2019, 15, 2150–2153. [Google Scholar] [CrossRef] [PubMed]
- Nieto, A.; Mazon, A.; Nieto, M.; Calderon, R.; Calaforra, S.; Selva, B.; Uixera, S.; Palao, M.J.; Brandi, P.; Conejero, L.; et al. Bacterial Mucosal Immunotherapy with MV130 Prevents Recurrent Wheezing in Children: A Randomized, Double-Blind, Placebo-controlled Clinical Trial. Am. J. Respir. Crit. Care Med. 2021, 204, 462–472. [Google Scholar] [CrossRef] [PubMed]
- Hutubessy, R.; Lauer, J.A.; Giersing, B.; Sim, S.Y.; Jit, M.; Kaslow, D.; Botwright, S. The Full Value of Vaccine Assessments (FVVA): A framework for assessing and communicating the value of vaccines for investment and introduction decision-making. BMC Med. 2023, 21, 229. [Google Scholar] [CrossRef]
- Guevara-Hoyer, K.; Saz-Leal, P.; Diez-Rivero, C.M.; Ochoa-Grullon, J.; Fernandez-Arquero, M.; Perez de Diego, R.; Sanchez-Ramon, S. Trained Immunity Based-Vaccines as a Prophylactic Strategy in Common Variable Immunodeficiency. A Proof of Concept Study. Biomedicines 2020, 8, 203. [Google Scholar] [CrossRef] [PubMed]
- Ochoa-Grullon, J.; Benavente Cuesta, C.; Gonzalez Fernandez, A.; Cordero Torres, G.; Perez Lopez, C.; Pena Cortijo, A.; Conejero Hall, L.; Mateo Morales, M.; Rodriguez de la Pena, A.; Diez-Rivero, C.M.; et al. Trained Immunity-Based Vaccine in B Cell Hematological Malignancies with Recurrent Infections: A New Therapeutic Approach. Front. Immunol. 2020, 11, 611566. [Google Scholar] [CrossRef] [PubMed]
- EMA; Committe for Medicinal Products for Human Use. Bacterial Lysates-Containing Medicinal Products for Respiratory Conditions; Assessment report. EMA/502527/2019; EMA: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Sanchez-Ramon, S.; Fernandez-Paredes, L.; Saz-Leal, P.; Diez-Rivero, C.M.; Ochoa-Grullon, J.; Morado, C.; Macarron, P.; Martinez, C.; Villaverde, V.; de la Pena, A.R.; et al. Sublingual Bacterial Vaccination Reduces Recurrent Infections in Patients with Autoimmune Diseases under Immunosuppressant Treatment. Front. Immunol. 2021, 12, 675735. [Google Scholar] [CrossRef]
- van Houten, C.B.; Cohen, A.; Engelhard, D.; Hays, J.P.; Karlsson, R.; Moore, E.; Fernández, D.; Kreisberg, R.; Collins, L.V.; de Waal, W.; et al. Antibiotic misuse in respiratory tract infections in children and adults-a prospective, multicentre study (TAILORED Treatment). Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 505–514. [Google Scholar] [CrossRef]
- Pallon, J.; Rööst, M.; Sundqvist, M.; Hedin, K. The aetiology of pharyngotonsillitis in primary health care: A prospective observational study. BMC Infect. Dis. 2021, 21, 971. [Google Scholar] [CrossRef]
- Ross, E. Pharyngitis. In Scott-Brown’s Essential Otorhinolaryngology, Head & Neck Surgery; CRC Press: Boca Raton, FL, USA, 2022; pp. 281–284. [Google Scholar]
- Roberts, S.C.; Zembower, T.R. Global increases in antibiotic consumption: A concerning trend for WHO targets. Lancet Infect. Dis. 2021, 21, 10–11. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J.; Tsilika, M.; Moorlag, S.; Antonakos, N.; Kotsaki, A.; Domínguez-Andrés, J.; Kyriazopoulou, E.; Gkavogianni, T.; Adami, M.-E.; Damoraki, G.; et al. Activate: Randomized Clinical Trial of BCG Vaccination against Infection in the Elderly. Cell 2020, 183, 315–323.e319. [Google Scholar] [CrossRef]
- Arts, R.J.W.; Moorlag, S.; Novakovic, B.; Li, Y.; Wang, S.Y.; Oosting, M.; Kumar, V.; Xavier, R.J.; Wijmenga, C.; Joosten, L.A.B.; et al. BCG Vaccination Protects against Experimental Viral Infection in Humans through the Induction of Cytokines Associated with Trained Immunity. Cell Host Microbe 2018, 23, 89–100.e5. [Google Scholar] [CrossRef]
- Kleinnijenhuis, J.; Quintin, J.; Preijers, F.; Benn, C.S.; Joosten, L.A.; Jacobs, C.; van Loenhout, J.; Xavier, R.J.; Aaby, P.; van der Meer, J.W.; et al. Long-lasting effects of BCG vaccination on both heterologous Th1/Th17 responses and innate trained immunity. J. Innate Immun. 2014, 6, 152–158. [Google Scholar] [CrossRef]
- Bodas-Pinedo, A.; Lafuente, E.M.; Pelaez-Prestel, H.F.; Ras-Carmona, A.; Subiza, J.L.; Reche, P.A. Combining different bacteria in vaccine formulations enhances the chance for antiviral cross-reactive immunity: A detailed in silico analysis for influenza A virus. Front. Immunol. 2023, 14, 1235053. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | All (n = 599) | Adults (n = 413) | Children (n = 186) |
|---|---|---|---|
| n (%) | n (%) | n (%) | |
| Gender | |||
| Male | 236 (39) | 138 (33) | 98 (53) |
| Female | 363 (61) | 275 (67) | 88 (47) |
| Groups of age | |||
| Infants and toddlers (<2) | 26 (4) | NA | 26 (14) |
| Children (2–11) | 128 (21) | NA | 128 (69) |
| Adolescents (12–17) | 32 (5) | NA | 32 (17) |
| Adults (18–35) | 145 (25) | 145 (35) | NA |
| Adults (36–64) | 174 (29) | 174 (42) | NA |
| Adults (≥65) | 94 (16) | 94 (23) | NA |
| Length of MV130 immunotherapy | |||
| 3 months | 482 (80) | 331 (80) | 151 (81) |
| 6 months | 117 (20) | 82 (20) | 35 (19) |
| Upper Respiratory Infections | 522 (87) | 379 (92) | 143 (77) |
| Tonsillitis | 183 (31) | 101 (25) | 82 (44) |
| Pharyngitis | 107 (18) | 101 (25) | 6 (3) |
| Pharyngotonsillitis | 86 (14) | 66 (16) | 20 (11) |
| Rhinitis/rhinosinusitis | 27 (5) | 21 (5) | 6 (3) |
| Rhinitis/rhinosinusitis/pharyngotonsillitis | 64 (11) | 54 (13) | 10 (5) |
| AOM | 16 (3) | 8 (2) | 8 (4) |
| AOM/pharyngotonsillitis/rhinosinusitis | 27 (5) | 19 (5) | 8 (4) |
| Common cold | 12 (2) | 9 (2) | 3 (2) |
| Lower Respiratory Infections | 77 (13) | 34 (8) | 43 (23) |
| Pulmonary exacerbation of bronchiectasis | 14 (2) | 14 (3) | 0 (0) |
| Recurrent bronchitis | 51 (9) | 10 (2) | 41 (22) |
| Other lower respiratory infections | 12 (2) | 12 (3) | 2 (1) |
| Number of Subjects | Episodes (n) | Median [IQR] per Subject | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | P (Wilcoxon) | H-L | % Decrease in the Number of Episodes | ||
| Upper Respiratory Infections | 143 | 744 | 151 | 5.0 (4.0, 6.0) | 1.0 (0.0, 2.0) | <0.001 | −4.0 (−4.5,−4.0) | 80% |
| Tonsillitis | 82 | 419 | 87 | 5.0 (4.0, 6.0) | 1.0 (0.0, 2.0) | <0.001 | −4.0 (−4.5, −4.0) | 79% |
| Pharyngitis | 6 | 43 | 6 | 5.0 (4.3, 5.0) | 1.0 (0.3, 1.0) | 0.027 | −4.0 (−12.5, −2.0) | 86% |
| Pharyngotonsillitis | 20 | 99 | 15 | 4.0 (4.0, 6.0) | 1.0 (0.0, 1.0) | <0.001 | −4.0 (−0.5, −3.0) | 85% |
| Rhinitis/Rhinosinusitis | 6 | 31 | 9 | 5.0 (3.3, 6.0) | 1.5 (1.0, 2.0) | 0.027 | −3.0 (−6.5, −1.5) | 71% |
| Rhinitis/rhinosinusitis/Pharyngotonsillitis | 10 | 52 | 7 | 5.0 (4.3, 5.8) | 1.0 (0.0, 1.0) | 0.005 | −4.5 (−5.0, −4.0) | 87% |
| AOM | 8 | 36 | 12 | 4.5 (4.0, 5.0) | 2.0 (1.0, 2.0) | 0.011 | −3.0 (−4.0, −2.0) | 67% |
| AOM/Pharyngotonsillitis/Rhinosinusitis | 8 | 43 | 10 | 5.0 (4.8, 5.0) | 0.5 (0.0, 2.0) | 0.017 | −4.0 (−6.0, −2.0) | 77% |
| Common cold | 3 | 21 | 5 | 8.0 (6.5, 8.0) | 2.0 (1.5, 2.0) | 0.103 | −5.5 (−6.0, −4.0) | 76% |
| Lower Respiratory Infections | 43 | 221 | 93 | 5.0 (4.0, 6.0) | 2.0 (1.0, 3.0) | <0.001 | −3.0 (−3.5,−2.5) | 58% |
| Recurrent bronchitis | 41 | 211 | 90 | 5.0 (4.0, 6.0) | 2.0 (1.0, 3.0) | <0.001 | −2.5 (−3.5, −2.0) | 57% |
| Other infections of the lower respiratory tract | 2 | 10 | 3 | 5.0 (4.5, 5.5) | 1.5 (1.3, 1.8) | 0.178 | −3.5 (−4.0, −3.0) | 70% |
| All | 186 | 965 | 244 | 5.0 (4.0, 6.0) | 1.0 (0.0, 2.0) | <0.001 | −4.0 (−4.5,−2.5) | 75% |
| Number of Subjects | Episodes (n) | Median [IQR] per Subject | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | P (Wilcoxon) | H-L | % Decrease in the Number of Episodes | ||
| Upper Respiratory Infections | 379 | 1986 | 340 | 5.0 (4.0, 6.0) | 1.0 (0.0, 1.0) | <0.001 | −4.0 (−4.5,−4.0) | 83% |
| Tonsillitis | 101 | 455 | 79 | 4.0 (3.0, 5.0) | 0.0 (0.0, 1.0) | <0.001 | −3.5 (−4.0, −3.5) | 83% |
| Pharyngitis | 101 | 528 | 102 | 5.0 (4.0, 6.0) | 1.0 (0.0, 2.0) | <0.001 | −4.0 (−4.5, −3.5) | 81% |
| Pharyngotonsillitis | 66 | 392 | 59 | 6.0 (4.0, 7.0) | 1.0 (0.0, 1.0) | <0.001 | −5.0 (−5.5, −4.5) | 85% |
| Rhinitis/Rhinosinusitis | 21 | 103 | 26 | 4.0 (3.0, 6.0) | 1.0 (1.0, 2.0) | <0.001 | −3.5 (−4.5, −2.5) | 75% |
| Rhinitis/rhinosinusitis/Pharyngotonsillitis | 54 | 310 | 45 | 5.0 (4.0, 7.0) | 1.0 (0.0, 1.0) | <0.001 | −4.5 (−5.0, −4.0) | 85% |
| AOM | 8 | 42 | 11 | 5.0 (3.8, 5.8) | 1.5 (1.0, 2.0) | 0.011 | −3.7 (−6.0, −2.0) | 74% |
| AOM/Pharyngotonsillitis/Rhinosinusitis | 19 | 104 | 11 | 5.0 (4.0, 7.0) | 0.0 (0.0, 1.0) | <0.001 | −5.0 (−5.5, −4.0) | 89% |
| Common cold | 9 | 52 | 7 | 6.0 (5.0, 6.0) | 1.0 (0.0, 1.0) | 0.007 | −5.0 (−6.0, −4.0) | 87% |
| Lower Respiratory Infections | 34 | 145 | 42 | 4.0 (3.0, 5.0) | 1.0 (0.0, 2.0) | <0.001 | −3.0 (−3.5,−2.5) | 71% |
| Pulmonary exacerbations of bronchiectasis | 14 | 62 | 22 | 4.0 (3.0, 4.8) | 1.0 (1.0, 2.8) | 0.001 | −2.5 (−3.5, −1.5) | 65% |
| Recurrent bronchitis | 10 | 41 | 14 | 4.0 (3.3, 4.0) | 1.0 (1.0, 2.0) | 0.005 | −2.5 (−3.5, −2.0) | 66% |
| Other infections of the lower respiratory tract | 10 | 42 | 6 | 3.5 (2.3, 5.0) | 0.0 (0.0, 1.0) | 0.005 | −3.5 (−5.0, −2.5) | 86% |
| All | 413 | 2131 | 382 | 5.0 (4.0, 6.0) | 1.0 (0.0, 1.0) | <0.0001 | −4.0 (−4.5,−4.0) | 82% |
| Number of Subjects | Antibiotic Courses (n) | Median [IQR] per Subject | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | P (Wilcoxon) | H-L | % Decrease in the Number of Antibiotic Courses | ||
| Upper Respiratory Infections | 143 | 671 | 115 | 5.0 (4.0, 5.0) | 0.0 (0.0, 1.0) | <0.001 | −3.0 (−3.5,−3.0) | 83% |
| Tonsillitis | 82 | 393 | 72 | 5.0 (4.0, 5.0) | 0.0 (0.0, 1.0) | <0.001 | −4.0 (−4.5, −3.5) | 82% |
| Pharyngitis | 6 | 41 | 6 | 4.0 (3.3, 4.8) | 1.0 (0.3, 1.0) | 0.043 | −3.0 (−14, −0.5) | 85% |
| Pharyngotonsillitis | 20 | 76 | 6 | 4.0 (3.0, 4.0) | 0.0 (0.0, 1.0) | <0.001 | −3.5 (−4.0, −2.5) | 92% |
| Rhinitis/Rhinosinusitis | 6 | 24 | 5 | 3.0 (3.0, 3.8) | 1.0 (0.3, 1.0) | 0.028 | −2.5 (−5.5, −1.5) | 79% |
| Rhinitis/rhinosinusitis/Pharyngotonsillitis | 10 | 46 | 4 | 5.0 (4.0, 5.0) | 0.0 (0.0, 1.0) | 0.005 | −4.5 (−5.0, −3.5) | 91% |
| AOM | 8 | 36 | 12 | 4.5 (4.0, 5.0) | 2.0 (1.0, 2.0) | 0.012 | −3.0 (−4.0, −2.0) | 67% |
| AOM/Pharyngotonsillitis/Rhinosinusitis | 8 | 46 | 10 | 5.5 (4.8, 6.3) | 0.5 (0.0, 2.0) | 0.018 | −4.5 (−6.5, −2.5) | 78% |
| Common cold | 3 | 9 | 0 | 3.0 (3.0, 3.0) | 0.0 (0.0, 0.0) | 0.109 | −3.0 (−3.0, −3.0) | 100% |
| Lower Respiratory Infections | 43 | 110 | 30 | 2.0 (1.0, 3.5) | 0.0 (0.0, 1.0) | <0.001 | −1.5 (−2.0,−1.5) | 73% |
| Recurrent bronchitis | 41 | 103 | 27 | 2.0 (1.0, 3.0) | 0.0 (0.0, 1.0) | <0.001 | −1.5 (−2.0, −1.5) | 74% |
| Other infections of the lower respiratory tract | 2 | 7 | 3 | 3.5 (3.3, 3.8) | 1.5 (1.3, 1.8) | 0.180 | −2.0 (−2.0, −2.0) | 57% |
| All | 186 | 781 | 145 | 4.0 (3.0, 5.0) | 0.0 (0.0, 1.0) | <0.001 | −3.5 (−3.5,−3.0) | 81% |
| Number of Subjects | Antibiotic Courses (n) | Median [IQR] per Subject | ||||||
|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | P (Wilcoxon) | H-L | % Decrease in the Number of Antibiotic Courses | ||
| Upper Respiratory Infections | 379 | 1400 | 185 | 4.0 (3.0, 5.0) | 0.0 (0.0, 1.0) | <0.001 | −4.0 (−4.0,−3.5) | 87% |
| Tonsillitis | 101 | 425 | 64 | 4.0 (3.0, 5.0) | 0.0 (0.0, 1.0) | <0.001 | −3.5 (−4.0, 3.5) | 85% |
| Pharyngitis | 101 | 272 | 37 | 3.0 (2.0, 3.0) | 0.0 (0.0, 0.0) | <0.001 | −2.5 (−2.5, −2.0) | 86% |
| Pharyngotonsillitis | 66 | 269 | 33 | 4.0 (3.0, 5.0) | 0.0 (0.0, 1.0) | <0.001 | −3.5 (−4.0, −3.0) | 88% |
| Rhinitis/Rhinosinusitis | 21 | 67 | 16 | 3.0 (2.0, 4.0) | 1.0 (0.0, 1.0) | <0.001 | −2.0 (−3.0, −1.0) | 76% |
| Rhinitis/rhinosinusitis/Pharyngotonsillitis | 54 | 247 | 26 | 4.0 (4.0, 5.0) | 0.0 (0.0, 1.0) | <0.001 | −4.0 (−4.0, −3.5) | 89% |
| AOM | 8 | 37 | 4 | 3.5 (2.8, 5.8) | 0.0 (0.0, 1.0) | 0.012 | −3.8 (−6.5, −2.0) | 89% |
| AOM/Pharyngotonsillitis/Rhinosinusitis | 19 | 58 | 2 | 4.0 (2.0, 4.0) | 0.0 (0.0, 0.0) | <0.001 | −3.0 (−4.0, −2.0) | 97% |
| Common cold | 9 | 25 | 3 | 3.0 (1.0, 3.0) | 0.0 (0.0, 1.0) | 0.008 | −2.0 (−3.5, −1.5) | 88% |
| Lower Respiratory Infections | 34 | 118 | 33 | 3.0 (3.0, 4.0) | 1.0 (0.0, 1.0) | <0.001 | −2.5 (−3.0,−2.0) | 72% |
| Pulmonary exacerbations of bronchiectasis | 14 | 52 | 20 | 3.5 (3.0, 4.0) | 1.0 (1.0, 2.0) | 0.002 | −2.5 (−3.0, −1.5) | 62% |
| Recurrent bronchitis | 10 | 35 | 11 | 3.0 (3.0, 4.0) | 1.0 (1.0, 1.8) | 0.005 | −2.0 (−3.0, −1.5) | 69% |
| Other infections of the lower respiratory tract | 10 | 31 | 2 | 3.0 (2.3, 3.8) | 0.0 (0.0, 0.0) | 0.005 | −3.0 (−3.5, −2.0) | 94% |
| All | 413 | 1518 | 218 | 4.0 (3.0, 5.0) | 0.0 (0.0, 1.0) | <0.001 | −3.0 (−3.0,−3.0) | 86% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montalbán-Hernández, K.; Cogollo-García, A.; Girón de Velasco-Sada, P.; Caballero, R.; Casanovas, M.; Subiza, J.L.; Conejero, L. MV130 in the Prevention of Recurrent Respiratory Tract Infections: A Retrospective Real-World Study in Children and Adults. Vaccines 2024, 12, 172. https://doi.org/10.3390/vaccines12020172
Montalbán-Hernández K, Cogollo-García A, Girón de Velasco-Sada P, Caballero R, Casanovas M, Subiza JL, Conejero L. MV130 in the Prevention of Recurrent Respiratory Tract Infections: A Retrospective Real-World Study in Children and Adults. Vaccines. 2024; 12(2):172. https://doi.org/10.3390/vaccines12020172
Chicago/Turabian StyleMontalbán-Hernández, Karla, Ana Cogollo-García, Patricia Girón de Velasco-Sada, Raquel Caballero, Miguel Casanovas, José Luis Subiza, and Laura Conejero. 2024. "MV130 in the Prevention of Recurrent Respiratory Tract Infections: A Retrospective Real-World Study in Children and Adults" Vaccines 12, no. 2: 172. https://doi.org/10.3390/vaccines12020172
APA StyleMontalbán-Hernández, K., Cogollo-García, A., Girón de Velasco-Sada, P., Caballero, R., Casanovas, M., Subiza, J. L., & Conejero, L. (2024). MV130 in the Prevention of Recurrent Respiratory Tract Infections: A Retrospective Real-World Study in Children and Adults. Vaccines, 12(2), 172. https://doi.org/10.3390/vaccines12020172